
Abstract
Background
Over the years, it has been observed that adverse drug reaction (ADR) is a major cause of mortality and morbidity and a major cause of concern for all healthcare professionals. ADR is a leading cause for hospitalisation and increases the financial burden of the patient. Thus, it is imperative that we need steps and strategies to decrease the burden of ADRs and effectively reduce the cost of therapy to treat ADR.
Objective
This study evaluated the pattern, severity, and preventability of ADRs in a tertiary care hospital.
Methods
A retrospective observational study of all the ADR reports due to medications submitted to the ADR monitoring centre in a Northern Indian tertiary care hospital from October 2017 to December 2019. Causality assessment of the ADRs was done using the WHO-UMC causality assessment scale, and the severity was assessed using the modified Hartwig scale. Furthermore, the preventability of the ADR was assessed using the Schumock and Thornton scale.
Results
A total of 252 ADRs were reported. A maximum number of the ADRs (33%) were due to antimicrobials followed by analgesics (16%) and antihypertensives (10%). Amongst the analgesics, a majority of ADRs were associated with Diclofenac (16 ADRs). Amlodipine was associated with maximum ADRs (10) amongst the antihypertensives. The ADRs of gastrointestinal systems (34.5%) were most common among all system organ class (SOCs) followed by skin and subcutaneous tissue disorders (32%). Majority of ADRs were probable and mild in severity. According to the Schumock and Thornton preventability scale 69% were not preventable while 12% were definitely preventable.
Conclusions
Antimicrobials were associated with majority of ADRs with gastrointestinal system being the most commonest organ involved. It was also observed that most of the ADRs were not preventable but some were definitely preventable. The awareness regarding preventability of ADRs needs to be emphasised and further studies to elaborate on the preventability of ADRs needs to be carried out.
Keywords
Introduction
Adverse drug reaction is defined as “a response to a drug which is noxious and unintended, and which occurs at doses normally used in man for the prophylaxis, diagnosis, therapy of disease, or for the modifications of physiological function.” 1 It should be differentiated from an adverse event. An adverse event is any untoward medical occurrence that may present during treatment with a pharmaceutical product but which does not necessarily have a causal relationship with the medicinal product. 1
Adverse drug reactions (ADRs) due to medications have been observed as a major cause of concern for all healthcare professionals in the last decade. 2 ADR is one of the leading causes of hospitalisation, and it increases the financial burden of the patient. ADR accounts for around 4–30% hospital admissions in countries like USA and Canada. 3 In India also, approximately 3.7 %–32.7% people are affected due to ADRs and may require hospital admissions. 3 A 7-year surveillance study conducted in central India also observes that a majority of ADRs were preventable. 4 In a prospective study in a tertiary care centre of Southern India, it was observed that the average cost per patient in the management of ADRs was ₹3367. 5
Pharmacovigilance, as defined by the World Health Organization (WHO), is the science and activities relating to the detection, assessment, understanding and prevention of adverse events or any other possible drug-related problems. 6 India has launched Pharmacovigilance Programme of India (PvPI) under Ministry of Health and Welfare. Under this programme, ADRs are collected throughout the country and reported to National Coordinating Centre (NCC) Ghaziabad.
Currently there are 976 functioning adverse drug monitoring centres in the country (in medical colleges and corporate hospitals) as part of the Pharmacovigilance Programme of India. ADR monitoring at an institutional level can help uncover various problems related to drug use.6,7 In India, ADRs are most commonly reported spontaneously, which is voluntary in nature and can be done by healthcare professionals, nurses, pharmacists, etc. So far, this type of reporting has been the mainstay of various national and international drug safety evaluations. 8 However, spontaneous reporting structure suffers from the serious problem of under-reporting which can be as high as 98%. Pharmacovigilance programme aims to gathers ADRs from all healthcare facility in India, to create a database of drugs for its safety profile. ADR reporting is an essential tool to decrease the burden of morbidity and incidence of hospitalisation.9,10 Therefore, it is pertinent that each healthcare facility should also analyse its ADR data and find out the pattern and means to prevent the ADRs, thus improving the patient safety and welfare. This study will further help in identification of the key problem areas with respect to the pattern and preventability of ADRs so that measures can be taken to improve patient care in long run.
Objective
The study was conducted to analyse the pattern, severity and preventability of ADRs among patients of a tertiary care hospital in Northern India.
Methods
Study design and setting
This was a retrospective observational study to analyse pattern, severity and preventability of ADRs among patients of a tertiary care hospital in Northern India.
This study was conducted in the Department of Pharmacology at a 800-bed tertiary care government hospital for 2 years from October 2017 to December 2019. The study protocol was reviewed and approved by the Institutional Ethics Committee of North DMC Medical College and Hindu Rao Hospital (ref no. IEC/NDMCMC/2020/17).
Inclusion criteria
All suspected ADR reports due to medications submitted to the ADR monitoring centre of Northern Indian tertiary hospital under the Pharmacovigilance Program of India for a 2-year period (October 2017 to December 2019).
Exclusion criteria
ADR reports of patients with minimal or incomplete data.
Data collection and analysis
The suspected ADR reporting form as per the recommendation form the Central Drugs Standard Control Organisation was used for data collection. The ADRs were reported spontaneously by the healthcare professionals to the ADR monitoring centre of the hospital. The data from 2017 to 2019 were analysed in department of pharmacology.
The data analysed for demographic details of patients, suspected drug as well as concomitant drug history, route of administration, purpose for taking drug, improvement after discontinuation of drug were entered in the excel sheet.
Different scales were used to analyse the suspected ADRs collected during the above mentioned period in Department of Pharmacology. The causality of the reported adverse reactions was categorised according to the WHO causality assessment scale into certain, probable, possible, unclassifiable, unlikely and unclassified. The severity was assed using the modified Hartwig scale into mild, moderate and severe. Furthermore, the preventability of the ADR was assessed using the Schumock and Thornton scale into definitely preventable, probable and not preventable.11–13
Results
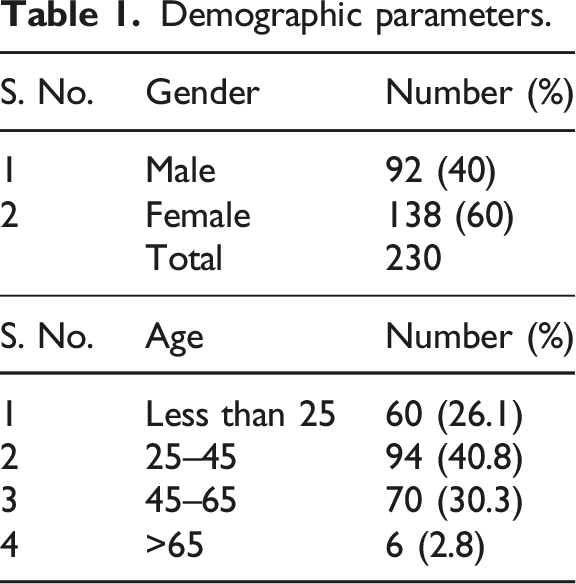
Patients’ demographics
Demographic parameters.
Department-wise distribution of ADRs
65.6% of ADRs were reported from the General Medicine Department followed by Dermatology, Gynaecology, Surgery and Orthopaedics (11.7%).
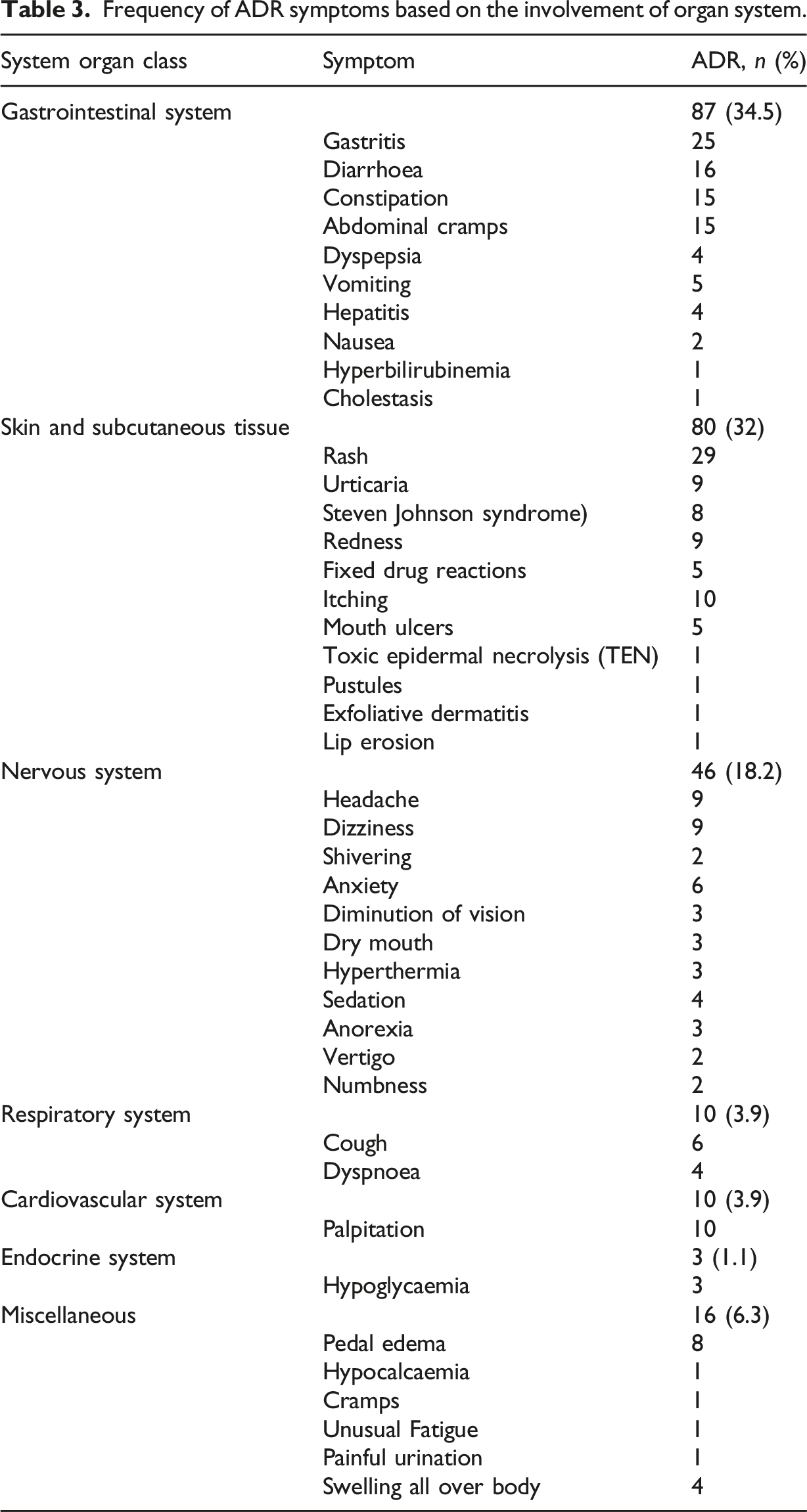
Frequency of ADR symptoms based on the involvement of organ system.
Type of ADRs and the implicated drugs
Among all the drug classes, antimicrobials were associated with the maximum number of the ADRs (30%) followed by analgesics (16%) and antihypertensives (10%).
Pharmacological drugs implicated in causation of ADRs.

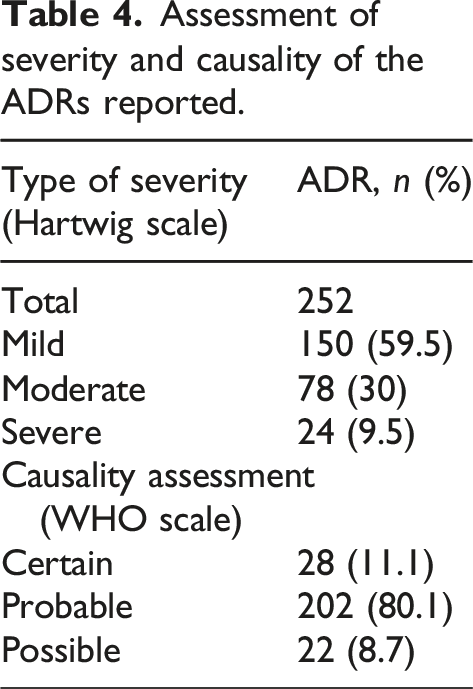
Causality assessment and severity
On causality assessment using the WHO-UMC Scale, majority (80)% ADRs were categorised as probable.
Assessment of severity and causality of the ADRs reported.
Seriousness and preventability of ADRs
Overall 24 serious ADRs were reported including 8 Steven Johnson Syndrome cases, two cases of Hepatitis, and one cholestasis and fixed drug eruption.
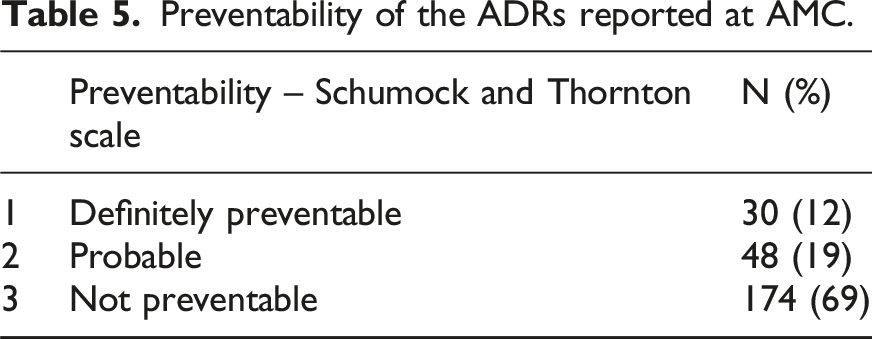
Preventability of the ADRs reported at AMC.
Discussion
The current study was initiated with the objective of determining the pattern, severity and preventability of ADRs in a tertiary care centre. This study observed that there is a female preponderance of the ADRs reported as compared to males. This is in conjunction to various previous studies where females were affected more than males. This could be attributed to the variable pharmacokinetic and pharmacodynamic profile of both genders.14,15
In the present study, it was noted that the antimicrobials group of drugs was the most common group to be associated with ADRs (30%). This could be attributed to rampant usage of antimicrobials. The maximum burden of ADRs was noted with ceftriaxone followed by amoxycillin and clavulanic acid combination and ofloxacin. Similar trend of ADRs associated with antimicrobials as a group has been observed in various studies.16,17 It was observed in an integrative review of various studies involving usage of antimicrobials and development of ADRs. The most probable explanation could be polypharmacy and irrational use of antimicrobial agents. It was observed that early detection and recognition of clinically important drug–drug interactions and ADRs by healthcare professionals are vital to identify patients who are at higher risk for such events.18,19
The second most common class associated with ADRs was observed to be analgesics (15.8%). The majority of ADR reports were associated with NSAIDs like diclofenac followed by paracetamol. Diclofenac has been attributed as the most common drug to have caused a majority of ADRs in various other studies as well. 20
Gastrointestinal system was most common organ system affected (34%) followed by skin (32%) and central nervous system (18%). Concurrent to our study various other studies also have shown gastrointestinal system to be the most common organ system affected.21,22 Contrary to present study few studies have demonstrated skin as the most common organ system affected. 23 This difference may be due to the variable patient profile and reporting in various centres.
As per the modified Hartwig and Siegel severity scale, the majority of ADRs (59%) were of mild nature followed by 30% moderate in nature and 9% severe in nature. Severity of an ADR increases not only the morbidity of patient but also increases the financial burden due to increased hospitalisation and treatment. In the case of moderate ADRs, the suspected drug was discontinued or changed. Meanwhile, some other treatment was given treat the ADR. Even though the stay of hospital not increased substantially in moderate ADRs, still it puts certain amount of financial burden on the patient. Corresponding findings were seen in a study by Keche et al. 24
In the present study as per the Schumock and Thornton scale, the majority (69%) of ADRs were not preventable; in another study, it was observed that 55.3% ADRs were unpreventable. This could be attributed to the fact that most of the ADRs were known adverse effects of the drugs. Definitely preventable were about 12% that could have been prevented by proper history of drug allergy and vigilant monitoring. 25 As it was observed in various studies that insufficient monitoring, inappropriate dosing and drug–drug interactions were causes of the preventable adverse reactions.26,27
Majority of ADRs on causality assessment revealed that most of the ADRs belonged to “possible” followed by “probable” category, this is consistent with that reported by other studies. 28
It was observed that the antimicrobials were associated with highest frequency of adverse drug reactions (ADRs), and the greatest number of ADRs were documented and reported from medicine department. Therefore, polypharmacy could be one of the reason for preventable ADRs. Therefore, we should emphasise on checking for any drug interactions when multiple drugs are prescribed to the patient, develop policies regarding antibiotics and which can further help to curb antimicrobial resistance and ADRs.
The awareness regarding preventability of ADRs needs to be emphasised, and further studies to elaborate on the preventability of ADRs need to be carried out. With analysis of the current data, we want to emphasise that it is the joint responsibility of all the healthcare providers to report ADRs, so that we can prevent any preventable ADRs in future.29–31
Limitations
One of the limitations of this study is that it was done in a single centre through spontaneous reporting. It was a retrospective study, so all the data which was collected were analysed.
Conclusion
In our study, it was seen that the antimicrobials group of drugs was the most common group to be associated with ADRs. The study indicates that a spontaneous reporting system was used to identify ADRs. We need to emphasise on active surveillance and detection of ADRs. Interventions aiming to reduce preventable ADRs should be incorporated and should be the main focus of the policy makers. By preventing ADRs, we can substantially reduce the burden of ADRs. The awareness regarding preventability of ADRs needs to be emphasised, and further studies to elaborate on the preventability of ADRs need to be carried out.
Statements and declarations
Footnotes
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.