
Abstract
Keywords
Introduction & Background
Although decline in physical function is part of the aging process, the prevalence of functional limitations varies across racial and ethnic groups (Warner and Brown, 2011). For example, despite evidence of Hispanic/Latino (hereafter “Hispanic”) populations in the United States having longer life expectancy at birth and at age 65 than the general U.S. population (Arias, 2016; Lariscy, Nau, Firebaugh, and Hummer, 2016), Hispanic groups have higher rates of functional limitation and disability than the general population, suggesting they live longer with poorer health and worse health-related quality of life (Cantu et al., 2013; Chinn & Hummer, 2016; Dunlop et al., 2007; Tirodkar et al., 2008).
The Hispanic population is fast growing but heterogeneous, comprising individuals of Mexican (62%), Puerto Rican (10%), Central American (9%), South American (6%), Cuban (4%), Dominican (3%), and other Hispanic (5%) origins (US Census Bureau, 2019). Studies have quantified significant variation in morbidity and mortality among Hispanic subgroups based on differences in nativity and race (Cantu et al., 2013; Chinn & Hummer, 2016; M. A. Garcia, Garcia, Chiu, Raji, & Markides, 2018), primary language spoken (Dunlop et al., 2007; Tirodkar et al., 2008), gender (Garcia, Garcia, Chiu, Raji, & Markides, 2018; Mueller & Bartlett, 2019), and morbidity type (Spencer et al., 2008). For example, Cantu and colleagues (2013) found that U.S.-born Hispanic adults age 50 and older experienced a greater proportion of functional limitations and chronic conditions compared to non-Hispanic White adults of similar age, while foreign-born Hispanic adults experienced lower rates of mortality, functional limitations, and chronic conditions. Another study investigating activities of daily living (ADL) found that Spanish-speaking Hispanic participants reported greater rates of lower-extremity dysfunction, but lower rates of walking disability compared with other racial/ethnic groups (Tirodkar et al., 2008). Using Health and Retirement Survey data, Dunlop and colleagues (2007) found that Hispanic adults interviewed in Spanish had a substantially higher risk of developing ADL difficulties compared with Hispanic adults interviewed in English. Garcia et al. (2018) found that among females, U.S.- and foreign-born Mexicans and island-born Puerto Ricans spent more years during later life with morbidity than Whites, while among males, U.S.-born Puerto Ricans were the only group who spent more years of later life with morbidity than Whites; foreign-born Cubans exhibited the least morbidity regardless of gender (Garcia, Garcia, Chiu, Raji, & Markides, 2018). In a separate study, Garcia et al. (2018) found that foreign-born Mexicans, Cubans, and Central/South Americans, regardless of gender, experienced an “immigrant advantage” for heart disease and cancer compared with non-Latino Whites, whereas island-born Puerto Ricans and U.S.-born Puerto Ricans and Mexicans had higher levels of morbidity (Garcia, Garcia, & Ailshire, 2018).
Cumulative Disadvantage
This study is informed by a cumulative disadvantage theoretical framework which suggests that disparate accumulation of and ability to accrue human capital over the life course result in inequalities in older age (Crystal & Shea, 1990). Societal and institutional structures such as racism or poverty can reduce an individual’s ability to accrue human capital (e.g., education or wealth), which in turn negatively impacts life outcomes over time (Crystal et al., 2017). Studies have found that Hispanic populations disproportionately have poorer health outcomes, including higher rates of non-communicable disease, obesity, teen pregnancy, tobacco use, and death compared with other racial/ethnic groups, in part due to social and structural factors that negatively impact human capital including income, educational attainment, occupation, lack of health insurance, and lower utilization and quality of healthcare services (Valdez and Arce, 2000; Escarce and Kapur, 2006). These cumulative disadvantage factors are exacerbated by anti-immigrant stigma (Morey, 2018), and further complicated by issues related to assimilation (Turra & Goldman, 2007).
Most research on health, physical functioning, disability, and health-related quality of life has treated Hispanics as a homogeneous group (Garrett et al., 2013; Howard et al., 2014; Huisingh-Scheetz et al., 2013; Shetterly, Baxter, Morgenstem, Grigsby, & Hamman, 1998; Shih et al., 2005; Spencer et al., 2008). However, the presence of significant heterogeneity in morbidity, mortality, and functional limitations among U.S. Hispanic subgroups (Garcia, Garcia, Chiu, Raji, & Markides, 2018) may have important public health implications.
We therefore examined heterogeneity in functional limitations and health-related quality of life among racially and ethnically diverse older adults and among subgroups of Hispanic older adults. Consistent with the cumulative disadvantage framework and observed heterogeneity in the Hispanic population, we hypothesized that compared to non-Hispanic Whites, racial and ethnic minority older adults would have more functional limitations and lower physical health-related quality of life. We also anticipated significant variation in these outcomes across Hispanic subgroups.
Research Design and Methods
Data and Sample
We analyzed baseline data from 2011 to 2015 Centers for Medicare and Medicaid Services (CMS) Health Outcomes Survey (HOS) Limited Data Sets. The HOS is a panel survey of racially and ethnically diverse participants enrolled in Medicare Advantage (MA) plans. More than four in 10 Medicare beneficiaries are currently enrolled in MA plans (Freed et al., 2021). The HOS is a self-administered mail survey with a 2-year telephone follow-up in English and Spanish, and a mail-only protocol for Chinese respondents. We included respondents with complete data for race, ethnicity, ADLs, physical health score, and covariates. We excluded respondents with CMS indicators for receipt of hospice care or institutionalization, and diagnosis of end-stage renal disease. Our final sample consisted of 828,946 community-dwelling HOS respondents aged 65 and older.
Dependent Variables
Functional limitations were measured by six indicators of ADL difficulty (Katz et al., 1963). Respondents were asked about any difficulty with the following activities without specific equipment or help from another person: bathing, dressing, eating, getting in and out of chairs (“transitioning”), walking, and using the toilet (“toileting”). We defined ADL difficulty as responding, “Yes, I have difficulty” or “I am unable to do this activity,” and no ADL difficulty as responding, “No, I do not have difficulty.” We also examined functional limitations as any ADL difficulty (i.e., having any difficulty in one or more ADLs), and as the number of ADL difficulties among all participants (possible range of 0–6) and among participants with at least one ADL difficulty (range of 1–6).
Physical health was measured by the Physical Component Summary (PCS) score, a self-reported measure for physical health-related quality of life (Lins & Carvalho, 2016). PCS scores are derived from the Veterans RAND-12 Item Health Survey, a validated short-form version of the SF-36 Health Survey (Preedy & Watson, 2010). PCS scores range from 0 to 100, where higher scores indicate better physical health (Preedy & Watson, 2010).
Main Independent Variables
Our main independent variables were self-reported race and Hispanic ethnicity, derived from two separate questions in the HOS. Respondents were first asked, “Are you of Hispanic, Latino/a, or Spanish origin?” and were next asked “How would you describe your race?” Respondents were allowed to select multiple categories for both the Hispanic ethnicity and race questions. Participants who answered “yes” to any category of the Hispanic ethnicity question were categorized as Hispanic. We also constructed 11 more detailed, mutually exclusive categories: (1) non-Hispanic White, (2) non-Hispanic Black or African American, (3) non-Hispanic Asian, (4) non-Hispanic American Indian or Alaskan Native (AIAN), (5) non-Hispanic Native Hawaiian or other Pacific Islander (NHPI), (6) non-Hispanic Multiple Race (respondents who selected two or more racial groups), (7) Mexican (i.e., Mexican, Mexican American, Chicano/a), (8) Puerto Rican, (9) Cuban, (10) Other Hispanic (respondents who selected “another Hispanic, Latino/a, or Spanish origin”), and (11) Multiple Hispanic (i.e., respondents who selected two or more Hispanic, Latino/a, or Spanish categories). We imputed missing baseline responses for race and ethnicity using follow-up responses where data were available.
Cumulative Disadvantage Variables and Covariates
Consistent with the cumulative disadvantage framework, we adjusted for sociodemographic variables: age, sex, marital status, educational attainment, household income, and language of HOS administration. We also adjusted for body mass index (BMI), and number of chronic conditions. Marital status was coded as married, divorced or separated, widowed, or never married. Educational attainment had four response categories: did not graduate from high school, high school graduate or General Education Development (GED), some college or 2-year degree, and 4-year college degree or more. Household income was a categorical variable coded as: less than $10,000, $10,000 to $19,999, $20,000 to $29,999, $30,000 to $49,999, and $50,000 or more. Language of HOS administration was English, Spanish, or Chinese. BMI was categorized as underweight (<18.5 kg/m2), normal (≥ 18.5 kg/m2 and < 25 kg/m2), overweight (≥ 25 kg/m2 and < 30 kg/m2), and obese (≥ 30 kg/m2). Number of chronic conditions was a count of the total number of self-reported chronic medical conditions, and ranged from 0 to 15. Chronic conditions counted were: hypertension or high blood pressure, angina pectoris or coronary artery disease, congestive heart failure, myocardial infarction or heart attack, other heart conditions (i.e., problems with heart valves or heartbeat rhythms), stroke, emphysema or asthma or chronic obstructive pulmonary disease, Crohn’s disease or ulcerative colitis or inflammatory bowel disease, arthritis of the hip or knee, osteoporosis, sciatica, diabetes, depression, and any cancer.
To examine cumulative disadvantage in more depth, we conducted sensitivity analyses in which regression models did not control for socioeconomic status (educational attainment and household income). It was hypothesized that racial and ethnic disparities would be wider in the models without socioeconomic status.
Analytic Approach
We computed summary statistics for all outcomes and independent variables by racial and ethnic group and Hispanic subgroup. We utilized linear models to estimate PCS score, and linear probability models to estimate the probability of having a specific ADL difficulty and probability of having any ADL difficulty, by racial and ethnic group and Hispanic subgroup. We used Poisson models to estimate the total count (i.e., number) of ADL difficulties among the subset of the study population who reported one or more ADL difficulties (n = 291,607). We controlled for age, sex, marital status, educational attainment, household income, language of HOS administration, BMI, and number of chronic conditions in all regression analyses. In all models, we computed robust standard errors using the sandwich estimator.
Results
Respondent Characteristics
Supplemental Appendix A presents descriptive statistics for the study population (n = 828,946), which was 74.2% White, 8.6% Black or African American, 3.5% Asian, .2% AIAN, .3% NHPI, 2.1% multiple race, and 11.1% Hispanic. The mean age was 74.0 years. All minority groups except the Cuban Hispanic subgroup were younger on average than Whites.
Over half of respondents (56.1%) were female. White and Asian respondents were less often female than were Black, AIAN, NHPI, multiple race, or Hispanic respondents. More than half of respondents were married (54.2%). White and Asian respondents were more likely to be married, and less likely to be divorced or separated than were respondents from Hispanic subgroups or other racial groups.
Approximately one in five respondents (21.1%) had attained at least a bachelor’s degree. Asian respondents were most likely to have a bachelor’s degree or higher (34.5%), followed by White respondents (23.7%). Hispanic (10.2%) and AIAN (9.5%) respondents were least likely to have completed college. White respondents were most likely (24.6%) to report household incomes of $50,000 or more, and least likely (8.8%) to report household incomes less than $10,000. Asian respondents reported the next-highest incomes, followed by respondents from other racial groups. Hispanic respondents were least likely (6.9%) to report household incomes over $50,000 and most likely (34.7%) to report household incomes below $10,000.
The overall prevalence of being overweight or obese was 68.4%. Asian respondents were least likely to be overweight or obese (38.1%). Prevalence of overweight or obesity among other racial/ethnic groups ranged from 68.3% for White respondents to 76.0% for Black respondents. Respondents reported a mean of 3.2 chronic conditions. Asian respondents reported the lowest number of chronic conditions (2.8) followed by White (3.1) and other racial/ethnic group respondents (≥ 3.5).
Among Hispanic respondents, approximately 2 in 5 were either Mexican (22.2%) or Puerto Rican (21.9%); 5.2% were Cuban, 3.4% multiple Hispanic, and 47.3% other Hispanic. Rates of being female, married, or divorced/separated varied less among Hispanic subgroups than among racial groups. More than half of all Hispanic respondents (53.2%) had less than a high school education. The Cuban subgroup had the lowest proportion not completing high school (43.4%) and the highest proportion completing college (18.1%); the Mexican subgroup had the highest proportion without a high school education (60.9%) and the smallest proportion with a bachelor’s degree or higher (5.4%). Household incomes were highest for Cuban respondents and lowest for Puerto Rican respondents. Prevalence of overweight or obesity ranged from 69.9% for other Hispanic respondents to 76.0% for Mexican respondents. The mean number of chronic conditions ranged from 3.5 for Mexican and other Hispanic respondents to 4.0 for Puerto Rican respondents.
Prevalence of Activities of Daily Living Difficulty
Health-Related Quality of Life (N = 828,946), Proportion With any Activities of Daily Living Difficulty (N = 828,946), and Number of Activities of Daily Living Difficulties among Beneficiaries With 1+ Difficulties (N = 291,607), by Race, Ethnicity, and Hispanic Subgroup.

Note. Black = Black or African American, AIAN = American Indian or Alaskan Native; NHPI = Native Hawaiian or Pacific Islander; PCS = Physical Component Score (quality of life); ADL = activities of daily living.
Among Hispanic subgroups, respondents who identified as multiple Hispanic ethnicities had the lowest mean PCS score (35.4%) and the highest proportion reporting ADL difficulties (46.8%), as well as the highest mean number of ADL difficulties (1.4) and the highest number of ADL difficulties among respondents reporting more than one (3.0). Cuban respondents had the highest mean PCS score as well as the lowest prevalence and number of ADL difficulties. Mexican respondents had the second-highest mean PCS score among Hispanic subgroups, and the second-lowest prevalence and number of ADL difficulties.
Figure 1 shows the prevalence of ADL difficulties by race and Hispanic ethnicity, and by Hispanic subgroup. The overall prevalence of difficulty walking was the highest of any ADL at 30.5%; it was 25.6% for Asians, 28.6% for Whites, and more than 35% for all other racial groups and Hispanic subgroups. The overall prevalence of difficulty transitioning was 21.1%; it was 16.5% for Asians, 19.4% for Whites, and more than 24% for all other racial groups and Hispanic subgroups. The overall prevalence of difficulty bathing was 14.2%; it was 12.4% for Whites, 13.9% for Asians, and more than 17% for all other racial groups and Hispanic subgroups. The overall prevalence of difficulty dressing was 11.4%; it was 9.6% for Whites, 11.4% for Asians, and more than 15% for all other racial groups and Hispanic subgroups. The overall prevalence of difficulty toileting was 8.4%; it was 6.9% for Whites, 9.9% for Asians, and more than 11% for all other racial groups and Hispanic subgroups. The overall prevalence of difficulty eating was the lowest of any ADL at 4.7%; it was 3.7% for Whites and more than 6% for all other racial groups and Hispanic subgroups. Prevalence of activities of daily living difficulty by race, ethnicity, and Hispanic subgroup (n = 828,946). Note. AIAN = American Indian/Alaska Native, NHPI = Native Hawaiian/Pacific Islander.
Native Hawaiian or other Pacific Islander respondents had highest rate of any ADL difficulty (48.0%), and higher difficulty rates than any other racial group or Hispanics for 4 of 6 ADLs (walking, transitioning, bathing, and dressing). Hispanic respondents had higher difficulty rates for toileting and eating than any racial group.
Among Hispanic subgroups, multiple Hispanic respondents had the highest rates of difficulty for four of six total ADLs (bathing, dressing, toileting, and eating), and Puerto Rican respondents had the highest rates for difficulty walking and transitioning. Cuban respondents reported the lowest difficulty rates for all six ADLs, and Mexican respondents the second-lowest rates for five of the six ADLs (except bathing).
Factors Associated with Differences in Activities of Daily Living Difficulty
Health-Related Quality of Life (N = 828,946), Probability (Percentage Points) of any Activities of Daily Living Difficulty (N = 828,946), and Number (Predicted Count) of Activities of Daily Living Difficulties among Beneficiaries With 1+ Difficulties (N = 291,607), by Race, Ethnicity, and Hispanic Subgroup.
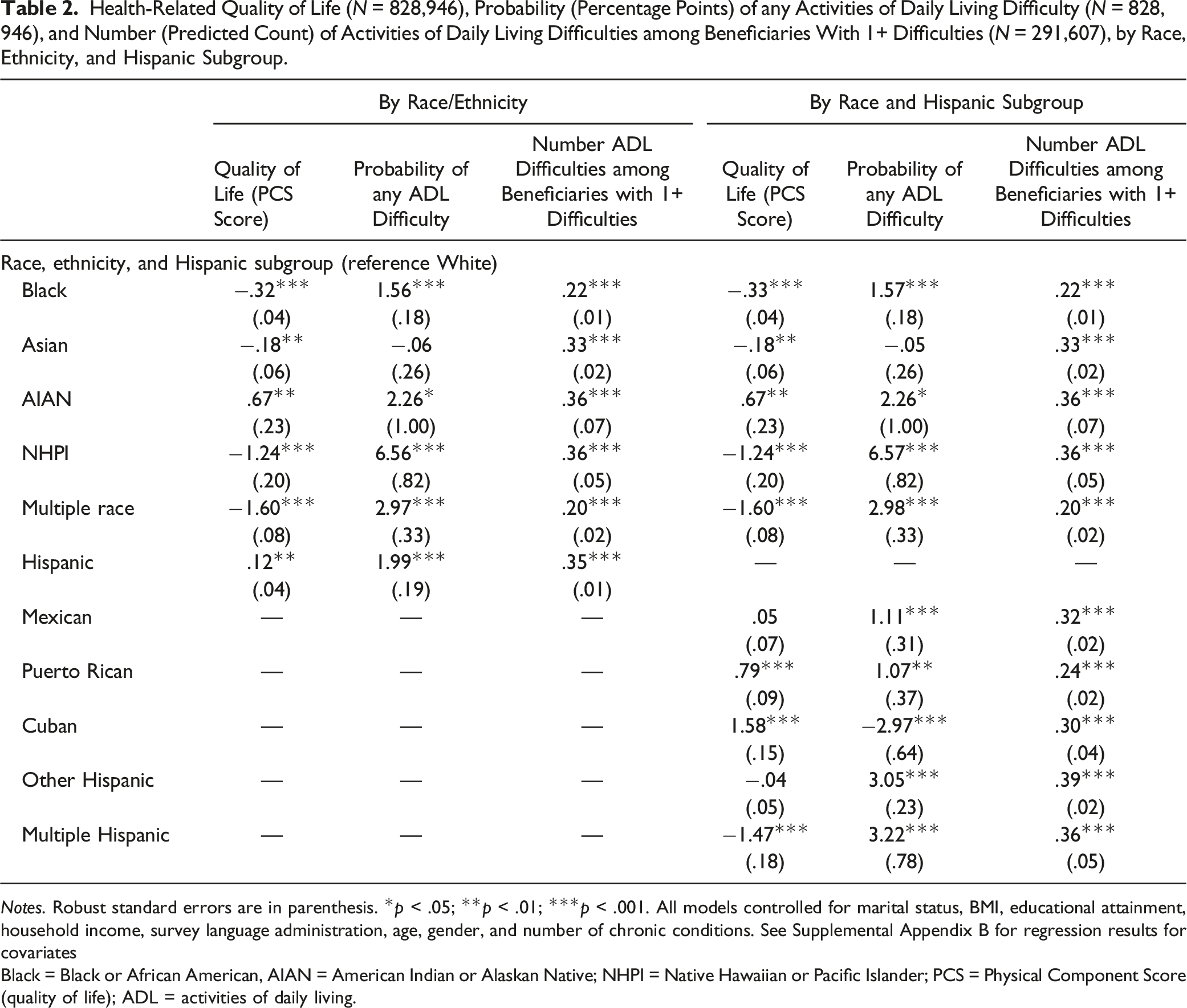
Notes. Robust standard errors are in parenthesis. *p < .05; **p < .01; ***p < .001. All models controlled for marital status, BMI, educational attainment, household income, survey language administration, age, gender, and number of chronic conditions. See Supplemental Appendix B for regression results for covariates
Black = Black or African American, AIAN = American Indian or Alaskan Native; NHPI = Native Hawaiian or Pacific Islander; PCS = Physical Component Score (quality of life); ADL = activities of daily living.
Among Hispanic subgroups (columns four through six of Table 2), Cuban respondents had the highest mean PCS score (1.58 units higher than White respondents, p < .001) after controlling for cumulative disadvantage factors, while only multiple Hispanic respondents had PCS scores significantly lower (−1.47 units, p < .001) than White respondents. Cuban respondents also had the lowest probability of having any ADL difficulty (2.97 percentage-points lower than White respondents, p < .001); all other Hispanic subgroups were more likely than White respondents to have any ADL difficulty. Among respondents who had at least one ADL difficulty, members of all Hispanic subgroups had a higher mean number of ADL difficulties than White respondents.
Probability (Percentage Points) of Activities of Daily Living Difficulty by Type of Activities of Daily Living Difficulty, and by Race, Ethnicity, and Hispanic Subgroup (N = 828,946).

Notes. Robust standard errors are in parenthesis. *p < .05; **p < .01; ***p < .001. All models controlled for marital status, BMI, educational attainment, household income, survey language administration, age, gender, and number of chronic conditions. See Supplemental Appendix C for regression results for covariates
Black = Black or African American, AIAN = American Indian or Alaskan Native; NHPI = Native Hawaiian or Pacific Islander; PCS = Physical Component Score (quality of life); ADL = activities of daily living.
Among Hispanic groups (last six columns of Tables 3), Cuban respondents were less likely than White respondents to have difficulty walking (−2.76 percentage-points, p < .001) and transitioning (−1.83 percentage-points, p < .01), and equally likely to have difficulty bathing. Cuban respondents also had lower estimated probabilities of difficulty dressing, toileting, or eating than other Hispanic subgroups. All other Hispanic subgroups were more likely than White respondents to have difficulty with every ADL (except for two ADL-subgroup cells where results differences were not significant). Mexican respondents had the second-lowest rates of difficulty among Hispanic subgroups for walking, transitioning, bathing, and dressing; Puerto Rican respondents had the second-lowest rates among Hispanic subgroups for difficulty toileting and eating. Multiple Hispanic respondents had higher rates of difficulty bathing, dressing, toileting, and eating than any other Hispanic subgroup.
Sensitivity Analyses
Regression models for PCS score, probability and number of ADL difficulties, and type of ADL difficulty were re-estimated without socioeconomic status variables (Supplemental Appendices D and E). In these models, the magnitude of all disparities between racial or ethnic minority groups and the White reference group increased compared to the base models. For example, the differential probability of any ADL difficulty among Hispanic (compared White) respondents more than tripled, from 1.99 to 6.47 percentage-points. For some groups and some outcomes, statistical significance also changed, always in the direction of increased disparity.
Discussion and Implications
This study analyzed HOS data to examine functional limitations and health-related quality of life among Medicare Advantage beneficiaries 65 years and older using a cumulative disadvantage framework. Consistent with that framework, White and Asian respondents were the least disadvantaged groups and had lower unadjusted rates of ADL difficulties and higher PCS scores than other racial groups or Hispanic subgroups. Significant variation among Hispanic subgroups was observed for unadjusted PCS scores and ADL difficulty measures. Racial and Hispanic subgroup differences were attenuated after adjusting for cumulative disadvantage and demographic and clinical factors, but significant differences among groups remained. In adjusted analyses, the Cuban subgroup had the highest PCS scores and lowest rates of ADL difficulty of any racial group or Hispanic subgroup, and White respondents had the lowest rates of difficulty with specific ADLs. NHPI and multiple Hispanic respondents had the highest and second highest rates of any ADL difficulties or specific ADL difficulties.
Our findings are consistent with prior research on patterns of health and disability among Hispanic elders in the United States. The apparent “paradox” of Hispanics’ low mortality in conjunction with low socioeconomic status has been extensively explored (Markides & Eschbach, 2005). Nevertheless, self-reported health status is lower among Hispanic elders than Whites (Administration for Community Living, 2017). Hispanic elders also have higher rates of disability than Whites, perhaps due to higher rates of chronic conditions such as diabetes (Garcia, Downer, Crowe & Markides, 2017). Being an immigrant appears to contribute to better health among Hispanics, but may also contribute to greater disability in older age (Angel et al., 2015; Sheftel & Heiland, 2018).
Among our sample of Medicare Advantage beneficiaries, we found that White and Asian respondents were the least disadvantaged, and observed significant heterogeneity in social disadvantage factors among the other racial and ethnic groups. White respondents had markedly higher incomes, educational attainment, and rates of marriage than any other racial group or Hispanic subgroup, except for Asian respondents who were the most educated and most likely to be married. We note that the high average educational and economic status of this sample of Asian older adults may obscure cumulative disadvantages among Asian subgroups (Budiman & Ruiz, 2021). Hispanics not only had lower incomes and education levels than any other racial group but also had high marriage rates. Among Hispanic subgroups, Cuban respondents had the highest income, education level, and marriage rate. Mexican respondents not only had the next-highest income and marriage rate but also had markedly lower educational attainment than any other racial group or Hispanic subgroup.
Medicare Advantage enrollment continues to grow, currently comprising more than 4 in 10 Medicare beneficiaries (Freed et al., 2021). High Medicare Advantage enrollment rates among Hispanic and Black beneficiaries (ATI Advisory, 2021) helped to yield larger subgroup sample sizes for this study. Hispanics enroll in Medicare Advantage at higher rates than any other racial or ethnic group (Meyers et al., 2021), and more than half of Hispanic beneficiaries are now in Medicare Advantage plans (ATI Advisory, 2021). Although average income and education levels are lower among Medicare Advantage enrollees than in traditional Medicare (Tarazi et al., 2022), we were able to control for these factors in our regression models. On the other hand, enrollees in Medicare Advantage are somewhat healthier than those in traditional Medicare (Jacobson et al., 2019; Shimada et al., 2009). Overall, Medicare Advantage enrollees are similar to those in traditional Medicare, after accounting for membership in Special Needs Plans (Jacobson et al., 2021).
We observed significant heterogeneity across racial and ethnic groups in other factors that may influence functional limitations and health-related quality of life. Comparing across all racial groups and Hispanic subgroups, average age was highest for Cuban, White, and Asian respondents and lowest for AIAN and Puerto Rican respondents. Despite their higher average ages, Asian and White respondents had the fewest chronic conditions; Puerto Rican and multiple Hispanic respondents had the most. Asian respondents were least likely to be obese in our sample, although other research has reported high rates of obesity among Asian American adults overall and among Asian subgroups (Adia et al., 2020). Cuban and Puerto Rican respondents had the next lowest rates of obesity, and obesity rates were highest among Black respondents.
Unadjusted PCS scores and rates of ADL difficulty largely appear to reflect the observed patterns of cumulative disadvantage, as well as significantly worse outcomes for some less advantaged groups. Comparing across all racial groups and Hispanic subgroups, unadjusted PCS scores were highest for Asian, White, Cuban, and AIAN respondents, respectively. Rates of any ADL difficulty were lowest for Asian, White, and Cuban respondents, respectively. PCS scores were worst for multiple Hispanic respondents and somewhat higher for NHPI and multiple race respondents. NHPI respondents had the highest rates of any ADL difficulty, followed by multiple Hispanic respondents.
Rates of difficulty varied widely across specific ADLs, and unadjusted rates of difficulty seem to reflect patterns of cumulative disadvantage. More than three in 10 respondents had difficulty walking and over two in 10 had difficulty transitioning, while fewer than one in 10 had difficulty toileting or eating. Comparing across all racial groups and Hispanic subgroups, White or Asian respondents had the lowest rates of difficulty for five of six ADLs. In contrast, multiple Hispanic respondents had the highest rates of difficulty for four ADLs, and NHPI and other Hispanic respondent each had among the highest difficulty rates for many ADLs.
Analyses that adjusted for cumulative disadvantage and sociodemographic and health factors revealed some clear patterns and other more nuanced findings. Comparing across all racial groups and Hispanic subgroups, Cuban respondents had the highest adjusted PCS scores the lowest rate of any ADL difficulty, as well as the lowest rates of difficulty walking or transitioning. White respondents had the second lowest rate of any ADL difficulty and the lowest number of ADL difficulties among respondents with one or more difficulties; White respondents also had the lowest adjusted difficulty rates for four ADLs (bathing, dressing, toileting, and eating). NHPI respondents had the highest adjusted rate of any ADL difficulty, and the highest adjusted difficulty rates for 3 ADLs (walking, transitioning, and bathing). Multiple Hispanic respondents had the second lowest PCS scores and second highest rate of and ADL difficulty, and the highest rates of difficulty for three ADLs (dressing, toileting, and eating). Other Hispanic respondents had rates of any ADL difficulty and difficulty rates for specific ADLs that were consistently among the highest across all groups. Black, Asian, AIAN, Mexican, and Puerto Rican respondents never had the highest or lowest adjusted rates for any outcome.
In sum, we found marked variation in functional limitations and health-related quality of life across Hispanic subgroups. Cuban respondents, the least disadvantaged Hispanic subgroup, had the best unadjusted outcomes of any Hispanic subgroup, and in adjusted models, better PCS scores and rates of any ADL difficulty than any other racial group or Hispanic subgroup. Multiple Hispanic respondents had the worst unadjusted outcomes among Hispanic subgroups and, in adjusted models, worse outcomes than all but one other racial group or Hispanic subgroup. Mexican and Puerto Rican respondents, despite having low levels of education and income, had intermediate levels of both adjusted and unadjusted outcomes.
Sensitivity analyses suggested that the patterns of disadvantage experienced by racial minority groups and some Hispanic subgroups were in fact cumulative. Specifically, regression analyses that omitted socioeconomic status variables (education and income) showed increased disparities for racial groups and Hispanic subgroups compared to the White reference group. Hispanics overall face significant socioeconomic disadvantage compared to Whites, which is associated with lower quality of life and higher rates of ADL difficulties.
Our results are broadly consistent with prior research among Hispanic subgroups regarding the prevalence of ADL difficulties (Cantu et al., 2013) and variation in rates of ADL difficulty across subgroups (Garcia, Garcia, Ailshire, 2018; Garcia, Garcia, Chiu, Raji, & Markides, 2018). The influence of cumulative disadvantage on health differs across Hispanic subgroups, in part because each subgroup has a unique history and relationship to the United States. For example, Puerto Ricans are U.S. citizens, while many foreign-born Cubans were admitted to the United States as political refugees (Duany, 2011). These distinct historical and political contexts have impacted access to institutional and societal resources that contribute to functional limitations and health-related quality of life in older age. Future research could examine the contribution of migration and acculturation to variation in social disadvantage and health outcomes.
Some policy implications flow from the above findings. We first note that unadjusted rates are a useful measure when targeting potential interventions because they reflect the total amount of need in specific subgroups. Difficulties in walking and transitioning are by far the most common but can also be prevented or mitigated by relatively low-cost interventions such as balance training and exercise promotion programs, and providing mechanical aids such as walkers or electric lift chairs. Addressing needs for other ADLs (bathing, dressing, toileting, and eating) requires more costly human assistance, often provided in elders’ homes, and may be financed by Medicaid for low-income elders. Comparing unadjusted difficulty rates for specific ADLs across all 11 racial groups and Hispanic subgroups, a few groups consistently have the highest needs: NHPI and multiple Hispanic respondents are in the four highest need groups for six ADLs, Puerto Rican respondents for five ADLs, and other Hispanic respondents for four ADLs. Interventions to provide ADL assistance to those highest need groups may be most effectively targeted at the neighborhood level, for example, by faith-based organizations or neighborhood-level organizations such as senior centers or adult day health centers. Other efforts could aim to reduce observed disparities in the quality of care received by Hispanic and racial minority enrollees within Medicare Advantage plans (Johnston et al., 2021; Markovitz et al., 2022; Meyers et al., 2021). Last, our findings highlight the importance of collecting and reporting data that allow assessment of varying levels of need both across and within-racial and ethnic groups.
This study also has some limitations and implications for future research. Although the HOS sample is very large, survey administration approaches may not be completely consistent across CMS survey vendors, and include limited Asian language follow-up protocols. This sample may limit generalizability outside of Medicare Advantage or to older adults who do not speak English, Spanish, or Chinese. Respondent characteristics and health outcomes analyzed in this study were self-reported. Additionally, we examined Asian Americans as one racial group, which may mask disparities among Asian subgroups. Future research should examine how cumulative disadvantage, functional limitations, and health-related quality of life vary among diverse Asian subgroups. Finally, this study used a cross-sectional design, but research (e.g., Lyu & Wolinsky, 2017) suggests that future research should explore functional limitations and health-related quality of life over time to better reflect cumulative disadvantage over the life course.
Overall, this study identified wide variation in functional limitations and quality of life across racial and ethnic groups. Variation was strikingly high within the Hispanic group, which comprised both the healthiest and the highest need subgroups of the entire population. Cumulative disadvantage factors explain a significant proportion of differences across racial and ethnic groups. Nevertheless, differences across groups may have implications for interventions that can prevent functional limitations or provide assistance to address them.
Supplemental Material
Supplemental Material - Functional Limitations and Physical Health in Community-Dwelling Medicare Advantage Beneficiaries: Variation by Race and Hispanic Subgroup
Supplemental Material for Functional Limitations and Physical Health in Community-Dwelling Medicare Advantage Beneficiaries: Variation by Race and Hispanic Subgroup by Jeff Luck, Diana Govier, Lan N. Ðoàn, Shyama Mahakalanda, Wei Zhang, and Carolyn Mendez-Luck in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LNÐ was supported by the National Institutes of Health (NIH) National Institute on Aging (NIA) R36AG060132 at OSU and is currently supported by National Institute on Minority Health and Health Disparities (NIMHD) Award Number U54MD000538 and U.S. Department of Health & Human Services, Centers for Disease Control and Prevention (CDC) Award Number NU38OT2020001477, CFDA number 93.421. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the NIH or the CDC.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.