
Abstract
Objectives
To investigate how indicators of psychological stress and physical health differentially influence subjective and objective memory in older adults.
Introduction
A large body of research documents that memory functions decline with age (Naveh-Benjamin, 2000; Nyberg et al., 2012; Park & Reuter-Lorenz, 2009). Because traditional lab-based memory assessments can be burdensome on older participants and geographically limiting, research realities often necessitate remote collection of memory performance information. This is frequently done using self-reported measures of memory experience, where participants report on their perceived memory difficulties via an online questionnaire. However, self-reported measures may be heavily influenced by psychological factors such as stress, anxiety, and/or depression, as well as by physical health status, making it difficult to tease memory performance apart from a participant’s psychological and health profile (Carrigan & Barkus, 2016; Paradise et al., 2011; Rönnlund et al., 2011), and thus may not accurately reflect the objective state of memory functions. Indeed, several studies found little to no correlation between subjective memory (SM) reports and objective memory (OM) performance assessed concurrently (e.g., Lenehan et al., 2012; Rönnlund et al., 2011; Wereszczyński & Niedźwieńska, 2021). While some researchers have addressed this issue by utilizing OM tasks that can be administered remotely via a web-based survey platform (Calamia et al., 2021; Hansen et al., 2015), little is currently known about the extent to which psychological or physical health factors are linked with performance on these objective, remotely-administered memory tasks. Understanding these associations may help researchers utilizing both SM and OM indicators anticipate person-level factors that influence memory performance, and thereby permit greater control of key confounders and provide valid measures of the construct of interest. Understanding these links may also shed light on how both psychological and physical health factors influence memory in older adults, and highlight potential points of intervention for those expressing concern about memory and cognitive function.
Psychological Distress (PDS) and Memory Function
Prior research has demonstrated the detrimental effects of PDS on memory performance. A systematic review investigating the impact of psychological disorders on self-reported cognitive failures (Carrigan & Barkus, 2016) found that depression had consistent effects across studies. Multiple studies (e.g., Ronnlund et al., 2011) found that depressive symptoms consistently predict more self-reported memory problems than task-based objective performance. A study exploring global PDS (depression and anxiety symptoms) in middle-aged adults also found strong associations between the PDS measure and SM complaints (Paradise et al., 2011). Similarly, Potter and colleagues (Potter et al., 2009) showed that higher perceived stress levels were correlated with more memory complaints even after accounting for depression and anxiety symptoms. Although the distress-memory link tends to be more pronounced in studies assessing memory via self-reported measures, PDS influences performance on OM tasks as well (see Sandi, 2013, for a review). It has been found that high stress may damage the hippocampus, a brain structure that plays a key role in supporting long-term memory (Dillon & Pizzagalli, 2018; Hickie et al., 2005; Lupien et al., 2009). Elevated cortisol levels, an indicator of high stress situations, have also been associated with brain volume reduction and impaired episodic memory (Echouffo-Tcheugui et al., 2018; Geerlings et al., 2015). In older adults, this effect can be especially pronounced (Fiske et al., 2009). Cognitive- and memory-related concerns are especially distressing for older adults due to over-arching fear about dementia (sometimes termed dementia worry; (Bowen et al., 2019)). It is not surprising, then, that there is much shared variance between self-reported measures of PDS and self-reported measures of memory function in older adults (Haavisto & Blaskewicz Boron, 2020; Lucas et al., 2016; Montejo Carrasco et al., 2017).
Physical Health (PHY) and Memory Function
The relationship between PHY and cognitive function is widely documented in middle-age and older adults. Systemic conditions, such as multimorbidity and obesity, are the norm rather than the exception among middle-age and older adults and have been previously shown to impact cognitive function in this population (Prickett et al., 2015; Wittenberg et al., 2022). Multimorbidity (i.e., two or more co-occurring chronic diseases) is highly prevalent, with ∼72% of adults ages 50–64 and up to 90% of those over the age of 65 having been diagnosed with at least two chronic diseases (Buttorff et al., 2017; Calderón-Larrañaga et al., 2017; King et al., 2018). Multiple studies have documented the association between a higher multimorbidity burden (i.e., a higher number of diseases) and a higher risk of incident cognitive impairment and dementia, most likely due to multiple etiologies and synergistic effects of the multiple co-occurring diseases (Grande et al., 2021; Vassilaki et al., 2015). Fewer studies have isolated the memory component of global cognitive function in its association with multimorbidity; those studies found that individuals with multiple co-occurring diseases reported more SM complaints and had poorer memory test performance compared with those without multimorbidity (e.g., Caracciolo et al., 2013; Pedro et al., 2016). However, the complex association between PDS and concurrently-assessed SM and OM functions, while accounting for systemic PHY conditions highly prevalent among older adults, such as multimorbidity and obesity, has not been fully investigated. Such investigation may help identify health characteristics (e.g., co-occurring chronic conditions or BMI category) that are typically assessed during medical screenings or annual wellness visits and that indicate an increased risk for one or both types of memory impairment and their consequences.
Present Study & Hypotheses
The present study sets out to investigate (1) how participant performance on OM tasks correlates with scores on widely-used self-reported SM questionnaires, both delivered via an online platform; and (2) whether indicators of PDS and PHY differentially influence the SM and OM assessments. To do so, we asked participants, recruited from Amazon Mturk, to complete an online Qualtrics package to assess their SM, PDS (focusing on perceived stress, anxiety, depression), and PHY (focusing on multimorbidity and obesity). We also embedded a face-name-occupation associative memory task in this online Qualtrics package to assess participants’ OM performance. Using this task, we obtained measures not only for face recognition (item memory), but also for associative memory measure, which has shown to decline in aging and to be related to hippocampal functions (Davachi, 2006; LaPlume et al., 2021; Naveh-Benjamin, 2000; Sperling, 2007). This design allowed us to concurrently assess OM and SM and investigate whether they show different associations with PDS and PHY measures. Based on existing research, we hypothesized that: 1. Fewer SM complaints will be associated with better OM performance. 2. Lower PDS will be associated with fewer SM complaints and better OM performance. 3. Better PHY (i.e., no multimorbidity and/or lower BMI category) will be associated with fewer SM complaints and better OM performance. 4. PDS and PHY will retain their significant effects when considered together, as they represent distinct mechanisms influencing memory complaints and performance.
Methods
Participants
We recruited 404 older adults (139 males and 265 females; age: M = 65.96, SD = 5.04, range = 55–85 years old) living in the United States, from Amazon’s Mechanical Turk (MTurk) using CloudResearch MTurk Toolkit (https://www.cloudresearch.com) and the Qualtrics survey platform. The sample was recruited in April and May 2021. To ensure appropriate data quality (Litman et al., 2017), we used the following CloudResearch’s recommended data quality filters to recruit the participants: (1) blocking participants with duplicated IP addresses; (2) blocking participants with suspicious geocode; (3) only including participants with verified worker country location, that is, USA; and (4) only including CloudResearch approved participants. The CloudResearch approved participants have similar demographics as those of the original MTurk population, but do not contain those who have often failed to pay attention to online tasks or were shown to be unable or unwilling to follow study instructions (https://go.cloudresearch.com/en/knowledge/enhancing-data-quality). Eight additional participants were excluded from this analysis because of (1) implausible body height or weight values (n = 7), likely due to inaccurate data entry by the participants, and (2) self-reported cognitive impairment (n = 1).
Five attention-check questions were also embedded in the online questionnaires to ascertain data quality. The average performance of the whole sample on the attention check questions was 4.96 (out of 5; SD = 0.22), indicating that the data quality was adequate. We found that only 16 (out of 404) participants did not respond correctly to all 5 questions. Among them, 15 responded incorrectly to 1 attention check question and 1 participant responded incorrectly to 2 attention check questions. Because there was no clear evidence that the quality of the data from these 16 participants was questionable, they were also included in the analyses.
On average, participants took 39.3 minutes to complete the online study (SD = 12.0) and were paid $10 for their participation. The study was approved by the Institutional Review Board at the University of Michigan (HUM00162268).
Face-Name-Occupation Memory Task
To objectively assess participants’ memory performance, we designed a face-name-occupation memory task, similar to Alegret et al. (2020). The task consisted of encoding and retrieval phases.
Face-Name-Occupation Encoding
Participants were first presented with 12 face images (6 females and 6 males), one at a time for 8 seconds (Figure 1). Under each face, a common English first name (e.g., Emily or David) was also presented. All the names had 5 letters and were chosen from the Social Security Administration website (https://www.ssa.gov/oact/babynames/decades/names1990s.html). The face images were taken from an open-source face database (DeBruine & Jones, 2017) and were cropped to include only the face area (no shoulder; see Figure 1 for examples of face stimuli). All faces are Caucasian with neutral facial expressions. The order of the face-name encoding trials was randomized across participants. Participants were asked to try their best to memorize the faces and the corresponding names. After a short delay during which participants completed two 4-item questionnaires (on their height, weight, and health conditions), they were presented with the face images again. This time, each face was paired with a common occupation name (e.g., nurse), chosen from https://7esl.com/jobs-and-occupations-vocabulary/. Participants were given 8 seconds to memorize each face-occupation pair. The order of the face-occupation encoding trials was also randomized across participants. The face-name and face-occupation stimuli were presented using Quatrics. The face image was scaled to be 450 x 554 pixels (width by height) and was adjusted by Quatrics based on participants’ own computer monitor. We confirmed that the participants can see both the face image and name on the screen without scrolling down the webpage on 13-inch and 14-inch laptop monitors. Illustration of the face-name-occupation memory tasks. Face images were selected from Face Research Lab London Set (DeBruine & Jones, 2017; https://doi.org/10.6084/M9.FIGSHARE.5047666.V2).
Face Recognition Task
After completing other questionnaires, including the General Anxiety Questionnaire (GAD) used in this study, participants were asked to perform a face recognition task (Figure 1). Specifically, in each trial of this task, participants were asked to identify the face that had been presented in the face-name/occupation encoding phase (i.e., the target), from two lure faces that were chosen from the same face database, had the same gender, and were cropped in the same way as the target. The target and lure faces were aligned horizontally and the locations of the target among the 3 images were balanced across trials. Participants were able to see all 3 face pictures on the same Qualtrics page without scrolling (down or left/right) their webpage. There were 12 face recognition trials and participants were given 8 seconds to complete each trial. As soon as participants recorded a response, the current trial would be terminated and the next trial would be presented. The order of the face recognition trials was randomized across participants. The percentage of the faces that were correctly identified was used to measure participants’ face recognition accuracy (this variable is labeled FaceRecog; higher percentage indicates higher accuracy).
Face-Name-Occupation Associative Identification Task
After the face recognition task, participants were asked to work on questionnaires, including the Perceived Stress Scale (PSS) and the Geriatric Depression Scale (GDS) used here. Then, they were asked to complete a face-name-occupation associative memory task (Figure 1). In each trial of the task, participants were presented with a face picture that had been presented during the encoding phase. Under the face picture, participants were given 3 names, one of which was previously paired with the face (i.e., the target name). The other 2 lure names were from other faces of the same gender presented during the face-name encoding phase. Participants were required to choose the name that they thought had been paired with the target face. Under the name question, participants were also given 3 occupations and one of them was previously paired with the face (i.e., the target occupation). The other 2 lure occupations were also from other faces of the same gender presented during the face-occupation encoding phase. Participants were asked to choose the occupation that they thought had been paired with the target face. The location of the target name/occupation on the screen was balanced across trials. The number of times that a name or occupation served as a lure was also equalized. The order of the face-name-occupation retrieval trials was randomized across participants. Participants can see the face and the name/occupation options on one Qualtrics page without scrolling down their webpage. There were 12 trials in this task and participants were given 12 secs to complete each trial. As soon as participants made a response, the current trial would be terminated and the next trial would be presented. The proportions of correctly identified names, occupations, and both names and occupations were averaged to measure participants’ associative memory accuracy. To increase the reliability of the memory measures, the task was given twice with a short time delay when participants completed a few questionnaires, including the Patients’ Assessment of Own Functioning Inventory—Memory subscale (PAOF_mem) and the Prospective-retrospective Memory Questionnaire (PRMQ) used here. Participants’ performance from the two rounds of testing was then averaged to produce the final associative memory accuracy (this variable is labeled F/N/O; higher values indicate higher accuracy).
Subjective Memory Measures
We used two instruments to assess self-reported, subjective memory function.
Prospective-retrospective Memory Questionnaire (PRMQ; Smith et al., 2000). This questionnaire contains 16 items: 8 questions assessing prospective memory (e.g., “Do you fail to mention or give something to a visitor that you were asked to pass on?”) and 8 questions assessing retrospective memory (e.g., “Do you fail to recognize a place you have visited before?”) Participants responded to these questions using a five-point scale (1 = never; 5 = very often). The ratings on the 16 items were summed so that higher scores indicate more self-reported prospective and retrospective memory failures. The questionnaire has been shown to have good internal reliability, with Cronbach’s alpha = 0.919 (Crawford et al., 2003).
The Patients’ Assessment of Own Functioning Inventory—Memory subscale (PAOF_mem; (Chelune & Lehman, 1986). This subscale of PAOF has nine items measuring the frequency of self-perceived memory difficulties on a six-point scale (1 = almost never; 6 = almost always) for each item. For example, “How often do you forget people whom you met in the last day or two?” and “How often do you forget things that you knew a year or more ago?” The total sum-score across the nine items was calculated (range 9–54; higher score indicates higher perceived frequency of memory difficulties). The scale has adequate reported reliability and validity ((Bell et al., 2013); Cronbach’s alpha = 0.876).
Psychological Distress Measures
Perceived Stress Scale (PSS)
The 14-item Perceived Stress Scale (Cohen et al., 1983) assesses overall stress perceptions by having participants report their stress-related experience during the past month using a 4-point scale (0 = never, 3 = all the time). Example items include How often have you felt nervous and “stressed?” and How often have you been able to control irritations in your life? The items were summed and scored so that higher values indicate higher levels of perceived stress, for a possible range of 0–42 (Cronbach’s alpha = 0.891).
Generalized Anxiety Questionnaire (GAD)
The 7-item Generalized Anxiety Disorder scale is a brief, non-clinical measure of overall anxiety levels (Spitzer et al., 2006). Participants report the frequency with which they have experienced things like feeling nervous, anxious, or on edge and worrying too much about different things over the past 2 weeks on a 4-point scale (0 = not at all sure, 3 = nearly every day). Items were summed and scored so that higher values indicate higher levels of anxiety, for a possible range of 0–21 (Cronbach’s alpha = 0.893).
Geriatric Depression Scale (GDS)
The 15-item Geriatric Depression Scale (Yesavage et al., 1983) has participants respond Yes (coded 1) or No (coded 0) to a series of questions designed to assess depressive symptomatology over the past week. Examples of questions include Do you often feel helpless? and Do you think it’s wonderful to be alive? Items were summed and scored so that higher values indicate higher levels of depressive symptomatology, for a possible range of 0–15 (Cronbach’s alpha = 0.889).
Physical health Measures
Body Mass Index (BMI)
Participants reported their weight (in pounds) and height (in inches). BMI was calculated using the formula: (weight/height^2) x 703. Raw BMI values were categorized into “healthy BMI” (corresponding to normal and overweight BMI; values ≥18.5 and <30) and an “unhealthy BMI” (corresponding to underweight and obese BMI; values <18.5 or ≥30). This dichotomous variable is labeled “BMIhlth” in the analysis and tables with 1 = healthy BMI and 2 = unhealthy BMI.
Multimorbidity
The following physician-diagnosed chronic conditions were assessed by self-report: (1) heart disease (i.e., myocardial infarction, coronary heart disease, angina, congestive heart failure, or other heart problems); (2) hypertension (i.e., high blood pressure); (3) high cholesterol; (4) stroke; (5) diabetes; (6) arthritis or other joint problems; (7) lung disease (excluding asthma and COVID-19); (8) cancer (excluding skin cancer); and (9) none of the above. Multimorbidity was defined as the concomitant presence of two or more chronic conditions (yes = 1; otherwise = 0). This dichotomous multimorbidity variable is labeled “MultiMorb” in the analysis and in the tables.
Analytic Approach
In order to permit the consideration of multiple measures on different scales, as well as a more complete conceptualization of the key variables of interest, a composite variable approach was used. Specifically, all raw values were standardized (M = 0, SD = 1), and summed to create the model variables as follows: zPSS + zGAD + zGDS = Psychological Distress composite (PDS; higher = worse) zBMIhlth + z MultiMorb = Physical Health composite (PHY; higher = worse) zPAOFmem + zPRMQ = Subjective Memory composite (SM; higher = worse) zFaceRecog + zF/N/O = Objective Memory composite (OM; higher = better)
Means and Standard Deviations for Raw Variables, Composite Variables, and Model Covariates for the Whole Sample and the Subgroup with and without Multimorbidity.
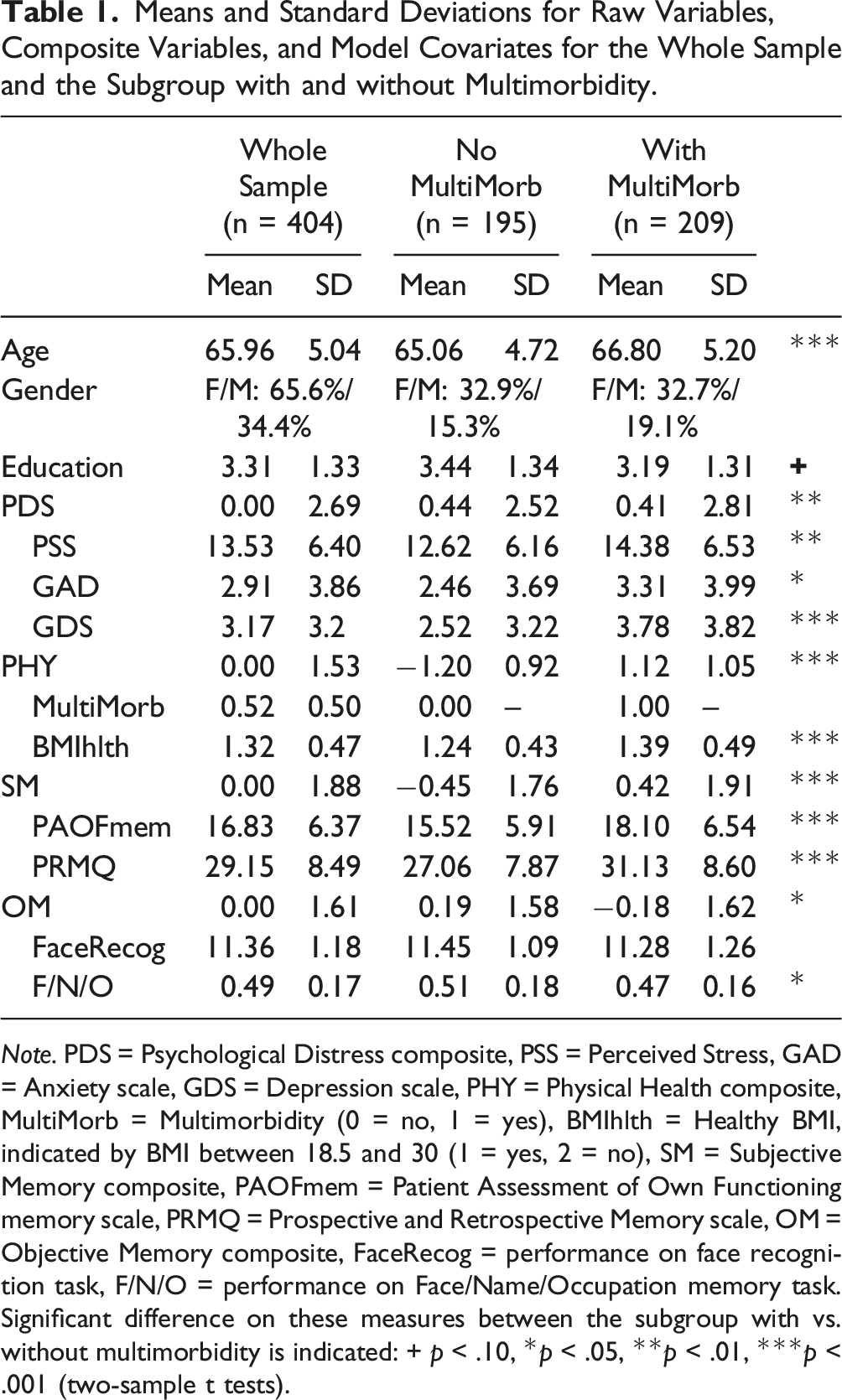
Note. PDS = Psychological Distress composite, PSS = Perceived Stress, GAD = Anxiety scale, GDS = Depression scale, PHY = Physical Health composite, MultiMorb = Multimorbidity (0 = no, 1 = yes), BMIhlth = Healthy BMI, indicated by BMI between 18.5 and 30 (1 = yes, 2 = no), SM = Subjective Memory composite, PAOFmem = Patient Assessment of Own Functioning memory scale, PRMQ = Prospective and Retrospective Memory scale, OM = Objective Memory composite, FaceRecog = performance on face recognition task, F/N/O = performance on Face/Name/Occupation memory task. Significant difference on these measures between the subgroup with vs. without multimorbidity is indicated: + p < .10, *p < .05, **p < .01, ***p < .001 (two-sample t tests).
Results
Descriptive Statistics
Correlations for Raw Variable, Composite Variables, and Model Covariates (N = 404).
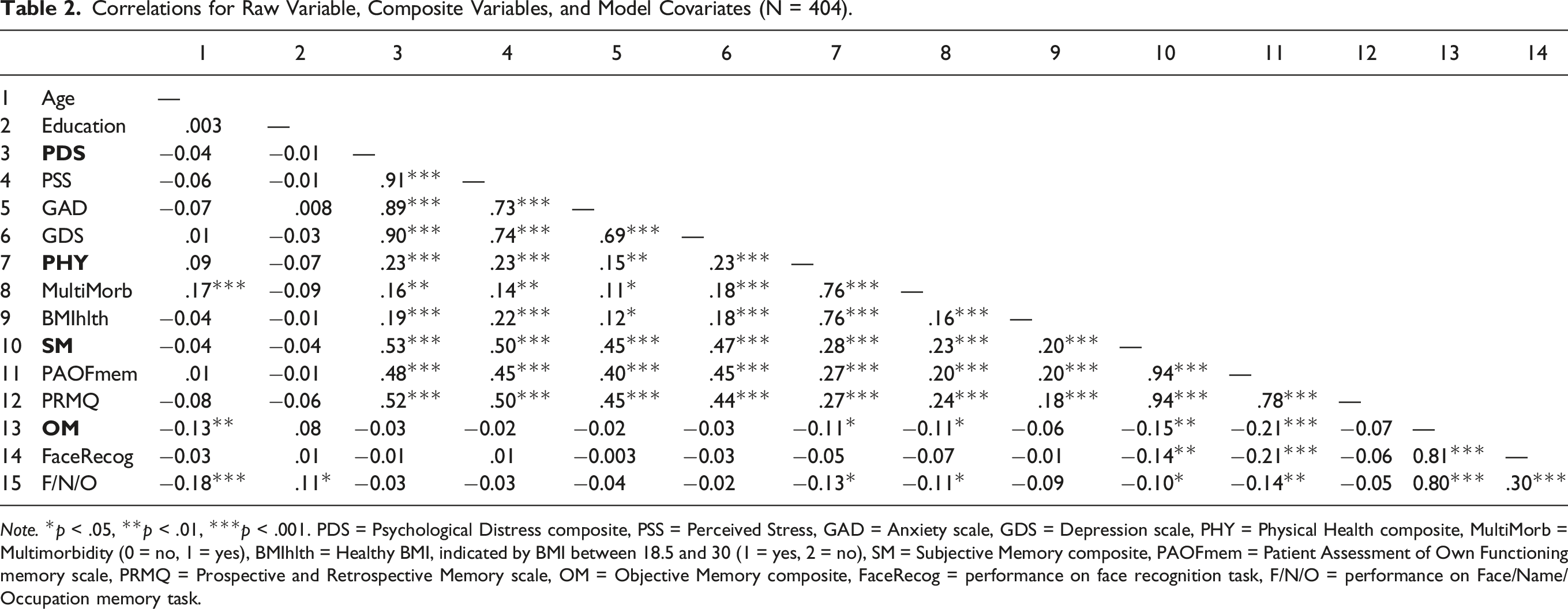
Note. *p < .05, **p < .01, ***p < .001. PDS = Psychological Distress composite, PSS = Perceived Stress, GAD = Anxiety scale, GDS = Depression scale, PHY = Physical Health composite, MultiMorb = Multimorbidity (0 = no, 1 = yes), BMIhlth = Healthy BMI, indicated by BMI between 18.5 and 30 (1 = yes, 2 = no), SM = Subjective Memory composite, PAOFmem = Patient Assessment of Own Functioning memory scale, PRMQ = Prospective and Retrospective Memory scale, OM = Objective Memory composite, FaceRecog = performance on face recognition task, F/N/O = performance on Face/Name/Occupation memory task.
Table 2 also depicts the correlations among the composite variables used in the analytic models, along with the age and education covariates. Whereas PDS is significantly correlated with the SM composite, there is no significant association with the OM composite; PHY, on the other hand, is significantly linked with both SM and OM composites. It is also important to highlight the significant correlation between the two memory outcome variables: worse SM is linked with worse OM (p < .001), supporting the validity of both. As expected, older age is associated with poorer OM performance (r = −0.13, p < .01). For completeness, correlations between all raw and composite variables are also presented in Table 2.
Regression Models
Results of Regression Models (N = 404).
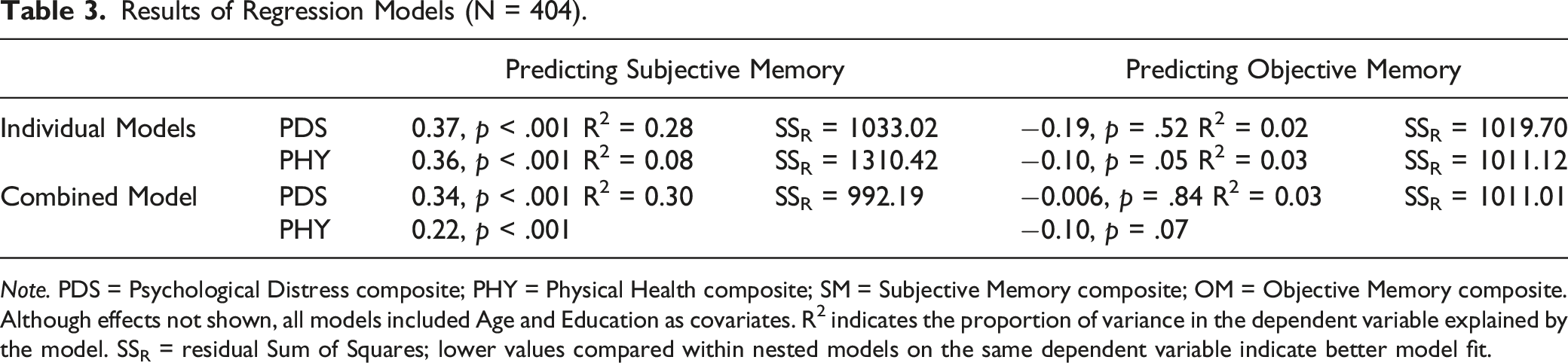
Note. PDS = Psychological Distress composite; PHY = Physical Health composite; SM = Subjective Memory composite; OM = Objective Memory composite. Although effects not shown, all models included Age and Education as covariates. R2 indicates the proportion of variance in the dependent variable explained by the model. SSR = residual Sum of Squares; lower values compared within nested models on the same dependent variable indicate better model fit.
Individual Models
Considered individually, lower psychological distress predicts significantly fewer subjective memory complaints, but does not have significant effects on task-based OM. The individual model for physical health reveals significant effects on both SM (p < .001) and OM (p = .05), with better physical health linked with better memory in both cases.
Combined Models
The models including PDS and PHY together indicate that both psychological distress and physical health are significantly associated with SM, but for OM, the shared variance between PDS and PHY brought the significant effect of PHY that appeared in the individual model to a trend significant effect in the combined model (p = .07). Considering the robust literature on the associative memory deficit in aging, which was also confirmed by the current study in that older age predicted worse F/N/O associative memory not FaceRecog item memory, we re-ran the combined model with F/N/O as the dependent variable. The result confirmed that PHY, but not PDS, maintained its unique prediction on objectively measured F/N/O associative memory (coefficient b = −0.07 and −0.006, t = −2.03 and −0.32, p = .04 and 0.75, for PHY and PDS, respectively. Model explained variance R 2 = 0.06; Residual Sum of Squares SSR = 372.48).
Post-hoc ANOVA
To separate the effects of the two physical health indicators on memory outcomes and to provide clinical relevance, post-hoc analyses tested for mean differences in SM and OM, separately, among four sub-groups: 1) healthy BMI and no multimorbidity (N = 148 participants); 2) healthy BMI and multimorbidity (N = 127); 3) unhealthy BMI and no multimorbidity (N = 47); and 4) unhealthy BMI and multimorbidity (N = 82). ANOVA results showed significant main effects for both multimorbidity (p < .001) and BMI (p = .001) on SM, and the lack of a significant interaction effect indicated the main effects are additive: participants with both unhealthy BMI and multimorbidity reported the most memory issues, whereas those with healthy BMI and no multimorbidity reported the least memory issues (see Figure 2 for plot of marginal means). For OM, mean comparisons revealed no significant effects for both factors and their interaction (all p > .2). These results indicate both factors contributed in a comparable way to the prediction of both OM and SM. Plots of post-hoc analysis for physical health variables. Multimorbidity alone or unhealthy BMI alone have similar individual detrimental effects on (a) subjective memory (SM) complaints or (b) objective memory (OM) performance; together, their effects are additive.
Discussion
The current study recruited 404 adults aged 55 and older and tested how psychological distress and physical health were associated with concurrently-assessed subjective and objective memory. Our hypotheses were partially supported. First, we confirmed that participants with fewer SM complaints tended to perform better on the remotely delivered OM task. As predicted, PDS significantly predicted SM, with higher distress associated with more memory complaints. This aligns with previous findings (e.g., Paradise et al., 2011) highlighting the influence of psychological distress indicators on subjective memory complaints (Carrigan & Barkus, 2016). However, PDS did not predict OM, which is a departure from the work cited previously establishing the association between psychological distress and objective memory tasks (e.g., Sandi, 2013). The third hypothesis was supported in that better PHY was associated with both better performance on the OM tasks (especially the associative memory) and fewer SM complaints, supporting the patterns found previously (e.g., Nelson et al., 2020; Qin & Basak, 2022). Consistent with our last hypothesis, the findings remained similar when PDS and PHY variables were considered together. Therefore, we conclude that although older adults’ self-reported memory difficulties and their objective performance on specific memory tasks are related, PDS and PHY seem to contribute differently to the two types of memory measures. Since a primary concern with using self-reported memory assessments is their conflation with participants’ psychological profile, the findings here point to remotely-delivered, objective memory measures as an option more resistant to influence by psychological factors and more representative of actual memory function.
Our finding that PDS predicted SM difficulties is consistent with a large body of research (Goda et al., 2020; Künzi et al., 2021; Potter et al., 2009; Rönnlund et al., 2011; Sabatini et al., 2021). Since there is a link between chronic stress and PDS conditions, such as depression (Monroe & Harkness, 2005), it has been proposed that long-term PDS may damage the neurogenesis in the hippocampus, a brain region crucial for supporting memory (Dillon & Pizzagalli, 2018). However, in the current study, we found that PDS did not predict older adults’ performance on the associative memory task that has been found to rely on the hippocampus and decline in aging (Davachi et al., 2003; Naveh-Benjamin, 2000; Sperling, 2007; Sperling et al., 2001; Tsukiura et al., 2011). The results suggest that other mechanisms may link PDS and OM loss. A prior study (Lucas et al., 2016) found that self-efficacy mediated the relationship between PDS (anxiety and depression) and SM complaints, while another study (Haavisto & Blaskewicz Boron, 2020) showed that cognitive concerns, a component of the Geriatric Depression Scale used also in our study, was a better predictor of SM complaints than performance on OM tasks. This suggests that older adults with high PDS may be less confident and/or have more concerns with their own cognitive functions, contributing to their reporting of SM complaints. This interpretation is consistent with previous findings that depressive symptoms had a stronger association with SM than OM measures (Montejo Carrasco et al., 2017; Zlatar et al., 2014). Future research needs to investigate how different types of PDS are associated with different cognitive functions, measured using self-report and objective tasks, and explore potential mediation and modulation factors.
Health issues such as multimorbidity and obesity are prevalent in older adults and may contribute to older adults' cognitive declines (Buttorff et al., 2017; Calderón-Larrañaga et al., 2019; Hassen et al., 2022; King et al., 2018; Schiltz et al., 2019). Different from our results on PDS, we found that PHY predicted both SM difficulties and performance on the OM task, especially the associative memory measure which has been found to show a robust decline in aging. It has been documented that older adults with multimorbidity tended to have more SM complaints (Aarts et al., 2011a, 2011b; Franco et al., 2022; Ghose & Abdoul Razak, 2017; Jacob et al., 2019; Pedro et al., 2016). Similarly, our finding that multimorbidity was associated with worse performance on an OM task is consistent with previous studies (Aarts et al., 2011b; Bendayan et al., 2021; Wei et al., 2020; for reviews, see Wittenberg et al., 2022). Our study contributes to this literature by simultaneously assessing subjective and objective memory, while considering important co-occurring psychological and physical health conditions. The association between multimorbidity and memory deficits in aging may be bidirectional (Nelson et al., 2020): while individual diseases within multimorbidity combinations may represent, separately or synergistically, etiologic harm to memory and cognition, the presence of memory loss or confusion can complicate the management of chronic diseases, particularly for those experiencing multiple chronic diseases. In turn, poorly managed chronic diseases could lead to further cognitive impairment, adding to the impact of memory loss on the patient’s ability to manage diseases and prevent or delay incrementally poorer health outcomes. Due to its cross-sectional nature, our study does not offer insights into the direction of this association and calls for longitudinal investigations to clarify this issue.
Obesity has been associated with changes in brain structures and cognitive deficits (Arnoldussen et al., 2014; Prickett et al., 2015; Spyridaki et al., 2016; Sui & Pasco, 2020). In young adults, it has been found that obesity was related to lower activity in the brain’s memory networks (Cheke et al., 2016, 2017). In older adults, obesity was also associated with reduced the brain’s gray matter (Beyer et al., 2019), which mediated lower memory performance (Kharabian Masouleh et al., 2016). Obesity may also lead to abnormal changes in the brain white matter (Daoust et al., 2021), cholinergic signaling system (Martinelli et al., 2022), and importantly, the hippocampal structure or functions that support memory processing (Parent et al., 2022). These effects may be caused by the low-grade inflammation, metabolic disturbances, or cerebro-microvascular impairment due to obesity (Balasubramanian et al., 2021; Buie et al., 2019; Spyridaki et al., 2016). While prior studies found that overweight BMI (in our study included in the healthy BMI category), but not obese/unhealthy BMI, may serve as a protective factor against cognitive declines in older age (Kim et al., 2016), especially for females (Bohn et al., 2020), the association between body-weight and cognitive function should be interpreted in the context of existing health status and potential weight loss (and thus seemingly “healthy” weight) due to preexisting conditions (for a review, see Sui & Pasco, 2020). Our analyses accounted for preexisting multimorbidity; and thus, it is possible that the non-significant association of BMI with OM in the current study was due to parsing out the effects of co-occurring diseases from the specific effect of excess weight. The post-hoc analysis showed that the detrimental effects of BMI and multimorbidity on both subjective memory difficulties and objective memory performance are additive. Given the high prevalence of multimorbidity and/or obesity among older adults, our findings suggest that a broad segment of this population may benefit from behavioral, medical, and cognitive training interventions aimed at minimizing multimorbidity risk and preventing memory impairment.
In terms of practical applications, having the ability to assess objective memory function remotely is a valuable tool which may allow clinicians to identify older adults’ urgent memory issues without the potential barrier of an in-person lab visit. This is particularly important in contexts where it is difficult or simply not feasible for the older adult to come into a clinical setting, as happened during the COVID-19 pandemic. Remote objective memory assessment is also valuable for therapeutic purposes, as it can help assess memory function apart from subjective reports, and therefore obtain a more accurate assessment of the patient’s memory function and start teasing apart whether any demonstrated memory deficit is due to an organic brain disease process or is a function of psychological factors or an alternative physical health diagnosis. This is necessary especially considering that SM complaints and OM performance are not always closely related (Burmester et al., 2017; Mol et al., 2006; Wereszczyński & Niedźwieńska, 2021). In a research context, our findings also highlight the importance of controlling for both psychological and physical health factors when assessing memory function, whether the chosen measure is subjective or objective in nature. In cases where researchers rely solely on measures of self-reported memory difficulties, it is especially important to measure and statistically account for psychological and physical health factors that can influence participants’ reports.
Several limitations of our study should be noted. First, this study used an online (Mturk) older adult sample. Recent evidence also showed that older adults participating in Mturk may have better memory, fewer physical health problems, and healthier BMI, compared to a US national representative sample (Ogletree & Katz, 2020). Thus, future studies utilizing more representative samples should investigate the generalizability of these findings. Second, a large body of literature shows that associative memory, which is likely supported by the medial temporal lobe regions (Davachi, 2006; LaPlume et al., 2021; Naveh-Benjamin, 2000; Sperling, 2007), may be particularly affected by aging. However, more work is needed to clarify the psychometric properties of tests of associative memory function delivered online, to better assess the sensitivity and reliability of online objective memory measures. Third, weight, height, and chronic disease diagnoses were self-reported, thus being subject to under-reporting or under-diagnosis. However, several studies have shown adequate concordance between patient reports and objectively validated weight and disease diagnoses (Skinner et al, 2005; Weir, 2008). Relatedly, in the current study, we only asked participants to report a few major medical conditions that are prevalent in aging population. Other medical conditions such as chronic pain, sleep disorders, or substance use should also be considered in future investigations, especially considering that some of the conditions/disorders, for example, sleep disturbance, have been found to modify the relationship between older adults’ subjective memory complaints and their objective memory performance (Costa et al., 2022). Finally, because of the cross-sectional nature of our study, no causal inference or clear suggestion of direction of association between psychological distress or physical health and memory measures can be made. Future longitudinal studies are needed in order to clarify these associations and provide basis for clinical recommendations.
In conclusion, the results of this study suggest that SM measures capture a significant portion not only of the psychological profile of the participant but of the physical health state of the participant as well. This makes it essential for studies relying exclusively on SM measures to control for indicators of both psychological distress and physical health status. Second, these results highlight the influence of PHY on OM performance. That PHY, especially multimorbidity, was the only significant predictor of participants’ performance on the OM task in this study not only points to PHY indicators as important factors to consider when utilizing remote OM tasks, but also supports previously-established links between physical health and brain function (Guidi et al., 2021). Lastly, this study demonstrated, at least in principle, that valid OM tasks can be embedded in online survey studies. Considering that OM deficits in older adults were associated with abnormal hippocampal activity, smaller hippocampal volume, and higher Alzheimer’s disease pathology, that is, amyloid positivity (Grober et al., 2022; Sperling, 2007), it is important to include OM measures in large survey studies that investigate older adults’ memory function and factors that influence it.
Footnotes
Acknowledgments
We would like to thank Nadia Aboumourad, Mariya Churina, and Seraj Farhat for their help in this research project. This research was financially supported by the University of Michigan Mcubed program, awarded to Z.-X.L., B.W., and A.B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the MCubed, University of Michigan (U064020).