
Abstract
Introduction
Once people are enrolled in a health intervention, ensuring their participation and completion is a priority for health researchers across disciplines, not only to establish an intervention’s effectiveness but also, more importantly, to help patients experience the intended benefits of the program (Brueton et al., 2013; Robinson et al., 2007). For older adults, the elevated risk of health concerns makes it especially important that they are empowered to follow health professional recommendations for disability prevention (e.g., exercise and meditation) and management of existing conditions (e.g., psychotherapy and medications).
Of all the factors that influence an individual’s treatment adherence, psychosocial variables are some of the most significant factors. Social support, often referring to the “provision or seeking of instrumental or emotional aid in response to stressful or negative life events” (Feeney & Collins, 2015), has been associated with treatment adherence (e.g., medication, diet, and exercise) for a number of chronic illnesses, such as HIV (Gonzalez et al., 2004), heart failure (Maeda et al., 2013), obesity (Wing & Jeffery, 1999), diabetes (Imayama et al., 2011), and epilepsy (Shallcross et al., 2015). In a randomized controlled trial of a community-based positive psychology intervention for people with depression, social support—which the study defined as the presence of a confidant—was one of the main predictors of both agreeing to start the program and actually completing it (Ayuso-Mateos et al., 2007). Studies of online cognitive behavioral therapy (CBT) interventions for adults with anxiety have also identified social support as a predictor of treatment participation and adherence (Al-Asadi et al., 2014).
In behavioral interventions, the optimal amount of treatment—often referred to as the recommended “treatment dose” or “dosage” (Voils et al., 2012)—is usually measured in the context of participant’s interactions with the intervention in the form of time, frequency, and amount received (Bauer et al., 2015; Voils et al., 2012). Treatment dose is impacted by treatment adherence and can vary by racial and ethnic group, with one study of Medicaid recipients indicating lower medication adherence among Black patients compared to White patients across a variety of health diagnoses including depression and diabetes (Khanna et al., 2012). Moreover, there are specific cultural variations (e.g., willingness to receive or ask for support) that can drive older adults’ underutilization of health services, which has prompted researchers to recognize the importance of patients’ cultural norms and worldviews (Kim et al., 2008; Mojaverian et al., 2012). Type and frequency of social support can also vary across racial and ethnic groups due to context and cultural norms (Ishii et al., 2017).
The present study explores the impact of social support among a racially, ethnically, and linguistically diverse sample of older adults in the context of a randomized controlled trial aimed at improving mental health and physical functioning (Alegría et al., 2019). We examined whether social support was associated with treatment adherence defined in two ways: by the number of treatment sessions attended and completing the recommended number of sessions. Although there are many dimensions and parameters of social support, in this study, we distinguished between the two main types according to Feeney and Collins (2015), using definitions from Finfgeld-Connett (2005): emotional (defined as the availability of family and friends to discuss problems) and instrumental (defined as the availability of family and friends to help with practical things). We hypothesized that (1) higher levels of emotional social support would be associated with greater treatment adherence for the mental health intervention and (2) higher levels of instrumental social support would be associated with greater treatment adherence for the physical exercise intervention. This study aims to inform our understanding of the role of social support on uptake and effect of disability interventions and of reported differential outcomes in disability prevention.
Methods
Setting and Sample
This study used secondary data from a multisite randomized controlled trial assessing the effectiveness of Positive Minds-Strong Bodies (PMSB), an intervention aimed at improving mental health and physical functioning among U.S. minority older adults. A full description of the intervention and a report of its findings have been published elsewhere (Alegría et al., 2019). Participants were recruited from community-based organizations (CBOs) and clinical sites in Massachusetts, New York, Florida, and Puerto Rico, which serve predominantly low-income racial/ethnic minority and immigrant older adults. Data collection occurred between May 2015 and March 2019. The trial was approved by the institutional review boards of Massachusetts General Hospital/Partners HealthCare and New York University, with ceded reviews for partnering CBOs. All participants established capacity to consent and provided informed consent.
Eligible participants were aged 60+ years; spoke English, Spanish, Mandarin, or Cantonese; had mild to severe anxiety or depressive symptoms—scored five or more on either the Patient Health Questionnaire (PHQ-9 (Kroenke & Spitzer, 2002), the Generalized Anxiety Disorder 7-item Scale (GAD-7 (Spitzer et al., 2006), or the Geriatric Depression Scale (GDS-15 (de Craen et al., 2003)—and had minor to moderate disability—scored between 3 and 11 on the Short Physical Performance Battery (SPPB (Guralnik et al., 1994). Participants were excluded from the trial if they screened positive for substance use disorders; attended mental health treatment within the prior 3 months or had an appointment within the next month; lacked capacity to consent; were homebound; had a neuromusculoskeletal impairment; or did not receive physician medical clearance for exercise.
Procedure
Of the 1057 potential participants screened, 381 were eligible and 307 completed the 2-hour baseline assessment for $25 compensation and were randomized to either the intervention (N = 153) or control condition (N = 154; see CONSORT diagram from the randomized controlled trial) (Alegría et al., 2019). Participants completed follow-up interviews at 2 and 6 months ($25 compensation each) and a final post-intervention follow-up at 12 months ($50 compensation) after the baseline. Since the present study examines whether higher levels of social support (described below) were associated with increased attendance to the intervention sessions, the final analytical sample uses only the 153 participants randomized to the intervention group. Assessments in the intervention condition were administered in English (N = 35), Spanish (N = 66), Mandarin (N = 24), or Cantonese (N = 28), based on participant preference.
Positive Minds (PM), adapted from the CERED intervention (Alegría et al., 2014), is a psychosocial intervention focused on psychoeducation, cognitive restructuring, managing unhelpful thoughts, and creating a self-care plan. PM consists of 10 one-hour individual CBT sessions over a 6-month period. Strong Bodies (SB), adapted from the InVEST intervention (Bean et al., 2004), is an exercise training program designed for elders involving 10 functional exercises with three sets of 10 repetitions each. SB consists of three sessions per week over 12–14 weeks for a total of 36 sessions. PM was administered by community health workers (CHWs), SB was administered by exercise trainers, and both were supervised by the trial principal investigators (Alegría et al., 2019). The intervention sessions were held at the CBOs, clinics, in participants’ homes, or, for PM, by phone (location depending on participant preference and accessibility).
Measures
Outcomes
Our four primary outcome variables were as follows: (1) the total number of PM sessions attended (M = 7.79 ± 3.61), (2) the total number of SB sessions attended (M = 14.93 ± 15.75), (3) a binary variable equal to one if the participant attended six or more PM sessions and equal to zero otherwise (M = 77.63% ± 41.81%), and (4) a binary variable equal to one if the participant attended 25 or more SB sessions and equal to zero otherwise (M = 49.15% ± 50.21%). Six PM sessions and 25 SB sessions have been determined as the minimum threshold for significant treatment adherence for mental health and physical functioning outcomes, respectively (Alegría et al., 2019).
Social support
Social support was assessed using seven items about quantity and quality of social support (Thoits, 1995) from the baseline assessment. Two of these items measured quantity and quality of social support from spouse/partner, but only 36.6% of participants in the sample (N = 56) were either married or cohabitating, leading to a significant amount of missing data in these two items. Thus, social support from spouse/partner was not included in the present study, and instead, all analyses adjusted for marital status (married/cohabitating, separated/divorced, widowed, and never married).
Consistent with previous literature distinguishing between two main types of social support (Finfgeld-Connett, 2005), we categorized the remaining five items into two different indicators of social support. (1) Emotional social support consisted of three items about frequency of discussing problems with family and friends; items were rated on a 4-point scale (0 = never and 3 = always) with a total score averaging the three items (range: 0–3; higher scores represent more emotional support; reliability score (Cronbach’s alpha) α = .60). (2) Instrumental social support involved two items assessing whether participants could depend on either relatives or neighbors/friends for help with practical things (1 = yes and 0 = no), with a total score averaging the two items (range: 0–1; higher scores represent more instrumental support; α = .37). The low reliability scores of our social support indicators—particularly instrumental social support—were most likely influenced by the low number of items with very few response options, as well as our small sample size. We conducted our analyses within the context of this limitation.
Additional covariates
We included as covariates baseline demographic and clinical characteristics that could be potentially correlated with the outcomes: age (60–64 years, 65–74 years, and 75 years or older), gender (male and female), race/ethnicity (White/Caucasian, Black/African/African American, American Indian, Hispanic, and others), educational attainment (less than high school, high school, or more), marital status, anxiety symptoms, and depressive symptoms.
Anxiety symptoms were measured using the GAD-7, a 7-item self-reported screening tool to assess symptom severity of generalized anxiety disorder (GAD) (Spitzer et al., 2006). Respondents were asked how often, during the last 2 weeks, they were bothered by each symptom; responses are rated on a 4-point scale (0 = not at all and 3 = nearly every day), and total scores were calculated summing all items (range: 0–21; higher scores represent worse symptoms; α = .83 overall, and .78, .77, .74, and .94 in English, Spanish, Mandarin, and Cantonese, respectively).
Depressive symptoms were measured using the PHQ-9, a 9-item self-reported screening tool corresponding to DSM-IV symptom criteria for major depression (Kroenke & Spitzer, 2002). Items were rated on a 4-point scale (0 = not at all and 3 = nearly every day), and total scores were calculated summing all items (range: 0–27; higher scores indicate worse symptoms; α = .72, and .63, .62, .61, and .92 in English, Spanish, Mandarin, and Cantonese, respectively)
We summarized all measures included in the present study among the 153 participants in the intervention group using means and SE for continuous variables and reporting frequencies for categorical variables. We examined the relationship between the two indicators of social support and the two continuous outcomes (i.e., number of PM sessions and number of SB sessions) using linear regression models. We examined the relationship between the two indicators of social support and the two binary outcomes (i.e., attended 6+ PM sessions and attended 25+ SB sessions) using logistic regression. All models adjusted for age, gender, race/ethnicity, education, marital status, and baseline anxiety (GAD-7) and depression (PHQ-9) scores. All analyses were conducted using Stata 15 (StataCorp, 2017) and two-sided design-based tests at α = .05 level for statistical significance. All analyses using PM excluded one participant who was not offered the PM sessions, and all analyses for SB excluded 35 participants who were not offered the SB sessions—no facilities were available to deliver the exercise sessions after hurricanes hit towns at two sites.
Results
Baseline characteristics of the intervention sample (N = 153).

Note: M = Mean; SE = standard error; GAD-7 = Generalized Anxiety Disorder Scale (Spitzer et al., 2006); PHQ-9 = Patient Health Questionnaire for depression (Kroenke & Spitzer, 2002).
Relation between social support and attendance of Positive Minds (PM) sessions.
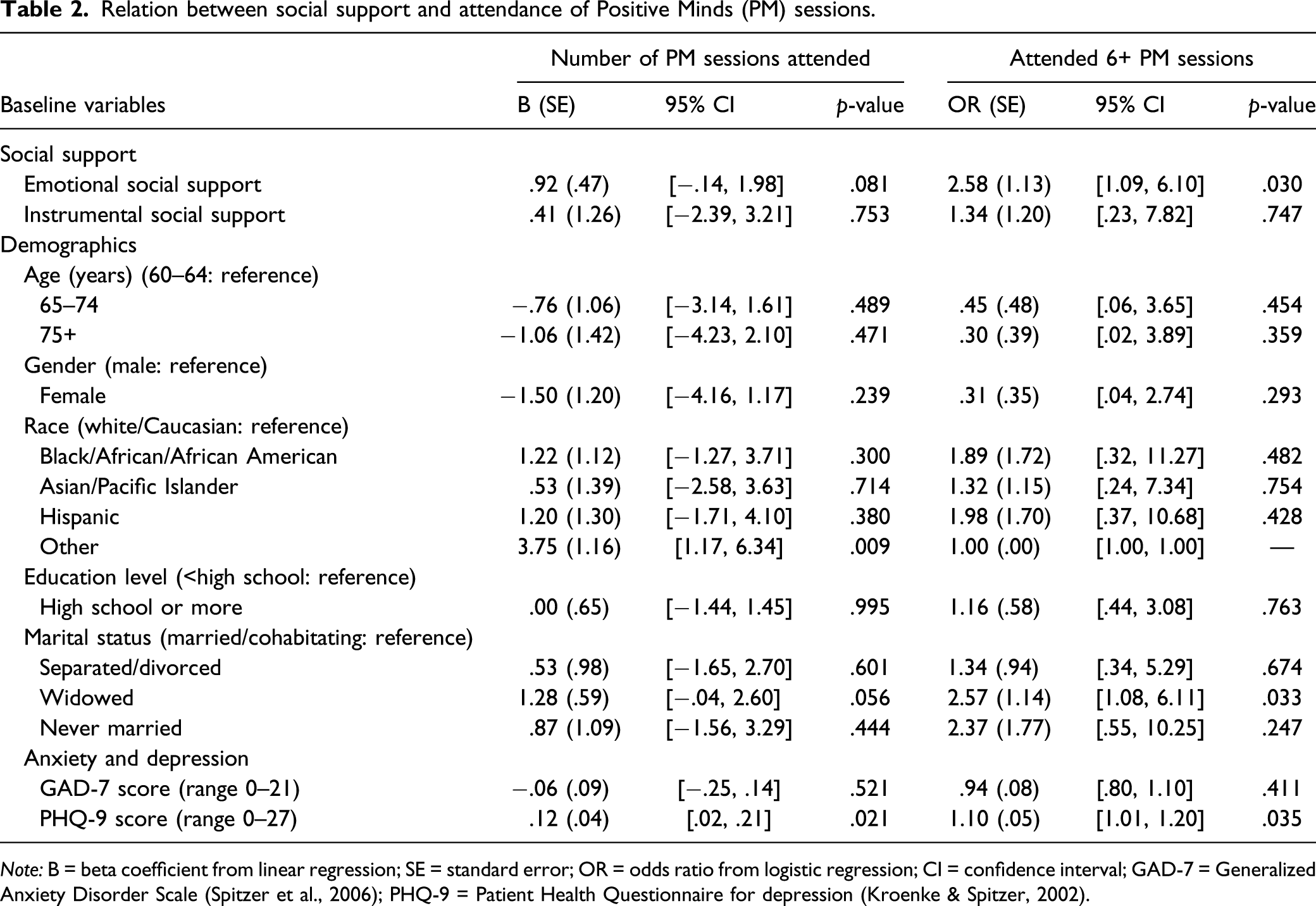
Note: B = beta coefficient from linear regression; SE = standard error; OR = odds ratio from logistic regression; CI = confidence interval; GAD-7 = Generalized Anxiety Disorder Scale (Spitzer et al., 2006); PHQ-9 = Patient Health Questionnaire for depression (Kroenke & Spitzer, 2002).
Relationship between social support and Strong Bodies sessions.
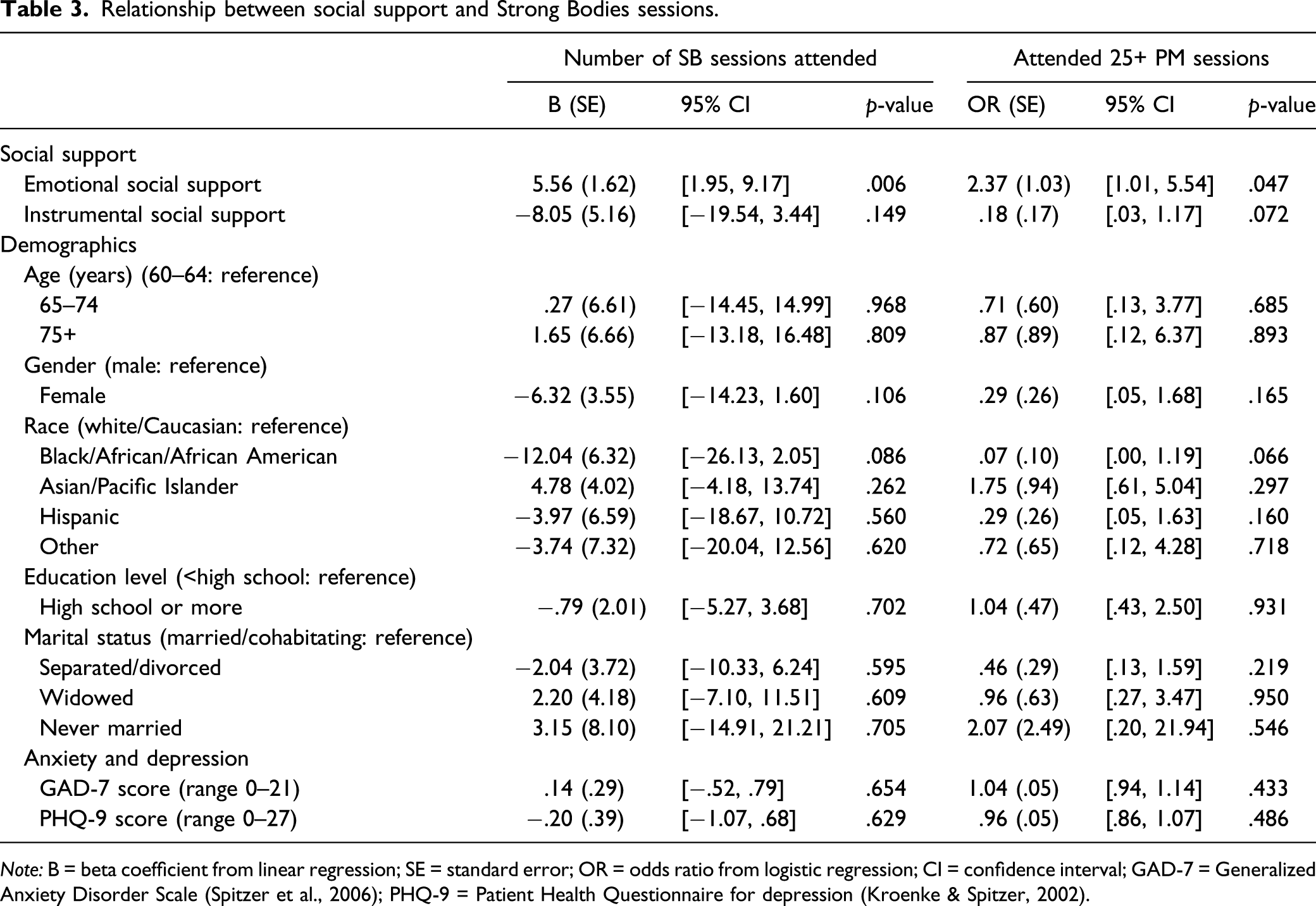
Note: B = beta coefficient from linear regression; SE = standard error; OR = odds ratio from logistic regression; CI = confidence interval; GAD-7 = Generalized Anxiety Disorder Scale (Spitzer et al., 2006); PHQ-9 = Patient Health Questionnaire for depression (Kroenke & Spitzer, 2002).
Discussion
Our results underscore the importance of social support for older adults’ adherence in mental and physical health preventive interventions. Consistent with our first hypothesis, individuals with higher levels of emotional social support at the outset of the intervention were more likely to complete the mental health intervention. This finding is in line with prior research indicating that greater social support is associated with more participation in psychotherapy (Al-Asadi et al., 2014; Ayuso-Mateos et al., 2007). While we did not examine mediators, one possible explanation is self-efficacy. Maeda et al. (2013) identified that self-efficacy fully mediated the effect of social support on treatment adherence after controlling for common covariates. They suggested that people with greater levels of social support have a wider range of external resources for encouragement, learning about resources, setting norms, and modeling proper disease management, which might increase their self-efficacy. In the case of chronic illness, multiple studies have shown that social support can help to minimize the negative effects of the illness (Berkman et al., 2014; Bloom et al., 2001; Cohen et al., 2000; Cohen & Wills, 1985). But our results highlight the importance of emotional support to assure that older adults obtain a sufficient adherence of an intervention.
Contrary to our expectations, instrumental social support was neither associated with the number of exercise sessions nor with completing the full exercise intervention. We found nonetheless that individuals with higher levels of emotional social support at the outset of treatment were likely to attend more exercise sessions for physical health and complete the full exercise intervention. The lack of significance regarding instrument social support may be due to the overall low levels of completing the exercise intervention in the study sample (49%). In qualitative interviews, participants indicated that transportation barriers, bad weather, and complicated family demands sometimes made it difficult to participate in all 36 exercise sessions (Porteny et al., 2020). Our results indicate that the amount of instrumental support received was likely not enough to offset these barriers. Older adults of color, like the ones involved here, might prioritize family demands over their personal physical activity, as is suggested by research on self-care among older adults in four ethnic minority groups (Gallant et al., 2010). It might also be explained by the changes in social relations that occur in later life, whereas for many, lifestyle changes such as physical activity occur in a context of friends and family members (Fleury et al., 2009). This finding is in line with the work of Barrera et al. (2006) who identified that social support systems are embedded in cultural factors and social norms that are further linked to health behavior change. Clinical trials that directly measure specific social support features, such as the nature of relationships (partners, children, and friends), are still relevant for understanding how social support influences individual compliance with health preventive behaviors and/or treatments among older adults.
As social distancing continues to prevent spreading the coronavirus, it is critical now more than ever to provide social support for older adults. We know that isolation and loneliness can be very damaging for the physical and mental health of older adults, worsening the risk for depression, anxiety, poorer cognitive function, and weakened immune system (Cacioppo & Cacioppo, 2014; National Institute on Aging, 2019). As outpatient mental and physical health care transitions from in-person to telehealth delivery, we need to know what factors can contribute to signing up, participating, and completing health prevention and treatment programs. The need for providing extra supports for participation in health interventions is particularly urgent for older people of color, immigrants, linguistic minorities, and low-SES communities, who are disproportionately affected from health and financial impacts of the COVID-19 outbreak compounding long-term racial and income disparities (Artiga et al., 2020; Garg et al., 2020). It might be that now the need includes getting support to enable the virtual sessions.
Our findings need to be interpreted in the context of the study strengths and limitations. Racial and ethnic minorities of all ages are vastly underrepresented in clinical trials of all kinds (Food and Drug Administration, 2020; Regnante et al., 2019); the PMSB trial is one of the few trials of mental health or exercise programs in the United States with a diverse sample of racial and ethnic and linguistic minority older adults. This study adds to our understanding of factors that influence racial and ethnic minority older adults’ participation in trials of healthcare treatment by identifying social support, and particularly emotional support, as a facilitator of participating and completing the mental health and exercise program. The ethnic, racial, and geographic diversity of the sample also adds complexity to interpreting the results.
Social support poses a particular challenge in this diverse sample due to cultural differences in seeking support when confronted with a problem (Ishii et al., 2017; Kim et al., 2008). Given our small sample, we did not have enough power to test interaction effects of race/ethnicity and social support, but future research should assess for potential interactions. Another limitation of this study is the generalizability of the sample, which came from a clinical trial. Low social support may have impeded trial eligibility, if people did not have sufficient family or friend support to accompany them to the community agencies or clinics where recruitment was done. Social support may influence willingness to participate in the trial as more social support could make participants more inclined to do a group activity (Foley et al., 2019) or more inclined to seek out health related information, as hypothesized by Sellars et al. (2010). However, in Sellars et al. (2010) study, social support was not found to be associated with willingness to participate in medical research, suggesting more research is needed to clarify this relationship.
Measurement of social support is another key consideration, particularly when assessing different types of social supports among a diverse population. While we did assess different types of social support, more comprehensive assessments of social support may have resulted in more precise estimates of impact. As we mentioned in the Measures section, the reliability scores of our social support indicators were low—most likely the result of a low number of items with very few response options within each indicator. Given an overall small sample, limited sample size within each language group was also likely the reason for the low reliability scores in the PHQ-9 in English, Spanish, and Mandarin. Future studies examining the effect of social support on treatment participation and adherence among older adults should not only recruit larger samples but should also include more complex measures of social support. Multidimensional assessments (e.g., combining emotional, instrumental, structural, and functional support) may have increased psychometric reliability and validity because they can better capture the multiple influences of social relationships (Holt-Lunstad & Smith, 2012; Uchino, 2006). Despite the limitations mentioned, this study is one of the few studies examining social support and treatment adherence in a diverse sample of racial and ethnically diverse older adults. Our findings highlight the need for continued evaluation of the impacts of social support on treatment adherence across diverse populations, and our findings also suggest that further work is needed to identify measurement approaches that enable comprehensive assessments of social support that are appropriate for diverse populations.
Conclusion
Developing and testing interventions, building the body of evidence that documents their effectiveness, and ensuring their dissemination are important aspects of the research enterprise. These efforts fall short, however, if we lack the understanding of how to achieve the uptake and intended therapeutic adherence of interventions in ethnic and racial minority elders. Strategies are needed to ensure that individuals with low social support participate in and complete health interventions, and particularly as we move toward telehealth interventions, in contexts of limited in-person social contact imposed by the current pandemic. This study suggests that social support might be an important factor influencing the adherence of mental health and physical health interventions. Future intervention research could adjust the implementation of an intervention to the social support of participants at baseline to support treatment adherence and identify effective strategies that reduce differential uptake and treatment completion among older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging and the National Institute of Mental Health under grant number R01AG046149. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Data Availability Statement
The data upon which this study is based are available upon request to the author.