
Abstract
Background
Existing research shows strong evidence of the independent effects of socioeconomic factors and gender on late-life health outcomes in India (Barooah, 2016; Brinda et al., 2016; Goli et al., 2014; Pandey, 2012; Roy & Chaudhuri, 2008; Sengupta & Agree, 2002). However, the potential interactive effects of these major social determinants on key dimensions of health remain understudied. Furthermore, studies of geographic variation in the effects of socioeconomic status (SES) and gender on older adults’ health are limited to the global North (Montez et al., 2016). Functional limitations are an especially important outcome. As an intermediary stage in the disablement process (Nagi, 1976; Verbrugge & Jette, 1994), they are highly prevalent, capture the effects of pathology and impairment, and are associated with decreased quality of life, increased risks of disability, falls and fractures, and depression, and increased health care costs (Tomey & Sowers, 2009). This study uses an intersectionality framework to explore potential sources of functional health disparities among adults aged 50 and over in India. Specifically, we use data from Wave 1 (2007–2010) of the Study of Global Ageing and Adult Health (SAGE) (N = 7150) to determine whether the effects of education on functional limitations differ for older men and women and if so, whether observed patterns in variation hold across six highly variable regional states in India.
Two salient features of the Indian context are the size of the country’s population (1.36 billion) and the marked regional differences that exist in language, culture, political economy, and level of social and economic development (World Bank, 2018). The sector aged 60 years and over has tripled over the past 50 years and is projected to rise from 125.7 million (9.4%) in 2017 to 316.8 million (19.1%) in 2050 (United Nations Department of Economic and Social Affairs, Population Division, 2017). Two thirds of older adults still live in villages, and nearly half are of poor SES (Dey et al., 2012). Just over half (52%) of India’s older adults (72% of females in both rural and urban areas, and 30% and 32% of males in urban and rural areas, respectively) are fully dependent on others for their day-to-day maintenance (Government of India, 2016).
The differential gender and educational experiences across regions make studies focusing on the influence of education on health highly pertinent in India. Broadly, education influences and enhances people’s social conditions. Formal education is a key pathway to social and economic capital, for example, knowledge, wealth, money, power, prestige, and social support networks (Link & Phelan, 1995). In India, societal preference for and disproportionate investments in males privileges their opportunities for educational attainment. They are favored in access to nutrition, education, decision making, landownership, labor market participation, socialized religious practices, and family authority, while women are traditionally relegated to a lifetime of household duties. These patterns of inequity and discrimination, which shape differential returns on education that men and women can realize during the life course, vary across India due to a mix of differences in cultural norms and practices and levels of state and regional social and economic development.
Regional Variations in Health
India is divided into six regions (central, north, northeast, east, south, and west) and comprises 29 states and 7 union territories. Gender, caste, and class norms differ greatly by region. Traditional gender roles in Northern states, for example, lead to discriminatory policies and practices that worsen health outcomes for women in these locales (Jejeebhoy & Sathar, 2001). Although India has enjoyed rapid economic development in recent decades, this progress is markedly uneven, even by developing country standards. Since the 1960s, regional growth performance has remained polarized into high-income states (e.g., Gujarat, Maharashtra, Punjab, and Haryana and more recently, Tamil Nadu and Karnataka) and low-income states (e.g., Orissa, Bihar, Rajasthan, Madhya Pradesh, Uttar Pradesh). A third “mobile” group of middle-income states, such as West Bengal, has experienced ups and downs in living standards. Less economically developed states and regions have lower levels of educational achievement—particularly among women, who are more likely to have poor health outcomes, such as disability and maternal mortality (Lee & Smith, 2014; Saikia et al., 2016).
Research on regional health differences has thus focused mainly on maternal and child mortality, with poorer outcomes in the North (Arokiasamy, 2004; Mukhopadhyay, 2015; Subramanian & Smith, 2006). The few studies on disability and other nonmortality outcomes have not shown clear regional differences. Saikia et al. (2016) examined eight categories of disability, for example, vision, hearing, speech, and movement disability and found low age-standardized prevalence rates in Assam, Karnataka, and Uttar Pradesh compared with West Bengal, Maharashtra, and Rajasthan. Contrary to expectations, Kastor and Mohanty (2016) found that persons aged 45 years and older in Karnataka had higher levels of impairment in activities of daily living (ADL), for example, walking, eating, dressing, and bathing, than their age peers in Rajasthan. However, differences in sample size and number and types of ADL indicators used to measure disability may account for this finding.
Regional Variations in the Effects of Education on Health
There is also little research on regional variations in the social determinants of functional limitations in later life in India; however, studies that do not compare regions report positive effects of education on physical functioning (Arokiasamy & Uttamacharya, 2015; Williams et al., 2017). The few studies that examine the health-related effects of education in different regions tend to focus on a single locale. For example, in a study of Dibrugarh district of the state of Assam, Medhi et al. (2006) found socioeconomic disparities in chronic diseases and disabilities among persons aged 60 and over, and working-class tea garden older adults were more likely to report ADL difficulties than higher socioeconomic age peers. Low educational attainment was also associated with ADL-IADL impairment. A Rapid Assessment of Disability in 50 villages of Andhra Pradesh showed similar patterns of socioeconomic effects on later life functional health (Ramachandra et al., 2016).
Regional Variations in Gender, Education, and Health
Researchers have explored regional and gender differences in health outcomes (Lee et al., 2015), but they have yet to consider the simultaneous effects of gender and SES on later life health. Women worldwide have lower age-specific mortality rates and more chronic illnesses than men (Bora & Saikia, 2015; Murray et al., 1992; Nathanson & Lopez, 1987). Studies on later life health in India confirm women’s disadvantages, including higher rates of physical functional impairment than men (Anson & Sun, 2002; Fikree & Pasha, 2004; Kastor & Mohanty, 2016; Leveille et al., 2000; Roy & Chaudhuri, 2008; Sulania et al., 2015).
Few studies on regional health variations report gender differences in disability. Sengupta and Agree (2002) used National Family Health data from representative samples of older adults in Uttar Pradesh and Haryana in the north and Kerala and Tamil Nadu in the south. Women in the two northern states were more likely than men in this region to have physical impairments of eyes and limbs and ADL-IADL disabilities, but disabilities did not differ by gender in the south.
Theoretical Framework: Intersectionality
Following Crenshaw’s (1989) original conceptualization of intersectionality, Hopkins (2017) notes that the term is “not only about multiple identities but is about relationality, social context, power relations, complexity, social justice and inequalities” (p. 1). Related social categories of individual and group identity can thus affect health outcomes through concurrent, interdependent systems of discrimination or disadvantage. This notion of the potentiated predictive power of co-occurring social forces has growing appeal across disciplines, topics, and methods. Long the purview of qualitative inquiry, intersectionality is also now gaining traction in multilevel quantitative studies of population health (Bauer, 2014; Green et al., 2017; Mullings & Schulz, 2006) and health disparities (Evans et al., 2018; Weber & Parra-Medina, 2003).
Recent literature that uses an intersectionality framework to examine health disparities moves beyond race, class, and gender by proposing to include location. Conceptualized as one axis in a social interactional process, location reveals “individual and group identities, systems of power, and processes of interaction and change” (Dhamoon, 2010; Sen et al., 2009: 398)—a process that may have implications for gendered health outcomes. A central point in assessing marginalization in terms of intersectional identities is that the effects are multiplicative rather than additive (Mwangi & Constance-Huggins, 2019).
We identified only one study that used an intersectional approach to functional health in later life. Warner and Brown (2011) used 1994–2006 U.S. Health and Retirement Study data to examine racial/ethnic/gender differences in intraindividual changes in functional limitations. Their findings strongly support an intersectional approach to examining the complex dynamics of late-life health and functional disparities.
Increased use of the concept of intersectionality has also led to its refinement. Choo and Ferree (2010: 129) distinguish three ways of understanding intersectionality in practice, which relate to the current study as follows: (a) inclusions, or group-centered processes that emphasize the central position of multiply-marginalized groups in the research (gender and education); (b) interactions, meaning the process that “highlights power as relational, seeing the interactions among variables as multiplying oppressions at various points of intersection, and drawing attention to unmarked groups” (age); and (b) institutional, whereby an entire social system is shaped through processes that are “fully interactive, historically co-determining, and complex” (geographic region).
Studies of the geographic locale as a dimension of intersectionality are largely confined to the national location in the global order (Whittle & Inhorn, 2001). However, spatial marginalization is a highly significant axis of intersectionality in developing countries where emergent markets and resources are unequally distributed, often along deeply rooted historical differences in culture, language, and religion. Kundu et al. (2013) note that India is still optimistic despite a recent shortfall in projected economic growth; yet, they also point to serious concerns that the country has not succeeded in transforming its growth into development. This failure is starkly apparent in regional imbalances, rural/urban disparities and inequalities across social and religious groups.
To date, work on the role of major social locators in India has focused on leveraging resources to improve behavioral and structural health care practices (see Iyer et al., 2007; Sen & Iyer, 2012; Sen et al., 2009). We extend this line of inquiry by examining how three key axes of social life operate in tandem to affect functional health in a nationally representative sample of older adults in India. We posit three questions to test the effects of education on functional limitations among men and women aged 50 and over in six regions of the country:
Do functional limitations among older adults in India vary by region?
Do the effects of education on older adults’ functional limitations vary by region?
Do the effects of education on functional limitations of older men and older women vary by region?
We hypothesize higher levels of functional limitations among older adults who live in northern states (e.g., Rajasthan, Uttar Pradesh) than those living in southern and coastal states (e.g., Karnataka, Maharashtra, and West Bengal). We expect outcomes in the northeast state of Assam to incline with the eastern state of West Bengal. We also expect that education will have greater effects on functional limitations in southern, eastern, and coastal states than northern states and wider educational differences in functional limitations for men in Southern states than Northern states. Finally, we hypothesize that the effects of education on functional limitations will be lower for women in Northern states than their counterparts in Southern states.
Data and Methods
Data Source and Sample
Data are from the World Health Organization Study on Global Aging and Adult Health (SAGE). SAGE is a longitudinal survey of probability samples of adults aged 50 and over in China, Ghana, India, Mexico, Russia, and South Africa. Wave I of the India sample (N = 7,150) was selected from six states: Maharashtra (West), Karnataka (Southern), West Bengal (Eastern), Assam (Northeastern), Rajasthan (Northern), and Uttar Pradesh (Central). A multistage stratified random sampling procedure was used to select eligible respondents through the random selection of households from primary sampling units (i.e., villages). Interviewers collected data on social, economic, physical, and psychological well-being face-to-face. For details on the study design, see Kowal et al. (2012).
We removed 8% of missing observations (listwise deletion from about 600 respondents) on our outcome variable. We examined the significance of associations of explanatory variables and the likelihood of missing; the association was not significant. Hence, listwise deletion of missing observations is not likely to bias our causal estimates, unless unmeasured factors exist.
Measures
Functional Limitations
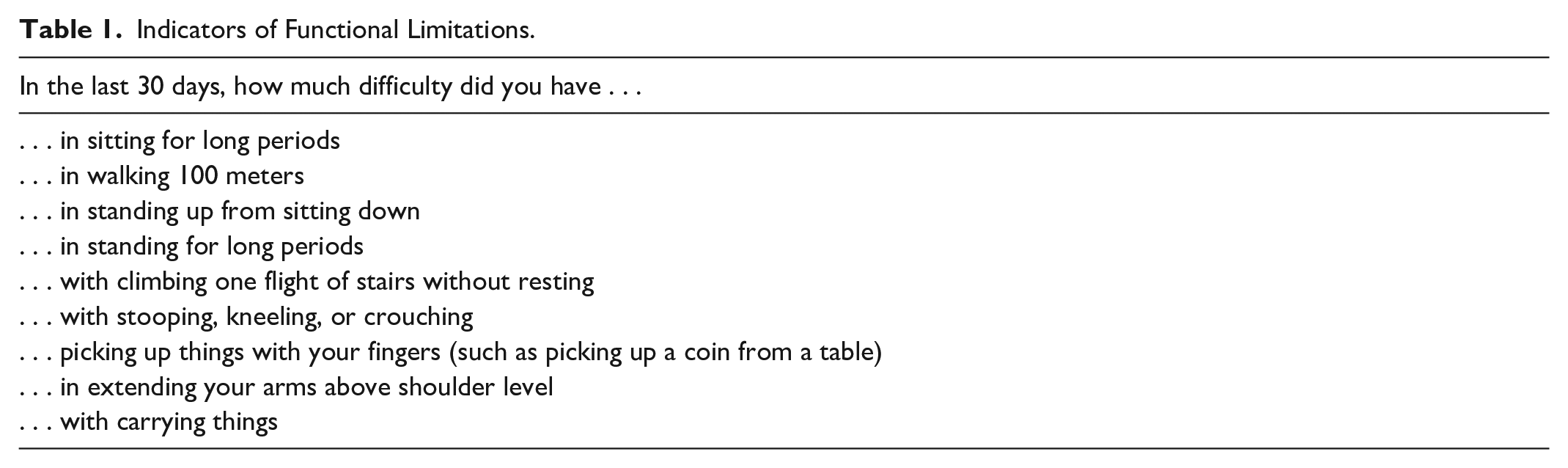
We used difficulties in performing nine activities (e.g., sitting for long periods, walking 100 meters, stooping) during the last 30 days (see Table 1) to assess functional limitations in later life. The functional limitations offer a global assessment of health which reflects the impact of disease and physical functioning across multiple physiological systems (Nagi, 1976; Verbrugge & Jette, 1994). All indicators of functional limitations loaded on a single factor (α = .89). Following Long and Pavalko (2004), we re-coded no difficulty/mild difficulty = 0, moderate difficulty = 1, and severe and extreme/cannot do = 2. We then summed responses for a total functional limitations score.
Indicators of Functional Limitations.
Educational Attainment
Education is our major explanatory variable. It is a preferred measure of SES due to difficulty in obtaining an accurate measure of income in India (Liberatos et al., 1988). For descriptive and bivariate analyses, we used education levels (no formal schooling = 0 to postgraduate degree completed = 6). We included years of education (range: 0–23 years) in regression models to capture greater variability in functional limitations.
Sociodemographic Characteristics
We adjusted for the following covariates that are likely to confound the relationship of education and functional limitation: gender (female = 1), age cohort (50–59 = 1, 60–69 = 2, 70–79 = 3, 80+ years = 4); marital status (married = 1; never married, separated, divorced or widowed = 0); place of birth (urban = 0; rural = 1); regional state (Assam = 1, Rajasthan= 2; Uttar Pradesh = 3, Maharashtra = 4, West Bengal = 5, Karnataka = 6); religious affiliation (Hindu = 1, Muslim = 2, other [Buddhist and Christian] = 3); and disadvantaged group status (scheduled caste/tribe = 1 vs. other castes = 0). Scheduled caste/tribe refers to groups, such as Dalits and indigenous people at the social, cultural, economic, and political margins of society.
We estimated the total effect of education on functional limitations, which is obtained without adjusting for mediator variables such as health behaviors. Controlling for variables in this pathway yields direct effects, or the remaining effects of education on functional limitations (Bhatta et al., 2017). Unlike the total effects of education, variation in the direct effect of education by gender and region is likely to reflect differences in unexplained effects of education on functional limitations. It could be misleading to interpret such variation as differences in overall effects of education when the variation could easily be induced by the gender and region-specific differences in the strength of mediator variables. For instance, if smoking explains the effects of education on health for men more than for women, the remaining effects of education could be higher for women than men.
Analyses
We calculated descriptive statistics on all variables and examined their distribution by gender and region and used assessment of the distribution of covariates and dependent variable to inform regression models in the next stage. We fitted negative binomial regression models to estimate the total average effect of educational attainment on functional limitations, adjusting for all covariates. We used negative binomial regression to accommodate the overdispersed nature (i.e., conditional variance > conditional mean) of functional limitation scores. The outcome of interest does not have the usual discrete count interpretation (in terms of number of failures, etc.), but the regression model provides a probability density function that offers a good fit to the distribution of functional limitations, which was positively skewed.
The first regression model assessed the overall effect of education for the total sample. The next two models examined gender differences by estimating the average effect of education on functional limitations separately for men and women. We used this same approach to examine the overall effects of education on functional limitations for each region and for men and women separately within each region. These stratified models are equivalent to models with all gender-covariate interaction terms for gender-stratified models and all region-covariate interaction terms for region-stratified models. We used two-way (gender*education) and three-way (Gender × Education × Region) interaction terms to test the statistical significance of the differences in the effects of education on functional limitations across gender and regions.
Results
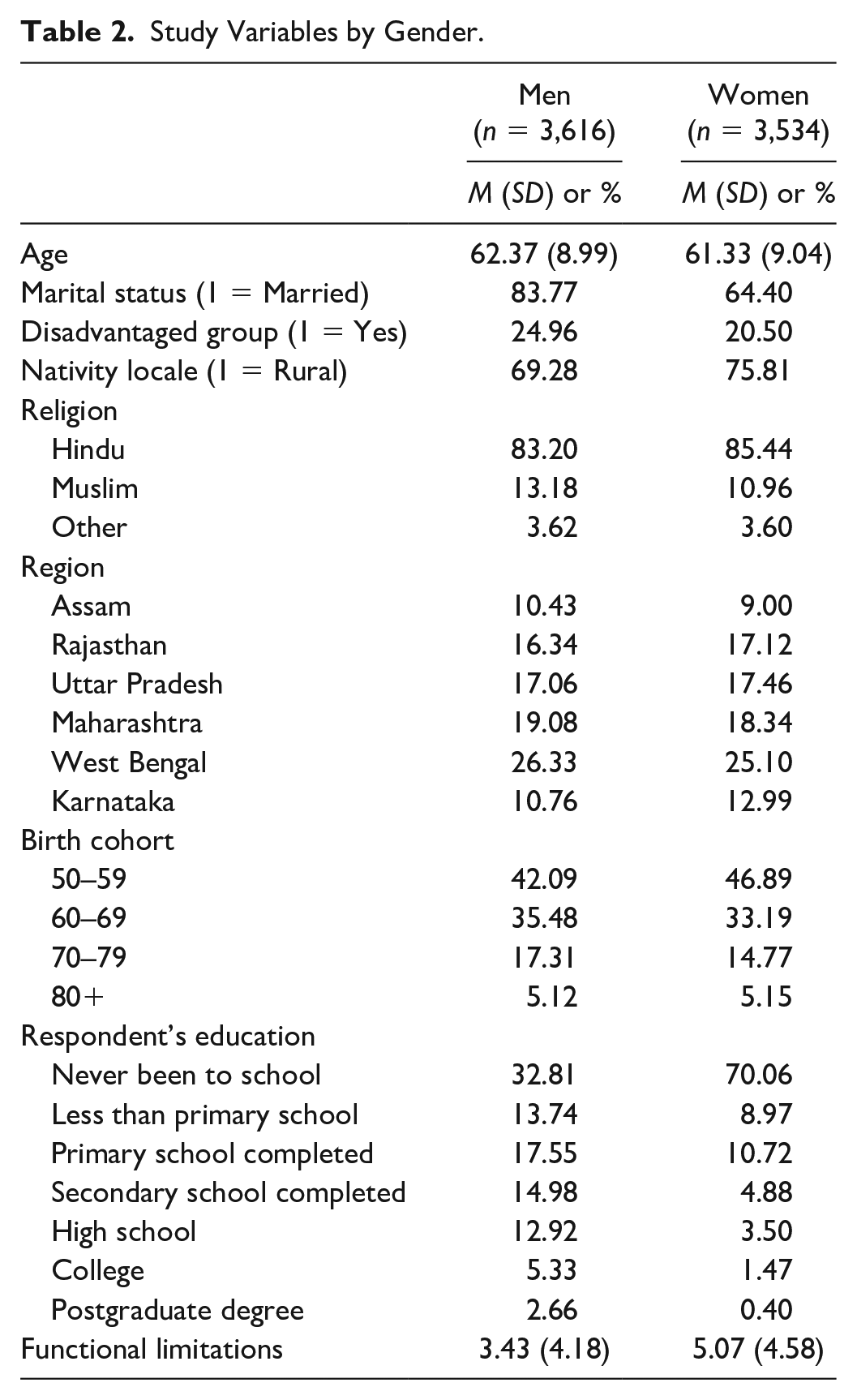
Men were significantly older than women (t = 4.85, p < .001) and represented a higher percentage of Scheduled Castes/Tribes, but they had lower rates of rural nativity (Table 2). Educational attainment among women was significantly lower (χ2 = 998.20, p < .001) than men. Fully 70% of women had no formal education, compared with 33% of men; only 5% of women (vs. 21% of men) had completed high school or beyond. Gender differences in education also varied by region. For example, 1.45% of women in Rajasthan and 1.21% in Uttar Pradesh had finished high school, compared with more than 6% in Assam, Maharashtra, West Bengal, and Karnataka (not shown in table). Older adults in Uttar Pradesh reported lower levels of functional limitations than those in the other regions (not shown in table). Functional limitations also varied by gender with women faring far worse (t = −15.07, p < .001) than men in all regions.
Study Variables by Gender.
Negative binomial regression coefficients assess the effects of education on functional limitations across gender (Table 3), and allow us to further examine regional differences in functional limitations after adjusting for covariates. In analyses of the total sample, educational attainment had negative effects on functional limitations. In gender-specific models, women benefited less from educational attainment than men. For instance, men gained an average 3% decline (exp −0.12) in functional limitations with each year of increase in education, compared with a 1% (exp −0.09) decline for women. As illustrated by the estimate for the two-way interaction term (Gender × Education) in the nonstratified model, the gender difference in the effects of education on functional limitations was statistically significant (β = .026, p < .001). Likewise, the estimate for gender shows its remaining influence on functional limitations—even after controlling for educational attainment, women report on average 40% (exp 0.34) higher functional limitations than men. After adjusting for variables such as educational attainment, functional limitations of both men and women in Uttar Pradesh remained lower than in the other regions.
Negative Binomial Regression Estimates of the Effects of Education on Functional Limitations by Gender.
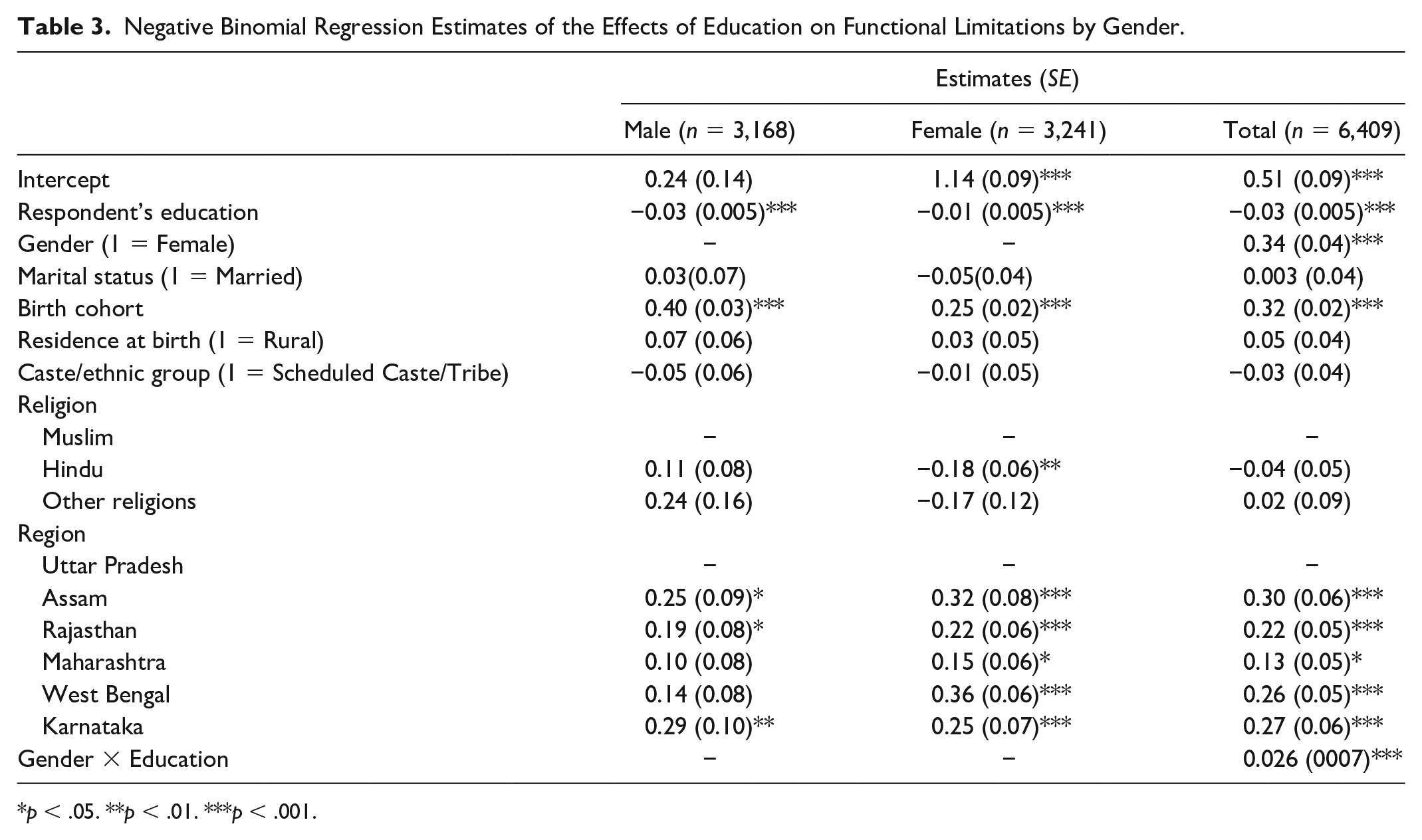
p < .05. **p < .01. ***p < .001.
Results presented in Table 4 (Panels A–F) extend our investigation of overall and gender-specific effects of education on functional limitations to regional dynamics. The overall effect of education on functional limitations varied by region. In Maharashtra, a 1-year increase in education was associated with an average 3% decline in total functional limitations, compared with a 2% decline in Rajasthan. Additional analysis using an interaction term (e.g., Region × Education) showed that the effect of education on functional limitations in Maharashtra was statistically not different (β = −.013, p = .27) than in Rajasthan (not shown in table).
Negative Binomial Regression Estimates (SE) of the Effect of Education on Functional Limitations by Gender and Region.
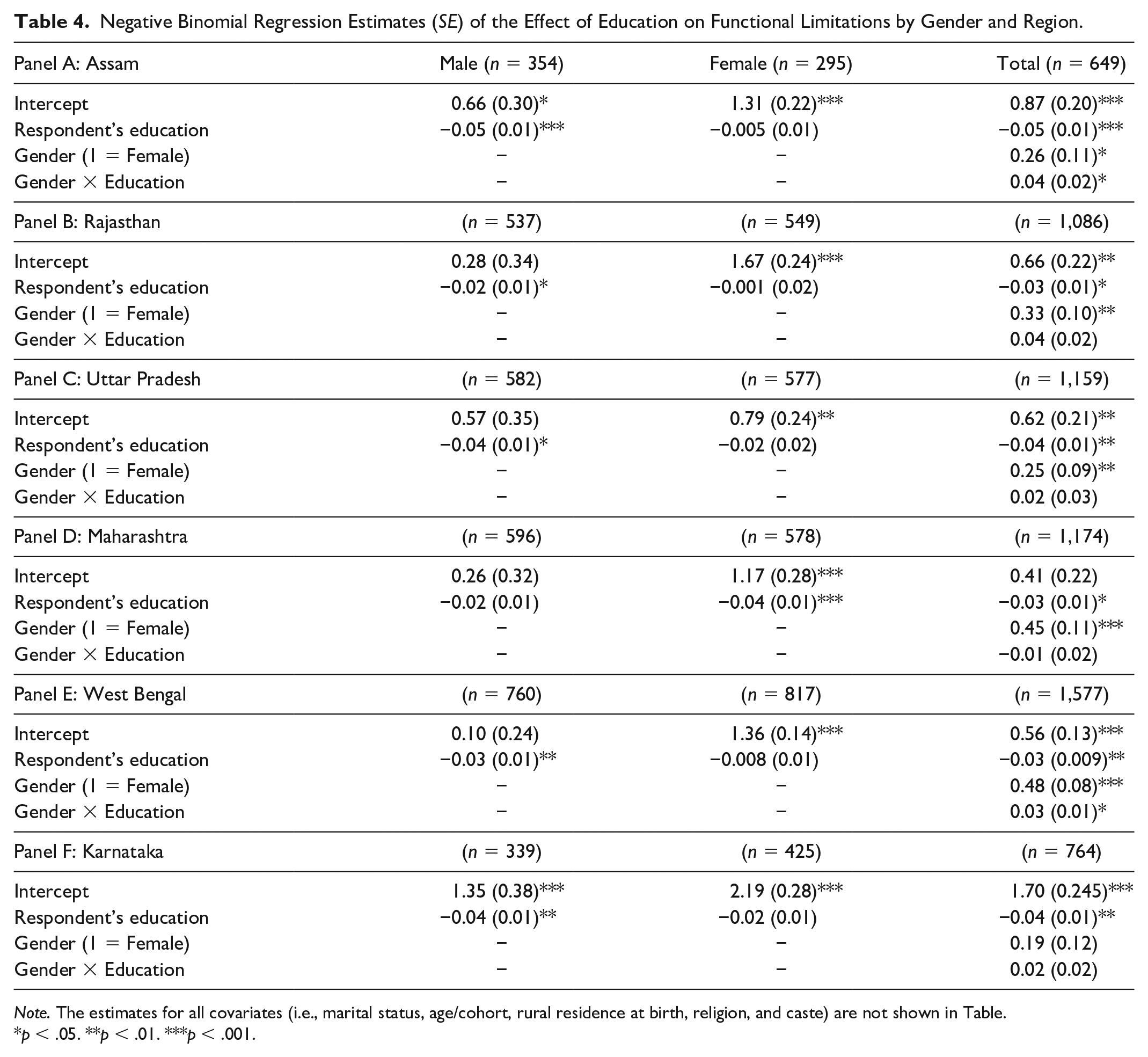
Note. The estimates for all covariates (i.e., marital status, age/cohort, rural residence at birth, religion, and caste) are not shown in Table.
p < .05. **p < .01. ***p < .001.
We also explored gender dynamics in the region-specific effects of education on functional limitations. As seen in Table 4, gender differences in the effects of education on functional limitations was statistically significant only for Assam (β = .04, p < .05) and West Bengal (β = .03, p < .05). In other words, the effect of education for women was significantly lower than for men only in these two states. For women, the negative effect of education on functional limitations was significant only in Maharashtra. Relative to women in Rajasthan, only the effect of education for women in Maharashtra was statistically different (β = −.04, p < .05) (not presented in Table). With the exception of Maharashtra, the influence of education on functional limitations was statistically significant for men across all regions. Although the influence of education for men in Rajasthan was lower than that for their counterparts in other regions, the differences in such effects across regions were not statistically different (not presented in table).
Discussion
This study used an intersectionality framework to investigate later life health disparities in a nationally representative sample of adults aged 50 and over in India. Specifically, we explored regional variations in the impact of gender-specific education-based inequities on functional limitations. Recognizing that deep-seated regional differences in gender norms and practices lead to variations in education and health outcomes for men and women, we reasoned that considering multiple social statuses simultaneously would permit a more fine-grained analysis of health disparities in later life.
Consistent with previous studies, we documented the positive total effect of education on functional health for men and women alike; but the influence was significantly greater for men than women. The statistical significance of gender in the effects of education on functional limitations held only in the states of West Bengal and Assam. Also reflecting regional differences in gender norms and practices, the influence of education on functional limitations for women varied by state and were significantly lower in Rajasthan than in Maharashtra.
Findings on regional disparities in functional limitations do not support our hypothesis and show an intriguing pattern that invites further exploration. Older adults in Uttar Pradesh reported fewer physical functional limitations than their age peers in other states. Other studies that did not use all regions included in SAGE also found lower functional limitations in states like Uttar Pradesh and Rajasthan (Kastor & Mohanty, 2016), as do studies using other national data (Bora & Saikia, 2015; Saikia et al., 2016). This finding is surprising because Uttar Pradesh is less economically and educationally advanced than states such as Maharashtra. Furthermore, older adults in the southeast (e.g., West Bengal and Karnataka) had higher educational attainment than those in the northwest (e.g., Uttar Pradesh and Rajasthan). An in-depth exploration of factors that account for such regional patterns is beyond the scope of this study, but they do resemble those reported by Sen (2002). He found the highest morbidity in Kerala (which has the highest literacy rate in the country at 94%) and the lowest morbidity in Bihar (which has the lowest literacy rate in the country at 64%). Literacy rates in Uttar Pradesh are lower than all other states in our study, except Rajasthan.
We also found that the associations of educational attainment and functional limitations varied by gender and region. Lack of resources available to less-educated older adults likely leads to more functional limitations in later life. This finding aligns with that of studies that show a socioeconomic gradient in functional limitations (Brinda et al., 2016; Goli et al., 2014; Nagarkar & Kashikar, 2016). Our hypothesis of wider educational differences in functional limitations in southern states was also not supported, as education-related gaps in functional limitations in socioeconomically privileged states such as Karnataka, Maharashtra, West Bengal, and Assam did not differ statistically from disadvantaged states such as Uttar Pradesh and Rajasthan.
Due to global structural changes, the more advantaged states of Karnataka, Maharashtra, and increasingly West Bengal and Assam have opened their spaces to global flows of capital, good and people—such as in Mumbai, Kolkata and Bangalore. Proliferation and intensification of these dynamics have transformed the core and periphery of these city spaces into indeterminate economic opportunities and communal formations (Holston & Appadurai, 1996). Imagined futures offer hope to disadvantaged people with low levels of education in these states and open spaces for formal and informal avenues for survival and coping with the challenges of functional impairments. Return on investment for the better educated is an ongoing challenge in the low opportunity structures of disadvantaged agrarian states of Uttar Pradesh and Rajasthan. On the other hand, kin-oriented agricultural practices that can be sustained with low levels of formal education in the states of Uttar Pradesh and Rajasthan allows for cohesive social support and prospects of better health. In addition, we note the study by Sen (2002) that suggests lower rates of morbidity in poorer states may be due to residents’ lack of knowledge about health and health care.
The effects of education on late-life functional limitations varied regionally only for women. There was a significantly wider education-related gap in functioning for women in Maharashtra than in Rajasthan. Although education had less influence on functional limitations for women than men in most states, this difference was statistically significant only in Assam and West Bengal, perhaps due to a mix of few opportunities for more educated women to gain high returns and, owing to their superior social position, current and cumulative advantages for men. There are also highly educated women who ascribe to traditional gender roles, idealizing characteristics of Bhadromohilas—mothers, wives, daughters of the English educated professional Bengali “middle class” men or Bhadroloks, for example, schoolmasters, lawyers, doctors, and government servants (Borthwick, 1984; Peacock, 2009). As Saikia (2011) explains, despite being educated, women’s prerogatives in Assam are offset by traditional gender norms. The cumulative effects of these norms may help explain low returns of education on functional limitations for women in West Bengal and Assam (see Duraisamy, 2002).
In closing, we note several limitations to this study. We experienced the usual limitations of secondary data, including reliance on available measures. The state of Kerala was not a study site; it would have enabled us to better understand how gender dynamics in education and health operate in highly literate, well-educated states. The cross-sectional nature of the data does not allow us to explore potential selective mortality, such that the influence of education on functional limitations could be biased. It is possible that chronic functional disability-to-mortality rates are higher among lower educated individuals generally, but even more so in states like Uttar Pradesh and Rajasthan. Consequently, higher mortality among less-educated older adults in those locales could mean narrower educational differences in functional limitations if study participants have better health profiles than those who are deceased.
Combining self-report and performance-based measurements can refine prognostic information on functioning, especially among older adults with high self-reported functioning—although not if there is ADL dependency (Reuben et al., 2004). Though it is not necessarily a limitation of the data, it is worth noting that the presence of very few individuals, especially women, with higher education in Uttar Pradesh and Rajasthan complicates comparisons of the effects of education across regions. Wider education-related differences in functional limitations in West Bengal could be due, for example, to a more highly educated general population. The education difference could only be observed between lower and higher levels of education, not between those with lower and primary levels of education.
Despite these limitations, this study advances theoretical and empirical knowledge on the long-range effects of complex intersectionalities on later life functional status. It represents a major step in using intersectionality as a theoretical and analytic framework for the study of late-life health disparities in the global South. The use of this model enabled us to detect additional disparities in later life functional limitations attributable to the intersecting effects of gender, education, and geography. It may be equally useful in moving future studies beyond looking at independent sources of heterogeneity on later life health outcomes. With growing attention to potentially mutable social determinants of health, this line of inquiry is especially important for developing policies and services that target the needs of older adults in low-resource settings with high rates of health-related disparities.
Footnotes
Author’s Note
Moushumi Roy is now affiliated with Delta College, University Center, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.