
Abstract
Fall prevention strategies informed by understanding sex differences in the perception of falls may be fruitful.
Introduction
Falls are prevalent among older people, and many older people express being moderately or very afraid of falling (Boyd & Stevens, 2009). Furthermore, falls are a major precursor of disability and death among older persons (Braun, 1998). While some older persons are receptive to fall prevention messaging and engaged in positive behaviors to prevent falls (Schepens et al., 2011), other older persons do not alter their behaviors or modify their home environment to prevent falls (Boyd & Stevens, 2009) and may not be receptive toward fall prevention messages (Hughes et al., 2008; Kruse et al., 2010). From the perspective of fall prevention messaging, studying sex differences in falls can be insightful. Specifically, uncovering the drivers behind sex differences related to fall perceptions enables fall prevention messages to be more gender relevant and potentially more effective. To our knowledge, currently there is no theoretical explanation for sex differences in the perceptions and behavioral tendencies related to falls. Furthermore, whereas higher risk for falls among women has been widely reported (e.g. Painter et al. (2009)), sex differences in perceptions toward falls, behavioral tendencies (e.g. restricting activities to prevent falls), and the underlying psychological mechanisms remain understudied, particularly in Asian cultures.
In the present study, we aimed to examine the effect of perceived susceptibility (as indicated by a recent fall episode) on gender stereotyping relating to falls to uncover the underlying mechanisms for sex differences in perceptions toward falls among older people. Sex presently refers to the biological classification of men or women according to reproductive organs. On the other hand, gender stereotyping presently refers to socially constructed belief and value systems that are used by people in the construction of gender identity, and gender stereotypes are traits that are considered typically feminine or masculine (Courtenay, 2000). For instance, men are perceived to be physically resilient and less vulnerable to injuries than women. Indeed, women are more vulnerable to falls than men (Painter et al., 2009) and perceive themselves to be at higher risk of falling than men (Hughes et al., 2008). In addition, men may underreport their challenges related to falling to preserve their masculine image (Chamberlin et al., 2005; Miller et al., 2001). Thus, it appears that sex differences in perceptions toward falls may be affected by gender stereotypic perceptions and one’s perceived susceptibility to falls. Below, we examine gender stereotyping related to falls and consider how it is affected by the perception about one’s tendency of falling and sustaining injuries from the fall (i.e. perceived susceptibility toward falls). Presumably, someone who has fallen before would perceive himself or herself to be more susceptible toward subsequent falls than someone who has never fallen.
Sex Difference in Falls and Fall Perceptions
Falls affect women and men differently. Gender analysis has been argued to be essential in understanding all aspects of health and can ultimately contribute to better healthcare policies and programming (Hartigan, 2001; Vlassoff & Moreno, 2002). Thus, gender analysis may reveal explanations for sex differences in fall perception. Currently, gender theories have been used to understand sex differences related to the psychological aspects of specific diseases such as screening for colorectal cancer (Farraye et al., 2004; Friedemann-Sánchez, et al., 2007), heart diseases (Jensen & Moser, 2008), and HIV (Bunting, 1996), but perceptions related to falls have not been subjected to gender analysis.
Previously, scholars questioned whether sex differences in terms of the reported fear of falling are a result of actual fear of falling or because of other psychosocial factors, such as stigma driven by gender stereotyping, that cause reluctance to admit having a fear of falling among men (Chamberlin et al., 2005; Miller et al., 2001). It has been suggested that the lower fear of falling among men relative to women may have stemmed from the stigma for expressing fear (Miller et al., 2001). Across different cultures, studies have found that men report higher self-efficacy related to falls (Hoang et al., 2017; Irez, 2014; Lawson & Gonzalez, 2014; Stel et al, 2004; Suzuki, 2002).
The stigma for expressing fear among men can be examined more closely through the lens of gender roles and social constructions of masculinity and how it is implicated in the perceptions of falls and fall-related beliefs. Gender roles and social constructions of masculinity can lead to lower awareness and motivation related to self-care, and well-being (Courtenay, 2000; Dean, 1989; Mansfield et al., 2003; Rothman & Salovey, 1997) because of the adherence to conventional masculine traits such as strength, toughness, and self-reliance among men (Courtenay, 2011). Such gender stereotyping is evident in Asian cultures. For instance, the gender ideal for Chinese men to suppress their emotions and exude toughness is exemplified by the philosophical phrases “男兒有淚不輕彈” (“nan er you lei bu qing dan,” i.e. “a man should not easily shed his tears”) and “大丈夫流血不流淚” (“da zhang fu liu xue bu liu lei,” i.e. “real men would rather bleed than weep”) (Yeung et al., 2015). This can be further understood in terms of men’s tendency to perceive lower susceptibility for health risks and fatalism about health outcomes (Courtenay, 2011), affecting how likely men will express their concerns regarding aspects of health they considered embarrassing, or endurable without complaints (Vlassoff & Moreno, 2002). As such, the observations that older men reported lower concerns toward falls and generally less concern about their health than women reflect a manifestation of such gender constructions.
Conversely, women appear to be at a greater risk for falls and that they tend to experience more deleterious consequences following falls. For instance, women compared to are more likely to fall and sustain fractures (Caban-Martinez et al., 2015; Stevens et al., 2006). Consequently, women are twice more likely to be hospitalized and admitted to the emergency department, although mortality associated with falls is disproportionately greater among men (Hendrie et al., 2003; Stevens & Sogolow, 2005). Furthermore, physical aspects such as deterioration in muscle and bone mass particularly among postmenopausal women put them at a greater disadvantage relating to falls. The perceived physical vulnerability among women extends to other aspects of health, such as perception of exercise risk (Cousins, 2000) and environmental health risk (Flynn et al., 1994), and may have similar effects on the psychological aspects of falls such as fall efficacy.
Falls efficacy is defined as a lasting concern about falling resulting in the avoidance or curtailment of activities an older person normally engaged in. Falls efficacy is related to multiple problems. For instance, lower falls efficacy may lead to less movement and poorer physical functioning (Chamberlin et al., 2005), and negatively affect a person’s psychosocial well-being because of reduced social interaction and lower quality of life (Walker & Howland, 1991). More specifically for tasks that require mobility, it is important to examine the older person’s perceived ability to complete the tasks without falling (Tinetti et al., 1994). Numerous studies found that women were more concern about falling than men (Boyd & Stevens, 2009; Chamberlin et al., 2005; Howland et al., 1998; Maki, 1997; Vellas et al., 1987). In addition, women are more likely than men to report falls and discuss with healthcare professionals regarding falls and fall prevention (Stevens et al., 2012). Relatedly, although women who fell resume prefall level of frequency for leisure and household activities more readily than men who fell, this might have resulted from the lower participation in physical activities initially and greater obligation to do housework among women (Stahl & Albert, 2015).
Effect of Perceived Susceptibility on Sex Differences in Fall Perceptions
Sex differences in perceptions of falls appear to emerge from sex differences in physical vulnerability related to falls. Men may express fewer concerns about falls and less negative fall perception than women because men tend to be less vulnerable to actual falls and the impact of falls (Stahl & Albert, 2015). Whereas physical vulnerability can explain causes and outcomes of falls, lifestyle habits additionally contribute to various aspects of falls. For instance, although muscular weakness predicts fall rates for both women and men (Moreland et al., 2004), women are less likely than men to exercise and relatedly have weaker lower body strength (CDC, 2014; Oman et al., 1999). This may have led to the higher fall incidence and slower recovery among older women. Thus, sex differences in perceptions toward falls could be explained by perceived susceptibility and severity relating to the consequences of falls.
The Current Study
The current study aims to explore the boundary of the theory on the construction of masculinity (Courtenay, 2000) and the influence on falls perception. In particular, part of the Health Belief Model (Janz & Becker, 1984) states that perceived susceptibility (i.e. having a recent fall) interacting with demographic variables (i.e. sex) impact perceived threat (e.g. perceived severity of the consequences of falls). Accordingly, we propose that the social construction of physical invulnerability among men would be eliminated by a recent fall, thereby equating men’s fall perception to a level similar to that of women. On the other hand, given that women tend to perceive that they are physically vulnerable regardless of their fall history, fall perception is less likely to differ between women who had a recent fall episode and women who did not compared with men. In the current study, we examine whether perceived susceptibility toward falls as indicated by a history of fall would affect sex stereotypic patterns in fall perception in terms of fall efficacy while engaging in daily activities such as taking a bath, perceived seriousness of falls and speed of recovery if the person falls (i.e. perceived effect of falls), and behavioral tendencies (i.e. restricting activities to prevent falls). In particular, we predict that although sex differences in fall perception would persist among nonfallers, the sex difference will be eliminated among recent fallers, given that the perceived susceptibility would be more pronounced because of a recent fall, thus equating perceptions toward falls between men and women. Thus, we hypothesize as follows: Among nonfallers, women will report lower fall efficacy than men. However, this sex difference will not be observed among fallers. Among nonfallers, women will report more negative effects for falls than men. However, this sex difference will not be observed among fallers. Among nonfallers, women will report a greater tendency to restrict activities to prevent falls than men. However, this sex difference will not be observed among fallers.
Methods
Design and Setting
The study described here was part of a larger cross-sectional study, National Fall Prevention Awareness, which aimed to examine the knowledge, attitudes, and practices of falls; fall-related risk factors; and fall prevention among community-dwelling older and middle-aged adults in Singapore. In the current analysis, we report sex differences relating to perceptions of falls among the older adults. Two thousand older adults 60 years and older and living in the community were initially solicited from a random sample of addresses in the central and northern regions of Singapore obtained from the Department of Statistics. A survey company was procured to recruit the older adults through door-to-door knocking over a period of four months, and those who were bedbound were excluded. Surveyors were trained by the research team and verified to be sufficiently qualified to conduct the interviews appropriately. Face-to-face interviews each lasting approximately 60 minutes were conducted with eligible older adults.
Participants
A final sample of 212 men (182 nonfallers and 30 fallers) and 337 women (262 nonfallers and 75 fallers) was attained. This group of participants was verified to be cognitively intact by means of the Abbreviated Mental Test (test score ≥ 7/10) (Jitapunkul et al., 1991), could answer the questionnaires without a proxy, and was independent in ambulation with or without aids.
Measures and Variables
Demographic Characteristics of Older Men and Women (n = 549).
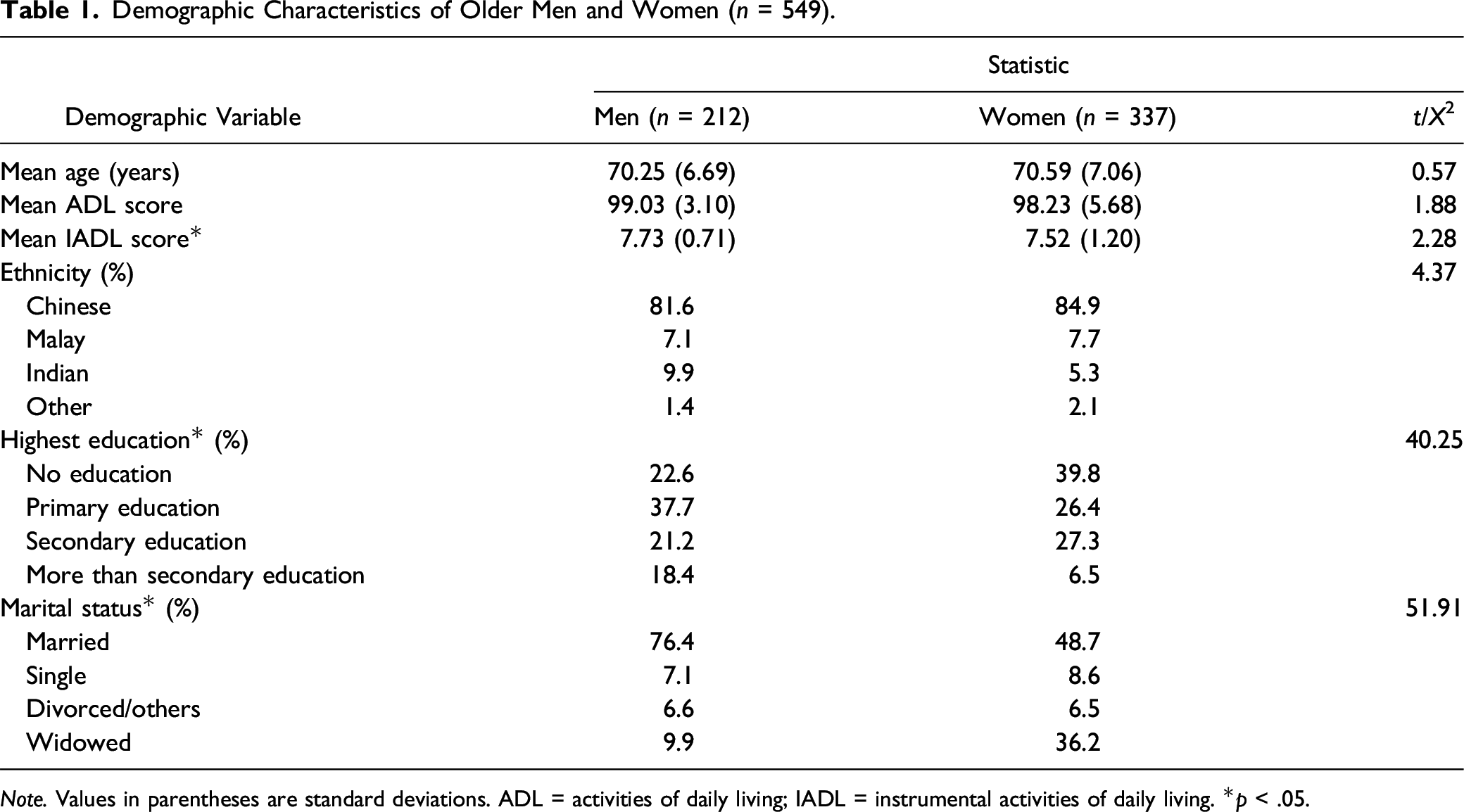
Note. Values in parentheses are standard deviations. ADL = activities of daily living; IADL = instrumental activities of daily living. *p < .05.
Recent fall episode
A recent fall episode was elicited by asking “Have you fallen in the past 12 months?” with binary responses, that is yes and no. A fall was defined “to have occurred when a person comes to rest unintentionally on the ground or lower level (Lamb et al., 2005),” with localization of threshold of same-level falls as 0.5 m or less (National Registry of Diseases Office Singapore, 2014).
Functional status
The participant physical functional statuses were established using the Barthel Activities of Daily Living (ADL, score range: 0–100) and Lawton Instrumental Activities of Daily Living (IADL, score range: 0–8). On the ADL scale, each of the 10 activities (e.g. feeding, bathing, grooming, and dressing) was scored on a 3-point scale, indicating independence (i.e. 10), need for assistance (i.e. 5), and total dependence (i.e. 0) (Mahoney & Barthel, 1965). On the IADL scale, each of the eight activities (e.g. ability to use telephone, shopping, food preparation, and housekeeping) was scored based on independence (i.e. 1) and dependence (i.e. 0) (Lawton & Brody, 1969).
Falls efficacy
To measure falls efficacy, we used the Fall Efficacy Scale—International version (FES-I, Yardley et al., 2006). The scale includes 16 items based on a 4-point scale, including (1) “not at all concerned,” (2) “somewhat concerned,” (3) “fairly concerned,” and (4) “very concerned” for engaging in activities such as cleaning the house, taking a bath or shower, and walking up or down a slope. A score for this measure was obtained by summing up the 16 items. Higher total scores indicate a lack of confidence in performing activities, that is lower fall efficacy. Cronbach’s alpha analysis showed an acceptable reliability, α = 0.94.
Perceived effects of falls
To elicit participants’ perceived effects following a fall episode, we asked the questions “If you fell, how likely would you be seriously injured? (e.g. fractures)” and “If you fell and were seriously injured, how likely would you return to your current living situation?” (Braun, 1998) based on a 6-point scale ranging from 0 “extremely unlikely” to 5 “extremely likely.” We excluded other items from the survey which were unrelated to the perceived severity of the consequences of falls. For this study, a score for this measure was obtained by summing up the first item with the reversed score of the second item. Higher scores indicate more negative perceived effect of falls. A Spearman–Brown analysis indicates moderate reliability, ρ = 0.35 (Eisinga et al., 2013).
Restriction of activities to prevent falls
To assess participants’ tendency to restrict activities, we asked the question “How important do you feel it is for you to restrict activities to prevent falls?” based on a 5-point scale ranging from 0 “not at all important,” through 2 “somewhat important,” to 4 “very important.” Higher scores indicate greater tendency to restrict activities to prevent falls.
Statistical Analysis
Comparisons of sociodemographics between older men and women were conducted using t-tests for continuous variables or contingency table analysis using the chi-square test for categorical variables. To test the physical vulnerability hypothesis that sex differences in perceptions for falls are observed to the extent that the individual did not have a recent fall episode, we conducted a simple effects analysis for fall efficacy, perceived effects of falls, and restriction of activities to prevent falls as the dependent variable. Cronbach’s alpha was used to examine reliability for the FES-I, and Spearman–Brown was used to examine the 2-item measure for the perceived effects of falls (Eisinga et al., 2013). For the analyses mentioned, p-values <.05 were considered statistically significant. All analyses were conducted using SPSS, version 23.0, statistical software for Windows.
Results
Our sample included 212 older men (182 nonfallers and 30 fallers) and 337 older women (262 nonfallers and 75 fallers) and mirrored the national distribution for ethnicity (i.e. Chinese, Malay, and Indian), marital status (i.e. married or single), and highest education level for adults 60 years and older (see Table 1). A chi-square test of independence showed that there was no significant association between sex and ethnicity, whereas there was a significant association between sex and education level where more men attained higher education than women and a significant association between sex and marital status where more men were married, whereas more women were widowed. There were no sex differences in terms of age and ADL score, whereas men reported slightly higher IADL score than women. The following presents findings for the main effect for sex and history of falls, followed by a focus on the simple effects for sex among fallers and nonfallers.
Main Effect for Sex and History of Falls
We observed a marginal significant main effect for sex for fall efficacy [F(1,535) = 2.890, p = .09, ηp2 = .005] but not perceived effects of falls [F(1,535) = 1.518, p = .22] and restriction of activities to prevent falls [F(1,535) = 2.274, p = .13]. In general, women (27.06 ± 0.63) reported lower falls efficacy than men (25.08 ± 0.95). We observed a significant main effect for history of falls for falls efficacy [F(1,535) = 8.576, p < .01, ηp2 = .016] but not perceived effects of falls [F(1,535) = 0.003, p = .95] and restriction of activities to prevent falls [F(1,535) = 0.006, p = .94]. In particular, older adults with a recent fall (27.73 ± 1.03) reported lower falls efficacy than those who did not (24.41 ± 0.46).
Simple Effects for Sex and History of Falls
Means (M), Adjusted Means (Madj), SDs, and SEs for Participants’ Perceptions toward Falls in Relation to Sex (n = 549). The Sample Includes 182 Nonfallers and 30 Fallers among Older Men, and 262 Nonfallers and 75 Fallers among Older Women.
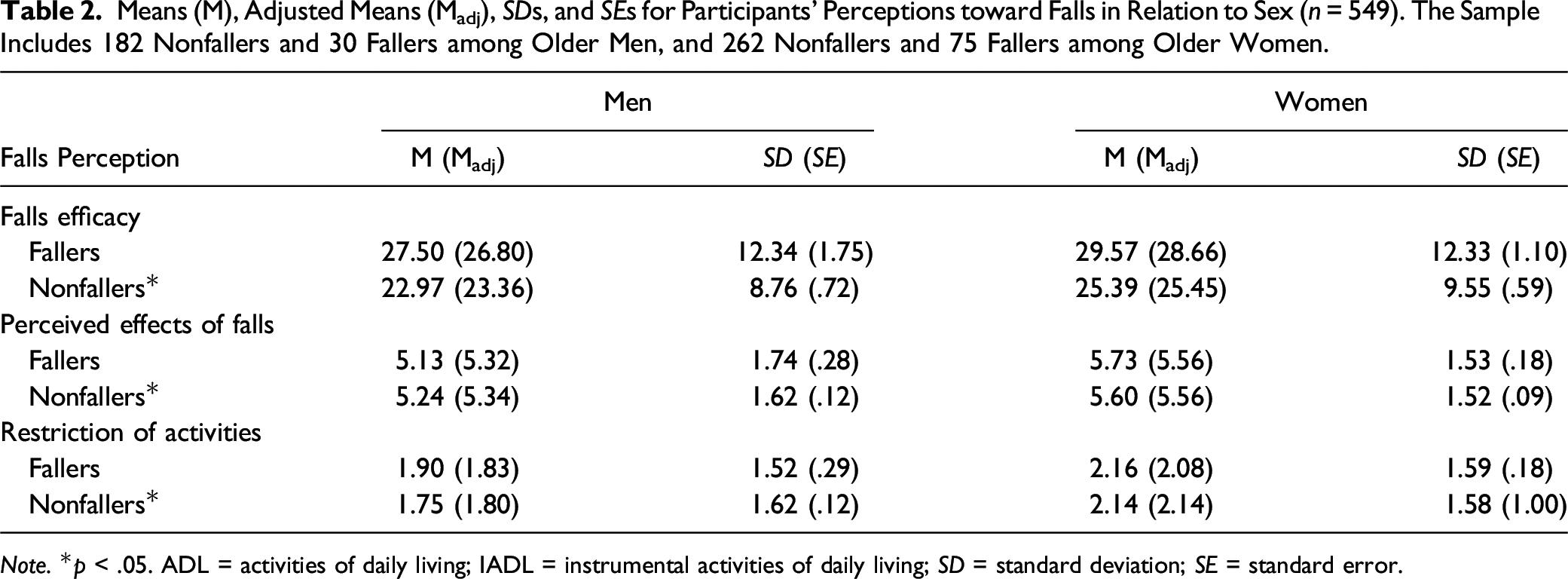
Note. *p < .05. ADL = activities of daily living; IADL = instrumental activities of daily living; SD = standard deviation; SE = standard error.
Discussion
The present study examined the notion of perceived susceptibility toward falls within the gender stereotype frameworks in explaining sex differences in perceptions toward falls. We found that women reported lower fall efficacy. Extending on the literature, we also found that women perceived more negative effect for falls and greater tendency to restrict activities to prevent falls. Supporting the present hypotheses, these sex differences were not observed among those who fell in the last 12 months. This observation is consistent with extant fall literature and is in agreement with the broader literature on sex differences in health and social beliefs. Broadly, the current findings suggest that sex differences in perceptions toward falls may be constrained to nonfallers.
Implications Related to Sex Differences in Perceptions toward Falls
Given that the current findings suggest that older men who fall experience lower fall efficacy and may reduce their physical activities, providing a general fall prevention message may not be adequate in changing concerns and behaviors pertaining to falls. As such, health messaging targeting men and women may need to be structured differently among those who have fallen before and those who have not fallen. For instance, raising concerns about falls among older male nonfallers may reduce their sense of physical invulnerability toward falls. In addition, it may be fruitful to target perceived susceptibility toward falls in the context of aging, given that older people appear to be sensitive toward psychological and behavioral aspects of falls, such as balance confidence and activity restriction respectively.
Sex Differences in Perceptions across Health and Social Domains
The present research suggests that sex differences in fall perception differ between fallers and nonfallers. Previous research on falls considered sex mainly as a moderating factor and acknowledged the contribution of sex toward falls (Stahl & Albert, 2015; Stevens & Sogolow, 2005). However, past research did not elucidate how sex effects emerge across domains related to falls and fall prevention. The present conceptual framework sheds light on the pathways through which sex affects fall perception, and this notion can be extended to understand other outcomes related to falls such as knowledge, attitude, and practices related to fall prevention. This understanding will enable practitioners and scholars to develop appropriate programs aimed at ameliorating psychosocial problems related to falls and preventing falls.
It is noteworthy that the current findings mirror the western population in terms of greater fear of falling and lower fall efficacy among women than men (e.g. Greenberg et al. (2016)), indicating that this observation is culturally invariant, and may have emerged from fundamental differences between men and women, such as perceived and actual physical susceptibility. The present findings also shed light on extant health and social care literature which suggests that men tend to be apathetic toward personal care. Previously described as the “white male effect,” health risks were perceived as lower among white men relative to women and people of color, depending on the sociopolitical context a person lives in (Finucane at al., 2000; Flynn et al., 1994). Taking all into consideration, sex differences in perceptions toward falls may have roots in perceived susceptibility but are nevertheless attenuated by a recent fall episode as reported in the current study. As such, understanding sex differences in fall perception can be better informed with reference to an individual’s history of fall.
Limitations and Future Directions
Given that the present study was a cross-sectional study and the effect sizes for sex differences among nonfallers were regarded small, we were unable to ascertain if a fall episode would lead to within-person changes in perceptions related to falls. In addition, sample sizes between men (N = 212) and women (N = 337) were different, the sample size for fallers (N = 105) was relatively small compared with that for nonfallers (N = 444), and activity restriction was measured by a single item. As such, prospective studies, including larger and more balanced subgroups (i.e. sex and fall history) and expanding items measuring activity restriction may provide further support to the present conceptualization that fall perception would be altered by perceived susceptibility. Furthermore, our findings indicate that sex differences were observed among people who did not fall. Among people who fell, it remains unclear whether concerns were accentuated among men or attenuated among women. Nonetheless, it would be unlikely that women who fell would experience lower concerns than women who did not fall.
Presumably, the present participants had more autonomy in their lives, given that they were living in the community. As such, this group of participants may perceive their physical vulnerability differently compared with individuals living in institutionalized settings such as nursing homes. Future studies that compare older adults living in the community with those in institutions or tertiary health settings can provide deeper insights relating to sex differences in perceptions toward falls.
Conclusion
Using gender analysis, the present study reveals the potential psychological phenomenon relating to fall perception. Importantly, we found that other than falls efficacy, a similar pattern in sex difference was also observed for fall-related beliefs and behavioral tendencies. As many governments now focus on health promotion through preventive measures, our findings serve important considerations for health promotion among pre- and postfall ambulant older adults. In addition, the current findings suggest that sex differences in fall perceptions in an Asian culture are similar to Western cultures. As such, sex differences in fall perceptions may be more strongly implicated in biological factors such as physical susceptibility, over and above culturally driven factors such as gender stereotyping.
Footnotes
Acknowledgment
We thank Dr Chan Yiong Huak for his advice on the statistical analysis during our revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Geriatric Education and Research Institute Intramural Grant (grant number: GERI1607) and the Centre for Ageing Research and Education, Duke-NUS.