
Abstract
Keywords
Introduction
Positive family environments have lifelong implications for people’s well-being. Considerable work has documented that parental support, intact family structure, and financial stability during childhood predict better health in adulthood (Gilman et al., 2003; Larson & Halfon, 2013; Meadows et al., 2006). In recent years, researchers have documented that this protective effect lasts long into adulthood. For example, adults growing up with close family relationships and in two-parent families tend to have better physical health, lower depressive symptoms, and fewer chronic conditions than those who did not (Andersson, 2016; Chen & Harris, 2019; Chopik & Edelstein, 2019; Ferraro et al., 2016; O’Rand & Hamil-Luker, 2005). While the role of positive childhood experiences on people’s overall health is well documented, much less is known about their impact on cognitive health at older ages. Here, we build on prior work to examine how positive childhood experiences protect later cognitive functioning.
Research on late life cognitive function has expanded in recent years, as more individuals face a higher lifetime risk of poor cognitive function and neurodegenerative diseases with greater longevity. Alzheimer’s disease, for example, is already the sixth leading cause of death in the United States (Alzheimer’s Association, 2016), and the social and economic burden of dementia has increased from $18 billion in 1993 to $200 billion in 2010 (Hurd et al., 2013). Prior work has identified adult socioeconomic status, social relationships, and health conditions as key risk factors for cognitive function in later life (Dale et al., 2018). An increasing number of studies have also linked early life factors to later cognition, but they have primarily focused on childhood SES and health as key indicators (Luo & Waite, 2005; Lyu & Burr, 2016; Marden et al., 2017; Zhang et al., 2016). The current study extends prior work to investigate the extent to which childhood family social environment, together with childhood socioeconomic status (SES) and health, contribute to healthy cognitive function in later life.
Background
Childhood Experiences, Adult Resources, and Cognitive Health
Cognitive function rapidly develops in the early years, rises to a peak at maturity, and gradually declines with age (Kuh, 2007). Given this age-related pattern of brain growth and development, researchers and policy makers have applied the life course perspective to inform intervention efforts. Life course theory posits that early life experiences may contribute to cognitive health through direct and indirect processes.
Childhood experiences and exposures may directly influence later cognitive function, as early childhood circumstances become “embodied” to affect later health (Hertzman, 1999). Most research linking early life experiences to later cognition has focused on how experiences of low financial well-being during childhood lower later cognitive function. Using the Health and Retirement Study, Luo and Waite (2005) showed that older adults who grew up with parents with less than 8 years of school have lower levels of cognitive function than those who did not. Nutritional deprivation and poverty, likewise, appear to have negative long-term effects (Barnes et al., 2012; Hale, 2017). Research also shows that early experiences shape the progression of cognitive decline; cognitive function across multiple domains drops most precipitously over a 12-year period for those growing up in disadvantaged homes (Lyu & Burr, 2016). The effect of childhood SES in these studies often remained significant irrespective of adult experiences, suggesting that growing up in a socioeconomically unstable family may exert long-term influences on cognitive health in later adulthood.
Although parental education and family economic resources are important inputs to health in adulthood, other features of the childhood family, overlapping with, yet distinct from household income and education, may play an important role. We are interested in two family factors, childhood family-life happiness and family structure, as indicators of early life family social well-being. As shown in Figure 1, we conceptualize that cognitive function at older ages is affected by childhood experiences, characterized by childhood family social and financial well-being (i.e., family-life happiness, family structure, and family SES) through adulthood resources. Conceptual Framework: Childhood Experiences, Adulthood Resources, and Cognitive Function in Older Adults.
Several pathways link childhood family to late life cognitive function. Though these developmental pathways cannot be explicitly tested in this study, they form the basis of our initial hypothesis. First, research in neuroscience suggests that exposure to positive emotions such as happiness may increase the brain activity in the prefrontal cortex, the brain region responsible for memory function during childhood (Schwartz & Davidson, 1997). Early brain activity and structure are found to carry over into adult cognitive function (Wang et al., 2013), providing a potential mechanism through which family social well-being may have enduring effects on cognitive health. Second, family social well-being may influence brain and cognitive development by promoting ongoing opportunities for learning and social interactions (Rogoff, 1990). For example, responsive parenting, verbal openness, and emotional support in two-parent families promote mental stimulation and related process that are ideal for cognitive development (Carlson & Corcoran, 2001). Exposure to adult language and conversation with multiple parents can also benefit cognitive maturity through language and reasoning development (Lewis & Lamb, 2003; Romeo et al., 2018). Other research has shown that children who are raised with lack of parental care tend to have enlarged amygdale in adulthood (Lyons-Ruth et al., 2016). Despite ready evidence of family social well-being on early brain development, it is unknown whether such benefits last into later adulthood. Given the extensive line of literature on positive family experiences and cognitive function, we expect to find the following:
Early life experiences and exposures can also indirectly impact cognitive health through adult resource and opportunity pathways (Ferraro & Schafer, 2017; Ferraro & Shippee, 2009). Ferraro et al. (2016) argue that “early disadvantage increases the likelihood of exposure to later risks—but resources help individuals respond to those negative exposures” (p. 109). Education is one such adult resource with important implications for lifelong cognitive health. Indeed, the cognitive reserve’s perspective (Stern, 2009) suggests that education builds more efficient brain networks and helps people adapt to brain pathology and retain cognitive function. Childhood conditions correlate with education, and individuals from high SES and stable families (two-parent families) tend to have higher adult education than those from disadvantaged backgrounds (Luo & Waite, 2005; Monserud & Elder, 2011). Previous research also suggests that supportive parenting and a nurturing family environment promote educational attainment (Melby et al., 2008; Robertson & Reynolds, 2010). Education provides access to mentally demanding occupations, and this stimulation can promote neuronal resources that preserve cognitive function (Fisher et al., 2014).
Early life experiences may also contribute to the development of multiple resources throughout the life course, especially psychosocial assets that promote cognitive health. Growing up in a nurturing, supportive family environment provides strong social attachments and fosters emotional competencies (Batcho et al., 2011; Kaufman, 2019), the factors which can help become and remain socially connected as they age. Social connectedness is a critical resource for cognitive aging because relationships impose cognitive demands and promote mental stimulation. Indeed, older adults with large networks, diverse social ties, and greater social contacts and participation have better cognitive function than those who are socially disconnected (Kelly et al., 2017; Lee & Ang, 2019). Positive childhood experiences may also promote sense of meaning in their lives and strengthen the ability to manage goals, behaviors, and problems (Biglan et al., 2012). Sense of control (self-mastery), the belief that one can master, control, and shape their own life, for example, is found to confer cognitive benefits by helping individuals interfere with reaching goals and cope with stress and strain (Soederberg Miller & Lachman, 2000). Good physical health is yet another adult resource that protects cognitive function (Dale et al., 2018), and early life experiences are known to influence health through a variety of mechanisms, including educational attainment, social connectedness, and self-mastery (Ferraro et al., 2016; Luo & Waite, 2005).
Many studies on this topic examine education, but very little research examines the possibility that social connectedness and sense of control, together with physical health status, mediate the relationship between childhood experiences and later cognitive health. To the extent that positive early life conditions increase the acquisition of key resources across the life course, we hypothesize the following:
Data and Methods
We used data from Wave 3 of the National Social Life, Health, and Aging Project (NSHAP; 2015/2016), a nationally representative longitudinal survey of US older adults. Initial face-to-face interviews occurred in 2005/2006 (including 3005 community-dwelling individuals aged 57–85 years), with subsequent waves fielded every 5 years (O’Muircheartaigh et al., 2014). NSHAP is, to our knowledge, one of the only population-based studies that include information on childhood and family social environment, social network characteristics, and cognitive functioning in older age. NSHAP first asked about childhood background in Wave 2’s leave-behind questionnaire (LBQ) and continued to collect this information when a refresher sample of baby boomers (born 1948–1965) entered the survey in 2015/2016. On average, 85% of respondents in Wave 2 and Wave 3 returned their LBQ. We used Wave 3 because it is the most recent round of data collection with the largest sample. This maximizes statistical power and minimizes the potential attrition problems for individuals with cognitive impairment at earlier waves. Our analytic sample was restricted to age-eligible Wave 3 respondents (aged 50 or older) who completed the NSHAP-LBQ and cognitive functioning test and was further reduced due to item-response missing data ranging from .25% (race/ethnicity) to 20.36% (childhood living arrangement), yielding an analytic sample of 3361.
Measures
Dependent variable
We measured cognitive function using an adapted Montreal Cognitive Assessment (MoCA). The MoCA was developed as a cognitive screening tool for use in clinical settings (Nasreddine et al., 2005). After extensive pilot testing, the NSHAP team developed an 18-item MoCA-SA for use by field workers during in-home, face-to-face interviews. The 18 items of MoCA-SA are as follows: (1) Orientation: date and month (2 points total); (2) Executive function: abstraction—similarity of watch and ruler (1 point)—modified Trails-b (1 point); (3) Visuospatial skills: clock—contour, numbers, and hands (3 points total); (4) Memory: 5-word delayed recall (5 points); (5) Attention: forward digits (1 point), backward digits (1 point), subtract 7 s (3 points); and (6) Language: naming rhinoceros (1 point), phonemic fluency—words with the letter “F” (1 point for >10 words in 60 seconds)—and sentence repetition (1 point) (e.g., see Kotwal et al., 2015; Shega et al., 2014 for more detailed information on this measure). Since NSHAP is a probability-based nonclinical research sample, MoCA-SA scores were then transformed into full MoCA scores using the following validated equation: MoCA = (1.14*MoCA-SA) + 6.83 (Lindau et al., 2018; Shega et al., 2014). MoCA scores range from 0–30, with higher scores indicating better cognition.
Childhood experiences
Childhood measures included childhood family-life happiness, family structure, and family SES. First, following the previous work, (Batcho et al., 2011; Bellis et al., 2013), we assessed childhood family-life happiness by using an item in NSHAP-LBQ that asked respondents to report how much they agreed with the statement: “when I was growing up, my family life was always happy” with a 6-point scale ranging from 1 (disagree very much) to 6 (agree very much). Respondents who reported that their family life was always “very much happy” and “pretty much happy” were compared to those whose family life was “a little” happy or those who disagreed to the statement about their childhood family being happy. Preliminary analyses with the original coding of childhood family-life happiness did not alter our overall findings.
The childhood family structure (corresponding to age 6–16 years) was grouped into two categories: an intact family with both parents and a nonintact family (reference). We assessed childhood family SES using respondents’ report on both parents’ educational attainment and financial well-being of their childhood family. Father’s and mother’s education were asked in a question, “what is the highest grade of school your father/mother completed?” Possible answers included 1 (no formal education), 2 (1–11 grades), 3 (high school graduate), 4 (13–15 some college), 5 (college graduate), and 6 (postcollege). Following the previous work (Andersson, 2016), we took the maximum value of parents’ level of education when both were reported and used either value when one was missing. NSHAP assessed respondents’ financial well-being during childhood in a question, “during the time from about age 6 to 16 years, would you say your family was very well-off financially, fairly well-off, about average, not so well-off, or not well-off at all?” with a 5-point scale ranging from 1 (very well-off financially) to 5 (not well-off at all). We reverse-coded the answers so that higher scores indicate better financial well-being. To create continuity among the three family SES items, we standardized and averaged the responses (mean = 0, SD = 1).
Adult resources
Four types of adult resources were measured: education, social connectedness, self-mastery, and self-rated health. We measured education by assessing respondents’ educational attainment with four categories: less than high school (reference), high school diploma, some college, and college or more.
NSHAP assessed respondents’ social networks using a name generator technique in the network roster. Respondents were asked to list the people with whom they discussed important matters (up to five people) and, if a spouse or partner did not appear on this initial list, they were asked about their partnership status. Spouses or partners were then added to the network roster. Following the previous work (Cornwell & Waite, 2009; Schafer, 2018), we created a Social Connectedness Index by standardizing and averaging the following items (alpha = .67): (1) core network size; (2) network range, which indicates the extent to which the respondent is connected to a distinctive type of individual (e.g., spouse, friend, and co-worker); (3) proportion of core network members who live in the household (reverse-scored); (4) frequency of contact with network members which indicates an individual’s exposure to his network members; (5) number of friends; (6) frequency of volunteering; (7) frequency of attending meetings of an organized group; and (8) frequency of interacting with friends and family. This measure of social connectedness has been validated in previous work (Cornwell & Waite, 2009; Schafer, 2018).
The self-mastery scale used in this study is a modified version of Cohen’s 4-item Perceived Stress Scale designed to capture individual appraisals of life events as controllable and overwhelming. Following the previous work (Karraker, 2014; Shiovitz-Ezra et al., 2009), self-mastery was measured using four items that asked respondents about, in the past week, (1) whether they were unable to control important things, (2) whether they felt difficulties are piling up so they could not overcome them, (3) whether they felt confident about their ability to handle personal problems, and (4) whether they felt things were going their way, using a 4-point Likert scale which ranged from 1 (rarely) to 4 (most of the time). The responses were reverse-coded and averaged (alpha = .60). This measure of self-mastery has been validated in previous work (Karraker, 2014; Shiovitz-Ezra et al., 2009).
Last, self-rated physical health was assessed using the question of “would you say your health is excellent, very good, good, fair, or poor?” Respondents who reported that their health is “excellent,” “very good,” and “good” were (=1) compared to those who reported “fair” or “poor” health (=0).
Covariates
All models included demographic covariates including age in years, gender (1 = female), and race/ethnicity in four categories, non-Hispanic white (reference), non-Hispanic Black, Hispanic, and other. Following the previous work (Lee, 2019; Luo & Waite, 2005; Zhang et al., 2016), we also controlled for childhood health, as it is closely related to later cognition, using the question: “from age 6 to 16 years, would you say that your health during that time was excellent, very good, good, fair, or poor?” Respondents who reported that they had “fair” or “poor” health were compared to those whose health was “excellent,” “very good,” or “good.”
Analytic Strategy
Weighted Sample Characteristics, National Social Life, Health and Aging Project, 2015/2016 (N = 3361).

Note. Values in parentheses are standard deviations of means.
Regression Estimates of the Associations of Childhood Experiences, Adult Education and Psychosocial Resources, and Cognitive Function, NSHAP, 2015/2016 (N = 3361).

Note. NH = non-Hispanic, ref. = reference. † p < .10; * p < .05; ** p < .01; *** p < .001. Values in parentheses are standard errors.
Preliminary analyses included employment statuses (e.g., working, retired, and unemployed) as part of adult achievements, but it did not affect the overall results nor explained the association between childhood experiences and cognition (results from the mediation analysis are not shown, available upon request), so we excluded it from the final model. In addition, evidence indicates that the effects of childhood experiences on cognitive function may differ by race (Zhang et al., 2016), but preliminary analyses found no significant interaction terms between childhood experience variables and race/ethnicity, so we did not stratify the final models by race/ethnicity.
Decomposition of the Effect of Childhood Family-life happiness on Cognitive Function, NSHAP, 2015/2016 (N = 3366).
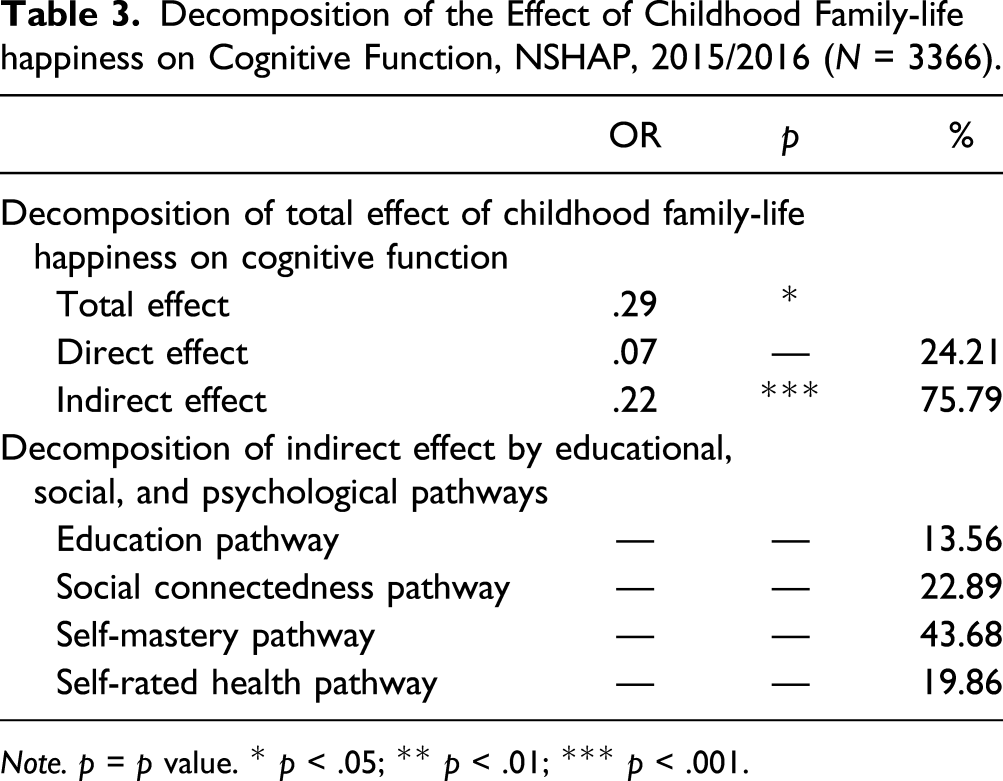
Note. p = p value. * p < .05; ** p < .01; *** p < .001.
Results
Table 1 presents sample characteristics of key variables. The average score of MoCA for cognitive functioning was 24.25 (SD = 3.72) on a 30-point scale. A sizable amount of respondents reported they had a very happy or happy family life during childhood (62.68%). The majority of respondents grew up with two parents (83.78%). Almost 70% of respondents attended some college or more. Sense of control was positively skewed, with the vast majority of respondents indicating that they had high mastery over their circumstances (mean = 3.33, SD = .65, range = 1–4). Additional analyses show that respondents who reported they had a very happy or happy family tend to report they had higher SES and lived with two parents during childhood. Childhood family SES was also related to family structure; intact families had a .39 mean value for childhood SES, while nonintact families had a .32 mean value for childhood SES. Respondents who reported a very happy or happy family during childhood also tend to report higher educational attainment, social connectedness, self-mastery, and better health than those who grew up in less happy homes. Demographically, most respondents were white (78.88%) and 54% were women.
Next, we turn to results from a series of nested models that test our hypotheses. Consistent with Hypothesis 1, we found in Model 1 that high levels of family social and financial well-being were positively and significantly associated with cognitive functioning. Specifically, those who grew up in a happy family had cognitive scores .29 units higher than those in less happy homes (p < .05). Similarly, those from high SES families had cognitive scores 2.56 units higher than those from low SES families (p < .001). This corresponds to about 9% change in the outcome variable. We also found that, though marginally significant, growing up in an intact family with two parents is also positively associated with better cognitive functioning (b = .30, p < .10).
When we introduced educational attainment in Model 2, we found the association between childhood family-life happiness and cognitive functioning, which was attenuated by 13% but remained statistically significant (b = .25, p < .05). However, the association of childhood SES with cognitive functioning became statistically insignificant after adding education in Model 2, suggesting, as others have found, that accumulation of socioeconomic resources in adulthood may compensate for the early financial disadvantage. Consistent with previous research, education was a strong predictor of later cognition, with increases in educational attainment associated with better cognitive functioning.
Finally, the coefficient for childhood family-life happiness was substantially attenuated and became insignificant when we added social connectedness and self-mastery (Model 3). Both social connectedness and self-mastery were strongly and positively associated with cognitive functioning (b = .57 and .70, respectively, both p < .001). When self-rated health was introduced into Model 4, the coefficient for childhood family-life happiness barely changed, from .09 to .07 (n.s.).
Overall, Models 2–4 suggest that the quality of family life during childhood may be an important predictor for cognitive functioning in old age, but works in large part through its influence on the achievement of adulthood resources, especially psychosocial resources. In Table 3, we conducted a formal mediation test to decompose the relative importance of the direct and indirect pathways between childhood family-life happiness and cognitive functioning (upper panel) and to estimate which pathways (adult education, social connectedness, self-mastery, and self-rated health) play the greatest role in mediating the association (lower panel). Results from the upper panel show that the majority of the total effect is, in fact, explained by the indirect, rather than direct, effect of childhood family-life happiness on cognitive functioning. Almost 76% of the association is explained by adult resources. And the lower panel confirms that, of those indirect effects, 44% were explained by the self-mastery pathway. The social connectedness pathway explains 23% of the indirect effect, while the rest is explained by the educational and health pathways.
Discussion
The current study had two goals. One was to examine whether childhood family social environment is, along with childhood SES, associated with later cognitive function. The second was to investigate how adult education, psychosocial resources, and physical health explain the association between childhood experiences and later cognition. We hypothesized that growing up in a socially and financially enriched family environment is positively associated with cognitive health in later life and that these childhood advantages work, in part, through their effects on adult resources.
We found partial evidence supporting our hypotheses. First, childhood family-life happiness (i.e., growing up in a happy family) and SES significantly predicted older adult cognitive functioning. Second, part of the effect of childhood family SES on cognitive functioning occurred through education. Third, the relationship between childhood family-life happiness and cognitive functioning was explained, in large part, by adult psychosocial resource in the form of self-mastery net of demographic covariates, education, and adult health.
Our results suggest that growing up in a nurturing, cherished family environment has the potential to cultivate a sense of control over life and build resilience which could provide an important pathway to successful cognitive aging. This is yet another reminder that family is one of the most important social contexts that affect lifelong health (McEwen & McEwen, 2017). The family environment reflects not only material but also emotional and psychosocial resources of caregivers and the quality of one’s learning environment. Although parental education and family income are closely related to adult health, our findings reveal that other features of the childhood family may also play an important role in shaping later cognitive function. The finding that childhood family-life happiness associated with cognitive function net of childhood SES and adult education suggests that differences in later cognitive function are not merely the product of socioeconomic origins.
To our understanding, the current study is one of the first to examine the potential mechanisms through which positive childhood experiences and growing up in a happy family, in particular, are associated with late life cognitive function in a nationally representative sample. Mediation analysis suggests that growing up in a nurturing family environment has the potential to cultivate a sense of control over life and build resilience which could provide an important pathway to successful cognitive aging. Although prior studies find that childhood consequences for cognitive function operate through adult pathways, existing research focuses on adult socioeconomic position and health conditions as potential mechanisms (Luo & Waite, 2005; Lyu & Burr, 2016; Zhang et al., 2016). Studies investigating the mediating role of psychosocial resources are limited mainly to physical health outcomes (Ferraro et al., 2016; Morton et al., 2012). Our findings provide novel insights into how family social environment improves and boosts resilience that may well protect cognitive function later.
The present study has several strengths, including the assessment of both family social and financial well-being as early life determinants of cognitive functioning, the exploration of adult resources as life course pathways to differences in cognitive performance in later life, and the application of a formal mediation test to determine which pathways play the greatest role in explaining the long-term effect of childhood family conditions on later cognition.
Despite these strengths, the study has several limitations. First, the measures of childhood circumstances are retrospective and, therefore, may be subject to recall bias. Such bias could conceivably lead to under or overestimates in our regression analysis. Should people with memory problems impute undue negativity to their childhood home, the association between family-life happiness and cognition would be upwardly biased. On the other hand, if impaired memory tends to produce excessively rosy recollections, associations would be underestimated. Ultimately, it is unknown how poor cognitive health affects people of how they remember their childhood home, so the direction of the bias is uncertain. Fortunately, Leyhe et al. (2009) found that older adults in population-based social survey seem to recall childhood circumstances quite well and propose that early life autobiographical memories may not be susceptible to declines in recall. Still, the possibility of recall bias in retrospective variables suggests that caution is needed when interpreting results. In addition, the generalizability of our findings may be limited to those cognitively intact who still live independently in their communities. NSHAP did not assess cognitive function for those who are institutionalized at the time of survey and who had proxy-interviewed, and their cognitive function may be at greater risk of being poor cognitive function. It is also possible that those who were not healthy did not survive to Wave 3. Respondents of Waves 1 and 2 who survived to the Wave 3 interview may, therefore, be healthier and more cognitively intact than the average older adult. This selection bias might have resulted in a relative underrepresentation of respondents who developed poor cognitive functioning, potentially leading to overly conservative estimates. Again, careful interpretation of results is warranted.
Furthermore, this study was cross-sectional and, therefore, unable to explore whether childhood family-life happiness contributes to changes in cognitive function over time. Some studies have found positive parent–child relationships benefit health over time (Andersson, 2016; Chen & Harris, 2019; Chopik & Edelstein, 2019). However, the underlying mechanisms that produce cumulative advantage processes for cognitive health during late adulthood are not yet well understood. We call for research testing causal pathways through which positive childhood experiences contribute to the progression of cognitive decline.
Last, the childhood family-life happiness measure used in this study focuses primarily on whether respondents had a happy family life and may not identify all key characteristics of a happy childhood. Positive childhood memories can occur across multiple contexts of individuals’ lives, including home, extended family, school, and community. Warm and cohesive relationships with grandparents, peers, and teachers and a sense of belonging to community could all positively contribute to childhood memories and experiences. In addition, interactions with older siblings may promote language and cognitive development for younger children and help create a cognitively stimulating home environment (Brody, 2004). However, information about birth order, number of siblings, and relationships with extended family members and other people in schools and neighborhoods is not available in NSHAP. Future work should determine if adult health is linked to these other dimensions of happy childhoods.
This study highlights the importance of accounting for childhood family life when examining how early life experiences predict late life cognitive health. We provide evidence that growing up in a socially enriched, nurturing family environment has a positive association with cognitive function, even decades later, in part, through developing mastery, a sense of control over goals, behaviors, and problems in one’s life. Research on resilience also suggests that mastery could be an important resource for those growing up with challenging circumstances by helping them recover, sustain a sense of purpose, and thrive (Infurna et al., 2015; Masten et al., 1990). Policies and programs encouraging the development of mastery during childhood and beyond may help individuals overcome early adversity and maintain healthy cognition over the life course.
Footnotes
Author’s Note
An earlier version of this study was presented at The 2019 Gerontological Society of America Annual Scientific Meeting in Austin, Texas.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Multidisciplinary Research Training in Gerontology at the University of Southern California [T32AG000037] and from the NSHAP Fellows Program at NORC at the University of Chicago. The National Social Life, Health, and Aging Project is supported by the National Institute on Aging and the National Institutes of Health [R01AG043538; R01AG048511]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.