
Abstract
A plethora of research examines the link between pain and sleep problems (e.g., having short, poor, or disrupted sleep), two major health concerns in later life that often co-occur (Eslami et al., 2016; Finan et al., 2013; Mathias et al., 2018). Scholars have tracked sleep in patients with chronic pain longitudinally (e.g., Ødegård et al., 2015; Jansson Fröjmark & Boersma, 2011), manipulated pain and sleep in the laboratory (e.g., Irwin et al., 2012; Kundermann et al., 2008; Tiede et al., 2010), and assessed pain and sleep experiences as they occur in daily life (Bromberg et al., 2012; Edwards et al., 2008). This study adds to the growing interest in understanding mechanisms underlying the link between daily reports of pain and sleep. We assessed specific sleep disturbance symptoms at night (e.g., waking up too early or too often) that may be related to inadequate or poor-quality sleep.
The key purpose of this study was to identify social factors that may attenuate the link between older adults’ pain and sleep disturbances. Theorists emphasize the study of pain in social contexts (Craig, 2015) such that some studies have documented the detrimental effect of interpersonal rejection and tensions on pain (e.g., Fuentecilla et al., 2019; Kross et al., 2011). However, surprisingly little is known about whether older adults’ positive encounters, a commonly examined buffer in times of stress (whose literature could be traced back to Cohen & Hoberman (1983)), may moderate the link between pain and sleep. Filling this gap will add to the literature and provide new insights into health-promotion interventions that aim to benefit older adults with pain or sleep problems.
Pain and Sleep Disturbances
The literature on associations between pain and sleep largely comprises prospective and experimental studies (Smith & Haythornthwaite 2004; Stocks et al., 2018). Prospective studies generally examine clinical samples (e.g., patients with acute burn injury, chronic pain, fibromyalgia, and cancer) and track changes in sleep and pain severity over time (Jansson-Fröjmark & Boersma, 2012; O’Brien et al., 2011; Smith et al., 2008). Experimental studies, in contrast, focus on sleep deprivation in healthy adults and test sensitivity to pain stimuli in the laboratory (Irwin et al., 2012; Kundermann et al., 2008; Tiede et al., 2010).
A growing literature examines pain and sleep using daily diaries, which may reduce retrospective biases and reflect more immediate health consequences in naturalistic settings (Hassan, 2006). These daily studies have primarily examined either sleep duration or general measures of sleep quality (Edwards et al., 2008; Lewandowski et al., 2010; Tang et al., 2012). The current study aimed to expand these sleep measures by examining specific symptoms individuals experienced during the night related to short or poor-quality sleep, such as having trouble falling asleep or waking up too early and too often.
We considered the link between pain and sleep disturbances in both directions. Many studies support Moldofsky’s (2001) argument that pain and sleep problems are reciprocally related, creating a vicious cycle. More recent data, however, suggest that sleep problems are a stronger predictor of pain than pain is of sleep (Finan et al., 2013). In this study, we tested bidirectional associations by asking whether older adults with more severe pain during the day would report more sleep disturbances at night, which would in turn exacerbate their next day feelings of pain.
Positive Encounters as a Buffer
We further examined whether these bidirectional links vary depending on older adults’ daily positive encounters. Several theoretical perspectives have discussed the buffering effect of positive encounters, many of which focus on the role of positive emotions that are elicited from social encounters. According to the dynamic affect model, positive emotions attenuate negative emotional responses when individuals incur chronic stress or encounter acute daily stressors (Leger et al., 2019; Ong et al., 2006; Zautra et al., 2005, 2001). In addition, the broaden-and-build theory states that positive emotions expand individuals’ thoughts and build key resources (e.g., relationships, knowledge, and skills) that may protect individuals’ psychological (e.g., depressive symptoms) and physiological well-being (e.g., cardiovascular system, immune system, and Hypothalamic-Pituitary-Adrenal stress response system; Fredrickson, 2013; Sin et al., 2017, 2015). These health outcomes are closely associated with pain and sleep in later life (Finan et al., 2013), but little research has incorporated positive encounters in the pain and sleep literature. This study asked whether the links between pain and nighttime sleep disturbances would be weaker on days when older adults have more positive encounters.
Close Partners and Nonclose Partners
Older adults prioritize encounters with close partners, but they also interact with people they feel less close to (e.g., extended family relatives and acquaintances) or do not know well (e.g., strangers). We assessed positive encounters with both close partners and nonclose partners and expected the buffering effect to be especially salient with close partners. Positive encounters likely strengthen social ties, among which close ties have a greater impact on older adults’ well-being than weak/peripheral ties (Antonucci et al., 2014; Charles & Carstensen, 2010). These close ties are also more likely to constitute the primary sources of support that older adults have (i.e., perceived support; Cohen & Wills, 1985; Uchino, 2009) when they encounter stressful experiences such as pain or sleep disturbances.
Current Study
The current study examined the bidirectional associations between daily pain and nighttime sleep disturbances in a nonclinical community-dwelling older population. We tested how pain is associated with specific sleep disturbances older adults incur at night and also how these disturbances influence older adults’ next day feelings of pain. We also asked whether older adults’ positive encounters moderate (attenuate) these links. We then compared positive encounters with close partners versus nonclose partners.
We adjusted for additional factors associated with pain and sleep, including age, gender, education, marital status, ethnic/racial group, overall pain, the number of health conditions, and depressive symptoms. Pain and sleep problems both become more prevalent with age (Finan et al., 2013; Nahin, 2015). Women tend to report more severe pain and greater sensitivity to pain than men (Fillingim et al., 2009; Hirsh et al., 2006). Less-educated individuals experience more pain than highly educated individuals (Poleshuck & Green, 2008; Schmidt et al., 2007), and married or cohabitated individuals are less likely to experience pain (Taylor et al., 2013). Individuals identified as racial/ethnic minorities (e.g., Black or Hispanic) tend to report more pain than their white counterparts (Green et al., 2003). Individuals who report greater overall pain are also more likely to report pain on a daily basis. Additionally, pain and sleep are related to a number of medical conditions and to depression, so we adjusted for the number of health conditions and depressive symptoms (Boakye et al., 2016; Patel et al., 2013).
Methods
Participants and Procedures
This study drew on data from the Daily Experiences and Well-being Study (DEWS). The University of Texas at Austin Institutional Review Board approved all procedures (#: 2015-02-0123), and participants provided informed consent. The DEWS recruited 333 community-dwelling adults aged 65+ years (65–92, M age = 74.15, SD = 6.57) residing in the greater Austin, Texas, metropolitan area in 2016–2017. Participants were retired (e.g., worked fewer than 20 hours per week) and came from a full spectrum of socioeconomic backgrounds. We oversampled male and minority participants to obtain a diverse sample.
Participants first completed a 2-hour face-to-face interview in their homes or a nearby place of choice. During the interview, participants reported their demographic characteristics and completed assessments of their social networks. Social network information was then used to customize ecological momentary assessments run on the ilumivu platform (ilumivu, Inc. www.ilumivu.com) preinstalled on study-provided Android devices. Participants received training before completing these assessments for 4–6 days (to capture at least two weekdays and two weekend days). The number of days varied across participants because interviewers scheduled to collect the Android devices at the convenience of participants, who could still complete assessments prior to the pickup day. Ecological momentary assessments included a number of brief surveys each day. Participants rated their prior night sleep in the first assessment of the day, which was set to pop up at participants’ self-reported typical wake-up time (e.g., 8:00a.m.). Then, every 3 hours throughout the day, participants indicated their pain and encounters with social partners until their self-reported bedtime (e.g., 10:30p.m.). Participants received $50 for the initial interview and another $100 for the daily data collection.
Descriptive Information of Participants (n = 292)

In-Person Interview Measures
Close partners
Participants listed their social partners using the three concentric convoy circles (Antonucci & Akiyama, 1987). Participants provided the first name and last initial of (a) people they feel so close to that it is hard to imagine life without them, (b) people they may not feel quite that close to, but who are still very important to them, and (c) people they have not already mentioned but who are close enough and important enough in their lives that these people should also be included in the diagram. Each participant had 15 social partners on average, and we considered the top 10 of them as close partners in this study. Nonclose partners were identified when participants indicated their social encounters throughout the day (elaborated in the Ecological Momentary Assessment Measures section below).
Background characteristics
Participants reported their age, gender as 1 (male) or 0 (female), and marital status recoded as 1 (married/cohabitating) or 0 (not married). Participants indicated their education level as 1 (no formal education), 2 (elementary school), 3 (some high school), 4 (high school), 5 (some college/vocation or trade school), 6 (college graduate), 7 (post college but no additional degree), and 8 (advanced degree). Participants revealed ethnic/racial identities, from which we generated three dummy variables indicating (a) non-Hispanic African American, (b) Hispanic/Latinx American, and (c) other race (e.g., Asian/Alaskan Native). Non-Hispanic white was used as the reference group.
Participants reported how much bodily pain they experienced during the past 4 weeks, on a scale ranging from 0 (no pain) to 10 (severe pain; Ware & Sherbourne, 1992). Participants also indicated by either 1 (yes) or 0 (no), whether a doctor had ever told them that they had any of the following health problems based on a list from the Health and Retirement Study: (a) high blood pressure or hypertension, (b) diabetes or high blood sugar, (c) cancer or a malignant tumor (excluding minor skin cancer), (d) chronic lung disease such as chronic bronchitis or emphysema, (e) heart problems (e.g., heart attack, coronary heart disease, angina, or congestive heart failure), (f) stroke, (g) arthritis or rheumatism, and (h) osteoporosis or osteopenia (Wallace & Herzog, 1995). We assessed the total number of health conditions each participant had. We measured participants’ depressive symptoms using the shortened Center for Epidemiologic Studies Depression Scale (CES-D; Gellis, 2010). Participants were asked how often they have felt each of the 11 items (e.g., depressed, lonely, or restless sleep) during the past week. Responses were coded as 0 (rarely or none of the time), 1 (some of a little of the time), 2 (occasionally or a moderate amount of the time), or 3 (most or all of the time). Two positively valenced items (i.e., enjoyed life and happy) were reverse coded, and items were summed (α = .78).
Ecological Momentary Assessment Measures
Pain
Every 3 hours throughout the day, participants rated how much pain or discomfort they experienced during the prior 3 hours coded as 0 (no pain), 1 (mild pain), 2 (moderate pain), and 3 (severe pain; Stewart, 1992). We calculated a mean score of pain ratings across each day for each participant.
Positive encounters
Every 3 hours, participants indicated whether they had interacted with close partners and nonclose partners, either in person or via phone or text. Responses were coded as 1 (yes) or 0 (no). Again, close partners referred to the top 10 people participants listed in their convoy measures (whose first full name and last initial were transferred from the in-person interview to the ecological momentary assessments). Nonclose partners were anyone not listed as the top 10 closest partners; they included extended relatives, friends, acquaintances, service providers, and strangers. If an encounter occurred, participants were asked to rate how pleasant each encounter was on a scale from 1 (unpleasant), 2 (a little unpleasant), 3 (neutral), 4 (a little pleasant), and 5 (pleasant; Zhaoyang et al., 2018). We calculated two sets of variables to examine older adults’ positive encounters with close partners and with nonclose partners (2 types of partners × 2 metrics = 4 variables). We first assessed the proportion of encounters with close partners that was at least a little pleasant (i.e., a value of 4 or 5 on the original scale), and the proportion of encounters with nonclose partners that was at least a little pleasant. Second, we measured the average pleasantness of encounters with close partners and the average pleasantness of encounters with nonclose partners. We also generated two variables to measure the proportion of positive encounters with anyone (combining close and nonclose partners) and the mean pleasantness of encounters with anyone. For the analyses, we first examined positive encounters with anyone and then compared between close and nonclose partners.
Start of Day Survey Measures
Sleep disturbances
Upon waking up, participants reported whether they had any sleep disturbances the prior night. We used five validated items adapted from the Midlife in the United States (Ryff et al., 2007) and Pittsburgh Sleep Quality Index (Buysse et al., 1989). Participants indicated whether they: (a) had trouble falling asleep, (b) woke up during the night and had difficulty getting back to sleep, (c) woke up too early this morning and had difficulty getting back to sleep, (d) worried about anything or thought about problems while trying to sleep, and (e) had pain or discomfort that disrupted their sleep. Responses were coded as 1 (yes) or 0 (no). We generated a sum score for each participant’s sleep disturbances each night.
Statistical Analyses
Consistent with other research using ecological momentary assessments (Shiffman et al., 2008), participants sometimes missed a survey during the day. Thus, we had unequal numbers of surveys on different days and estimated multilevel models using SAS 9.4 (Statistical Analysis System). All models adjusted for participant age, gender, education, marital status, racial/ethnic group, overall pain, number of health conditions, and depressive symptoms. We centered all continuous covariates on the sample means.
We first examined how older adults’ pain during the day was associated with their sleep disturbances at night. We estimated two two-level linear models (SAS PROC MIXED) considering the day level (level 1) nested within the participant level (level 2) to examine this link in two directions. In the model with sleep disturbances as the outcome, the predictor was older adults’ pain averaged across 3-hour assessments within each day. In the model predicting next-day pain as the outcome, we treated sleep disturbances the prior night as the predictor.
We then tested whether older adults’ positive encounters attenuated the bidirectional links between older adults’ pain and sleep disturbances at night. We added interaction terms to the two-level linear models using SAS PROC MIXED, as described above. We examined the moderating role of (a) the proportion of positive encounters and (b) the average pleasantness of encounters. In all models, variables included in the interaction terms were mean centered. We conducted simple slope analysis for significant interactions.
Close partners and nonclose partners
We then reestimated the moderation tests above; but this time, we examined positive encounters with close partners and with nonclose partners separately. These two moderators were entered into the same model.
Results
Table 1 presents descriptive information regarding participants’ pain, sleep, and positive encounters with social partners. The majority of participants (95%, n = 274) did not report severe pain in any of the daily assessments, with 63% (n = 183) reporting mild or moderate pain and 32% (n = 91) reporting no pain at all. Older adults reported no pain across 63% of 3-hour assessments, mild pain across 28% of assessments, moderate pain across 8% of assessments, and severe pain across 1% of assessments. With regard to sleep at night, older adults on average reported about one sleep disturbance each day (M = .88), with only 33% of participants (n = 90) not reporting any sleep disturbance at all.
Most social encounters throughout the days (85%) were considered as at least a little pleasant, with 86% of encounters with close partners at least a little pleasant and 83% of the encounters with nonclose partners at least a little pleasant. On average, encounters were highly pleasant, with the mean ranging from 4.55 to 4.68 (4 = a little pleasant and 5 = pleasant).
Hypothesis Testing
Multilevel Model Predicting Pain from Sleep Disturbances the Prior Night.

Note. Participants n = 292. B = unstandardized beta; SE = standard error; VAR = variance. p < .05. **p < .01. ***p < .001.
We also explored whether older adults’ positive encounters moderated the bidirectional links between pain and sleep disturbances at night. We did not find any interaction effects on the link of pain predicting same day nighttime sleep and do not present the null findings here.
Multilevel Linear Models Predicting Participants’ Feelings of Pain from Prior Night Sleep Disturbances.
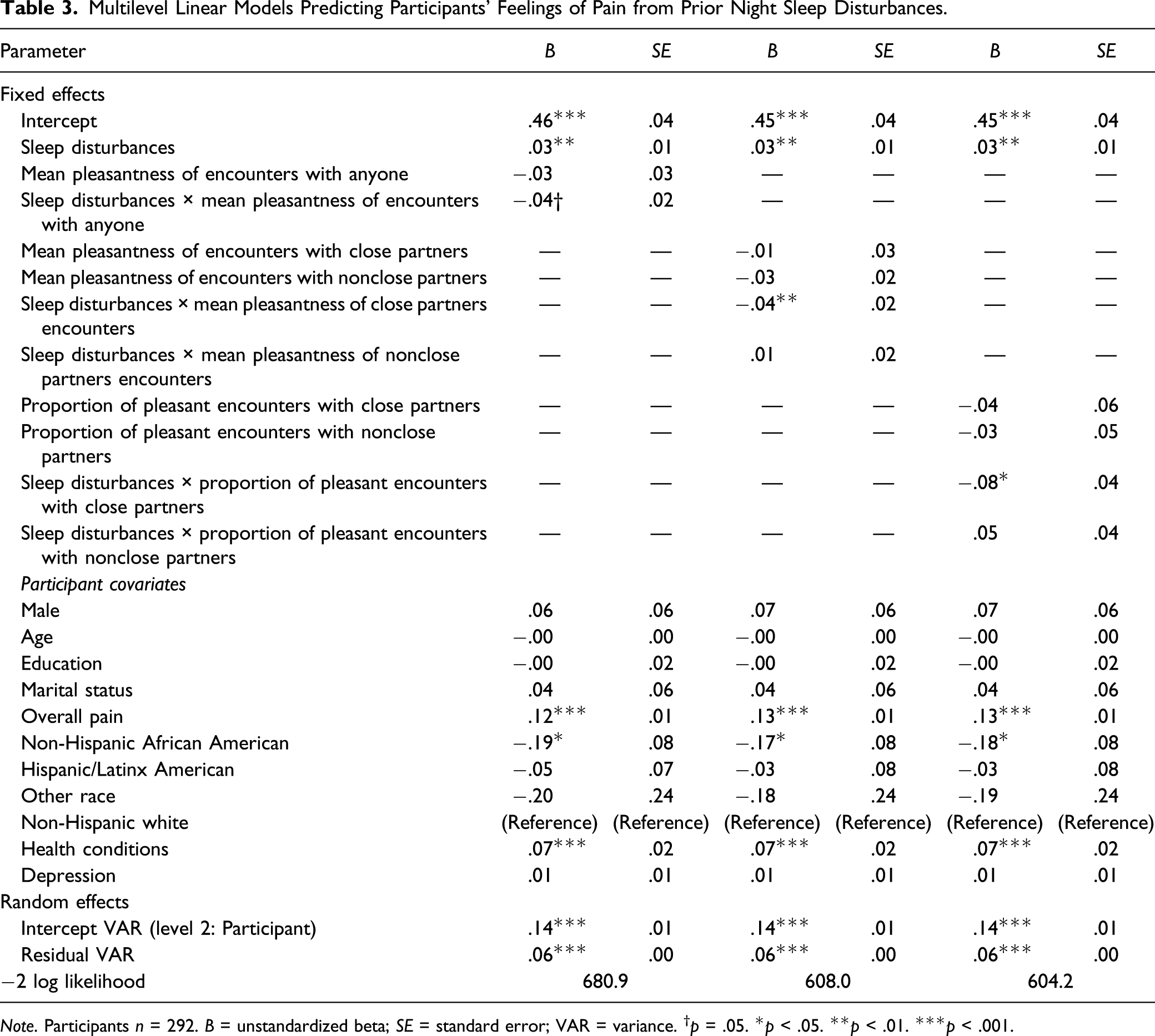
Note. Participants n = 292. B = unstandardized beta; SE = standard error; VAR = variance. †p = .05. *p < .05. **p < .01. ***p < .001.
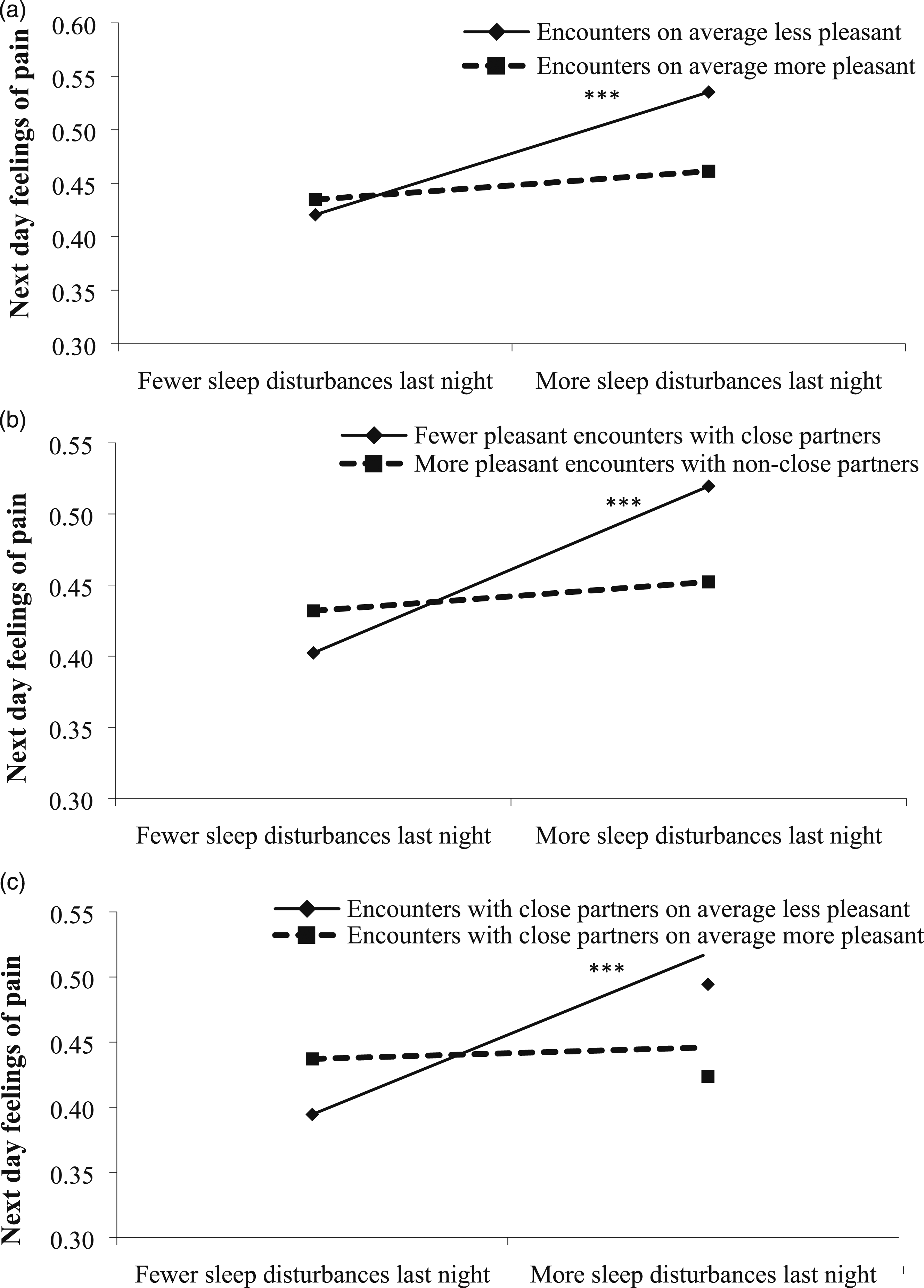
Interaction effect of sleep disturbances × (a) mean pleasantness, (b) proportion of pleasant encounters with close partners, and (c) mean pleasantness of encounters with close partners, on next day feelings of pain.
Close partners and nonclose partners
When examining close partners and nonclose partners separately, we only found significant interactions involving positive encounters with close partners, both for the proportion of these encounters (B = −.08, p = .03) and for the mean pleasantness of these encounters (B = −.04, p = .008), see Table 3. Simple slope analyses revealed that prior night sleep disturbances predicted more severe pain the next day on days when older adults had a smaller proportion of pleasant encounters with close partners (B = .05, p < .001) but not on days when they had a greater proportion of these encounters (B = .01, p = .41; see Figure 1(b)). Likewise, the sleep–pain association was only significant on days when older adults viewed encounters with close partners as less pleasant (B = .05, p < .001) but not on days when they viewed these encounters as more pleasant (B = .00, p = .78; see Figure 1(c)). We did not find significant interaction effects involving positive encounters with nonclose partners, and thus do not present these findings in details: proportion of encounters (B = .05, p = .23) and mean pleasantness (B = .01, p = .45).
Sensitivity Analyses
We also ran several sets of additional sensitivity analyses. We reestimated our models twice, first excluding participants (a) who reported no pain in the past month during the initial interview (n = 49, 17%; the analytic sample n = 243) and then excluding those (b) who reported no pain in any of the ecological momentary assessment during the study week (n = 94, 32%; the analytic sample n = 198). Findings remained the same as those reported above.
We also tested each sleep disturbance symptom separately and observed a similar pattern of findings, with one exception. In the main results, we did not find a significant link between pain and the total number of same day sleep disturbances that night. Yet, older adults who experienced more severe pain during the day were more likely to report that their sleep was disrupted by pain or discomfort (odds ratio = 1.73, p = .04). Thus, we regenerated a new sum score of sleep disturbances, excluding the pain-related sleep disturbance. Findings using the new sleep measure remained the same as the main results.
Last, we considered the maximum level and variability of pain reports within each day. These two metrics of pain reports were not associated with older adults’ nighttime sleep, and interaction effects were likewise not significant. Findings are available upon request.
Discussion
This study examined pain and sleep disturbances in older adults’ everyday lives and the potential buffering effects of positive encounters for these associations. We found prior night sleep disturbances were associated with older adults’ next day feelings of pain. Yet, this effect varied depending on older adults’ positive encounters during the day, especially those with close partners. It is also interesting to note that prior night sleep and social encounters seem to only influence older adults’ overall state of the day (i.e., averaged feelings of pain), rather than their most extreme pain report anytime that day or the variability of pain within the day. Findings emphasize the importance of positive social encounters in pain and sleep research and may hopefully inspire future studies to understand ways to alleviate older adults’ pain from a social perspective. This study may offer new insights into the development of health promotion interventions targeting older adults who experience pain or sleep concerns.
Pain and Sleep Disturbances
We found that older adults who incurred more sleep disturbances the prior night reported more severe pain the next day but not vice versa. Findings offer evidence that sleep problems precede feelings of pain (Finan et al., 2013) and suggest the key role that sleep interventions may play for older adults with pain. Some research has also found that pain impairs sleep quality. However, these studies examined individuals who had chronic pain disorders (Kelly et al., 2011; Mathias et al., 2018). Given that our findings are from a nonclinical sample, our findings provide insights into how the cycle of pain and sleep observed in pain patients may have started. That is, this cycle may start with poor sleep impacting pain. Poor sleep may also result in other health problems that co-occur with pain, consistent with findings documenting sleep issues as a mechanism underlying long-term pain and other well-being outcomes (e.g., depression; Campbell et al., 2013; Finan et al., 2013; Moldofsky, 2001).
Older adults’ daily pain did not impact their nighttime sleep. The only exception occurred when we looked at specific sleep disturbance symptoms. In these single-item analyses, we found that older adults with more severe pain were more likely to report pain- or discomfort-related sleep disruptions at night. It is worth noting that the majority of our participants did not report severe pain; as such, their feelings of pain may not be salient enough to cause other sleep problems. To better understand the link between pain and sleep, researchers may consider collecting more detailed reports from participants on the reasons why they have trouble falling asleep or wake up too often during the night. Future research may also examine a wider range of pain severity and explore whether there is a threshold above which older adults’ pain will be severe enough to have an impact on their sleep.
Positive Encounters as a Buffer
Our findings add to the burgeoning interest in the social context of pain (Craig, 2015; Hadjistavropoulos et al., 2011) and identified positive encounters as a potential buffer for the effect of prior night sleep on next day pain. Research has increasingly documented the buffering effect of positive encounters on individuals’ emotional mood and diurnal cortisol rhythms in the face of acute and chronic stressors (Bostock et al., 2011; Hong et al., 2020; Leger et al., 2019). The current study extends this work by showing that the sleep–pain link was less evident on days when older adults had a greater proportion of positive social encounters or viewed encounters as more pleasant.
As hypothesized, the buffering effect of positive encounters only applied when these encounters occurred with close partners. Perhaps, positive encounters with close partners help retain close ties, which are especially important in later life (Charles & Carstensen, 2010). Older adults prioritize close ties over novel ties, and these close ties have been shown to reduce daily somatic symptoms including pain (Stadler et al., 2012). Positive encounters with close partners may contribute to older adults’ perception of support availability (i.e., having someone to count on during problematic situations; Gleason & Iida, 2015), which has also proved to reduce experiences of pain (Keefe et al., 2003; López-Martínez et al., 2008). Further, given the correlational nature of this study, it is possible that on days when participants had poorer sleep and greater pain, they were less likely to seek out close partners or experience pleasant encounters with these partners.
It is worth noting that positive encounters seem to primarily benefit older adults when they are under more severe stress (i.e., had more sleep disturbances the prior night) but not when they reported better sleep. Indeed, when older adults had fewer sleep disturbances the prior night, they appeared to report slightly more severe pain on days with more positive encounters. This seemingly paradoxical finding has also been documented in previous studies (Cohen & Hoberman, 1983; Riskind et al., 2013). Future research may better understand this finding with a further investigation on the content of positive encounters. One possibility is that older adults may receive support during encounters, which typically increases closeness but reduces their well-being (Gleason et al., 2008). These encounters may be pleasant, but the support receipt per se may exacerbate their pain (Boothby et al., 2004; McCracken, 2005). In contrast, when older adults have more sleep disturbances (i.e., exposed to greater stress), according to the contingent exchange model (Davey & Eggebeen, 1998), they may find it more acceptable and rewarding to receive care (Huo et al., 2018).
Limitations and Conclusions
Some limitations to this study warrant consideration. We did not collect detailed data on the severity, type (acute vs. chronic), and cause of participants’ pain. As for sleep, we measured participants’ sleep on a daily basis but did not include an assessment of their overall sleep quality or disturbances over a longer period of time (e.g., in the past month). This study is also limited because we relied solely on subjective sleep reports, which have been shown to yield different findings from objective accelerometer measures (Lunde et al., 2010). Additionally, we did not assess medication use to examine its effect on sleep or pain, which could have influenced their symptoms. Further, although we tested bidirectional links, this study was still correlational in nature. No causal relationships could be conferred.
Despite these limitations, the current study adds to the growing literature regarding the complex relationship between sleep and pain in older adults’ everyday lives. We tested the bidirectional links between these two major health concerns, and we identified social factors that might attenuate these links. This study drew on a community-dwelling older adult sample and provides suggestive evidence for the importance of positive encounters among older adults with preclinical levels of pain. Sleep disturbances exacerbate older adults’ next day feelings of pain, necessitating the development of therapies and interventions that may break this link. This study offers additional support for the power of close ties for the health and well-being of older adults (Charles & Carstensen, 2010). Our findings may be of modest clinical significance, but they create the foundation for future research on pain in a social context and point out the promising role positive encounters play in benefiting older adults in the real world. Therapies and interventions involving family and friends are necessary and probably even more effective than those that focus only on levels of social activity. Perhaps, interventions with dyadic programs including older adults in pain and their close social partners will be most effective for increasing the quality of daily life among those with pain symptoms.
Footnotes
Author Contributions
M. Huo designed the study, performed statistical analyses, and wrote as well as revised the manuscript. Y. T. Ng, J. L. Fuentecilla, K. Leger, and S. T. Charles assisted in conceptualizing the study and rewriting drafts of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Institute on Aging [R01AG046460] and the Eunice Kennedy Shriver National Institute of Child Health and Human Development [P2CHD042849].