
Abstract
Introduction
Rescue and recovery workers involved in the emergency response and cleanup efforts following the 2001 World Trade Center (WTC) attacks were exposed to high levels of toxicants and intense psychological trauma. In the years following the attacks, studies have documented a high level of disease burden among the WTC General Responder Cohort (GRC) (Crane et al., 2013). About one-half of these responders have developed abnormal spirometry and respiratory diseases (Dasaro et al., 2017), and approximately one-third have developed mental health conditions such as depression and post-traumatic stress disorder (Singh et al., 2020). Additionally, studies have observed elevated risk of various cancers among this cohort (Shapiro et al., 2020; Solan et al., 2013). As the cohort ages, it is expected that responders, similar to older adults in the community, will accumulate multiple comorbidities and develop age-related syndromes such as osteoarthritis and hypertension (Fried et al., 2004); in fact, cognitive impacts are now also documented as WTC-related “emerging conditions” (Clouston et al., 2020). Thus, there is a pressing need to characterize, assess, and monitor the development of age-related syndromes among this cohort, as the WTC exposures may alter the trajectory of aging among these responders.
Frailty is characterized by physiological declines and vulnerability to adverse health outcomes; as a validated conceptual framework for understanding age-related health problems and variability, it may be applied to understand the trajectory of age-related changes associated with WTC exposures. Frailty is a recognized syndrome common among older adults resulting from cumulative declines across multiple physiological symptoms (Chen et al., 2014; Ko and Walston, 2012). It is characterized by an individual’s increased vulnerability to adverse events (including mortality, morbidity, disability, and hospitalizations) occurring after exposure to stressors (Clegg et al., 2013; Morley et al., 2013). Because it can have a serious impact on quality of life, frailty assessment is now recommended in routine clinical examinations among older adults (Morley et al., 2013).
A validated and commonly used approach to measure frailty is the Frailty Index model (Mitnitski et al., 2001), which conceptualizes frailty as the accumulation of functional and health deficits resulting from (and indicative of) a diminishing ability to maintain normal function/homeostasis. With this “deficit accumulation” model, frailty is measured by computing the proportion of deficits in multiple domains of health and well-being: disability, functional impairment, health conditions, and comorbidities. The frailty index has been developed and validated on various secondary datasets and found to be associated with adverse outcomes, such as mortality and hospitalizations (Kojima et al., 2018; Theou et al., 2018; Woo et al., 2006). These results are consistent across various studies, despite the fact that the deficits used to construct the frailty index vary from study to study (Bergman et al., 2007; Mitnitski et al., 2002). As a construct, the frailty index is fairly robust to the deficits used in its construction, as long as they meet certain criteria; for example, deficits should be related to health status, deficit prevalence should increase with age (without plateauing/saturating too early), and the deficits as a group should be sufficiently large and span multiple domains of health (Searle et al., 2008). This gives the frailty index the flexibility to be adapted for use with different secondary data.
An alternative approach for measuring frailty is the Frailty Phenotype, which conceptualizes frailty as a distinct syndrome, assessed via a fixed set of five criteria representing the presence of specific clinical signs, symptoms, and physiology (Fried et al., 2001). However, because of its greater flexibility and consistency, in this study we focus on the deficit accumulation approach to frailty, the Frailty Index model.
Conventionally, the frailty index is constructed largely using clinically observable health deficits, that is, impairments in activities of daily living, disease, weakness, limited mobility, cognitive changes, sensory loss, etc. Recent years have seen the introduction of a new frailty index instrument constructed exclusively using laboratory test results, that is, serum biomarkers of organ and overall physiological function (Howlett et al., 2014). Referred to as FI-Lab, it is thought to assess physiological dysregulation, that is, systemic, organ-level dysregulation that occurs as a direct result of molecular- or cellular-level damage (e.g., oxidative stress and inflammation). This dysregulation may be a precursor to the clinically observable (“macroscopic”) functional deficits assessed in the conventional frailty index (sometimes referred to as FI-Clinical, to distinguish it from the FI-Lab instrument) (Zaslavsky et al., 2013).
Because it offers a large degree of latitude in the variables used in its construction, the frailty index approach is especially suitable for the WTC cohort, who have had repeated health-related assessments with information managed by the World Trade Center Health Program (WTCHP) General Responder Data Center. In previous work, using this cohort we developed and validated the WTC FI-Lab, a laboratory test–based frailty index for assessing age-related deterioration in physiological function (Bello et al., 2018). This frailty index was constructed using standard laboratory test biomarkers and spirometric indices (see Bello et al. (2018) for full details).
In the present study, we directly assess clinically evident deficits using data collected on the WTC GRC. As part of the WTCHP, a battery of clinical data has routinely been collected. We will use these data to develop and validate a clinical frailty index (henceforth referred to as WTC FI-Clinical) to characterize the burden of age-related clinical deficits in this population, as well as to identify factors associated/correlated with frailty. Relative to laboratory-based frailty indices, clinical frailty indices are considered the more standard tool for frailty assessment. The validity of the WTC FI-Clinical will be assessed by evaluating its relationship with all-cause mortality. With this newly created index, we will assess and characterize clinical frailty among WTC cohort members aged 40 years and older, starting from the year 2012 (approximately a decade after 9/11) through 2017. We will then examine the relationship of the WTC FI-Clinical with various cohort characteristics, as well as with the physiological frailty index, WTC FI-Lab.
Methods
WTC GRC
After the 9/11 WTC attacks, various health programs were established to provide clinical monitoring and treatment for responders. The CDC/NIOSH-funded WTC Health Program (WTCHP) was set up to consolidate these programs (Dasaro et al., 2017). This study is based on a large cohort of general (largely non-firefighter) responders to the 9/11 WTC attacks, who enrolled in the WTCHP beginning in 2002. Details on this cohort have already been described elsewhere (Dasaro et al., 2017). As part of the WTCHP, enrollees undergo periodic (often annual) clinical monitoring visits at which they receive a battery of health assessments. This study utilizes clinical data collected during these monitoring visits, details of which are described in the next section. All procedures contributing to this study comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The WTCHP obtained the signed consent of all participants. Informed consent was solicited via a standardized form approved by the Institutional Review Board (IRB) of the clinical center at Mount Sinai. The consent form gave options to use data for research, be contacted for research, and have information passed to state cancer and other registries. The WTCHP was initially approved by the IRB of the Mount Sinai School of Medicine and subsequently by the IRB of the Icahn School of Medicine at Mount Sinai.
Study Sample
Because the goal of this study was to assess clinical frailty among the WTC GRC beginning about 10 years after November 9, 2001, we used only data collected from 2012 onward. We selected WTC GRC members who had at least one follow-up clinical monitoring visit between 2012 and 2017 and who were aged 40+ years at the time of the visit. We chose 2017 as the upper limit of the study because this was the last year of follow-up for our mortality data (described below). Our study was restricted to members whose monitoring visits were conducted at the largest WTCHP clinic, the Mount Sinai Selikoff Centers for Occupational Health in New York City. Any visits missing data required for frailty scoring were excluded from further consideration. For the purpose of our analyses, only one visit per subject (the most recent) was selected, henceforth referred to here as the “index visit.” The resulting study dataset had a sample size of 6197.
Measures
At each monitoring visit, WTC GRC members receive a battery of clinical tests, questionnaires, and interviews. Details of these assessments are given in Dasaro et al. (2017), but we provide a brief overview here, particularly for the data elements used in this study.
Physical Examinations
Physical examinations were performed at each monitoring visit by qualified physicians. These involved assessment of body measures (e.g., blood pressure and height/weight), eyesight, hearing, general appearance, etc.
Exposure Assessment Questionnaire
WTC exposure has been characterized with different variables that include time of arrival, duration of work on the site, having worked on the debris pile, and being caught in the dust cloud on 9/11. The contents of WTC dust have been extensively analyzed and were characterized as a mixture of cement dust, glass fibers, asbestos, lead, polycyclic aromatic hydrocarbons, polychlorinated biphenyls, organochlorine pesticides, and polychlorinated furans and dioxins (Lioy et al., 2002). At their first monitoring visit only, members complete the Exposure Assessment Questionnaire (EAQ), designed to evaluate the extent of exposure to pollutants prior to, and while working on, the rescue and recovery effort. For our analyses, we used responses from the EAQ to assess the extent of exposure, applying a procedure outlined previously (Wisnivesky et al., 2011). This yielded an exposure severity variable with four category levels: low, intermediate, high, and very high exposure. These categories were defined based on a cohort member’s duration of work on the WTC cleanup effort, exposure to the dust cloud on 9/11, and whether or not they worked on the debris pile (complete details are available in Wisnivesky et al. (2011)). Because of low sample size in the “very high” exposure category, in this study we merged the “high” and “very high” exposure categories into one.
Interviewer-Administered Medical Questionnaire
At every visit, a structured, medical-history questionnaire, the Interviewer-Administered Medical Questionnaire (IAMQ), is administered to each WTC GRC member by a trained medical professional. This questionnaire gathers information such as demographics, medical conditions (self-reported), tobacco use history, and employment status.
Self-Administered Mental Health Questionnaire
Beginning with their second monitoring visit, members complete the Self-Administered Mental Health Questionnaire (SAMHQ), a questionnaire that solicits, among other things, information about general well-being, ability to perform activities of daily living, memory loss, etc.
Mortality Data
All-cause mortality data were obtained for the cohort via National Death Index (NDI) linkage with identifier data (for more details on the linkage procedure, see Bello et al. (2017)). For a portion of the cohort, identity information (names, date of birth, social security number, etc.) was provided to the NDI, and probabilistic matching was carried out (National Center for Health Statistics 2013) to determine occurrence of death up to December 31, 2017. For the remainder (those with WTCHP follow-up visits after 2017), their identity information was not sent to NDI because their post-2017 follow-up visits confirmed they were alive after December 31, 2017.
WTC FI-Lab (Physiological Frailty Index)
Development of the FI-Lab using data on WTC cohort members has been described in a previous study (Bello et al., 2018). Briefly, this frailty index was constructed using various physiological parameters (serum biomarkers typically measured in routine clinical laboratory tests and spirometry measures). A pool of these parameters was screened for inclusion in the FI-Lab using a well-established frailty index construction protocol outlined in Searle et al. (2008) (see details in the next section). Twenty of these parameters were selected and used to construct the FI-Lab according to the deficit accumulation model of frailty; that is, the FI-Lab for each subject was computed as the proportion of these physiological parameters on which the subject had abnormal values (fell outside the standard clinical reference ranges for the parameters in question). Examples of physiological parameters selected included albumin, creatinine, neutrophil:lymphocyte ratio, potassium, and the pulmonary function measure FVC (forced vital capacity).
Development and Validation of WTC Clinical Frailty Index
In the first step, a large pool of potentially age-related indicators from the available data collected by the WTCHP was screened for inclusion in the index. These candidate indicators were obtained from responses to the IAMQ, the SAMHQ, and the physical examination. Candidate items from the IAMQ included responses to questions about clinical signs and symptoms potentially related to aging (e.g., difficulty hearing, history/onset of diabetes, and pneumonia). Candidate items from the SAMHQ included responses to questions about physical and mental health issues potentially related to aging (e.g., difficulty climbing stairs and problems with short-term memory). Candidate items from the physical examinations included physician assessments of eyes, ears, heart, and general appearance.
The pool of candidate items (see Appendix Table A1) was screened in a systematic fashion, following a widely used protocol (outlined in Searle et al. (2008)) for constructing frailty indices. This protocol considers that an item/variable is appropriate for inclusion in a frailty index if it is associated with health status and if the prevalence of deficits on this variable increases with age, without plateauing/saturating too early (Rockwood and Mitnitski, 2012; Searle et al., 2008). Each candidate item was coded as a binary value indicating the presence or absence of a deficit, and the correlation between age and the prevalence of deficits on the item was computed. For example, self-rated health was obtained from the SAMHQ, which is administered to responders at every monitoring visit. The question 1 asks responders to rank their health using a five-point Likert scale: Excellent, Very Good, Good, Fair, and Poor. To determine if this item was appropriate for inclusion in our WTC FI-Clinical, we coded it as a binary value where a response of Fair/Poor was considered as a “deficit” (and assigned a score of 1), and a response of Excellent/Very Good/Good was assigned a score of 0 (i.e., not a deficit). For each age (in years) in the 40 to 70 range, the sample prevalence of deficits on this item was calculated (i.e., proportion of individuals with a “deficit” on this item among 40-year-olds, 41-year-olds, 42-year-olds, etc.), after which the Spearman correlation of age with deficit prevalence was computed (the upper limit of 70 years was chosen due to insufficient sample sizes for each year of age beyond this point). If the correlation was at least 0.3, the item (self-rated health) was considered appropriate for inclusion in our WTC FI-Clinical. This procedure was repeated for each item in our candidate pool, and those items with a correlation ≥0.3 with age were selected for inclusion in the WTC FI-Clinical. Once the items were selected, WTC FI-Clinical for each individual in the study sample was computed by averaging their binary scores on all the items, yielding a value between 0 and 1.
Statistical Analyses
Demographic and other cohort characteristics were assessed using median, interquartile range (IQR), and percentages. Age distribution in our sample was assessed using a histogram.
Distributional properties of the newly created WTC FI-Clinical were assessed using a histogram and basic descriptive statistics. Criterion validity for the WTC FI-Clinical (Drubbel et al., 2014) was assessed by examining its association with, and predictive accuracy for all-cause mortality. Specifically, we used a Cox proportional hazards model, with WTC FI-Clinical as the independent variable, adjusting for the following cohort characteristics potentially associated with mortality: age, sex, race, pre-9/11 occupation, education, smoking status, and WTCHP enrollment year. Kaplan–Meier plots and the logrank test were used to compare survival trends between subjects scoring in the lower 50th percentile of WTC FI-Clinical and those in the upper 50th. To assess the predictive accuracy of WTC FI-Clinical for all-cause mortality, we used Harrell’s concordance index (Harrell et al., 1982), an extension of area under the receiver operating characteristic curve for censored time-to-event outcomes. We also examined the correlation of WTC FI-Clinical with age. For each year of age (up to 70 years), the average WTC FI-Clinical was derived, and the correlation between age and mean WTC FI-Clinical was assessed via the Pearson correlation coefficient. The upper limit of 70 years was used here due to low sample size for each year of age beyond this point.
Assessment of Relationship of WTC FI-Clinical with Cohort Characteristics
In a negative binomial regression model, WTC FI-Clinical was treated as the dependent variable, expressed as the count of each subject’s deficits. The following characteristics were included in the model as independent variables: age, sex, race/ethnicity, pre-9/11 occupation, educational status, 9/11 exposure severity (see the previous section Measures), smoking status, year of index visit, and enrollment year.
Comparison of WTC FI-Clinical with WTC FI-Lab
The relationship between WTC FI-Clinical and WTC FI-Lab was assessed via Pearson correlation. Adjusted Cox proportional hazards models were used to assess whether WTC FI-Clinical and WTC FI-Lab were independently associated with all-cause mortality. This model was adjusted for age, sex, race/ethnicity, pre-9/11 occupation, education, smoking status, and enrollment year.
In this study, data preparation was carried out with SAS (SAS Institute, 2016) and R (R Core Team, 2019), and all statistical analyses were performed in R.
Results
Characteristics of study sample.
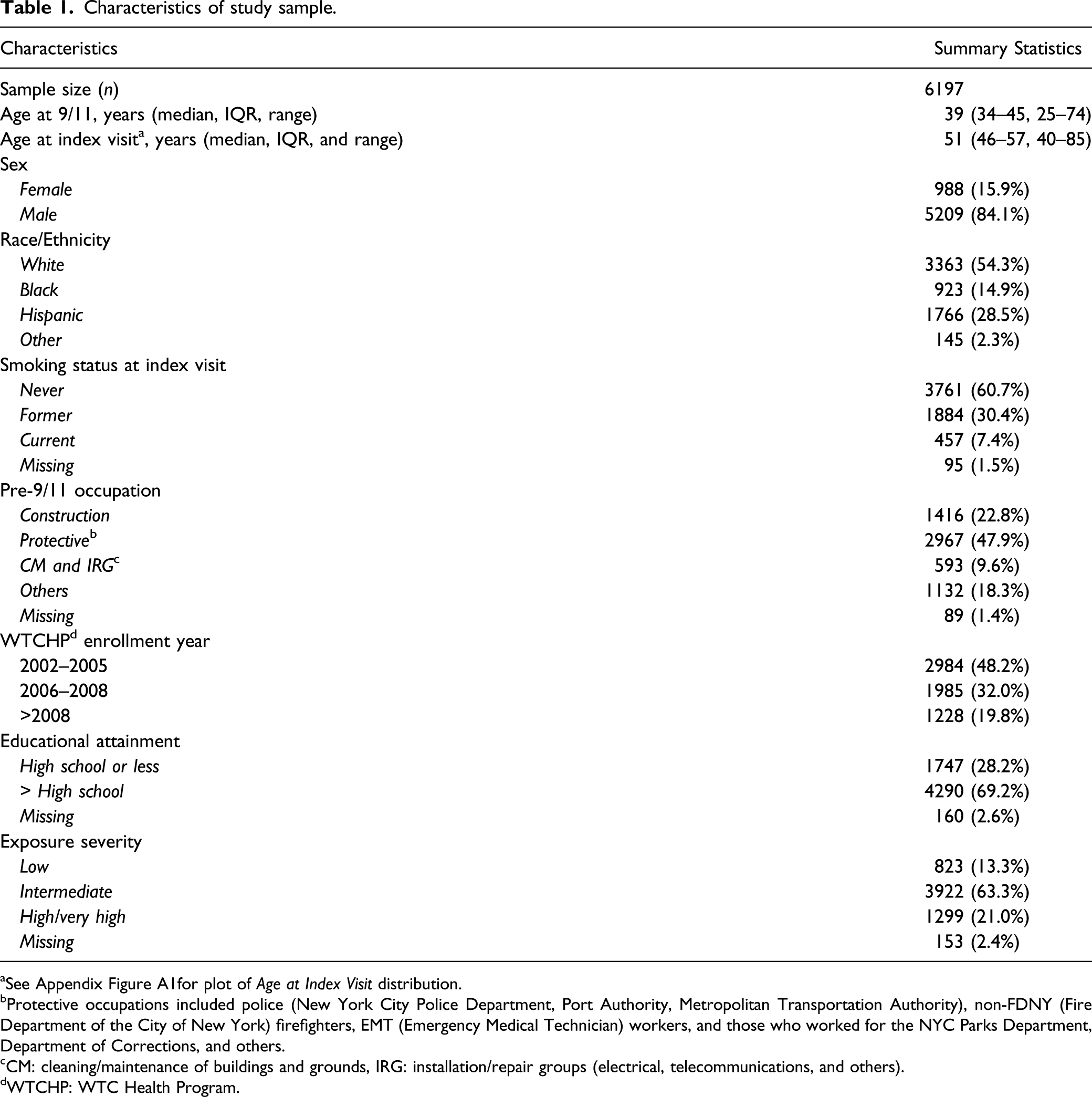
aSee Appendix Figure A1for plot of Age at Index Visit distribution.
bProtective occupations included police (New York City Police Department, Port Authority, Metropolitan Transportation Authority), non-FDNY (Fire Department of the City of New York) firefighters, EMT (Emergency Medical Technician) workers, and those who worked for the NYC Parks Department, Department of Corrections, and others.
cCM: cleaning/maintenance of buildings and grounds, IRG: installation/repair groups (electrical, telecommunications, and others).
dWTCHP: WTC Health Program.
List of WTC FI-Clinical Deficits.
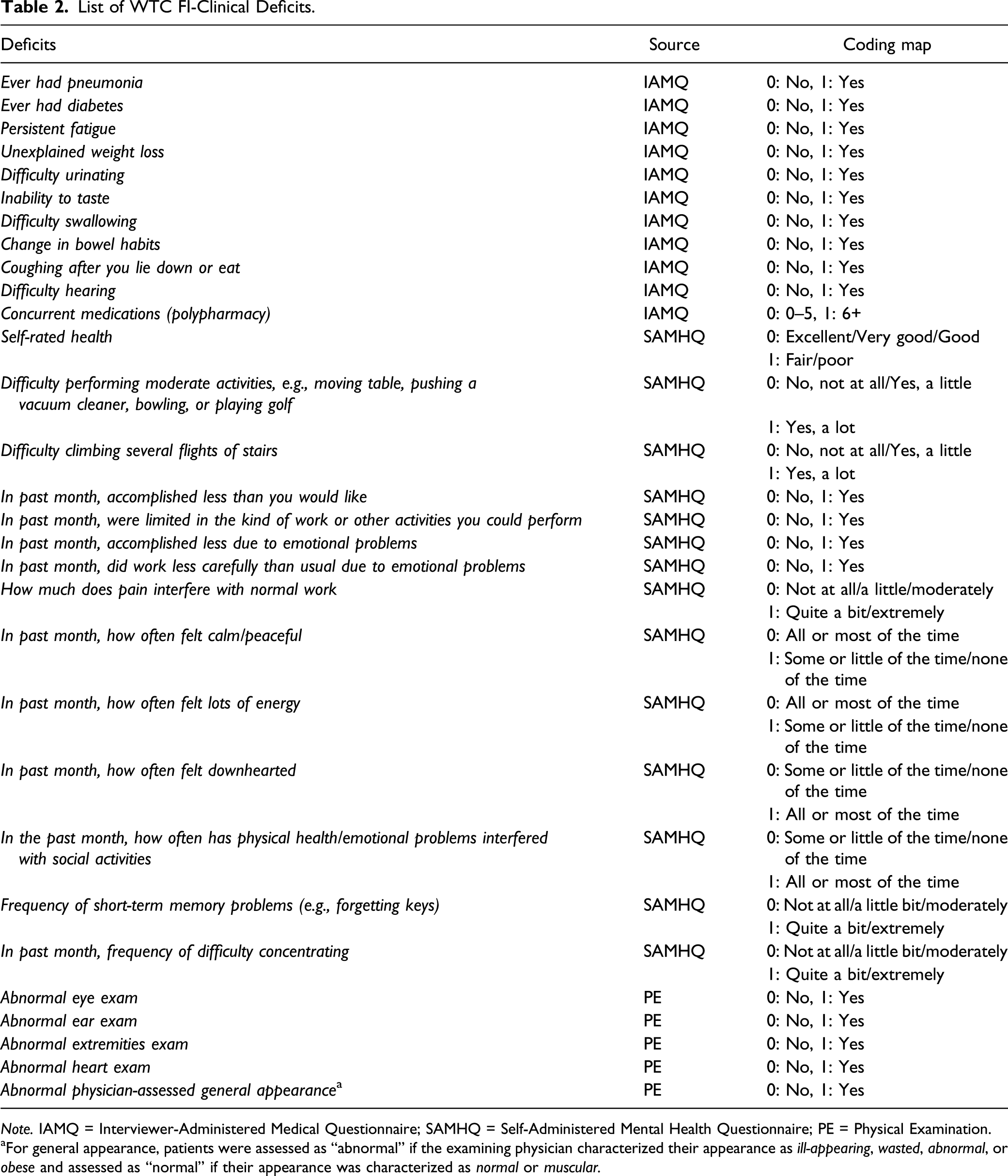
Note. IAMQ = Interviewer-Administered Medical Questionnaire; SAMHQ = Self-Administered Mental Health Questionnaire; PE = Physical Examination.
aFor general appearance, patients were assessed as “abnormal” if the examining physician characterized their appearance as ill-appearing, wasted, abnormal, or obese and assessed as “normal” if their appearance was characterized as normal or muscular.
In general, the items selected for WTC FI-Clinical spanned multiple domains of health and well-being: disability, functional impairment, and health conditions. These domains overlap significantly with those from other frailty indices (e.g., the 70-item Frailty Index developed in Rockwood et al. (2005)). Examples of items that were not selected for our WTC FI-Clinical include presence/absence of physician-observed abnormalities in neck physical examination and questions about presence of acid reflux/regurgitation into mouth or throat.
For each subject, a frailty index score was computed, as described in the Methods section. Figure 1 shows the distribution of the WTC FI-Clinical in the study sample. The distribution shows extreme right-skewness, indicating a preponderance of near-zero frailty scores in our study sample (13.4% had scores of zero). The mean score was 0.18 (SD: 0.17), and the median score was 0.13 (IQR: 0.267). The 99th percentile was 0.63 (below the 0.7 threshold considered to be the theoretical limit of deficit accumulation (Rockwood and Mitnitski, 2006)). WTC FI-Clinical distribution.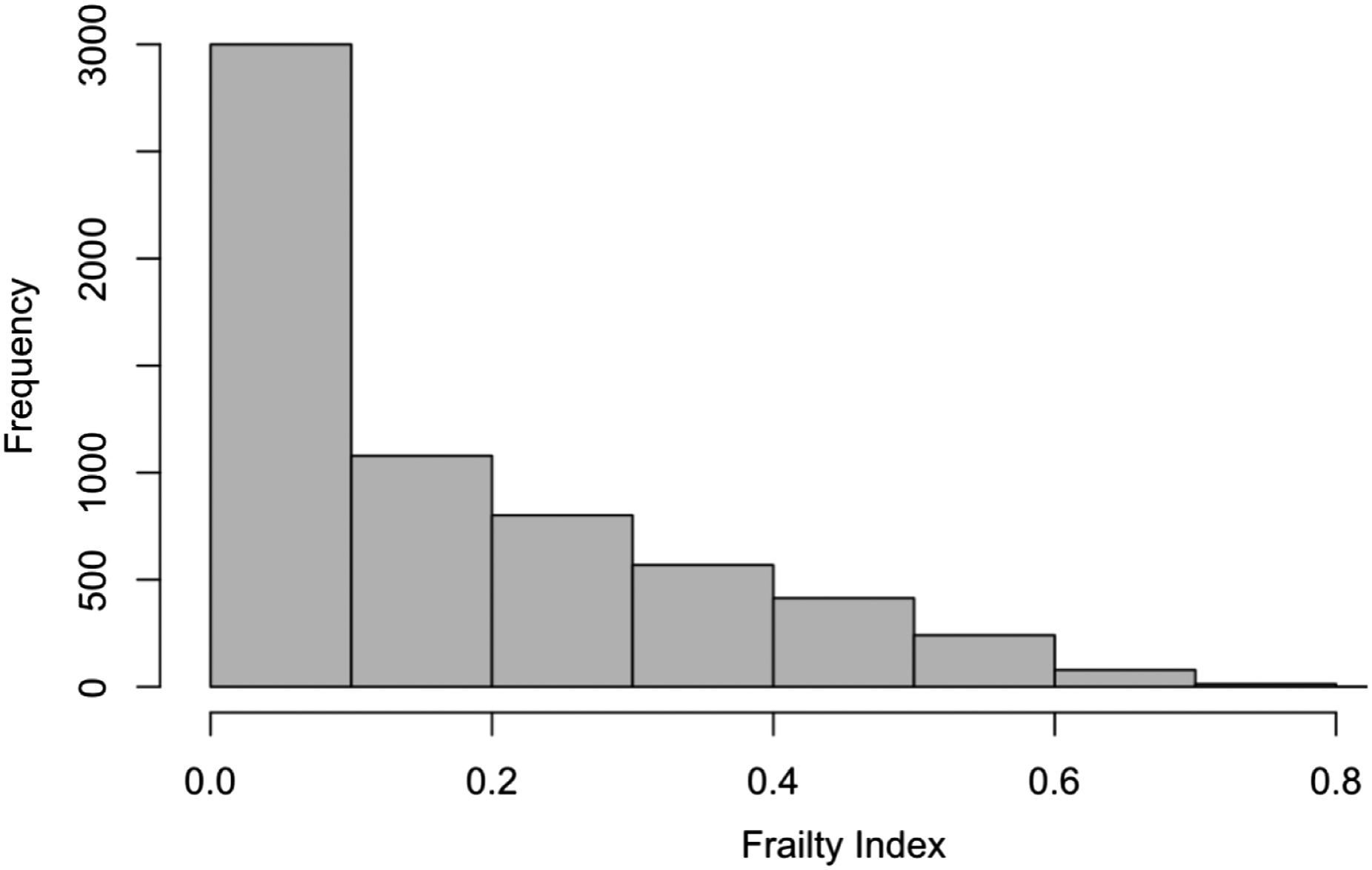
Age showed a strong correlation with mean WTC FI-Clinical, with Pearson correlation coefficient ρ = 0.9 (p <.0001). Figure 2 shows the relationship in the study sample between age and average WTC FI-Clinical. Relationship between age and WTC FI-Clinical. The scatter plot in Figure 2 shows the mean WTC FI-Clinical for each year of age up to 70 (ages beyond 70 excluded due to insufficient sample size). Smooth fit (solid blue curve) was computed using locally weighted scatterplot smoothing (LOWESS).
We also assessed the association of WTC FI-Clinical (expressed as deficit counts) with various cohort characteristics. Figure 3 summarizes the incidence rate ratios (and 95% CIs) for the continuous variables (age and year of index visit) and for non-baseline categories of the categorical variables (race, education, WTC exposure severity, sex, smoking status, pre-9/11 occupation, and enrollment year). Association between WTC FI-Clinical and cohort characteristics.
Baseline (referent) categories for nominal variables were as follows: race: white; education: >high school; WTC exposure severity: low exposure; sex: female; smoking status: current smoker: pre-9/11 occupation: other occupation; enrollment year: >2008.
These results indicate that multiple demographic and risk factors are associated with clinical frailty. In particular, we found that those with high/very high WTC exposure severity had higher frailty, relative to those with low exposure severity (p = 0.005). Those in the protective occupation category (e.g., law enforcement and emergency medical services) up to and at the time of 9/11 had significantly lower frailty (p < .0001) compared to those in the other category (i.e., all other occupations outside of construction, protective, cleaning/maintenance and installation/repair services). And relative to this other occupations category, those in the construction-related occupations had higher frailty (p < .0001). Males in this cohort had higher frailty relative to females (p < .0001), as did Hispanics relative to whites (p < .0001). Relative to (self-reported) current smokers, former smokers, and those who reported never having smoked had significantly lower frailty (p = 0.002 and p < .0001, respectively). Those less educated (high school education or less) had significantly higher frailty (p < .0001) relative to those with greater than high school education.
In the study sample, the median survival time (measured from index visit date) was 4.2 years, and the censoring rate was 98.8%. In a Cox Proportional Hazards model, WTC FI-Clinical showed a strong association with all-cause mortality (p < .0001), after adjustment for the following potential confounders: age, sex, race/ethnicity, pre-9/11 occupation, education, smoking status, and WTCHP enrollment year. The Kaplan-Meier plot in Figure 4 shows survival curves for subjects scoring below and above the median value of WTC FI-Clinical (logrank test: p < .0001): Kaplan-Meier survival curves for low and high WTC FI-Clinical.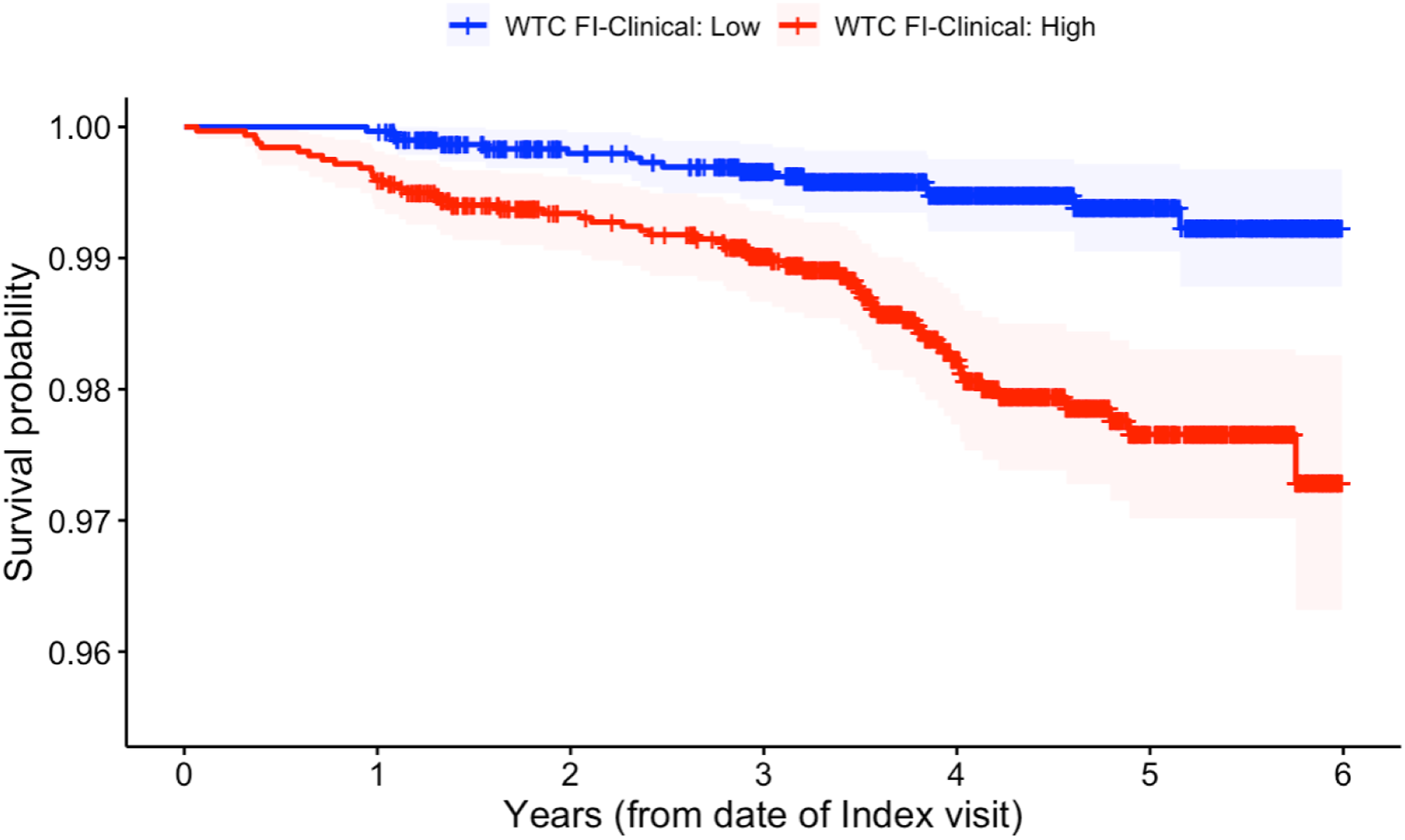
WTC FI-Clinical showed reasonable predictive accuracy for mortality, with a Harrell’s concordance index of 0.69 (95% CI: 0.631–0.749).
Both WTC FI-Clinical and WTC FI-Lab were independently associated with all-cause mortality (p = .0012 and p < .0001, respectively). Pearson correlation of WTC FI-Clinical with WTC FI-Lab was 0.2 (p < .0001), in line with prior estimates of the concordance between these frailty instruments (Rockwood et al., 2015). Figure 5 shows the relationship between WTC FI-Clinical and WTC FI-Lab. Relationship between WTC FI-Clinical and FI-Lab. In Figure 5, the continuous WTC FI-Clinical scale was divided into 7 segments, each of length 0.1 ([0–0.1], (0.1–0.2], (0.2–0.3], etc.). Within each segment, the mean and standard deviation of WTC FI-Lab was computed. The midpoint of each WTC FI-Clinical segment was plotted against the mean WTC FI-Lab within that segment. Standard deviations around the mean are denoted by error bars.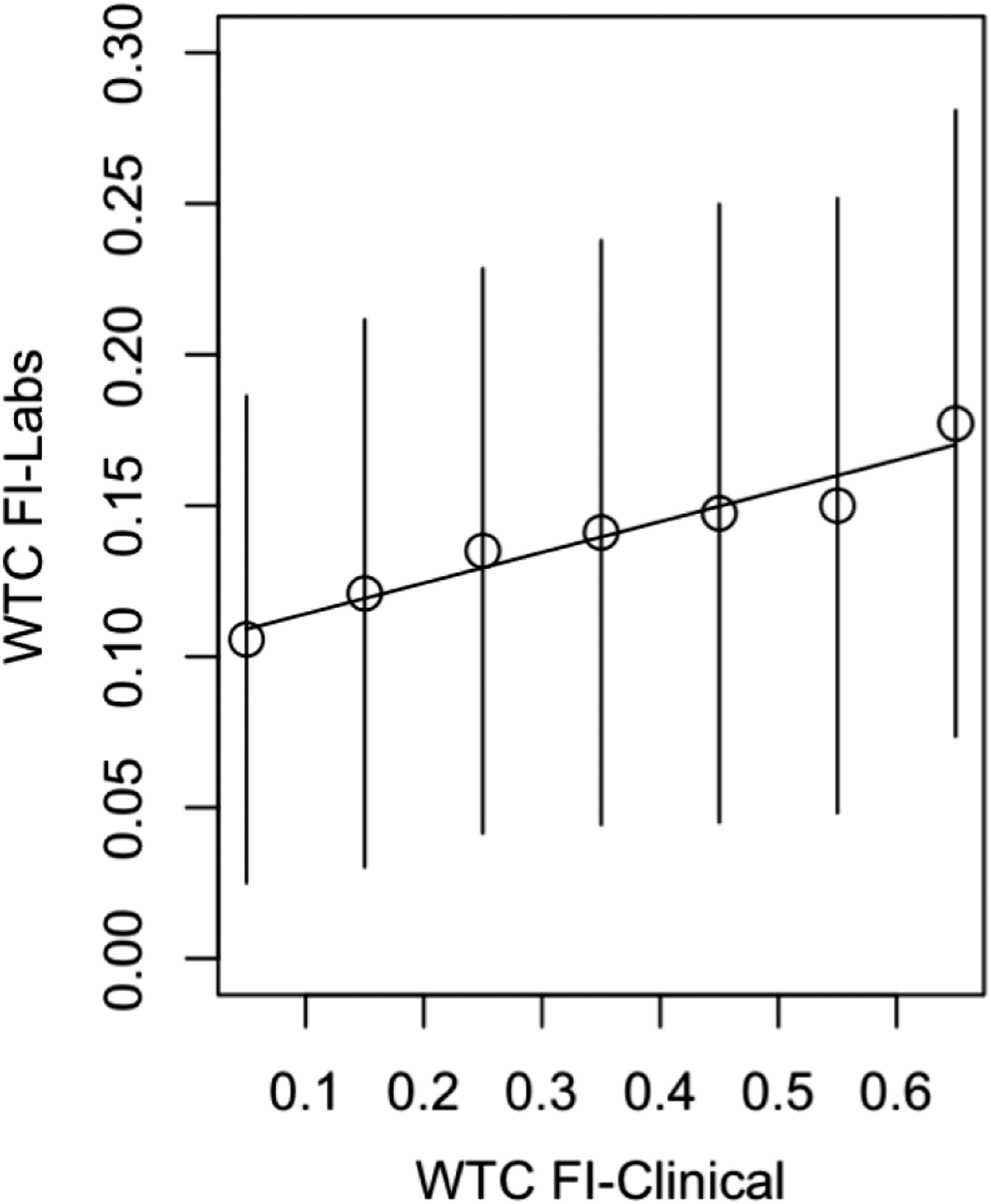
Discussion
In this study, we constructed a clinical frailty index using data routinely collected to monitor WTC general responders. This index was constructed using data elements spanning multiple domains: clinical conditions, health symptoms, and ability to perform activities of daily living. The newly developed WTC FI-Clinical showed a strong association with all-cause mortality, even after adjustment for potentially confounding risk factors. It also showed decent discriminative ability in the prediction of mortality. Multiple cohort characteristics were associated with WTC FI-Clinical. Some of the associations we observed for socio-demographic factors and smoking status have been previously reported in other studies (de Carvalho Mello et al., 2014). For pre-9/11 occupation, we found that construction workers had higher frailty while protective services workers had lower frailty, relative to all other occupations outside of construction, protective, cleaning/maintenance and installation/repair services. This aligns with observations from a prior WTC cohort study which showed that all-cause mortality among construction workers was elevated relative to protective services workers (Stein et al., 2015). Construction workers are exposed to a variety of occupational risks and hazards, for example, chemical toxicants, physical agents (such as the use of vibrating tools), ergonomic hazards, noise, and outdoor/weather conditions (Aarhus et al., 2018; Hajaghazadeh et al., 2019; House et al., 2010). Given this constellation of occupational risks, we believe the increased relative frailty in this occupation group is expected, although this is definitely an understudied area. On the other hand, the protective services occupation group (comprised primarily of New York Police Department personnel) tends to be fitter than the general population since qualification for these occupations often requires passing fitness criteria (and periodic physical and mental tests); thus, the healthy worker effect (Choi, 1992) is particularly pronounced for this group (Solan et al., 2013). Of note, severity of WTC exposure (on 9/11 and over the subsequent cleanup effort) showed a significant association with WTC FI-Clinical over a decade later.
While a mild correlation was observed between WTC FI-Clinical and the previously constructed WTC FI-Lab (Bello et al., 2018), we found both frailty measures to be independently associated with mortality, suggesting they provide somewhat independent information about mortality risk. This trend has been observed in other studies comparing clinical and laboratory test (biomarker)–based frailty indices (Howlett et al., 2014; Mitnitski et al., 2015; Rockwood et al., 2015). It has been suggested that laboratory test–based and clinical frailty influence mortality via different pathways (Blodgett et al., 2016). Further, these frailty measures have also been found to be independently associated with hospital/healthcare utilization and medication use (Blodgett et al., 2016). These findings suggest these two types of frailty indices may provide potentially complementary information about frailty. The key distinction between laboratory-based and clinical frailty indices is that the former, based entirely on biochemical and physiological parameters, is believed to represent the burden of pre-clinical or sub-clinical deficits (deficits at the molecular and cellular level [microscopic]), while the latter is based on clinically evident (macroscopic) deficits (Blodgett et al., 2016). One salient piece of evidence supporting this distinction is the fact that telomere attrition (a correlate of cellular-level aging) has been reported to be associated with laboratory-based frailty indices but not clinical frailty indices (Dent et al., 2018; Bello et al., 2019).
We found a significant association between WTC FI-Clinical and 9/11 exposure severity. This is a relevant relationship that was not observed with WTC FI-Lab. FI-Clinical is constructed with clinical deficits and, therefore, likely provides a more detailed and holistic picture of clinical health than the biomarker-focused FI-Lab. The observed relationship between FI-Clinical and 9/11 exposure severity could be driven by aspects of health that are related to WTC exposure but are not captured by the FI-Lab. Future studies will be dedicated to more comprehensive analyses and comparisons of these frailty indices, including contrasting their ability to predict various WTC-related outcomes and geriatric syndromes.
The findings we report herein need to be considered in light of certain limitations of our study. This study was carried out only on the subset of the WTC GRC, whose monitoring visits were conducted at the largest WTCHP clinic, Mount Sinai Selikoff Centers for Occupational Health in New York City. However, we chose to restrict our analysis to those visiting this clinic because, relative to monitoring visits at other WTCHP clinics, data elements required for computation of WTC FI-Lab and FI-Clinical were more readily available, and the Mount Sinai Selikoff cohort is representative of the larger WTC GRC (Dasaro et al., 2017). Furthermore, WTC exposure characterization suffers from potential misclassification because of recall bias. Responders enrolling in the WTCHP several years after 9/11 may have had inaccurate recollections of their experiences during that period, which impacts exposure assessment accuracy (Shapiro et al., 2020). Due to the uniqueness of our cohort, the generalizability of our findings is likely limited to other cohorts of WTC rescue and recovery workers. Another potential limitation concerns the relatively young age of our study sample (median age in the 50s). With only 2% over the age of 70, this is a largely middle-aged sample. However, multiple studies have focused on frailty in early and late middle-age cohorts and have highlighted its significance in these age groups (Griffin et al., 2018; Gordon et al., 2020; Prince et al., 2019; Thorpe et al., 2016), as well as the need for early identification (Hanlon et al., 2018). This is particularly relevant for our cohort since the long-term influence of exposure to multi-dimensional disasters such as 9/11 on aging is relatively unexplored, and identification of modifiable risk factors for premature aging has a relevant impact for the WTC Health Program. Given the high documented disease burden among this cohort, this study is timed at a critical inflection point at which members are beginning to age into the risk of morbidities of older age. This puts us in a good position to begin tracking signs of early aging, and the progression as the cohort ages. Monitoring frailty at this stage will ultimately enable us to identify those at greatest risk for negative consequences as they age and develop/test appropriate interventions. Cognitive impairment is one of the most salient features of frailty, and many frailty index formulations include items assessing cognition (Rockwood et al., 2005; Clegg et al., 2016; Canevelli et al., 2017; Shahrokni et al., 2019; Won et al., 2020). Cognitive testing is not a routine part of WTCHP monitoring assessments; therefore, our frailty index includes only two brief items related to cognitive function. However, efforts are currently underway to incorporate formal cognitive assessments into routine WTCHP monitoring, and future studies will utilize more comprehensive cognitive data.
Despite these limitations, we have successfully developed a clinical frailty assessment tool using available data collected for nearly two decades on the WTC cohort: more than 30,000 individuals. Calculation of the WTC FI-Clinical does not require collection of any additional data elements, thus paving the way for large-scale retrospective analyses of aging within this cohort. Also, this measure will be useful for current and future WTC research projects focused on the long-term health and well-being of responders across a number of areas, for example, cognitive health, which is already an ongoing area of focus (Clouston et al., 2019, 2020).
The WTC cohort may be especially at risk for negative effects of aging because of previous exposure to environmental toxicants and intense psychological trauma; as such, monitoring of frailty will be critical in the next decade. Frailty can be reduced or delayed through various interventions such as exercise, nutritional supplementation, vitamin D, cognitive training, behavioral therapy, reduction of polypharmacy, and also interventions that could be delivered through clinical care such as comprehensive geriatric assessment and tailored management (Macdonald et al., 2020; Marucci et al., 2019; Morley et al., 2013; Ng et al., 2015; Tarazona-Santabalbina et al., 2016; Walston et al., 2018). For example, the Frailty Intervention Trial (Fairhall et al., 2008), a randomized controlled trial of an intervention comprising an individualized exercise program and management of medical, psychological, and social problems, demonstrated significant improvement in risk factors for falls (Fairhall et al., 2014). For the purposes of optimally managing individuals with a higher degree of vulnerability, frailty can and should be identified at an early stage. Within our cohort, the newly developed WTC FI-Clinical can be deployed in routine clinical follow-up, which will not only enable frailty monitoring within this cohort, but also identify individuals at risk for further decline based on both accumulated deficits and physiological change. Having a reliable WTC cohort–specific frailty instrument will also enable development and testing of potential interventions and early implementation of emerging therapies from other frailty intervention trials. Potential future approaches to target factors impacting both frailty and its manifestations may include solutions that leverage the increasing use of technology for monitoring and support, especially those tested during the course of the current pandemic.
In summary, we have developed and validated a frailty index for quantifying clinically evident deficits, one that serves as a key frailty assessment tool for use in this aging and vulnerable cohort. Ongoing and future research on the WTC general responders should include frailty assessments in order to monitor and improve their long-term health.
Footnotes
Ethical Approval
The World Trade Center Health Programs were initially approved by the IRB of the Mount Sinai School of Medicine and subsequently by both the IRB of the Icahn School of Medicine at Mount Sinai and IRBs of the clinical sites listed in the author affiliations. All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The Health Programs obtained the signed consent of all participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health (CDC/NIOSH) (Contracts and Grants 200-2002-00384, U10-OH008216/23/25/32/39/75, 200-2011-39356/61/77/84/85/88, and U01-OH012068-01). Data were obtained from the WTC Health Program General Responder Data Center at Mount Sinai (CDC/NIOSH contract 200-2017-93325) which also supported the work. The authors are grateful to the responders, all past and present staff of the Programs, the work force, community and volunteer organization program stakeholders, and the philanthropic sources that funded treatment from 2003 to 2006.
Note
Appendix
Pool of candidate deficits considered for inclusion in WTC FI-Clinical (shaded rows correspond to deficits that did not meet inclusion criteria).

| Deficits | Source | Coding map |
|---|---|---|
| Ever had pneumonia | IAMQ | 0: No, 1: Yes |
| Ever had diabetes | IAMQ | 0: No, 1: Yes |
| Persistent fatigue | IAMQ | 0: No, 1: Yes |
| Unexplained weight loss | IAMQ | 0: No, 1: Yes |
| Difficulty urinating | IAMQ | 0: No, 1: Yes |
| Inability to taste | IAMQ | 0: No, 1: Yes |
| Difficulty swallowing | IAMQ | 0: No, 1: Yes |
| Reflux/regurgitation into mouth or throat | IAMQ | 0: No, 1: Yes |
| Change in bowel habits | IAMQ | 0: No, 1: Yes |
| Coughing after you lie down or eat | IAMQ | 0: No, 1: Yes |
| Frequent heartburn/indigestion | IAMQ | 0: No, 1: Yes |
| Difficulty hearing | IAMQ | 0: No, 1: Yes |
| Concurrent medications (polypharmacy) | IAMQ | 0: 0–5, 1: 6+ |
| Self-rated health | SAMHQ | 0: Excellent/Very good/Good |
| 1: Fair/Poor | ||
| Difficulty performing moderate activities, for example, moving table, pushing a vacuum cleaner, bowling, or playing golf | SAMHQ | 0: No, not at all/Yes, a little |
| 1: Yes, a lot | ||
| Difficulty climbing several flights of stairs | SAMHQ | 0: No, not at all/Yes, a little |
| 1: Yes, a lot | ||
| In past month, accomplished less than you would like | SAMHQ | 0: No, 1: Yes |
| In past month, were limited in the kind of work or other activities you could perform | SAMHQ | 0: No, 1: Yes |
| In past month, accomplished less due to emotional problems | SAMHQ | 0: No, 1: Yes |
| In past month, did work less carefully than usual due to emotional problems | SAMHQ | 0: No, 1: Yes |
| How much does pain interfere with normal work | SAMHQ | 0: Not at all/a little/moderately |
| 1: Quite a bit/extremely | ||
| In past month, how often felt calm/peaceful | SAMHQ | 0: All or most of the time |
| 1: Some or little of the time/none of the time | ||
| In past month, how often felt lots of energy | SAMHQ | 0: All or most of the time |
| 1: Some or little of the time/none of the time | ||
| In past month, how often felt downhearted | SAMHQ | 0: Some or little of the time/none of the time |
| 1: All or most of the time | ||
| In the past month, how often has physical health/emotional problems interfered with social activities | SAMHQ | 0: Some or little of the time/none of the time |
| 1: All or most of the time | ||
| Frequency of short-term memory problems (e.g., forgetting keys) | SAMHQ | 0: Not at all/a little bit/moderately |
| 1: Quite a bit/extremely | ||
| In past month, frequency of difficulty concentrating | SAMHQ | 0: Not at all/a little bit/moderately |
| 1: Quite a bit/extremely | ||
| Abnormal eye exam | PE | 0: No, 1: Yes |
| Abnormal ear exam | PE | 0: No, 1: Yes |
| Abnormal extremities exam | PE | 0: No, 1: Yes |
| Abnormal heart exam | PE | 0: No, 1: Yes |
| Abnormal neck exam | PE | 0: No, 1: Yes |
| Abnormal physician-assessed general appearance a | PE | 0: No, 1: Yes |
Note. IAMQ = Interviewer-Administered Medical Questionnaire; SAMHQ = Self-Administered Mental Health Questionnaire; PE = Physical Examination.
aFor general appearance, patients were assessed as “abnormal” if the examining physician characterized their appearance as ill-appearing, wasted, abnormal, or obese and assessed as “normal” if their appearance was characterized as normal or muscular.