
Abstract
Introduction
The number of older American Indians and Alaska Natives (AI/ANs) will substantially increase over the next 50 years (Griffin-Pierce et al., 2008), from 464,000 in 2012 to 1,624,000 in 2050 (Goins et al., 2015). Their aging, and concomitant risk for Alzheimer’s disease and related dementias, pose particular challenges for this historically neglected, under-resourced population (Griffin-Pierce et al., 2008). As of 2018, it is estimated that 5.7 million people in the United States suffer from Alzheimer’s disease with an anticipated increase to 14 million by 2050 (Alzheimer’s Association, 2018; Herbert et al., 2003; Plassman et al., 2007; Schaefer et al., 2019). The potential compromises of the health status and function of older AI/AN people are obvious, as are the subsequent demands on family and the increased costs to formal, as well as informal, systems of care (DHHS, CMS, 2015). However, the less tangible consequences are not as immediately evident but may be just as injurious. These consequences relate to the strength and resiliency older AI/AN adults draw from their traditions, cultural identity, and connection to community.
We know, for example, that cultural identity plays a significant role in overcoming personal challenges and in instilling a sense of coherence and belonging among AI/AN people (Kahn et al., 2016; Wexler, 2014). Indeed, the relationships older AI/AN adults enjoy with respect to their tribal communities have been shown to strengthen individual resilience, coping abilities, and self-efficacy (Ramirez & Hammack, 2014; Grandbois & Sanders, 2009). Moreover, tribal communities are strengthened by the participation of their tribal elders. Older AI/ANs are the wisdom keepers who embody life’s lessons and knowledge of how to survive in an adverse world (Kahn et al., 2016; Brave Heart & Debruyn, 1998; Grandbois & Sanders, 2009; Masten, 1994). They represent, therefore, a treasured asset in tribal communities, underscoring the ways in which cultural participation, social support, and identity can buffer Native people from contemporary vicissitudes (Cross, 1998; Kahn et al., 2016; Kulis et al., 2016; EchoHawk, 1997; Grandbois & Sanders, 2009; LaFromboise et al., 2006; Wexler, 2014; Wexler et al., 2009).
Social engagement is often defined as preserving social connections and partaking in social activities (Bassuk et al., 1999; Krueger et al., 2009). Among older, non-Native adults, social engagement is a widely recognized correlate of health status, function, and well-being (Coulton et al., 2015; Daykin et al., 2018; Fancourt & Steptoe, 2019; Jones et al., 2012; Fancourt, Perkins, Ascenso, Atkins et al., 2016; Fancourt, Perkins, Ascenso, Carvalho et al., 2016; Fancourt & Perkins, 2018; Mössler et al., 1996). It promotes social support, coping skills, cognitive stimulation, regulation of emotions, problem-solving skills, and reduced symptoms of depression. Additionally, a lack of social engagement is associated with cognitive decline. Recent studies show that older people who are not socially engaged experience lower levels of cognitive function than their counterparts who are so engaged (Barnes et al., 2004; Bassuk et al., 1999; Crooks et al., 2008; Green et al., 2008; Holtzman et al., 2004; Krueger et al., 2009; Li et al., 2019; Yeh & Liu, 2003; Zunzunegui et al., 2003). There is every reason to anticipate similar circumstances pertain to older AI/ANs, especially in light of the tight-knit, face-to-face communities in which they live.
Drawing upon cross-sectional data acquired from 14,827 older AI/AN adults during the 2014–2017 cycle of Identifying Our Needs: A Survey of Elders (ION), this article examines the associations of cultural participation and social engagement with cognitive status among older AI/ANs, specifically with their self-reported diagnosis of memory problems.
Methods
Data Source
In 1999, the National Resource Center on Native American Aging launched the Identifying Our Needs: A Survey of Elders (ION) to assess the needs of this special population. Over the ensuing decades, every 3 years, older American Indians, Alaska Natives, and Native Hawaiians completed a health and social needs questionnaire, which was either self- or interviewer-administered. Eligibility requirements included (1) 55 years of age or older; (2) membership in a federally recognized tribe, and (3) qualifying for Older Americans Act (OAA) Title VI services. Title VI provides grants to improve nutrition, provide supportive services, and promote caregiving for tribal elders.
OAA Tribal Title VI program directors and staff administered the surveys to local elders. We sought systematic randomized samples of program participants. However, this ultimately proved impractical and beyond the Title VI staff’s ability to carry out, resulting in a large convenience sample recruited from a known universe, but subject to uncertain selection biases. Study details have been published previously (Adamsen et al., 2018; Schroeder et al., 2018).
Study Population
The present analyses drew upon survey data from the 2014–2017 cycle. After excluding Native Hawaiian respondents, the dataset yielded 14,827 older AI/AN members of federally recognized tribes. Participants resided in 28 states and represented 11 of 12 Indian Health Service regions.
Study Approvals
The original study, Health and Social Needs Assessment of Native American Elders, was approved in 2007 and has been granted continued approval each year by the University of North Dakota Institutional Review Board (approval number IRB-200712-139). In addition, a tribal resolution was obtained from each participating tribe granting permission to administer the survey to the elders in their communities. Consent was sought and obtained verbally by survey administrators. Administration for Community Living grantors reviewed and approved this article before publication.
Cultural Participation, Social Engagement, and Self-Reported Diagnosis of Memory Problems
Cultural participation was determined by the answer to the question: “Do you participate in cultural practices that include traditional food, music, and customs?” Response options included all of the time, most of the time, a good bit of the time, some of the time, a little of the time, and none of the time. In like fashion, social engagement was operationalized in terms of the answer to: “How often do you get out and socialize (attend church/religious meetings, clubs/organizations you belong to, or attend cultural activities/traditional ceremonies)?” The respondent was asked to indicate the number of times per month s/he socialized as her/his response. Cultural participation and social engagement were then combined to create a categorical variable yielding four categories: low cultural participation + low social engagement, low cultural participation + high social engagement, high cultural participation + low social engagement, and high cultural participation + high social engagement. With respect to cultural participation, responses of all of the time, most of the time, a good bit of the time, and some of the time were categorized as “high” cultural participation, while responses of a little of the time and none of the time were coded as “low” cultural participation. During exploratory data analysis, we found 8 or less times per month versus 9 or more times per month was a change point with respect to the association between social engagement and self-reported diagnosis of memory problems. Therefore, social engagement was also treated as a binary variable. Responses of 9 or more times per month were recoded as “high” social engagement and 8 or less times per month as “low” social engagement. Self-reported diagnosis of memory problems was determined by asking the participant, “Have you been diagnosed with Alzheimer’s disease, dementia, or other problems with memory or thinking?” The response options provided were yes and no.
Covariates
Selected covariates included age (continuous), gender (male/female), annual personal income (<$15,000, $15,000 to < $25,000, $25,000 to < $50,000, ≥ $50,000), education (<high school diploma, high school diploma, and beyond high school), employment status (employed and unemployed), marital status (married or living with partner, single/never married, divorced, separated, or widowed), and residence (resided on reservation and off reservation). These covariates represented key demographics thought to have an effect on health-related outcomes of older AI/ANs. In addition, self-reported clinical diagnosis of depression (yes and no) and feeling downhearted and blue (all of the time/good bit of the time, some of the time, a little of the time, and none of the time) were included as covariates because they are thought to have an effect on self-reported diagnosis of memory problems of older AI/ANs.
Statistical Analysis
Sample characteristics were summarized by frequencies and percentages of categorical variables. Chi-square tests were performed to compare the characteristics of older AI/ANs who self-reported diagnosis of memory problems to those who did not report such problems.
Logistic regressions (separate logistic regression models adjusted by age and gender only) were employed to assess the association of self-reported diagnosis of memory problems with cultural participation and social engagement and each of the covariates without controlling for differences in other covariates (except age and gender). Multivariate logistic regressions—adjusted by age, gender, self-reported clinical diagnosis of depression, feeling downhearted and blue, annual personal income, education, employment status, marital status, and residence—were used to examine the association of self-reported diagnosis of memory problems with cultural participation and social engagement while adjusting for the differences in all the covariates considered. All analyses were conducted using IBM SPSS Statistics software (version 25).
Results
Sample Characteristics by Self-Reported Diagnosis of Memory Problems Among Older American Indians and Alaska Natives.

Association of Self-Reported Diagnosis of Memory Problems With Cultural Participation and Social Engagement Among Older American Indians and Alaska Natives.
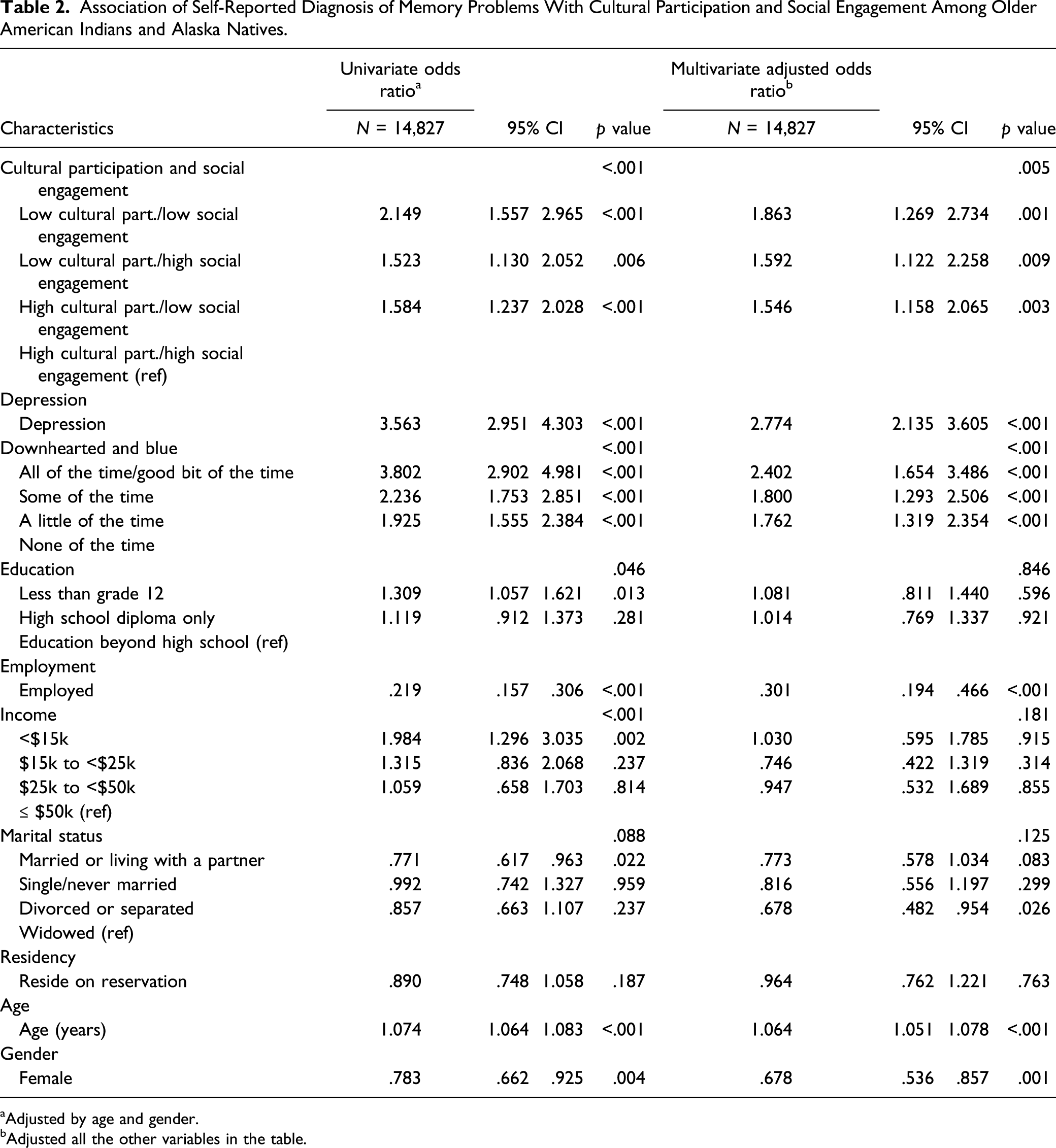
aAdjusted by age and gender.
bAdjusted all the other variables in the table.
The multivariate analyses, after controlling for all demographic variables, revealed that cultural participation and social engagement were significantly associated with self-reported diagnosis of memory problems. Older AI/ANs who exhibited low cultural participation and low social engagement (OR = 1.863, 95% CI: [1.269, 2.734], p < .001), low cultural participation and high social engagement (OR = 1.592, 95% CI: [1.122, 2.258], p = .009), and high cultural participation and low social engagement (OR = 1.546, 95% CI: [1.158, 2.065], p = .003) were significantly more likely to self-report diagnoses of memory problems compared to those who reported high cultural participation and high social engagement. Furthermore, after adjusting for other demographic characteristics, older AI/ANs who were employed (OR = .301, 95% CI: [.194, .466], p <.001), divorced or separated (OR = .678, 95% CI: [.482, .954], p = .026), and female (OR = .678, 95% CI: [.536, .857], p = .001) were significantly less likely than their reference group to acknowledge self-reported diagnoses of memory problems. Education, income, and residency were not significantly associated with the dependent variable in the multivariate model.
Discussion
Our study found significant associations between cultural participation and social engagement with self-reported diagnosis of memory problems among older AI/ANs. Participants reporting low cultural participation and low social engagement endorsed higher rates of memory problems.
The protective and therapeutic value of culture for AI/ANs is acknowledged, especially with respect to health outcomes (Bassett et al., 2012). Cultural activities reinforce a sense of self, promote psychological coherence, affirm individual value, assert order in the world, and locate one within it (Cross, 1998; Grandbois & Sanders, 2009; Kahn et al., 2016; Lewis, 2016). Drumming, beading, dancing, storytelling, harvesting and preparing traditional foods, seasonal ceremonies, and praying, as well as more formal spiritual practices, revolve around elders in Native communities (Bassett et al., 2012; Lewis, 2011; Lewis & Allen, 2017). These elders give to as much as they receive from participation in this cultural life. It is not difficult, then, to imagine the benefits that may accrue in terms of fostering their cognitive well-being. If cultural participation indeed offers such benefits, can we mobilize the power of “culture as medicine” (Bassett et al., 2012) to forestall declines in memory loss among AI/ANs as they age?
Cultural practices are not just about the making of meaning, about human knowledge, or about beliefs. Like more mundane aspects of social life, they also present opportunities to interact with family, friends, and other community members and to be engaged. The gatherings of Native people—home visiting, caring for children, Bingo games, fiddling contests, lacrosse competitions, potlatches, giveaways, memorials, powwows, to name a few—are in service of this sociocentric view. Again, elders are typically at the center of such events, acting as the agents who bond infants, children, adolescents, and adults together. AI/AN peoples are socially oriented; their self-hood is rooted in the group, and they look to others for affirmation of personal value (Kahn et al., 2016; Wexler, 2014).
The literature documents that higher levels of cognitive function in older adults are associated with greater social engagement (Krueger et al., 2009). It also describes the reduced risk of late-age cognitive decline and dementia associated with satisfying social relationships, with taking part in productive and stimulating cognitive activities, and with possessing a large number of social contacts (Crowe et al., 2003; Fabrigoule et al., 1995; Fratiglioni et al., 2000; Holtzman et al., 2004; Saczynski et al., 2006; ; Scarmeas et al., 2001; Wang et al., 2002; Wilson et al., 2002). A recent study even underscores the contribution of social engagement to improved brain health and lower likelihood, as well as severity, of the pathology associated with Alzheimer’s disease (Johnson et al., 2018). For these reasons, then, maintaining or even enhancing the social lives of older AI/ANs may promise to ameliorate their risk of memory loss and related problems.
Limitations
The findings of this study and their implications are limited by several factors. First, given the cross-sectional nature of the available data, we cannot specify the nature of the relationships we found. High cultural participation and high social engagement may protect older AI/ANs from such memory problems; alternatively, memory problems may in turn lead to low cultural participation and to low social engagement. We were unable to determine from these data if these associations reflect an underlying causal mechanism or its likely valence. Nevertheless, the associations are intriguing, pose several interesting possibilities, and warrant further investigation.
Second, the self-report requirements of the survey prevented the inclusion of older AI/ANs who suffered moderate to severe memory loss. Those who participated were likely to be in the early stages of cognitive decline. Therefore, it is difficult to determine if the outcomes would have been similar among older AI/AN adults experiencing more severe memory problems. Third, the sample was recruited from OAA Title VI tribal programs. As a consequence, elders in these communities who did not meet the eligibility for Title VI programs were unable to participate in the survey. This may have reduced the representation of higher functioning, community-dwelling older adults who do not require access to nutritional and other resources available through these programs. Fourth, though the survey design called for random sampling of OAA Title VI program participants, we were not able to faithfully execute this plan. Hence, there may be unknown selection biases at work which could temper our conclusions. Last, the dependent variable—self-reported diagnosis of memory problems—is vulnerable to possible recall bias as well as inconsistencies in alleged assessment. Yet, despite these limitations, this study drew upon the largest dataset available specific to this special population and yielded robust findings consistent with the relevant literature, which had not previously considered older AI/AN adults.
Conclusion
This study confirmed associations between cultural participation and social engagement with self-reported diagnosis of memory problems among older AI/ANs. Nevertheless, cultural participation and social engagement may figure importantly in ameliorating risk of memory loss and related problems in this special population. If so, these observations support the growing call to incorporate such experiences into programs intended to prevent as well as to treat memory loss and its consequences among older AI/ANs. Pragmatically, we should seek to maximize opportunities for Native elders to actively participate in cultural practices and in the social life of their communities. With respect to the scientific agenda, careful attention to evaluating the ensuing efforts may afford us greater insight into the dynamics that underlie such relationships.
Nonetheless, the findings of this study can help inform evolving treatment options related to memory problems that tie in cultural and social engagement aspects specific to AI/AN elders. Studies related to this topic on this population are limited; therefore, the observations will contribute to filling the gap of much needed information related to memory problems among AI/AN elders. Furthermore, the study will help us better understand memory problems and related risks among this population, which will lead to an improvement in caregiving and treatment options for AI/AN elders.
Footnotes
Acknowledgment
The authors would like to thank Sara Mumby for her editorial contributions to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging [P30 AG015292, SM Manson; P30 AG059295, D Buchwald & SM Manson] and the National Institute on Minority Health and Health Disparities Center of Excellence [P60 MD000507; SM Manson]. The Identifying Our Needs: A Survey of Elders and the National Resource Center on Native American Aging (NRCNAA) are funded by the Administration for Community Living [90OI0008-03-00].