
Abstract
Recent research indicates that consumers associate nonprofit organizations mainly with the trait “warmth,” whereas for-profit organizations are perceived as being “competent.” Trustworthiness is another dimension of consumer perceptions of nonprofit organizations. This article attempts to combine two strands of research: Aaker, Vohs, and Mogilner’s research on perceptions of warmth and competence and Handy et al.’s and Schlesinger, Mitchell, and Gray’s research on individuals’ perceptions of trustworthiness in nonprofits. Our study indicates that “warmth,” “trustworthiness,” and “competence” are distinct dimensions of patient perceptions of hospitals. Perceptions of these traits vary across different manifestations of ownership status. Nonprofit hospitals are perceived as more trustworthy and warm but less competent than their for-profit competitors. With nonurgent care, analysis shows that only trustworthiness and competence influence patients’ hospital evaluations. Nonprofit hospitals should try to make their ownership status public as well as to alleviate detrimental deviations of perceived competence from actual competence.
Introduction
The hospital sector provides an interesting setting for research into perceptions of nonprofit organizations compared to for-profits, especially because health services have major economic as well as societal significance. Moreover, nonprofits compete with for-profits as well as with public organizations in the hospital sector (Gray & Clement, 2002).
Extant research into perceived ownership-related differences in the hospital sector focuses primarily on variations in trustworthiness depending on ownership status of the institution (Handy et al., 2010; Schlesinger, Mitchell, & Gray, 2004a, 2004b). However, no research analyses how patient decision making is influenced by perceived trustworthiness of the institution’s ownership structure (e.g., patient beliefs about quality). Schlesinger et al. (2004b) fail to validate the hypothesis that ownership status of a hospital affects patient perceptions and decision-making behavior. They thus recognize the need to refine the available measures of ownership-related dimensions of patient perceptions of hospitals. Within this context, Handy et al. demonstrate that consumers are more likely to patronize nonprofit health service providers, but they do not explicitly investigate the causal relationship between how individuals perceive ownership of the facility and their decision-making processes.
Aaker et al. (Aaker, Vohs, & Mogilner, 2010) show that consumers associate nonprofit organizations with “warmth” and that for-profit firms have a reputation for being more competent. Although Aaker et al.’s article shows that perceived competence influences consumer decision making, perceived warmth may be more relevant in the health sector since trusting relationships between health service providers and patients are of major importance (Schlesinger et al., 2004b). In addition, individual expectations regarding quality of care and humanity of treatment may vary depending on a hospital’s ownership status. Considering this line of argument, Schlesinger et al. (2004a) call for further research to determine whether nonprofit hospitals outperform for-profit hospitals due to their caring reputation, even beyond the effects of perceived trustworthiness and competence.
Social cognition research indicates that warmth, competence, and trustworthiness are distinct dimensions of individuals’ perception of everyday behaviors and other persons (Fiske, Cuddy, & Glick, 2007). However, and to the best of our knowledge, whether these dimensions are distinguishable as ownership-related factors remains unanswered. It is unclear whether ownership-related traits, including “trustworthiness,” “competence,” and “warmth” are distinct dimensions of patients’ hospital perceptions and whether patients judge these traits differently depending on ownership status of the institution. Researchers also have not investigated whether individual perceptions of “trustworthiness,” “competence,” and “warmth” impact patient evaluations of hospitals.
Considering these research gaps, we combine research (Aaker et al., 2010) on the effects of nonprofit status on perceptions of warmth and competence with investigations into how perceptions of trustworthiness depending on ownership status influence patients’ hospital evaluations (Handy et al., 2010; Schlesinger et al., 2004a). This article also considers public and confessional (religious) hospitals as further manifestations of ownership status. This study fills these research gaps by addressing three questions:
Research Question 1: Are warmth, competence, and trustworthiness distinct dimensions of hospital perception?
Research Question 2: Does hospitals’ ownership status impact patient perceptions of warmth, competence, and trustworthiness?
Research Question 3: Do warmth, competence, and trustworthiness influence patients’ hospital evaluations?
In the next section, we first discuss the relevance of nonprofit status in the health care market and then develop a conceptual model of ownership-related effects on patient perceptions and beliefs about quality (see Figure 1). For nonurgent care, we present the results of an empirical study that validates our conceptual model. In the concluding section, we provide a summary, a discussion of the study’s limitations, managerial implications, and avenues for further research.

Overview of proposed relationships.
Relevance of Nonprofit Status
In Germany, as the social context for our study, nonprofit hospitals as well as for-profit and public hospitals have provided health services for decades (Tiemann & Schreyögg, 2009). And since the European hospital sector is deeply rooted in Christianity, confessional hospitals have the longest tradition. Public hospitals emerged in the 18th century (e.g., Berlin’s Charité). For-profit hospitals debuted in the European market in the 19th century. In recent years, the number of for-profit hospitals has risen considerably (Healy & McKee, 2002) in Germany, mainly as a result of ownership conversions, replacing public hospitals (Klenk, 2011). In contrast, nonprofit hospitals as well as religious nonprofit hospitals have maintained their market share of about 30% (Forder, 2002; Prognos, 2009) of German hospitals. Compared to nonprofits in Germany, the number of nonprofit hospitals in the United States exceeds for-profit and public hospitals, accounting for 58% of the total number of all community hospitals (AHA, 2012). As in Germany, the market share of nonprofits in the United States has remained relatively stable over the past decades (O’Neill, 2009; Schlesinger et al., 2004b). Unlike U.S. hospitals (Mechanic, 1996), the German hospital sector remains untroubled by corporate scandals such as deceptive marketing, kickbacks, and corporate self-dealing (van der Schee, Braun, Calnan, Schnee, & Groenewegen, 2007).
The increasing importance of patient empowerment implies greater information needs among patients, especially in the rapidly changing health care markets in the United States (Kurz & Wolinsky, 1985; Sloane, Tidwell, & Horsfield, 1999) as well as in Europe (Coulter & Jenkinson, 2005; de Cruppé & Geraedts, 2011; Scheibler, Janßen, & Pfaff, 2003). Within this context, the literature review of Dietrich and Gapp (2005) indicates that 30% to 40% of German and U.S. consumers act confidently as single decision makers when choosing a hospital for inpatient treatment. Patient participation in the choice of a hospital for an inpatient stay only holds for elective surgery and not for urgent care (Calnan, 1984). Yet elective surgeries represent a major field of hospital activity, and, according to the German Federal Census Bureau, 63% of total surgeries are elective.
Patients access multiple information sources to evaluate and choose a hospital within the context of nonurgent care or elective surgeries. To make informed decisions, health care consumers have to rely on relevant and appropriate information, even more so than consumers in other markets (Robinowitz & Dudley, 2006). However, consumers’ hospital choices are not usually influenced by their own treatment experiences (Woodside, Frey, & Daly, 1989) because they have little personal experience and must rely on third-party information sources, such as general practitioner referrals (Trigg, 2011) or recommendations by relatives and acquaintances (Edgman-Levitan & Cleary, 1996). Information provided by health care providers such as hospital quality reports or hospital websites represents another third-party information source (Leister & Stausberg, 2007). Yet consumers exhibit a lack of awareness, interest, comprehension, and acceptance of information on the quality of health service providers (Jewett & Hibbard, 1996; Marshall, Shekelle, Leatherman, & Brook, 2000; Schneider & Lieberman, 2001). In addition, conflicting and overly detailed information may result in information overload (Walsh & Mitchell, 2010) since patients implicitly look for easy ways to make hospital choices and take shortcuts. This lack of interest and awareness occurs even when consumers decide whether and where to undergo elective surgeries (de Cruppé & Geraedts, 2011; Dietrich & Lindenmeier, 2009). A study of Tscheulin and Helmig (1998) reveals that patients rated hospital advertisements depicting practicing physicians as informative. Even if these indicators are inadequate for an objective evaluation of hospital quality, these advertisements may have a major impact on patient hospital evaluations (e.g., quality beliefs).
In line with this reasoning, the current study focuses on ownership-related dimensions of hospital perceptions as peripheral information cues on patient beliefs about hospital performance (quality beliefs). Patients’ quality beliefs relate to the consideration set phenomenon (e.g., Mehta, Rajiv, & Srinivasan, 2003). That is, if patients believe that a hospital performs below a minimum-quality threshold, that hospital will not be part of their hospital consideration set. According to the consideration set rationale, patients make their hospital choices from among only those hospitals in their consideration set (e.g., Hauser & Wernerfelt, 1990). Within this context, nonprofit ownership status presumably represents an information cue (Luft et al., 1990), even when controlling for quality information, charges, or copayments or distance to the hospital as well as other peripheral information cues. In addition, medical treatment ranks among credence goods. To evaluate the utility provided by these credence goods and to reduce perceived purchase risk (Darby & Karni, 1973), consumers may rely on external stimuli as makeshift criteria to indicate the quality of a health care provider (Hibbard, Sofaer, & Jewett, 1996; McKee, 1997; Robinson & Brodie, 1997).
Existing research indicates that consumers tend to prefer nonprofit hospitals over for-profit hospitals (Handy et al., 2010; Schlesinger et al., 2004b), although such preferences vary according to sociodemographic and psychographic characteristics (Handy et al., 2010). Contract failure theory (Hansmann, 1981) provides a theoretical basis for this finding. Specifically, the nondistribution constraint signals that nonprofit hospitals will actually provide the noncontractible quality that they promise (Malani & David, 2008). By pursuing profit maximization, for-profit hospitals at least partially contradict the values inherent to the provision of quality medical services (Arrow, 1963).
However, low awareness of ownership status and a lack of understanding of nonprofit enterprises can minimize these comparative strengths for nonprofit hospitals (Handy et al., 2010; Malani & David, 2008; Schlesinger et al., 2004b). In the health care sector, low awareness of ownership status probably derives from isomorphic market pressure that results in vague missions of nonprofit hospitals (Weisbrod, 1998). Such pressures stem from increased competition among hospitals and the increasing institutionalization of business management methods (Clarke & Estes, 1992; Dimaggio & Anheier, 1990; Kramer, 2000). But despite their low understanding and awareness of ownership status, most Americans believe that ownership status matters when it comes to evaluating medical care (Schlesinger et al., 2004b; Wilson & Hegarty, 1997) and ownership conversions draw public attention to the hospital sector and are of major importance for health policy worldwide (Claxton, Feder, Shactman, & Altman, 1997).
Handy et al. (2010) state that an inability to identify an organization’s (e.g., hospital’s) ownership status without prompting does not imply that ownership has no effect on individuals’ decision making (e.g., hospital choice). Besides, consumers with differing levels of understanding of ownership status are present in real-market situations. The majority of consumers in the United States and in Germany have at least a minimal understanding of a company’s ownership status. Schlesinger et al. (2004b) show that about 70% of Americans have some sense of what legal ownership entails. Schlesinger and Gray (2006) conclude that a majority of Americans believe that for-profit hospital expansion would make a difference in the provision of health care and that ownership matters in several aspects of heath care. In a survey of German nonprofit organizations, 30% of the firms state that the public has a low or misleading understanding of their nonprofit status (Zimmer & Priller, 2007).
Ownership-Related Dimensions of Patients’ Hospital Perceptions
A number of researchers (Aaker et al., 2010; Handy et al., 2010; Schlesinger et al., 2004a) find that warmth, competence, and trustworthiness are ownership-related dimensions of patients’ hospital perceptions. But it remains unclear whether the traits are distinguishable from each other. From research we know that the reputation of an organization depends on its perceived competence and trustworthiness (Aaker, Fournier, & Brasel, 2004). According to social judgment research (Grandey, Fisk, Mattila, Jansen, & Sideman, 2005; Judd, James-Hawkins, Yzerbyt, & Kashima, 2005) people differentiate organizations on the basis of warmth and competence. Warmth suggests a motivation to be other-focused and behave in line with moral codes, whereas competence suggests the effective capacity to bring about one‘s intent (Cuddy, Fiske, & Glick, 2008). Warmth judgments also relate to perceptions of trustworthiness, sincerity, and honesty. Fiske et al. (2007) find that whether trustworthiness is distinct from warmth is not clear. Trustworthiness may also correlate with competence. Mechanic and Meyer (2000) reveal that competence and trustworthiness represent dimensions of the higher-order construct trust (e.g., in medical services providers) and that both constructs may correlate.
The first evidence for the independence of dimensions occurs in Schlesinger et al.’s (2004b) research, which distinguishes among competence and trustworthiness and humane treatment as determinants of individual beliefs about hospital performance. According to Hall, Dugan, Zheng, and Mishra (2001), trustworthiness toward a provider of medical services is not necessarily linked with perceptions of high competence and vice versa although both dimensions positively determine the general evaluation. Trustworthiness in a medical context is determined by the provider’s motivation to satisfy patient needs rather than to pursue other interests (e.g., profit maximization). In contrast, competence can be seen as how consumers perceive the hospital staff’s professional expertise as well as the staff’s ability to make correct decisions and avoid mistakes (Hall et al., 2001). With regard to the independence of trustworthiness and warmth we refer to McAllister’s (1995) research, which distinguishes between emotional trust (that another person has one‘s best interests in mind) and cognitive trust (that another person can enact the behaviors to accomplish the given task). According to this argument, the caring dimension of health services, reflected by the trait warmth, should be separable from trustworthiness.
Effects of Ownership Status on Perceptions of Ownership-Related Dimensions
Health care management research confirms that consumers generally ascribe higher-quality health care to for-profit hospitals than to nonprofits (Schlesinger et al., 2004b), in line with Aaker et al.’s (2010) findings about ownership-related differences in the evaluation of organizations. Gilson, Sen, Mohammed, and Mujinja (1994) posit that nonprofits have resource constraints similar to those that limit government providers. Consumers therefore infer the poor competence of public and nonprofit hospitals from media coverage of their urgent capital needs (Claxton et al., 1997) and high debt-to-asset ratios (Sloan, Ostermann, & Conover, 2003), which often prompt ownership conversions to for-profit status (Helmig & Lapsley, 2001). Possibly as a result of profit orientation, process management in for-profit hospitals is better coordinated, resulting in shorter waiting times and smooth clinical pathways.
Religious nonprofit hospitals face the same market pressures as other hospitals, although confessional hospitals have a degree of adherence to religious values (White, Begun, & Tian, 2006). In recent years, the existence of religious nonprofit hospitals has been questioned, and their role clearly needs to be redefined (White, 2000). In particular, efforts to conform to religious values at the expense of technical or organizational innovation may be perceived as outmoded business behavior. In addition, religious nonprofit hospital staff consist partly of aged nuns and friars, leading to similar perceptions (Nelson & Gordon, 2004). Within this context, Cuddy, Norton, and Fiske (2005) find that individuals tend to stereotype the older adults as being warm and incompetent. According to Cuddy et al., these stereotypic perceptions are rooted in cognitions of the older adults as being noncompetitive. We thus present Hypothesis 1a:
Hypothesis 1a: Nonprofit hospitals, religious nonprofit hospitals, and public hospitals are perceived as less competent than for-profit hospitals.
According to Schlesinger et al. (2004a, 2004b), the perception of affectionate care may vary with hospitals’ ownership status, with nonprofits enjoying a moderate comparative advantage in terms of humane and fair treatment. A perception of warmth is associated with other-focused and moral employee behavior (Cuddy et al., 2008), an attribute commonly attached to nonprofit organizations (Aaker et al., 2010). Thus, nonprofit hospitals may outperform for-profit hospitals with respect to “warmth” (Schlesinger et al., 2004a). The greater focus on cost reduction strategies and profit margins as well as efficiency (Comondore et al., 2009) may lead patients to expect that for-profit hospitals will treat them merely as cases, not individuals.
Some for-profit hospitals try to achieve high patient satisfaction and have implemented customer relationship management programs (Akinci, Esatoglu, Tengilimoglu, & Parsons, 2005; Kim, Kim, Kim, Kim, & Kang, 2008). Nonprofits may thus find it more difficult to benefit from an ownership-related advantage in terms of the warmth dimension. Ownership-related advantages also do not apply to public hospitals, which are perceived as less warm since they are public bureaucracies. Unlike public and for-profit hospitals, nonprofit hospitals should thus appear more responsive to patient needs (Smith & Lipsky, 1993). The study of Nix and Gibson (1989) suggests that confessional hospitals’ religious affiliation leads to perceptions of high quality of care and religious nonprofit hospitals are perceived as being warm. However, White et al. (2006) cannot find any differences between Catholic and other nonprofit hospitals in the number of compassionate services offered. In line with White et al.’s research, we assume that consumers hold similar perceptions of nonprofit and religious nonprofit hospitals. Hypothesis 2a is:
Hypothesis 2a: Nonprofit and religious nonprofit hospitals are perceived as warmer than for-profit or public hospitals.
Because of the rarity of hospital stays for most consumers, patients do not build trusting relationships with hospitals and attending physicians (Woodside et al., 1989). However, perceptions of trustworthiness are crucial for patient decision making (Handy et al., 2010; Schlesinger et al., 2004a, 2004b). Nonprofits seem more trustworthy than for-profits because consumers expect for-profits to focus on reducing costs for medical treatment to increase profits. From the patient’s perspective, nonprofit status signals that the hospital will provide the noncontractible quality it promises (Malani & David, 2008) while for-profit hospitals’ profit motive intersects with the altruistic values inherent in medical care (Hansmann, 1981). This conflict of interest may lead to a situation where for-profit hospitals stand out due to their entanglement in malpractices (Mechanic, 1996). Within this context, for-profit hospitals try to overcome their ownership-related disadvantages with regard to trustworthiness by affiliating with social causes or welfare initiatives (Lichtenstein, Drumwright, & Braig, 2004). Religious nonprofit hospitals should particularly aim at providing health to all (Nix & Gibson, 1989), especially the poor, even if the service is not profitable (White & Dandi, 2009). According to contract failure theory (Hansmann, 1981), we assume that religious hospitals are perceived as at least as trustworthy or even more trustworthy than nonprofit hospitals. With regard to public hospitals, de Walle, van Roosbroek, and Bouckaert (2008) show that citizens’ trust in the public sector fluctuates, whereas Handy et al. find that a majority of people believe that nonprofits are more trustworthy than government organizations. But since public hospitals incorporate public service missions in part, we assume that consumers regard public hospitals as being as trustworthy as nonprofit hospitals. Hence, Hypothesis 3a is:
Hypothesis 3a: Nonprofit and religious nonprofit hospitals as well as public hospitals are perceived as more trustworthy than for-profit hospitals.
Effects of Perceived Ownership-Related Dimensions on Patients’ Hospital Evaluations
Ownership status may function as an informational and risk-reducing cue when patients select a hospital for an inpatient stay because it signals differing levels of competence, warmth, and trustworthiness. Perceived competence, defined as the ability to make correct decisions and to avoid mistakes, as a dimension of trust affects intentions to seek treatment and remain with a health care provider (Hall et al., 2001). According to social psychology and organizational behavior research, effectiveness, capability, skillfulness, and intelligence represent important facets of competence judgments (Aaker, 1997; Grandey et al., 2005; Judd et al., 2005) and patients likely evaluate hospital competence by observing these cues during the process of consideration set formation. According to Javalgi, Whipple, McManamon, and Edick (1992), hospital image in particular derives from features that can be regarded as structural indicators of competence. Within this context, Akinci et al. (2005) also highlight the importance of physical appearance and technological capabilities for perceived competence. Aaker et al. (2010) predict a positive relationship between the trait “competence” and willingness to buy in a nonmedical product category. In addition, perceptions of hospital quality constitute one of the most important determinants of consumer health care behavior (Cheng, Wei, & Chang, 2006). Therefore, Hypothesis 1b is:
Hypothesis 1b: The perceived competence of a hospital has a positive and direct influence on patient evaluations of that hospital (quality beliefs).
The caring dimension of health services, reflected by the warmth trait, affects how consumers evaluate a hospital that is also shortlisted. As Schlesinger et al. (2004a, 2004b) note, affectionate care is a key criterion used by patients to evaluate and differentiate hospitals because they can assess the level of process quality more easily than outcome quality (Marley, Collier, & Meyer Goldstein, 2004). Aaker et al.’s (2010) article finds that perceived warmth has no direct influence on willingness to buy in a nonmedical product category, but they suggest that perceived warmth may be more relevant in the health sector, since trusting relationships between health service providers and patients are of major importance. According to this rationale, the caring dimension of health services, reflected by the warmth trait, should have a significant influence on patients’ quality beliefs. Accordingly, Hypothesis 2b is:
Hypothesis 2b: Consumers’ perceived warmth of a hospital has a positive and direct influence on their evaluation of the hospital (quality beliefs).
Like Handy et al. (2010) we assume that trustworthiness is of particular importance for patient decision making because credence attributes characterize health services and outcome quality (improvement of health status or healing) as the primary benefit of medical services (Luft et al., 1990). Due to asymmetric distribution of information between patients and health services providers, consumers cannot judge outcome quality dependably, even after the actual service has taken place (Bergen, Dutta, & Walker, 1992). Kim et al. (2008) note that trust has a positive effect on hospital image, whereas Hall et al. (2001) point out that trustworthiness is critical for patients’ willingness to seek care and evaluate health care providers. In line with these arguments, Hypothesis 3b follows:
Hypothesis 3b: Consumers’ perceived trustworthiness of a hospital has a positive and direct influence on their evaluation of that hospital (quality beliefs).
Figure 1 gives an overview of this study’s conceptual framework. The model considers the effects of ownership status on patient perceptions of ownership-related dimensions (Hypotheses 1a, 2a, and 3a) as well as the effects of ownership-related dimensions on patient hospital evaluations as the basis for consideration set formation (Hypotheses 1b, 2b, and 3b).
Method
To obtain empirical support for our hypotheses, we used a four-level, single-factor design to manipulate ownership status of a fictive hospital (for-profit vs. public vs. nonprofit vs. religious nonprofit). For the experimental between-subject design, participants were randomly assigned to one of the four conditions. Using scenario technique we at first described a hypothetical scenario (Shadish, Cook, & Campbell, 2006; Smith, Bolton, & Wagner, 1999) and participants had to imagine that they suffered from nonacute appendicitis requiring a nonurgent inpatient stay. Participants then reviewed the first page of the hospital’s website, which described its ownership status (for-profit, public, nonprofit, or religious nonprofit). The manipulated ownership information was presented on the hospital website because we believe hospitals can easily communicate this information through such a source. In addition and according to Gruca and Wakefield (2004), for example, the internet has increased significance as a communication platform for physicians as well as patients. Each scenario also included a remark that indicated the hospital was profitable, which prevented participants from making evaluations on the basis of the hospital’s financial situation. After reading the scenario the participants were asked to respond to a series of questions.
We conducted the experiment in spring 2011. Using a quota sampling procedure, student research assistants distributed the questionnaires to a population of German residents between the ages of 25 and 69 years. The students considered respondents who fit our quota criteria for gender, age, and educational background. We excluded the data of two participants from the final sample since they could not correctly recall the ownership status of the hospital in the hypothetical scenario immediately after reading the scenario. Our procedure yielded a sample of 200 informants, whose sample characteristics appear in Table 1. At first view, a sample size of 200 participants may appear comparatively small, but cutting-edge experimental research is commonly based on even smaller samples (e.g., Aaker et al., 2010; Passyn & Sujan, 2006). Considering the quota criteria for age (F = 0.21, p > .10), gender (χ2 = 0.28, p > .10), and educational background (χ2 = 0.22, p > .10), the interviewees are distributed uniformly throughout the experimental groups and the exclusion of two participants did not bias this uniform distribution.
Sample Characteristics.
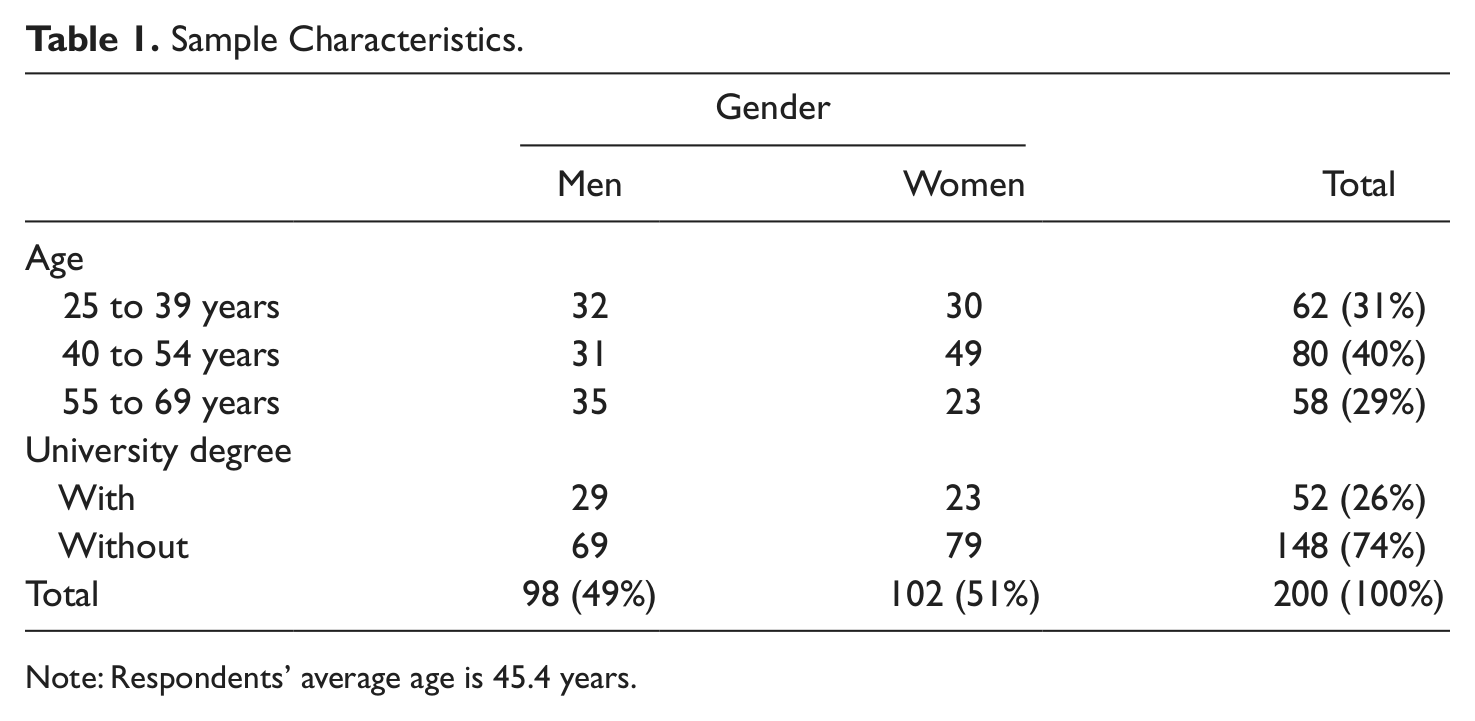
Note: Respondents’ average age is 45.4 years.
To measure patient hospital evaluations, we used a single-item, 7-point Likert-type scale (M = 4.58, SD = 1.13): “I could imagine being under medical treatment in the described hospital” (Babakus & Mangold, 1992). To measure perceived warmth, we used three items from Aaker et al.’s (2010) warmth index (warm, kind, generous). We considered three items from Grandey et al.’s (2005) and Judd et al.’s (2005) measurement instrument that makes up a competence index (competent, effective, efficient). The trustworthiness measure relied on a four-item scale (reasonable, trustworthy, honest, credible), which we derived from Aaker (1997). Finally, respondents indicated their perceptions of the relevance of ownership status for their hospital choice (M = 4.49, SD = 1.72) on a 7-point Likert-type scale (“It is important to bear the hospital ownership status in mind when choosing a hospital for inpatient treatment”). The mean value of 4.49 indicates that ownership status matters in the sample, independently from the level of understanding of what ownership status means, similar to findings of Handy et al. (2010). In support of the experiment’s internal validity, the perceived relevance of ownership status did not vary across the experimental groups, F(3, 195) = 1.13, p = .34.
Findings
In Table 2 we present the results of reliability and validity analyses. All latent constructs used reflective indicators, and the loadings of all indicators on their corresponding constructs were greater than .70 and significant, which indicates the reliability of the individual question items. To evaluate the internal consistency of the ownership-related dimension scales, we used Cronbach’s alpha, which exceeds the .70 threshold for all constructs. Because the average variance extracted (AVE) is greater than .50, we can assume convergent validity. For the analysis of discriminant validity, we compared the AVE values with all corresponding squared interconstruct correlations (Fornell & Larcker, 1981), and all the square roots are greater than the correlations. Therefore, all the considered constructs exhibit satisfactory discriminant validity. Summing up, the results of the reliability and validity analyses confirm that warmth, competence, and trustworthiness are separate dimensions of patient hospital evaluations.
Measures of Perceived Ownership-related Dimensions—Descriptive Statistics, Reliability, and Validity Analysis.
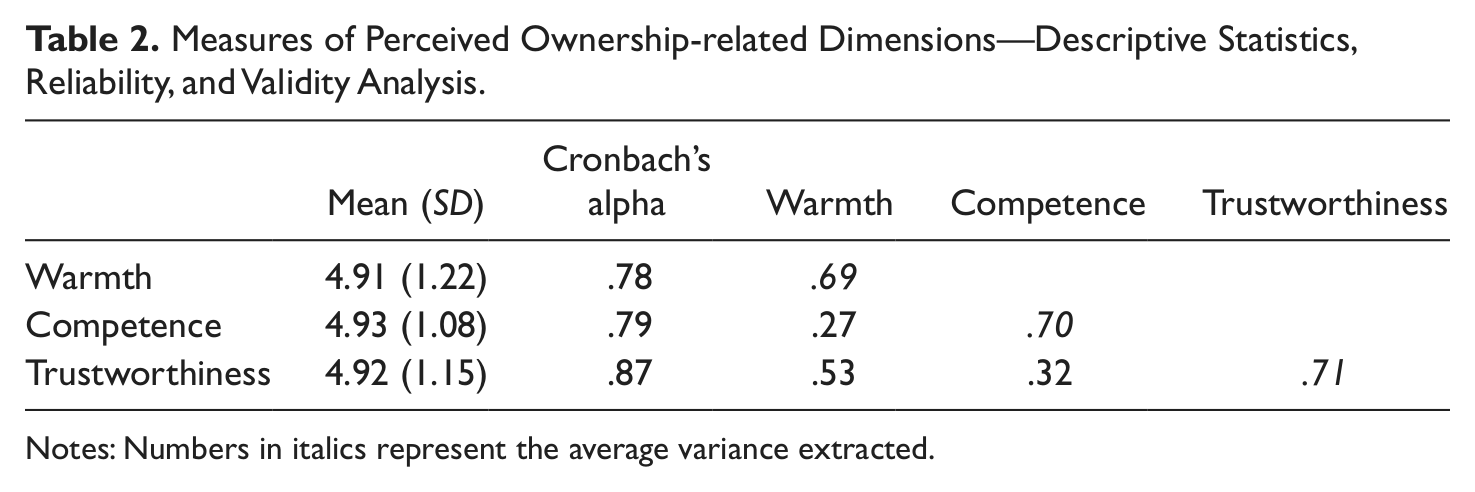
Notes: Numbers in italics represent the average variance extracted.
To validate Hypotheses 1b, 2b, and 3b, we conducted a regression analysis using group mean-centered values of the independent variables. As Table 3 shows, the variance inflation factors illustrate low multicollinearity and the adjusted R2 of .33 indicates moderate to good overall model fit. In contrast with Hypothesis 2b, perceived warmth does not affect individuals’ hospital quality beliefs. As Hypotheses 1b and 3b predict, both competence and trustworthiness positively influence individual beliefs about hospital quality. To control for possible confounding effects, we considered perceived relevance of ownership status as well as age and sex as independents but neither perceived relevance of ownership status (b = −.04, t = −1.00, p > .90) nor age (b = −.01, t = 1.58, p > .90) and sex (ΔR2 = .003, p > .90) have a significant effect on individuals’ hospital evaluations.
Effects of Perceived Ownership-Related Dimensions and Demographics on Patients’ Beliefs—Regression Analysis.
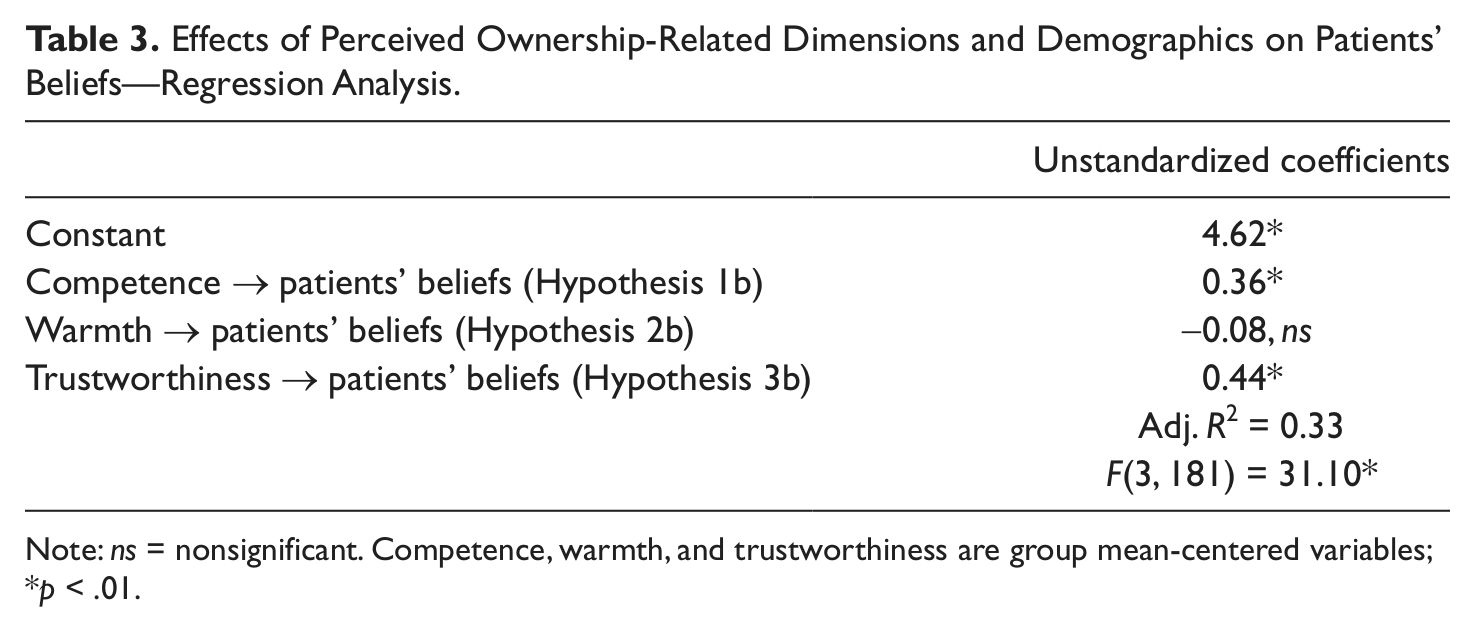
Note: ns = nonsignificant. Competence, warmth, and trustworthiness are group mean-centered variables;
p < .01.
To evaluate ownership-related differences in hospital perceptions, we conducted one-way analyses of covariance. To control for possible confounding effects, we again considered perceived relevance of ownership status as a covariate, finding that perceived relevance of ownership status has no significant effect on the ownership-related dimensions (p >. 90). As Table 4 shows, we find support for Hypothesis 2a because warmth differs significantly with ownership status (p < .95). A post hoc test reveals specifically that perceived warmth is significantly higher for nonprofit hospitals (nonprofit, M = 5.30, SD = 1.20; religious nonprofit, M = 5.25, SD = 1.09) than for those with for-profit status (M = 4.31, SD = 1.24) or public hospitals (M = 4.82, SD = 1.12). In line with Hypothesis 2a, perceived competence is significantly lower (p < .95) for nonprofit hospitals (M = 4.97, SD = 1.03) and religious nonprofit hospitals (M = 4.67, SD = 1.23) than for for-profit hospitals (M = 5.29, SD = .94). Compared with public hospitals (M = 4.78, SD = 1.05), the perception of competence is similar. Finally, as we predicted in Hypothesis 3a, nonprofit (M = 5.16, SD = 0.929), religious nonprofit (M = 5.23, SD = 1.21), and public (M = 4.78, SD = 1.05) hospitals significantly (p < .95) outperform for-profit hospitals (M = 4.51, SD = 1.25) with respect to perceived trustworthiness.
Ownership-Related Differences in Evaluation Dimensions–Mean Values.

Note: Values in parentheses are the standard deviations.
Conclusions
Using data from a German sample, our experimental study offers new insights into the relevance of ownership status for patients’ hospital perceptions and quality beliefs. First, our exploratory study confirms that warmth, trustworthiness, and competence are separate dimensions in hospital evaluations. Second, nonprofit hospitals are perceived as more trustworthy and warm but less competent than for-profit institutions in line with Handy et al.’s (2010) research on competitive advantages of nonprofits as well as research on general firm stereotypes (Aaker et al., 2010). In addition, the perceptions of religious nonprofit and other nonprofit hospitals are similar. Third, only trustworthiness and competence influence patient hospital evaluations. In particular, the results of our study indicate that from patients’ perspectives, trustworthiness is the most important dimension, possibly because health services represents a typical credence good where consumers have difficultly ascertaining actual quality even after consumption.
Any interpretation of our study results must include limitations. First, one has to consider limitations due to methods since patients process available information in more depth when they actually make hospital choices (Petty & Cacioppo, 1986). Patients will actively seek and process additional information (e.g., from hospital report cards) but, in the presence of too much and conflicting information, they may experience confusion (Walsh & Mitchell, 2010). One strategy to reduce confusion is to rely on easily available information cues such as ownership status (Marshall & McLoughlin, 2010). We focused only on the hypothetical scenario of a routine procedure (nonacute appendicitis) necessitating an inpatient stay, a diagnosis that might affect the relevance of trustworthiness and competence for patients’ quality beliefs. The results might differ if participants instead imagined, for example, medical treatment that demanded intensive care (Elliott, Kanouse, Edwards, & Hilborne, 2009; Weng, 2006).
Second, this investigation does not focus on behavioral intentions or actual behavior. Rather, we consider the effects of ownership-related dimensions on patients’ quality beliefs (see Figure 1), which is presumably of major significance for consideration set formation. Hence, we did not include the relevance of the attending outpatient physicians, of proximity (i.e., going to the nearest hospital; Adams & Wright, 1991; Luft et al., 1990), and of social network effects (e.g., recommendations of family and friends) among other factors. These determinants of hospital choice may influence patients when they evaluate alternatives in their consideration set.
Third, some patients in the United States, unlike Germany, have no or limited choice about what hospital they go to (Kurz & Wolinsky, 1985). As a member of a HMO, patients receive medical services from health care providers that the HMO has contracted with to make up its network (Town & Vistnes, 2001). In that case ownership-related dimensions and quality beliefs might still be relevant because the quality of the selectable providers is a primary variable in HMO choice (Scanlon, Chernew, & Lave, 1997). The ownership status of the selectable hospitals could be a first, easily accessible, informational cue about the available HMOs. Moreover, unfavorable perceptions of ownership-related dimensions and low-quality beliefs might have detrimental effects on satisfaction with health plans. As another reason for limited choice, in remote rural areas, primary care frequently is provided by a single hospital. Within these settings, hospital ownership is not a factor in choosing a hospital; in particular, rural hospitals in the United States are in many cases organized on a nonprofit basis (Ricketts & Heaphy, 2000). However, due in part to the costs and inconvenience of the journey to the hospital (Lishner, Levine, & Patrick, 1996), low performance on the ownership-related dimensions or quality beliefs might mislead reluctant or disabled patients not to seek medical treatment.
Our results imply that nonprofit hospitals should increase communication about their ownership status. Few nonprofit hospitals signal their ownership status (Malani & David, 2008), thus ignoring the existence of ownership-related attitudes among patients. They fail to take advantage of a way to improve their image and compete more effectively with for-profit competitors. Such a communication strategy could increase public awareness of ownership considerations and improve patient perceptions of nonprofit hospital. The results of Schlesinger et al. (2004b) imply that an increased understanding of the meaning of nonprofit-status goes along with more favorable perceptions of the relative performance of nonprofit hospitals. Hence, we conclude that the positive effect of communicating nonprofit status may increase understanding what nonprofit means. The implementation of these communication strategies is easy and demands little cost, including visible placement of nonprofit status on websites, letterheads, and brochures. For patients, ownership status also is easy to grasp (Malani & David, 2008) and outperforms other quality cues such as mortality rates and quality records. However, nonprofit hospitals must overcome the ownership-induced discrepancy between their actual and perceived competence by addressing the negative effect of nonprofit status on perceived competence through communication, including benchmarks and quality reports, about the hospital. In Germany, unlike the United States, these communication strategies about nonprofit status circumvent legal prohibitions against advertising in the hospital sector (Tscheulin & Helmig, 1998). Moreover, ownership status could make up for weak hospital brand effects because branding plays a special role for service firms. Strong brands increase trust in intangible products and help customers evaluate service quality (Berry, 2000). Similar to a hospital’s image, its nonprofit status could provide a branding-type function and improve its competitive position (Javalgi et al., 1992).
Our study suggests several possibilities for further research. First, researchers might examine the relevance of ownership to physicians, who are important decision makers in health care markets (Burns, Wholey, & Huonker, 1989). For example, Schlesinger, Quon, Wynia, Cummins, and Gray (2005), in a study of the U.S. health care system, find that physicians’ views of for-profit health plans tend to be rather negative because they perceive cost-oriented quality reductions and attempts to manipulate patients. Physicians should serve as outside endorsers who can increase patient perceptions of the trustworthiness of the hospital (Naidu, Parvatiyar, Sheth, & Westgate, 1999). Second, the similarity of our results for religious nonprofits and nonprofits may neglect spirituality as a possible, perceptual, ownership-related dimension (Büssing, Ostermann, & Matthiessen, 2005; Nix & Gibson, 1989). To elaborate more on this point, future research could add spirituality as an ownership-related dimension. Third, ownership conversions in the hospital sector remain controversial and continue to attract media attention (Claxton et al., 1997), which makes further research into the consequences of ownership conversions critical (Gray & Clement, 2002). Do patient or physician perceptions of a hospital change in accordance with ownership conversions? Can new hospital owners benefit from existing ownership-related perceptions of the former owner? Context effects likely influence the potential image transfer as well. For example, a takeover of an insolvent nonprofit hospital could be valued differently from a hostile takeover by a private investor.
Fourth, ownership perceptions also might affect postchoice evaluations. The trustworthiness-based competitive advantage of nonprofit hospitals might provide a kind of quality insurance in the case of a service failure, resulting in fewer complaints and better postchoice evaluations. Theoretical support for this proposition comes from analyses of differences in failure attributions. Patients may expect fewer service failures by a nonprofit hospital. However and in case of a service failure, higher disconfirmation of expectations about the service quality would result in higher dissatisfaction with the nonprofit hospital. Accordingly, Tangcharoensathien, Bennett, Khongswatt, Supacutikul, and Mills (1999) find differences in patient satisfaction, depending on hospital ownership. Fifth, the current study does not differentiate between chain hospitals and independently owned hospitals (e.g., municipal hospitals). The brand name recognition of chain hospitals may be higher due to chain brand management (Cuellar & Gertler, 2003; Kim et al., 2008). One might expect that variations in brand awareness may affect ownership-related differences in hospital perception.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.