
Abstract
Introduction
The prevalence of individuals affected by Alzheimer’s disease and related dementias (ADRD) is rapidly increasing across the globe. Current estimates indicate that nearly 50 million people are living with dementia, a number projected to reach 152 million by 2050 (Patterson, 2018). As the cohort of baby boomers is reaching old age, and life expectancy is generally increasing, it is predicted that the availability of family caregivers will decline (Feinberg & Spillman, 2019; Jutkowitz et al., 2020). At the same time greater care demands are anticipated due to rising rates of chronic disease and declines in functional ability (Benoit et al., 2020; Maresova et al., 2015).
Although the needs of persons with dementia are widely variable across the disease course, the care role becomes more demanding and intensive as care-recipients grow increasingly dependent on family caregivers to meet their basic needs. Family caregivers are also responsible for managing unpredictable dementia-related behavioral and psychological symptoms in addition to navigating other stressors, including financial hardship, care coordination, and role conflict (Schulz et al., 2020).
The majority of care for individuals with ADRD is provided by unpaid relatives, primarily daughters and wives, often for long periods of time (Alzheimer’s Association, 2021). Some research has shown that caregiving may have positive aspects for caregivers, such as feeling good about oneself or giving more meaning to life (e.g., Roth et al., 2015). However, the long-term, progressive nature of dementia caregiving, and the stressors derived from the care setting, represent a unique chronic stress experience associated with a myriad of negative physical and mental health outcomes, such as high levels of burden and depressive symptoms (Collins & Kishita, 2020).
Empirically validated stress and coping models such as the one developed specifically for caregivers by Pearlin et al. (1990) have served as guiding theoretical frameworks for understanding key dimensions and variables (e.g., coping and social support) that influence the appraisal of, and outcomes associated with, the caregiving stress process. Notably, the sociocultural stress and coping model (Aranda & Knight, 1997; Knight & Sayegh, 2010) highlighted the importance of contextual variables, such as racial, ethnic, and cultural values, on the perceived appraisal of the caregiving role and the coping strategies used to deal with such stressors, which may differentially impact caregiving outcomes. According to this model, the degree to which care-related stress influences mental health is highly dependent on caregivers’ available internal and external coping resources (Crellin et al., 2014), which may stem from internalized cultural expectations and beliefs that influence how caregivers perceive their experience.
The literature on cross-cultural variations (e.g., racial/ethnic differences) in dementia family caregiving has gained significant momentum, but empirical work comparing caregiving outcomes in cross-national samples is much more limited. Although stress and coping are universally experienced regardless of culture, ethnicity, and race, the macro-level sociocultural contexts in which individuals are embedded can lead to heterogeneity in how the care role is experienced. Additional study of this topic is warranted to gain a more comprehensive understanding regarding the factors that influence care-related outcomes. Enhanced understanding of such cross-national differences can lead to the design and development of culturally sensitive behavioral interventions that may be more feasibly translatable across contexts.
Caregiver self-efficacy, defined as “confidence in the ability to execute specific behaviors in response to situational demands” (Steffen et al., 2019, p. 326), is one protective resource that may mitigate against adverse caregiving outcomes, as caregivers navigate a wide range of heterogeneous tasks and an unpredictable disease course, which are major sources of stress and burden (Gallagher et al., 2011). Considering the behavioral and cognitive challenges that caregivers usually face, several self-efficacy dimensions have been identified.
Specifically, Steffen et al. (2019), drawing on extensive research, highlights three self-efficacy domains or factors: self-efficacy for obtaining respite (how confident are caregivers that they can ask family or friends for help in order to receive support), self-efficacy for managing disruptive behaviors (how confident are caregivers in their personal resources for coping in an adaptive way with disruptive behaviors), and self-efficacy for controlling upsetting thoughts (how confident are caregivers that they can control maladaptive thoughts related to caregiving). In a cross-national review of studies evaluating caregiver self-efficacy, Steffen et al. (2019) found that feelings of self-efficacy were negatively associated with caregivers’ levels of burden and depression, among other outcomes. Collectively, research underscores the importance of considering cultural issues to better understand differences in physical and mental health outcomes among caregivers from diverse cultural contexts (Huertas-Domingo et al., 2021; Knight & Sayegh, 2010; Losada et al., 2010).
A key variable examined in the context of the sociocultural stress and coping model is the construct of familism. Familism has been studied as a driving mechanism of cross-cultural differences in caregiving outcomes. Defined as “a strong identification and attachment of individuals with their families (nuclear and extended), and strong feelings of loyalty, reciprocity, and solidarity among members of the same family” (Sabogal et al., 1987, p. 398), many studies conducted in both caregiving and non-caregiving samples hypothesized associations between familism and positive outcomes (e.g., Cahill et al., 2021; Valdivieso-Mora et al., 2016). Under stressful circumstances, participants who reported greater levels of familism reported higher self-esteem compared to participants with low familism (Corona et al., 2017).
However, research examining familism in the context of caregiving has been mixed. In a study comparing cross-cultural differences in caregiving in the US, Falzarano et al. (2021) found higher levels of familism in African American and Hispanic participants compared to White caregivers, but no associations were identified between familism and burden and depression. However, they found that familism was associated with higher levels of positive aspects of caregiving in African Americans when compared to Whites. In a longitudinal study in the United Kingdom, Parveen and Morrison (2012) found a positive association between familism and caregiver gains. However, in Spain, Frías-Osuna et al. (2019) found that caregivers are less likely to report positive care-related outcomes when familial obligation was the main motive for caring.
Research has shown that individuals with more traditional familism beliefs may provide care due to feelings of obligation to the family, which can exacerbate caregivers’ feelings of distress (Dilworth-Anderson et al., 2004). In a similar vein, Rozario and DeRienzis (2008) found a positive association between familism and caregivers’ levels of depression and perceived stress in African American caregivers. Losada et al. (2010) in Spain, and Sayegh and Knight (2011) in the US, found an indirect effect of familism on depressive symptoms through its association with dysfunctional thoughts and avoidant coping strategies, respectively.
Interestingly, in a study conducted in Korea, Lim et al. (2016) analyzed the associations between familism and self-efficacy in family caregivers of frail older adults and found that female caregivers who strongly endorsed familism but exhibited low self-efficacy reported more burden associated with older adults’ behavior. Conversely, female caregivers who reported weak levels of familism and high self-efficacy reported lower burden (Lim et al., 2016). As Mendez-Luck et al. (2016) suggest, the positive effects of familism may end when there is an important family need, such as long-term caregiving, to be fulfilled without the adequate support or involvement of other family members. Therefore, familism may lead to adverse outcomes due to the incongruence between one’s cultural ideals versus the actual reality of caregiving. Indeed, although familism may be protective for individuals with greater family cohesion or more extensive kin and non-kin social support networks, the discrepancy between the demands of caregiving and available family resources and support can exacerbate negative mental health outcomes.
One explanation for the mixed findings may be related to the multidimensional nature of the familism construct. For example, familism, as measured with Sabogal et al.’s (1987) familism scale, consists of three factors: familial obligations, support from the family, and family as referents. Of these, different studies have found that familial obligations and family as referents seem to be associated with negative outcomes (e.g., higher burden or levels of depression; Kim et al., 2007; Losada et al., 2010).
Although support from the family has been associated with positive outcomes (Losada et al., 2010), gender may be another factor contributing to the discrepancy in whether familism serves as a risk or protective factor in the caregiving stress process. A recent study by Losada-Baltar et al. (2023) found significant gender differences in the relationship between family obligations and self-efficacy, coping strategies, and distress. Specifically, familial obligations were found to be associated with lower self-efficacy for self-care and leisure and higher depressive feelings in female caregivers, but not in males.
An additional explanation for the discrepant literature was proposed by Losada et al. (2006), who suggested that certain socio-cultural contexts may facilitate or impede the degree to which caregivers identify with familism principles. Specifically, forces such as acculturation may impact values of familism, leading to the dissipation of strong familial beliefs due to a discrepancy between one’s cultural values and the current societal context in which they are embedded (Gelman, 2014). Falzarano et al. (2021) found that Hispanics who spent a longer length of time in the US were more likely to report lower levels of familism. Further, the authors found that nonnative US Hispanics (i.e., those who immigrated to the US after the age of 10-years-old) reported higher levels of familism compared to Hispanic US natives. These results point to the possibility that acculturation may diminish the influence of cultural values in caregiving because of the mismatch between the collectivist values stemming from one’s country of origin that become embedded within an individualistic society.
Alternatively, Hispanic older adults with a greater active network of extended families or peers in the US, who share the same immigrant status, may benefit more from sharing familistic values, and have a higher perception of self-efficacy. In line with this hypothesis and in terms of cross-national studies, Losada et al. (2006) found that familism was related to lower burden in Hispanic caregivers living in Los Angeles (US), while familism was related to higher levels of depressive symptoms in caregivers from Spain. These findings collectively indicate that the study of cultural values as mitigating or risk factors in influencing caregiving outcomes is highly dependent on the role such cultural values play in one’s larger sociocultural context, warranting further investigation into cross-cultural, and in particular cross-national, comparisons on the influence of familism on the caregiving stress process.
Increasing our knowledge on how cultural dimensions and coping variables interact with and influence caregivers’ distress among diverse caregiving populations can help to better elucidate theoretical models of caregiving and can guide the development of culturally tailored interventions for caregivers (Cheng et al., 2019; Gallagher-Thompson et al., 2020). Tailoring interventions to accommodate cultural differences that can be translatable across different cultural groups is increasingly important given the heterogeneity and sheer size of the caregiver population. Drawing upon the sociocultural stress and coping model as a guiding theoretical framework (Knight & Sayegh, 2010), the purpose of this study is to examine the cross-national associations between the three dimensions of familism and self-efficacy, and how these associations may differentially influence levels of burden and depression in a sample of caregivers from the US and Spain.
Considering previous studies that found positive associations between familial obligations, family as referents, and increased caregiver distress, we hypothesize similar positive relationships to emerge regarding caregivers’ burden and depression, and a negative association with caregivers’ perceptions of self-efficacy. Further, we hypothesize positive associations between familial support and self-efficacy, and subsequently lower levels of burden and depression. As no previous study has analyzed cross-national differences in these variables, we do not have specific hypotheses regarding potential differences between the two countries.
Methods
Participants
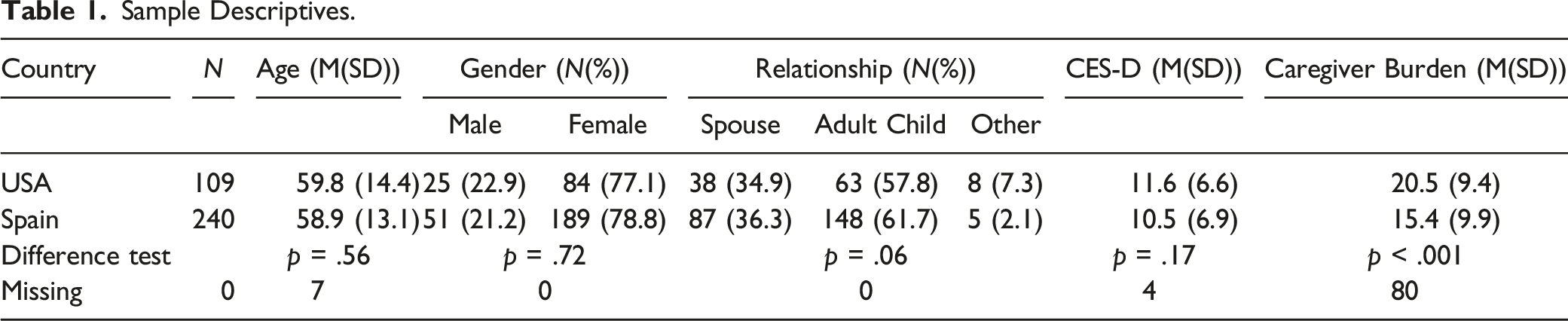
Participants in this study were 349 family caregivers of people with dementia. Of these, 109 were Hispanic caregivers from Miami (US), and 240 were Spanish caregivers from Madrid (Spain). Participants from Spain were recruited through health and social care centers within the Madrid Community. Participants from the US were recruited using a multi-pronged approach (e.g., health care clinics, radio advertisements) in the greater Miami area.
The data for this study were gathered in two different projects (one from Spain and another from the US) that were developed and run independently of each other. Taking advantage of the similarities between the projects, especially in terms of the targeted population (family caregivers of people with dementia) and the assessed variables (see methods), researchers from both studies considered that a comparison between both a comparson between both samples would advance the study of the impact of culture in the caregiving stress process. For this reason, eligibility requirements differed between the two studies. To meet eligibility criteria, participants from Spain were required to: be over the age 18-years, serve as the primary source of care for a person with dementia, provide care for at least three consecutive months, and devote at least one hour a day to caregiving tasks.
A first telephone contact was made with the participants in order to confirm the inclusion criteria. Once confirmed, a face to face assessment was done in the health or social care center. Participants first reviewed and signed the informed consent and then the needed information was gathered through an individual interview. Participants from the US were required to be older than 18 years, provide care for minimum of 15 hours a week for more than six months, have contact with the care-recipient at least five times a week, and resides with or in close proximity to the care-recipient. US-based participants were provided with the option to complete study measures in Spanish or English. 53.2% and 44% of participants completed study assessments in Spanish and English, respectively (2.8% missing). All participants provided informed consent prior to study enrollment. All study materials were approved by the Ethics Committee of the Universidad Rey Juan Carlos and the University of Miami, for the Spanish and US samples, respectively.
Measures
Covariate Variables
Caregivers’ age and gender, and relationship to the care-recipient were assessed.
Independent Variable
Familism
Familism was measured using Sabogal et al.’s (1987) familism scale (Spanish version by Losada et al., 2008), a 14-item measure comprising three subscales: Familial obligations (e.g., “One should make great sacrifices in order to guarantee a good education for his/her children”), support from the family (e.g., “When one has problems, one can count on the help of relatives”), and family as referents (e.g., “Much of what a son or daughter does should be done to please the parents”). Response options ranged from 1 (very much in disagreement) to 5 (very much in agreement). Cronbach’s alpha for the present study is .79 for the Spanish sample and .72 for the US sample. As shown in Supplementary Table 2, Cronbach’s alphas for the subscales range from .64 (Familial Obligations) to .68 (Family as Referents) in the Spanish sample, and from .51 (Family as Referents) to .67 (Support from the Family) in the US sample. Although these reliability indexes are low, they are similar to those obtained in the validation of the scale in US Hispanic/Latinos (N = 5313) (Campos et al., 2019), that ranged from .59 (Family as Referents) to .74 (Support from the Family).
Mediating Variable
Self-Efficacy
Self-efficacy was measured using the Revised Scale for Caregiving Self-Efficacy (RSCSE; Steffen et al., 2002; Spanish version by Márquez-González et al. (2009). The RSCSE is a 15-item scale comprising three factors: (1) self-efficacy for obtaining respite (e.g., “How confident are you that you can ask a friend/family member to stay with [your care recipient] for a day when you feel the need for a break?); (2) self-efficacy for responding to disruptive patient behaviors (e.g., “When [your care recipient] asks you 4 times in the first one h after lunch when lunch is, how confident are you that you can answer him/her without raising your voice?”), and (3) self-efficacy for controlling upsetting thoughts related to caregiving (e.g., “How confident are you that you can control thinking about unpleasant aspects of taking care of [your care recipient]?”). Items are rated from 0 (cannot do at all) to 100 (certainly can do). Items are summed, with higher scores representing higher feelings of self-efficacy. The internal consistency (Cronbach’s alpha) for this scale in the Spanish sample is .83 and .86 for the US sample. As shown in Supplementary Table 2, Cronbach’s alphas for the subscales range from .81 (dealing with upsetting thoughts and with disruptive behaviors) to .85 (self-efficacy for obtaining respite) in the Spanish sample, and from .87 (self-efficacy for obtaining respite) to .90 (dealing with disruptive behaviors) in the US sample.
Dependent Variables
Depressive Symptomatology
Depressive symptoms were measured through the 10-item version of the Center for Epidemiologic Studies-Depression Scale (CES-D, Radloff, 1977; Spanish version by Losada et al., 2012). The CES-D measures the frequency of depressive symptomatology experienced during the past week (e.g., “I felt that everything I did was an effort”), with response options ranging from 0 (rarely or none of the time) to 3 (most or all the time). Cronbach’s alpha for this scale was .85 and .82 for the Spanish and US samples, respectively.
Burden
Caregivers’ perceived burden was measured through the 12-item Zarit Burden Interview (ZBI; Zarit et al., 1980; Spanish version by Martín et al., 1996). Sample items include: “Do you feel stressed between caring for your relative and trying to meet other responsibilities (work/family).” Participants responded to each item on a Likert scale ranging from 0 (never) to 4 (nearly always). The internal consistency (Cronbach’s alpha) for this scale was .88 and .84 for the Spanish and US samples, respectively. The available sample for the ZBI in the Spanish sample was 161.
Data Analysis
To examine cross-national differences across participants from the US and Spain, multiple mediation models were examined using a structural equation modeling framework, grouped by country and controlling for gender. The self-efficacy subscales were included as potential mediating variables in separate models in the relationship between the familism subscales and our two outcomes of interest: depression and burden (see Figure 1 for the proposed model). The same model, as in Figure 1, was applied to both depression and burden. All variables were entered as observed variables, which were the sums of the constituent items. An unconstrained model, where the associations of the tested variables with the outcomes were tested separately for each country was compared to a model that constrained the countries equally. That is, the paths between each variable were constrained to be the same for each country in the constrained model. A chi-square difference test was then used to examine if the unconstrained model was significantly different from the constrained model. If significant differences emerge, then the countries are considered statistically different in their respective models. Several indices of model fit were examined, including the chi-square test statistic (χ2/df), the comparative fit index (CFI), the standardized root mean square residual (SRMR), and the root mean square error of approximation (RMSEA). Model fit statistics of χ2/df < 5, CFI >.95, SRMR <.08, RMSEA <.06 were used as benchmarks indicative of good model fit. Full information maximum likelihood (FIML) estimation was used for missing data. All analyses were conducted in Mplus version 8.5 (Muthén & Muthén, 2017). Proposed mediation model. Note: SE, Self-efficacy.
Results
Sample Descriptive Statistics
Sample Descriptives.
Multiple Mediation Models
Caregiver Depression
Standardized and unstandardized path coefficients for all models are shown in Supplementary Table S3. The constrained and unconstrained multiple mediation models were significantly different from each other, suggesting different models for each of the countries, χ2(25) = 47.97, p = .003. The model estimating parameters for each country had mixed support for model fit, with two indices suggesting adequate model fit (χ2/df = 3.76, RMSEA = .13, CFI = .89, SRMR = .05). Significant paths for the US and Spanish sample are shown in Figures 2a and b, respectively. In the US sample, there was a significant indirect effect through both self-efficacy for obtaining respite (β = −.09, S.E. = .03, p = .01) and self-efficacy for controlling upsetting thoughts and behaviors (β = −.13, S.E. = .05, p = .01) on the relationship between familism: support from family and depression. Familism: support from family was positively related to both self-efficacy for obtaining respite and self-efficacy for controlling upsetting thoughts and behaviors. In turn, both self-efficacy constructs were negatively related to depression. That is, higher scores on self-efficacy for obtaining respite and controlling upsetting thoughts were associated with lower depressive scores in the US sample. (a) Standardized factor loadings for significant indirect effect paths– US sample. (b) Standardized factor loadings for significant indirect effect path– Spanish sample.
In the Spanish sample, the only significant indirect effect was from familism: family as referents, which operated through self-efficacy for obtaining respite, on depression (β = .06, S.E. = .03, p = .01). Higher scores on family as referents were associated with lower levels of self-efficacy for obtaining respite, and lower scores on self-efficacy for obtaining respite were associated with higher scores on the depression scale.
Caregiver Burden
When evaluating the outcome of caregiver burden, the constrained and unconstrained multiple mediation models were significantly different from each other, suggesting different models for each of the countries, χ2(25) = 56.44, p < .001. The unconstrained model demonstrated mixed support for model fit, similar to the model described above (χ2/df = 3.75, RMSEA = .13, CFI = .87, SRMR = .05). When examining burden as the outcome, the pattern of results was similar for the US sample (not shown, similar to 2a). For the indirect effect of familism: support from family through self-efficacy for obtaining respite, the model was marginally significant, (β = −.05, S.E. = .03, p = .07). The indirect effect between familism: support from family through self-efficacy for controlling upsetting thoughts and behaviors on burden was significant (β = −.15, S.E. = .06, p = .02). There were no significant indirect effects on burden for the Spanish sample.
Discussion
We conducted a cross-national analysis on the associations between familism and self-efficacy dimensions on burden and depressive symptoms in two samples of Hispanic dementia family caregivers from Spain and the US. Previous cross-national studies (e.g., Losada et al., 2006) have shown cross-cultural differences in the associations between familism and depression, and familism and burden, in Hispanic dementia family caregivers. This study builds upon prior literature on this topic by considering the interplay between familism (familial obligations, family as referents, and support from the family) and self-efficacy (for obtaining respite, for managing disruptive behaviors, and for controlling upsetting thoughts) on feelings of depression and burden. Given prior findings indicating that higher caregiver self-efficacy can help mitigate negative dementia caregivers’ outcomes (e.g., Steffen et al., 2019), we hypothesized that higher levels of perceived family support would result in greater levels of self-efficacy. Examining these relationships cross-nationally allows us to examine how unique cultural contexts influence the caregiving process.
Our findings indicate that the associations between the assessed variables significantly differ between countries. Overall, our results support the hypothesis regarding a significant association between family support and higher self-efficacy and lower depression and burden in the US sample. It seems that perceived support from the family was a protective factor against depression and burden among caregivers in the US. Perceiving support from the family may increase the chances of obtaining respite and perceiving oneself as more capable of controlling upsetting thoughts and behaviors.
This finding was not obtained in the Spanish sample, where, endorsing family as referents seemed to be a risk factor for greater depressive symptomatology. In the Spanish sample, providing care with the family as a behavioral and attitudinal reference seems to be related to lower chances of obtaining respite. No significant associations were identified for familial obligations. Thus, our hypothesis of a positive association between familial obligations and family as referents and depressive symptomatology has been partially confirmed in the Spanish sample, although only for the family as referents dimension, which was linked to lower self-efficacy for obtaining respite.
Taken together, these findings provide support for the importance of cultural variables, such as familism, for understanding differences in the caregiving stress process, as hypothesized by the sociocultural stress and coping model (Knight & Sayegh, 2010), that was developed mainly for understanding the dementia caregiving process. Our findings also partially support previous research demonstrating mixed results regarding the impact of familism on dementia caregivers’ distress (e.g., Losada et al., 2010), and highlight the relevance and importance of understanding the impact of contextual variables and cultural values on the dementia caregiving experience.
Additionally, our results provide support for three important considerations: the multidimensional nature of familism, the associations between familism and self-efficacy factors (in the US, support from the family and higher caregivers’ perceptions of self-efficacy for obtaining respite and controlling upsetting thoughts; and in Spain, family as referents and lower self-efficacy for obtaining respite), and the central role of cultural context in shaping the impact of familistic beliefs on caregivers’ well-being. First, the multidimensional nature of the familism construct is supported by our findings demonstrating that perceived support from the family is positive for caregivers as it is associated with higher perceptions of self-efficacy (for obtaining respite and controlling upsetting thoughts), while other dimensions such as family as referents may be negative, as they are associated with lower perceptions of self-efficacy (for obtaining respite and controlling upsetting thoughts).
Second, in addition to confirming the relevance of self-efficacy factors (specifically self-efficacy for obtaining respite and for controlling upsetting thoughts) on caregivers’ feelings of distress, our results show a significant interplay between familism and self-efficacy, which in turn significantly influenced caregiving outcomes, such as depressive symptomatology and burden. Further, caregivers’ reports of having family as a source of support was related to an increased perception of caregivers’ ability to cope effectively within the caregiving role, obtaining respite and controlling upsetting thoughts (Steffen et al., 2019).
Conversely, having family as behavioral or attitudinal referents may be a source of additional stress as caregivers may perceive that asking for help (i.e., self-efficacy for obtaining respite) could be a source of stigma, weakness, or considered an act against one’s cultural expectations (i.e., “one should care for the family without asking for help”). Failing to ask for help, in addition to caregivers having fewer opportunities in general for social contact and emotional support, reduces the likelihood of receiving adequate support, which may further decrease caregivers’ perceived self-efficacy for controlling upsetting thoughts.
Finally, focusing on the cross-national comparison, the significant differences between countries suggest that the cultural contexts unique to each country may exert a significant influence on the caregiving process, specifically with regard to how cultural values impact coping strategies. In the US, for example, immigrants or immigrant-descendants of Hispanics may maintain active involvement with both Hispanic kin and non-kin networks for peer support, and thus the presence of extended social networks may positively influence the appraisal of the caregiving role, as discussed in Losada et al. (2006).
Furthermore, it is important to note that the healthcare systems in the US and Spain are vastly different in terms of organization, financing, and access to care. The US, which is comprised of a mixed system of public and private providers, has no universal healthcare system, high healthcare costs, and is accompanied by difficulties in accessing coverage and services. Conversely, Spain’s universal healthcare system provides access to free healthcare services including primary care, mental health services, as well as options for home- and adult-day care, with substantially lower healthcare costs compared to the US. The inherent differences between the two country’s healthcare systems have implications on financial costs-of-care as well as accessing needed services to support caregivers in their role, all of which can have implications on family caregivers’ feelings of burden, caregiving self-efficacy, as well as physical and mental health. Although Spain is a very familistic country (e.g., Rainer & Siedler, 2012), the shift towards a more individualistic approach to caregiving, coupled with decreases in the size family networks (e.g., less potential available primary and secondary caregivers), may add additional sources of stress and pressure in being able to respond to “what is expected” as a caregiver. Indeed, post hoc analyses of the familism subscales by caregiver-care recipient relationship among the Spanish sample revealed significantly higher scores (F(2.227–.230) > 3, p < .05, post hoc Tukey HSD p < .05) across all familism subscales for spousal caregivers, compared to adult child caregivers, demonstrating a shift towards more individualism. Therefore, while holding familistic beliefs placing family as a central reference in their lives, Spanish caregivers in this context may find it difficult to meet their desired family expectations, which may exacerbate stress and depressive symptoms.
The idea or reality of receiving help may generate feelings of guilt in dementia family caregivers (Gallego-Alberto et al., 2022). Some caregivers may feel that asking for help is something that a caregiver should not do based on pre-established familial expectations, and believe that only the closest (or most proximal) person to the care-recipient can adequately provide care (Losada et al., 2003). Additionally, most of the participants in the current study consisted of female caregivers. Machismo is a prevalent cultural value in Hispanic and Latino cultures, reflecting an expectation that females will take on the majority of the care role with little to no support (Jaldin et al., 2023). The findings of this study support the need to continue to explore research on the influence of cultural values on the experiences, behaviors, and outcomes of dementia family caregivers.
These findings have important implications for practice. Our results highlight the need to address the influence of cultural values related to the family (values regarding the support or role of families in the caregiving process, or their role as referents) on caregivers’ feelings of distress and methods of coping. Further, our findings point to the need for culturally-tailored intervention strategies designed to buffer the negative effects associated with some of these values (e.g., family as referents or familial obligations) that may contribute to a rigid or inflexible standard that caregivers are expected to fulfill in response to their role.
Both Cognitive-Behavioral and Acceptance and Commitment therapies provide useful therapeutic frameworks for dementia family caregivers to increase flexibility in one’s beliefs with regard to pre-conceived values and norms (Márquez-González et al., 2010). Also, given the results showing the influence of cultural values on caregivers’ perceptions of self-efficacy, clinical work should also include reflections (insight) on these influences, and train caregivers in specific, and culturally sensitive, coping strategies that have proven to be useful in mitigating stress, such as through engaging in self-care behaviors, asking for help and obtaining respite, and managing difficult thoughts and emotions (Steffen et al., 2019). Finally, although it is well known that caregiving has an impact on the whole family, family interventions (e.g., Systemic Therapy) for caregiving issues is an under-developed area (Cheng et al., 2019) that should be further explored in future work.
This study has limitations that point to directions for further research. First, the samples from each country are not representative and are comprised of cross-sectional study designs, which limit the generalizability of our findings. Further, the samples from both countries, although similar in terms of being family caregivers of people with dementia and having provided care for a significant time period, were obtained using different inclusion criteria and methodologies, with the Spanish sample being larger than the US sample. This issue may have an impact on the statistical power for finding group differences. In the case of Spain, the research team had no access to all the caregivers that were approached by the centers that provided them with potential participants. Therefore, the response rate for the Spanish sample was not available, which should recommend caution when considering the generalizability of the findings. Moreover, the inclusion criteria for each country was different, with respect to number of hours per week of caregiving provided. Participants in the Spanish sample were required to provide at least one h of caregiving each day to be eligible, whereas participants from the United States had to provide at least 15 h of care peer week. The exact amount of time spent caregiving each week was not measured, which may partially account for the current findings. In addition, important contextual variables such as educational level, income, or access to supportive services were not available for testing comparisons between samples. Future studies using a longitudinal or experimental design are needed to further analyze the dynamic interplay between cultural factors and coping strategies on caregiving outcomes. Through these type of designs, it will be possible to obtain data that could confirm the causal relationship between familism factors (e.g., perceived support from the family) and higher self-efficacy (e.g., for asking for support), and how these factors are related to depressive symptomatology and burden. Although this study was guided by the socio-cultural stress and coping model (e.g., Knight and Sayegh, 2010), other relevant variables that have not been measured (e.g., stress derived from behavioral and psychological symptoms of dementia) should be further explored in future research. These variables may contribute to understanding the obtained findings (e.g., caregivers exposed to more stress might perceive less support from the family). Further, it should be noted that US-based Hispanic participants were recruited from the Miami area, which may limit generalizability due to the unique qualities of this population and given the understanding that Latino/Hispanic populations do not represent a monolith. Although Miami comprises a majority of individuals of Cuban background, there is also representation from other Latino communities, including those of South American and Caribbean background. Nonetheless future research should seek to further examine differences in cultural values and caregiving outcomes in more diverse samples of Hispanic/Latinos.
Despite its limitations, this is the first study to analyze the relationship between the three dimensions of familism and perceived self-efficacy on caregivers’ burden and distress using a cross-national design. The findings suggest that cultural variables (e.g., familism dimensions) and coping (e.g., self-efficacy dimensions) are related, and that examining this interplay significantly contributes to our understanding of the heterogeneous dementia caregiving experience. Additionally, differences identified between cultures suggest that the same value may not be considered inherently good or bad, but its impact may instead depend on the general cultural context in which the caregiver is embedded. Our findings show that Hispanic caregivers from different nations are exposed to different cultural contexts that have an influence on how dimensions of the stress and coping model relate to one another, influencing outcomes such as depression and burden. In future research, cultural context should be considered when analyzing caregiving outcomes.
Supplemental Material
Supplemental Material - Cross-National Analysis of the Associations Between Familism and Self-Efficacy in Family Caregivers of People With Dementia: Effects on Burden and Depression
Supplemental Material for Cross-National Analysis of the Associations Between Familism and Self-Efficacy in Family Caregivers of People With Dementia: Effects on Burden and Depression by Andrés Losada-Baltar, Francesca B. Falzarano, David W. Hancock, María Márquez-González, Karl Pillemer, Cristina Huertas-Domingo, Lucía Jiménez-Gonzalo, José A. Fernandes-Pires, and Sara J. Czaja in Journal of Aging and Health
Footnotes
Acknowledgments
We thank all the caregivers for their participation in the study and the following centers for collaborating with us on the project: Fundación Cien, Fundaciónn María Wolff, Centro Reina Sofía de Cruz Roja, and Centro de Psicología Aplicada de la Universidad Autónoma de Madrid.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Spanish Ministry of Economy and Competitiveness (PSI2015-65152-C2-1-R) and the Spanish Ministry of Science and Innovation (PID2019-106714RB-C21); Lucía Jiménez-Gonzalo and José Fernandes-Pires were supported by pre-doctoral grants from the URJC. Cristina Huertas-Domingo was supported by a pre-doctoral grant from the Spanish Ministry of Science and Innovation. Support for this project also came for Dr. Czaja from the National Institute of Nursing Research (NINR) (5R01NR014434-05). F. Falzarano acknowledges support from a National Institute on Aging K99/R00 Career Development Award (AG073509). Karl Pillemer acknowledges support from Edward R. Roybal Center Grant from the National Institute on Aging (P30AG022845).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.