
Abstract
This article tests the theory that anxiety about death causes feelings of lack of control, which, with other factors, results in reluctance to donate organs, despite endorsement of the act. Using a survey of U.S. and U.K. registered organ donors and unregistered adults (N = 777), we tested the impact of trust in medical professionals, perceived importance of information on the transplant processes, anxiety regarding loss of control at one’s end-of-life, and a prosocial view of organ donation on willingness to register as donor. Structural analyses show that control mediated the associations of trust and information with willingness, while prosocial did not predict willingness. The findings explain the gap between stated attitudes and actual behavior, and suggest that framing donor card registration and organ donation as a way to gain control over the loss of agency in death and dying may encourage organ donation.
Demand for human organs suitable for use as transplants far exceeds supply, and only a minority of persons awaiting transplantation receive organs. To become an organ donor, one needs to register as such. Evidently, a gap exists between the number of people who say they support organ donation and those who are registered as donors: 85% of Americans support organ donation, but only 40% to 45% of individuals are registered (http://donatelife.net; Kessler & Roth, 2012). Consequently, in the United States, more than 21 people daily die waiting for a transplant. Various strategies to increase registration, such as opt-out systems (Johnson & Goldstein, 2003), promotion in transplantation wait-lists (Kessler & Roth, 2012), public education (DeJong, Drachman, Gortmaker, Beasley, & Evanisko, 1995), and financial incentives, have had little impact on registration rates (Arnold et al., 2002).
Research into registration rates suggests beliefs that indicate a desire to avoid death, the need to maintain bodily integrity for the afterlife, and concerns regarding unethical recovery of organs (Newton, 2011; Parisi & Katz, 1986). The theory of planned behavior (TPB) (Ajzen, 1991) is specifically relevant to the research of organ donation (Bresnahan et al., 2007; Park & Smith, 2007). In TPB, behavioral intention is the closest determinant of behavior, preceded by three independent constructs: subjective evaluation toward the behavior (attitudes), perception about social expectations related to the behavior (subjective norms), and the perceived difficulty of completing a particular behavior (perceived behavioral control) (Ajzen, 1991). Furthermore, beliefs and evaluation of behavioral outcomes affect attitudes, normative beliefs and motivation influence subjective norms, and control beliefs and perceived power influence perceived behavioral control (Figure 1). Finally, intention to incorporate the behavior also increases the likelihood of action (Baban & Craciun, 2007). Although most people hold positive attitudes toward organ donation (U.S. Department of Health and Human Services, 2013), many will not register to be donors, as other variables effect a gap between attitudes and behavior.
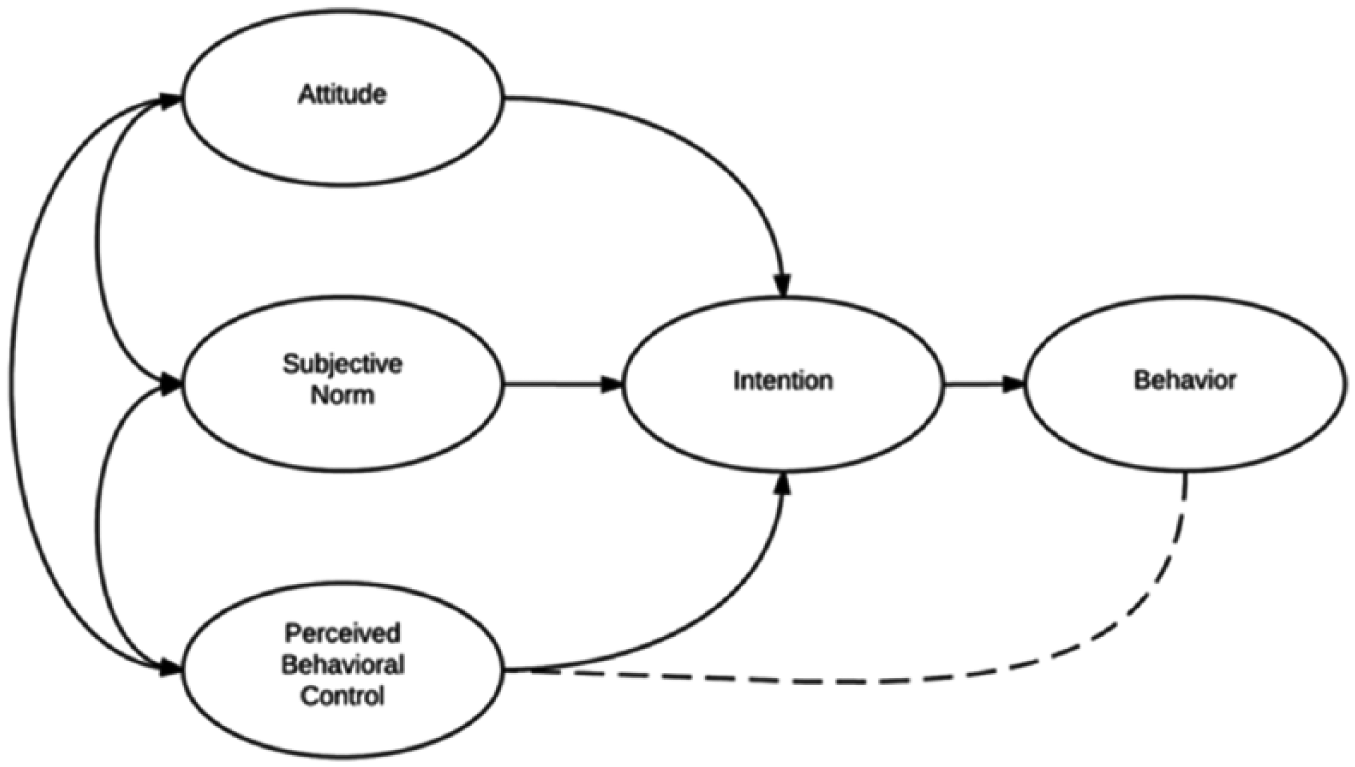
Theory of planned behavior (Ajzen, 1991).
Trust, particularly in the medical system, is strongly related to autonomy and control when considering the question of consent in the context of bioethics (O’Neill, 2002; Sanner, 2006). Andaleeb and Basu (1995) found that trust is a better predictor of blood donations than is altruism. Siminoff and Mercer (2001) found that nondonor families have low trust in an equitable organ distribution system. In Brazil, mistrust in the health system is the most frequent reason stated for not registering as donors among medical students (Dutra et al., 2004). In Spain, messages that increase confidence in the transplant system improved dispositions toward organ donation (Conesa et al., 2004). Trust levels among different ethnicities correlate with donor card registration rates (Minniefield, Yang, & Muti, 2001; Siminoff & Arnold, 1999; Siminoff, Burant, & Ibrahim, 2006). Alden and Cheung (2000) found that trust in doctors correlated with improved attitudes and behavioral tendencies toward organ donation. The differences between African Americans and Whites in the willingness to donate blood for genetic research disappeared after controlling for trust (Bussey-Jones et al., 2010).
Information is another important factor affecting registration. Nondonors tend to believe myths about organ donation more than donors do (Horton & Horton, 1990; Morgan, Miller, & Arasaratnam, 2002; Sanner, 2006; Sanner, Hedman, & Tufveson, 1995). Sanner (2006) showed that “facticity” (p. 143)—knowledge of the facts pertaining to organ donation, and particularly those relating to the donor side—increase donations. However, rational consideration of facts is affected by the psychological discomfort caused by discouraging information. Siegel and associates (2010) looked into information-seeking behavior and noted that most persons are “passive-positives” (have not registered despite having positive attitudes toward organ donations) and seldom seek information proactively.
The need for control is particularly important in philanthropy of the body decisions (Giles & Cairns, 1995; Hyde & White, 2009). Bagozzi, Lee, and Van Loo (2001) found that decisions to donate bone marrow are volitional, guided by attitudinal and normative control. Reid and Wood (2008) surveyed blood nondonors and found that perceived behavioral control, with subjective norm and time-related barriers, affect intent to donate. Bresnahan et al. (2007) found a need for control effect on donation decisions in Japan, South Korea, and the United States. In addition, both need for information and trust are critical contributors to a sense of control or agency (Bandura, 1997).
Consequently, it is theorized that lack of control associated with natural anxiety about death (Radecki & Jaccard, 1997), along with lack of relevant information (Morgan & Miller, 2002; Tumin et al., 2014) and low trust (Siminoff et al., 2006; Tumin et al., 2014), reduce willingness to register as donors, regardless of the positive beliefs and attitudes about the act and its prosocial benefits. In addition, it is posited that the effect of both trust and need for information on willingness to donate is mediated by lack of control.
Method
Participants
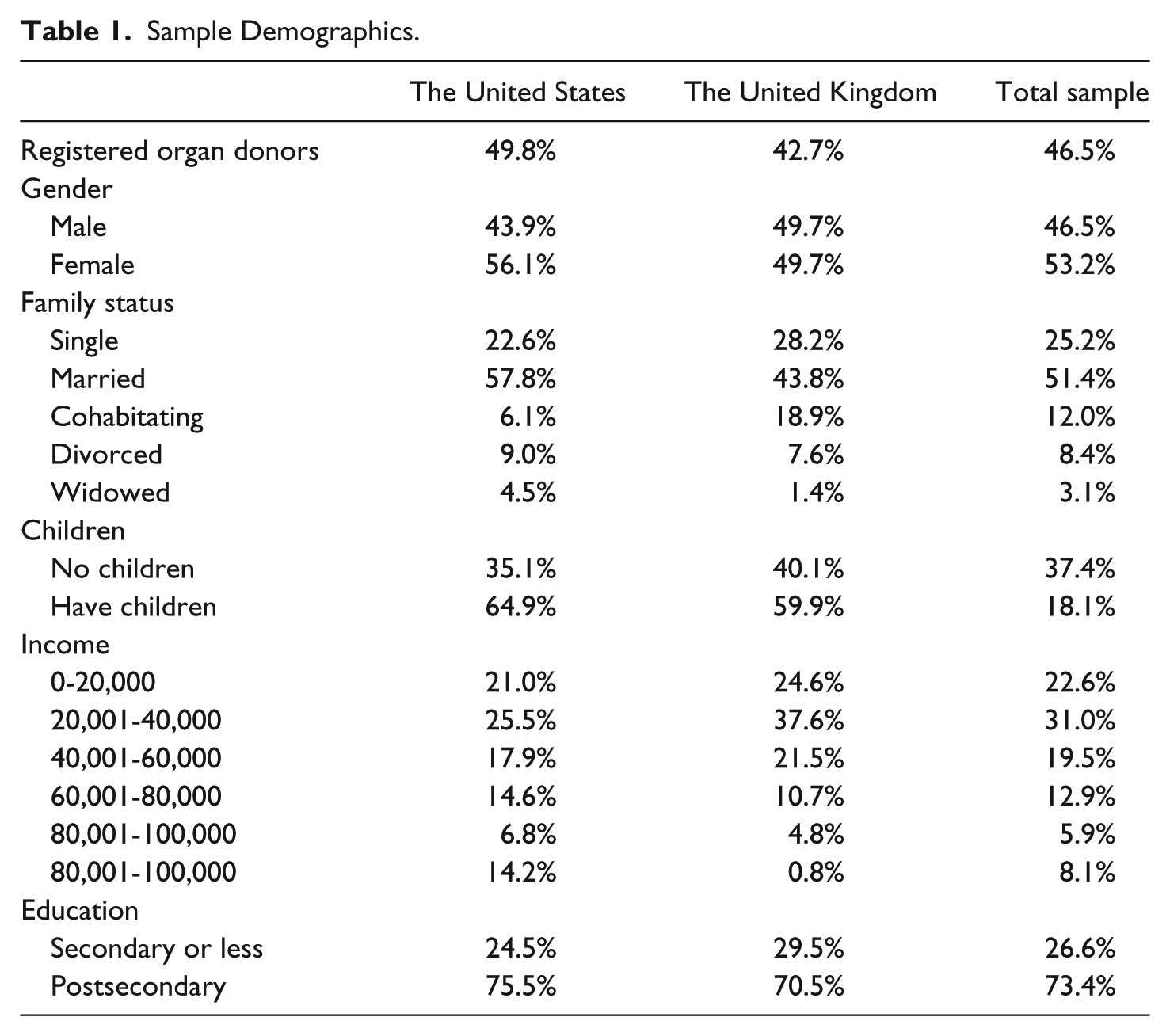
Participants were surveyed online using Qualtrics data collection systems, which aggregates multiple sample partners, each using randomized sampling proportional to the general population. Respondents (adults over 21) join the panels voluntarily, and were sent an email invitation to participate, without specific details about the contents of the survey, to avoid self-selection bias. The incentive was the equivalent of US$1 or £1. Sample size was 777 (423 United States, 354 United Kingdom), with response rate of 11.8% (14.2% United States, 9.4% United Kingdom). All participants answered all questions; there were no missing data. Sample demographics are presented in Table 1.
Sample Demographics.
Measures (see Table 2)
Predictors
Lack of control
Lack of control measured anxiety regarding compromised agency when relating to one’s end-of-life. Participants rated concern that “I might not receive necessary medical attention” (marker), “organs will be removed before I am dead,” “organs will not go to those who really need them,” and “how my body will be treated after death.”
Latent Variables and Corresponding Indicators.

Note. Correlated errors indicated by brackets.
Prosocial
Four items measured a prosocial view of organ donation: “organ donations help save lives” (marker), “organ donations advance medical research,” “organ donations give someone a better quality of life,” and “donating organs is the right thing to do.”
Need for information
Four items asked how important it is to have information about what happens to a donor’s body after harvesting (marker variable), the transplant processes, efforts to save registered donor’s life, organ usage, and necessity.
Trust
Two items captured general trust in other people, “How often do you trust other people?” (marker variable) and “Do you believe that most people can be trusted?” and two measured specific trust in medical professionals, “To what extent do you trust doctors?” and “To what extent do you trust nurses?”
Outcomes
Registration status (Model 1)
The outcome variable was a single item measuring whether participants are registered with the relevant registry in their country (“Are you registered as an organ donor?”).
Willingness to donate (Model 2)
A single item asked participants who were not already registered as donors: “If asked now, would you be willing to register with your state’s organ donor registry?”
All items used in this study were rated on a 7-point scale. See Table 3 for descriptive statistics, correlations, and Cronbach’s α validity.
Descriptive Statistics, Measures, and Outcome Variable.

p < .01.
Data analysis
Confirmatory factor analyses (CFA), structural equation modeling, and mediation analyses were conducted using MPlus 6 (Muthén & Muthén, 2012), using a robust weighted least squares parameter (WLSMV) to simultaneously estimate the ordinal and categorical outcome variables. Indirect paths were estimated using a 5,000 resamples bootstrap analysis (Preacher & Hayes, 2008) with 95% confidence level. Similar results were achieved when controlling for gender and religiosity; therefore, the more parsimonious model is presented.
Results
Model 1—Predicting Registration Status
The sample included registered and nonregistered individuals (N = 777). Skewness was between −1 and 1 for 13 of 17 variables; all indicators of the prosocial construct were negatively skewed (from −1.047 to −2.331), as expected in questions endorsing normative morals, and consequently should be interpreted with caution.
CFA
CFA was performed to test the appropriateness of the theorized measurement model (Figure 2). Root mean square error of approximation (RMSEA) (.046, 90% confidence interval [CI] = [.039, .052]) and weighted root mean residual (WRMR) (.906) indicated a good model fit (Yu & Muthén, 2002); comparative fit index (CFI) (.934) and Tucker–Lewis index (TLI) (.912) indicated a satisfactory model fit (Garrido, Abad, & Ponsoda, 2016; Yu, 2002).
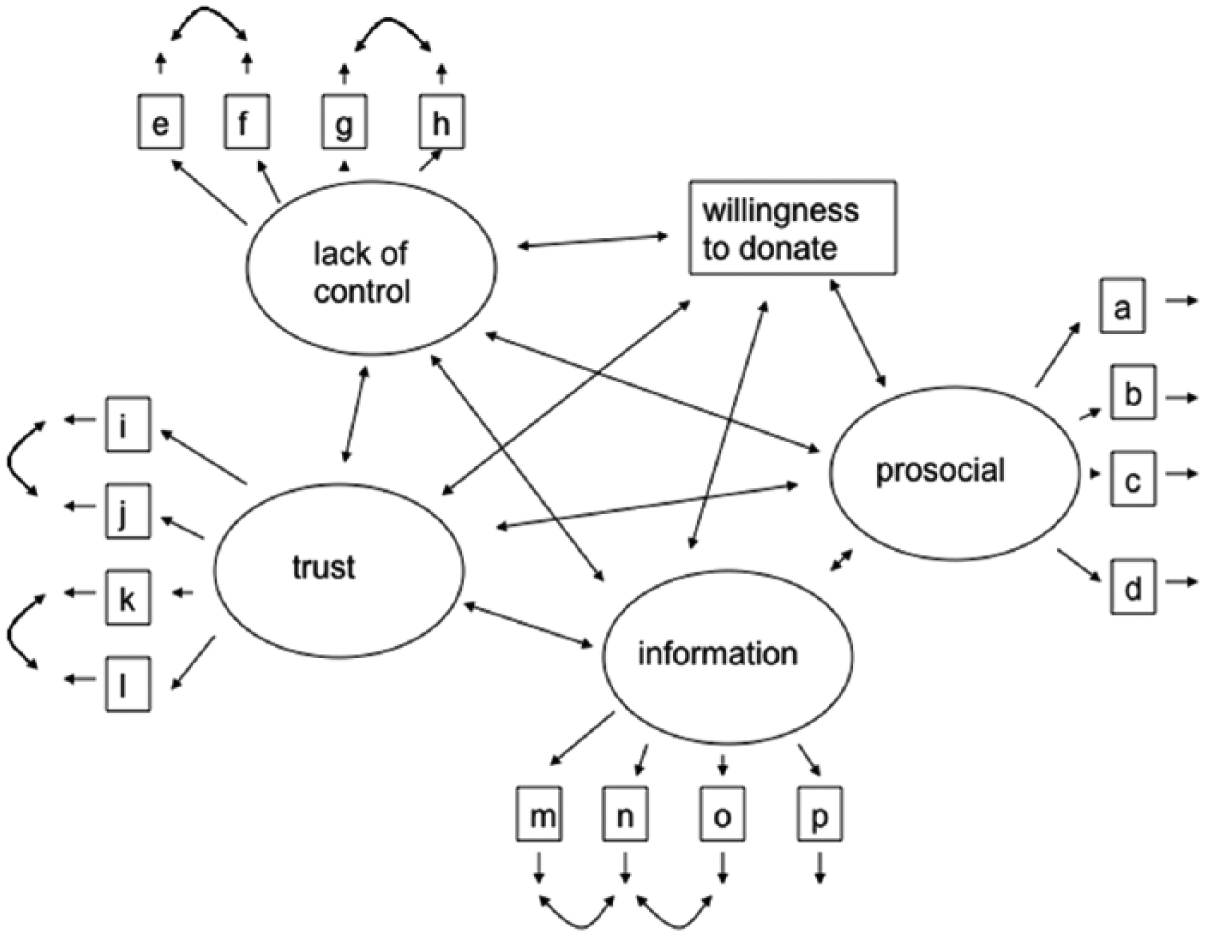
Theoretical model tested in confirmatory factor analysis.
Structural model
No paths were eliminated from the measurement model so fit indices remain unchanged. As predicted, need for information was positively associated with lack of control (b = .506, SE = .081, β = .306, z = 6.231, p < .05; see Figure 3). Trust was negatively associated with lack of control (b = −.575, SE = .102, β = −.282, z = −5.623, p < .05). Need for information was marginally associated with registration status (b = .085, SE = .049, β = .087, z = 1.731, p = .08), whereas the association between trust and registration status was not significant (b = .035, SE = .067, β = .029, z = .527, p > .05). Lack of control was negatively associated with registration status (b = −.200, SE = .030, β = −.338, z = −6.730, p < .05).
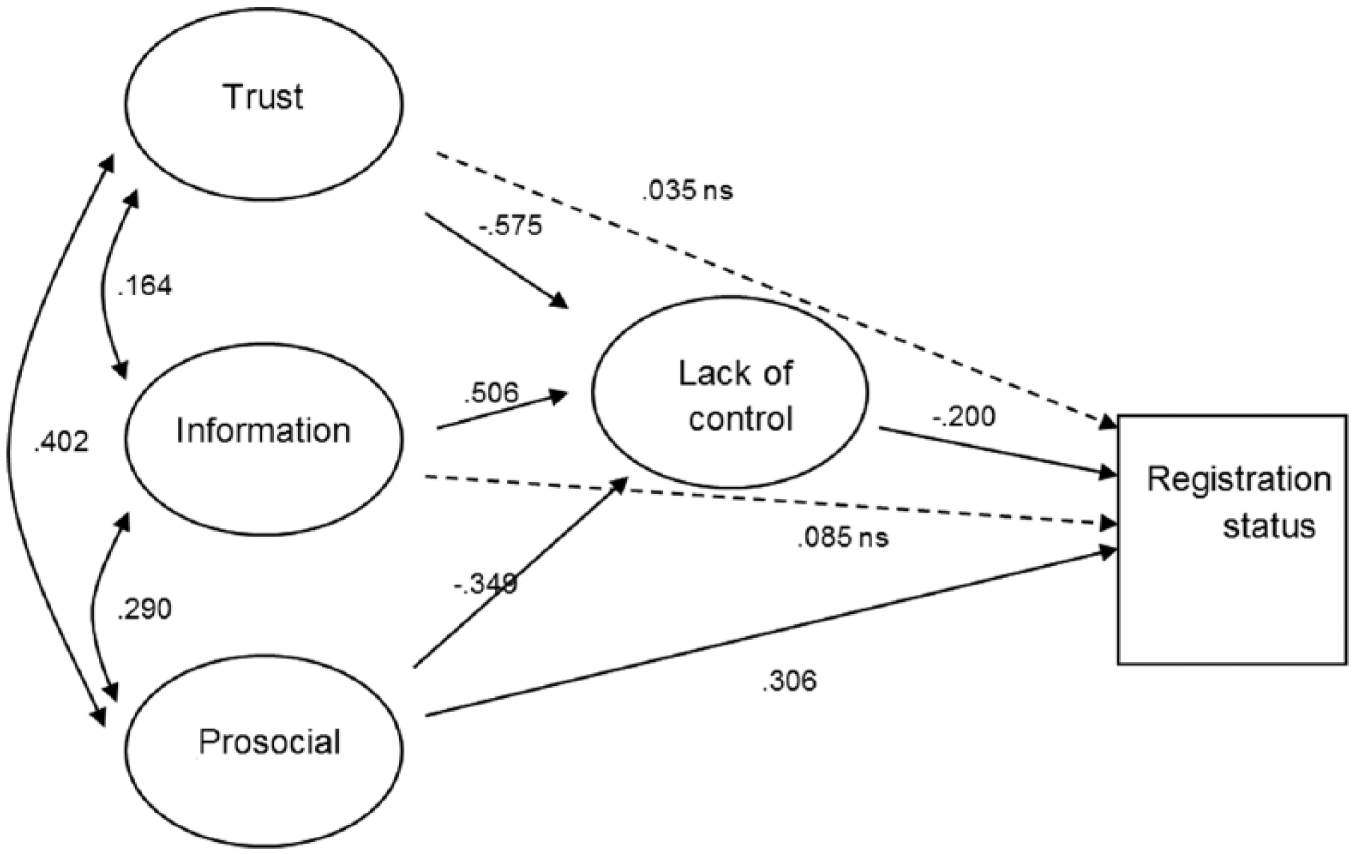
Structural model including mediation paths, Model 1.
With the inclusion of both registered and unregistered participants, prosocial was expected to be predictive of registration status. Registered donors are likely to endorse prosocial statements such as “donating organs is the right thing to do” because it lines up belief with matching behavior. In contrast, unregistered participants who believe that organ donation is morally good may be reluctant to show full endorsement or may experience cognitive dissonance between belief and behavior. Despite a distinct ceiling effect for all four prosocial indicator variables, prosocial was negatively associated with lack of control (b = −.349, SE = .074, β = −.296, z = −4.739, p < .05) and positively associated with registration status (b = .306, SE = .062, β = .439, z = 4.970, p < .05).
Mediation analysis
As predicted, lack of control mediated associations between need for information and registration status (CI = [–.061, –.151]), trust and registration status (CI = [.182, .060]), and prosocial and registration status (CI = [.104, .042]). Although the direct path between both trust and need for information and the outcome variable were not significant, the zero-order correlations were significant—trust: r(777) = .309, p < .001; need for information: r(777) = .114, p = .023. These results indicate that lack of control significantly mediated all three theorized associations with registration status (trust, need for information, and prosocial).
Model 2—Predicting Willingness to Donate
Whereas Model 1 analyzed the full sample, in Model 2, only participants not registered to donate organs were included: 415 adults over 18 years of age (212 United States, 203 United Kingdom). All 415 participants answered all questions; there are no missing data. Skewness was between −1 and 1 for 14 of 17 variables; three indicators of the prosocial construct were slightly negatively skewed (−1.620 to −1.194), as expected in questions endorsing normative morals.
CFA
The CFA demonstrated good model fit between the observed covariance and the a priori model shown in Figure 2 (RMSEA = 06, 90% CI = [.051, .069], CFI = .963, and TLI = .952). Because of sample size and model complexity, chi-square test is a less informative measure, χ2(104) = 257.52, p < .001, so the Hoelter index was computed; results estimated that N = 208 would render χ2 nonsignificant, further supporting good model fit.
Structural model
No paths were eliminated from the measurement model, so fit indices remain unchanged. Results (see Figure 4) reveal that, as predicted, need for information was positively associated with lack of control (b = .653, SE = .139, β = .407, z = 4.690, p < .05), and trust was negatively associated with lack of control (b = −.805, SE = .280, β = −.271, z = −2.872, p < .05). Need for information was also positively associated with willingness to donate (b = .662, SE = .150, β = .322, z = 4.409, p < .05) whereas the association between trust and willingness to donate was not significant (b = .235, SE = .253, β = .062, z = 0.931, p > .05). Lack of control was negatively associated with willingness to donate (b = −.261, SE = .087, β = −.204, z = −3.019, p < .05).
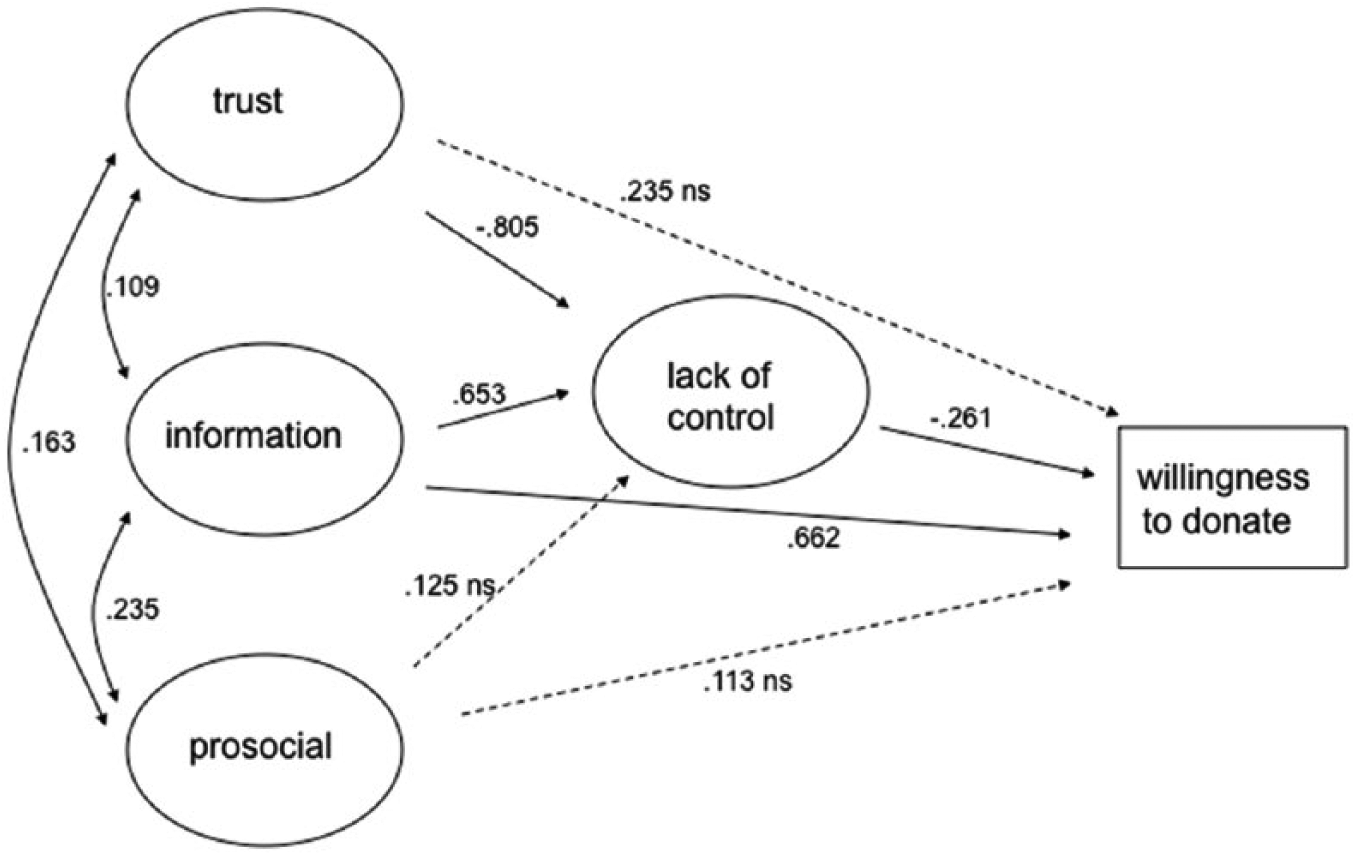
Structural model including mediation paths, Model 2.
The comparison model was contained within the structural model above, where the alternative is a significant contribution of prosocial to the outcome variable or to lack of control or to both. Importantly, prosocial was not significantly associated with either lack of control (b = .125, SE = .067, β = −.129, z = −1.854, p > .05) or willingness to donate (b = .113, SE = .069, β = .091, z = 1.651, p > .05).
Mediation analysis
Indirect effects were tested using bootstrapping analysis finding that, as predicted, lack of control mediated associations both between need for information and willingness to donate (CI = [–.314, –.049]) and trust and willingness to donate (CI = [.046, .418]). Note that while the direct path between trust and the outcome variable is not significant, the zero-order correlation is marginally significant, r(415) = .125, p = .069. Furthermore, while Baron and Kenny’s (1986) rules suggested that indirect effects should not be tested if the correlation is not significant, Zhao, Lynch, and Chen (2010) pointed out that there is no need for significant zero-order correlation if a × b and c are opposite signs, as in this case. These results indicate that lack of control significantly mediated the theorized associations between both trust and need for information and willingness to donate.
Discussion and Implications
The results support the proposed theoretical model in which a nonregistered person’s willingness to register for organ donation is driven by trust and the need for information, mediated by feelings of lack of control. Specifically, lower trust and greater need for information contributed significantly and independently to feelings of lack of control. Increased feelings of lack of control, in turn, significantly reduced willingness to donate organs. Feelings of lack of control were found, through mediation analysis, to be the intervening variable between trust and lack of information and the outcome measure, willingness to donate. Critically, endorsement of prosocial goals did not significantly affect either lack of control or willingness to donate. No matter how much one may believe that donating organs is morally justified, one’s decision to sign up is a function not of altruistic or normative moral motivations, but of other, more self-directed, factors. Anxiety associated with thinking about one’s own death appears to subordinate social concerns and future benefits to the immediate—and likely irrational—fears of the individual.
Prior research indicates that organ donation is motivated by incentives that benefit the potential donor (Andreoni, 1990; Cialdini, Darby, & Vincent, 1973). For example, a decision to become an organ donor can enhance self-esteem, feelings of pride, and positive emotions, and in some instances provides individuals with the opportunity to “keep on living” after death (Hessing & Elffers, 1987; Parisi & Katz, 1986; van den Berg, Manstead, van der Pligt, & Wigboldus, 2005). “After death” may provide a potent clue. Clearly, the consideration of organ donation evokes the classic tension between momentary temptation versus long-term goal. Much research has investigated this tension in the self-regulation and motivation literature, for example, in dieting, exercise, finance, and addiction (Bandura, 1997; Baumeister & Vohs, 2003; Gollwitzer & Oettingen, 2001). But what is so appealing about not registering to donate organs? If the overarching goal is to do the right thing, to fulfill a prosocial norm, then perhaps the role of temptation is played by “temporary immortality,” that is, denial of the certitude of death. Thinking about death of the self is associated with anxiety, in particular, specific fear of loss of control (Penson et al., 2005). Normative prosocial/moral goals are often subordinated by anxiety (Wells & Matthews, 1994; Wells & Papageorgiou, 1998). The notion that self-focused anxiety (personal distress) robustly discourages altruistic behavior (Batson, 1991; Davis, 1980, 1983, 1996) has been well established in the research on empathy.
The salience of lack of control in our model calls for further exploration of its construct validity. In this context, an interesting path to explore would be to establish discriminant validity between what we called “anxiety regarding situations in which agency is compromised when relating to one’s personal end-of-life” and death anxiety caused by mortality salience as it is used in Terror Management Theory (Greenberg, Pyszczynski, & Solomon, 1997). Terror Management Theory has been used to study organ donation decisions (e.g., Hirschberger, 2010; Jain & Ellithorpe, 2016). In Terror management theory, human motivation is affected by the anxiety associated with awareness of their own mortality, and individuals use elaborate symbolic defense mechanisms, mainly investment in cultural worldviews and self-esteem, to buffer the potential for death anxiety. It may be argued that lack of control in the context of organ donations would evoke, or at least is correlated with mortality salience and death anxiety. In our study, the measurement of lack of control places the respondents’ concerns specifically in the context of organ donations and TPB, but future research should contrast the two theories and aim to explore discriminant validity of these constructs.
This study addressed only opt-in organ donation, as practiced in the United States and the United Kingdom. Future research could investigate the mechanisms driving opt-out choice, in which one is automatically a registered donor but can actively ask to be removed from the list of donors. In this case, normative goals may be more influential, and the active choice to not comply may be construed as distinctly heretical. In addition, further investigations including measures of trait and/or state empathy could prove enlightening. For example, the Personal Distress subscale of the Davis Interpersonal Reactivity Index (Davis, 1980, 1983) might be expected to augment lack of control, whereas perspective taking may actually reduce it.
Institutions that would like to encourage organ donation among the skittish might best frame donor card registration as a way to gain control over the loss of agency in death and dying. Presented, perhaps not quite so starkly, and, as with many marketing strategies, a little less directly. Emphasizing that registering for organ donation is a way to maintain control at end of life could prove empowering to many. Likewise, favoring transparency in the process, providing easily accessible sources of information, and highlighting the expert status and professionalism of the medical teams involved could bolster confidence and reduce feelings of lack of control. Accepting the prosocial side as established (and largely irrelevant), campaigns should seek to reframe donating as a means of gaining control over illness and death. While the language and nuances of presentation require further inquiry, the underlying message holds a tantalizing hint of immortality. All questions of cultural and social value aside, such promises can prove to be quite alluring.
Footnotes
Acknowledgements
The authors wish to thank Ayelet Gneezy (UCSD Rady School of Management) for her imperative contribution to the research that produced this article. They are thankful to Uri Gneezy (UCSD Rady School of Management) and to Hila Riemer (BGU Guilford Glazer Faculty of Business and Management) for their comments on earlier versions of the article. They thank the reviewers for their insightful comments, which helped them bring the article to its current form.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the BGU IRB (#HK10062013).