
Abstract
Background
Patient safety is a global public health issue. It aims to reduce medical errors to ensure patients’ health and achieve the best possible outcomes.
Purpose
This study aims to examine the perceptions of healthcare workers about medical errors in a tertiary hospital in Jordan.
Methodology/approach
The descriptive-analytical cross-sectional study included 246 healthcare workers in a tertiary hospital in Jordan. Systematic random sampling technique was used to select the participants. Data were collected using a questionnaire that was used in previous literature. The Statistical Package for the Social Sciences Software (SPSS), version 27, was used to analyze the data. Descriptive and inferential statistics were used to address research objectives.
Results
The majority of the participants were females and had a bachelor’s degree. Human error, lack of resources and failure of the communication system were the most frequently reported causes of errors (38.2%, 32.5%, and 30.0%, respectively). The findings show that disclosure of patient errors was perceived by 78% of the participants as a method to reduce the effect of medical errors on patient health. Raising awareness and training were perceived as the most impactful way in which hospitals could reduce medical errors. Reporting errors was stated by 52% of the respondents as a method to deal with medical errors. However, the commonest barriers to reporting errors were identified as culture (38.2%) and a long complicated process of errors reporting (28.9%). The emergency department was reported as the commonest place for medical errors occurrence.
Conclusion
The findings revealed the experience of a Jordanian hospital regarding medical errors. Healthcare organizations and policymakers can utilize the findings presented in this paper to reduce medical errors, therefore promoting quality healthcare and patient safety.
Introduction
Patient safety has become a topic of increasing concern worldwide.1,2 Patient safety is based on the “First, do no harm” principle, with a focus on preventing Medical Errors (MEs)before they lead to harm, injury, or damage to the patient. 3 Understanding the frequency, seriousness, and causes of MEs is essential for improving patient safety. 4 MEs are preventable events of omissions (a result of actions not taken) or commissions (a result of the wrong action taken) in planning or execution that lead or could lead to unintended results, whether these events harm the patient or not.5,6,7 No medical care unit remains immune to the occurrence of MEs, which have emerged as a serious public health problem.8,9 Therefore, it is deemed a paramount concern in the development of policies and improvement strategies for healthcare systems worldwide. 10
The World Health Organization’s (WHO) latest report identifies that approximately 10% of patients experience harm within the healthcare system, leading to over 3 million fatalities each year as a result of unsafe medical practices. 11 In low- to middle-income nations, the mortality rate due to unsafe care can reach as high as 4 in every 100 individuals. 12 More than 50% of harm, equivalent to 1 in every 20 patients, can be prevented. 13 In the United States, MEs were ranked as the third leading cause of death following heart diseases and cancer.14,15 Estimates indicate that MEs cost the U.S. healthcare system over 17 billion dollars annually, contributing to a significant economic burden through additional healthcare costs and lost productivity from missed workdays.4,14 The impact of MEs extends beyond mortality, affecting healthcare professionals who experience profound psychological effects such as anger, guilt, inadequacy, depression, and even suicide due to real or perceived errors. Furthermore, legal actions looming over medical professionals may compound these emotional challenges, leading to a loss of clinical confidence and burnout. 8 A study conducted in Poland reveals that burnout increases the odds of making an error more than five times. 16 Occupational disengagement among healthcare professionals may contribute to a decrease in work performance, elevating the prevalence of MEs. 17
The Middle East region reports higher rates of MEs, with a study in Jordan indicating that 28% of all hospital admissions were affected by MEs particularly medication errors. Workload, inadequate staffing, technical performance issues, negligence, poor ethics, poor management, psychosocial job demands, and written guidelines were identified as common causes of adverse events in Jordan. 18 Furthermore, it is noticeable that the overall patient safety culture was low in Jordan with a reported score of 42%. 19
The healthcare system in Jordan is marked by a growing demand for services, escalating costs, and a shortage of available resources. 20 MEs can arise from various factors, primarily including the neglect of safety guidelines and protocols, insufficient access to patient information, lack of necessary equipment, overwhelming schedules, and physician exhaustion. These errors can result in medical liability. Conversely, the apprehension of facing penalties encourages the adoption of Defensive Medicine (DM) practices. 21
DM is defined as the phenomenon where physicians stray from established medical practices due to concerns about potential liability claims and lawsuits. 22 DM is inherently unethical and raises the expenses associated with medical practice. Furthermore, its implementation does not safeguard against potential future lawsuits. 21 Behaviors associated with DM can pose risks to patient safety. For instance, the unwarranted utilization of MRI and CT scans exposes patients to radiation, which can be harmful to their health. 23 A recent Jordanian study found that the prevalence of adopting DM among physicians was 68%. 24 In this regard, it is essential to highlight that fostering a culture of openness within healthcare facilities could lead to an enhancement in the implementation of DM practices. 25
Openness seems to play a crucial role in shaping the organizational culture within the healthcare sector. 26 Openness is defined as the ability to express and reveal concerns freely, without the fear of repercussions. 27 It is considered essential for allowing all individuals engaged in healthcare delivery to express their concerns regarding issues related to quality and safety, irrespective of their position or seniority. 28 Amy Edmondson’s groundbreaking article indicated that a key factor in identifying errors in healthcare delivery was the staff’s readiness to engage in open discussions about these issues. 29 However, a recently published study that examined PSC in a Jordanian tertiary hospital using Hospital Survey on Patient Survey Culture (HSOPSC) revealed that the average positive responses for the culture of openness were 42.5%. 30 Another cross-sectional Jordanian study that evaluated PSC in a teaching hospital using the Safety Attitude Questionnaire (SAQ) uncovered that only 40% of the participants perceive that they were encouraged by their colleagues to report patient safety concerns they may have. 31 These findings pinpoint to the necessity to promoting speaking up about patient safety events in the Jordanian context. Therefore, reducing the prevalence of MEs and enhancing patient safety.
Previous research on MEs in Jordan was restricted and focused on a specific group of healthcare providers, such as nurses,7,32 and medical and nursing students.7,33 To the best of our knowledge, no previous studies explored MEs as perceived by various healthcare providers in a teaching hospital in Jordan. Consequently, this research was undertaken to address this gap in current body of knowledge. This study aims to examine the perspectives of the healthcare providers in a teaching hospital in Jordan regarding MEs. The findings of this research will assist healthcare providers and managers in identifying the most attributable causes of MEs and try to find suitable solutions for these causes in the future. The research questions of the present study were (1) What are the perceptions of Healthcare Workers (HCWs) regarding the causes of MEs in a tertiary hospital in Jordan? (2) What are the barriers to reporting MEs in the study hospital? (3) What are the factors associated with MEs occurrence in the involved hospital?
Methods
Study design
This is a cross-sectional study with an analytic component carried out in Jordanian University Hospital during the period from December 2023 and February 2024. The involved hospital offers 34 medical and surgical specialty and subspecialty services, providing care to over (500,000) patients in outpatient clinics every year and performing over (25,000) surgical operations. 35
Population and sampling
All categories of HCWs on duty for at least 1 year were invited to participate in the study. HCWs who were not available during the data collection period were excluded from the study. Sample size was calculated using MedCalc statistical program (MedCalc Statistical Software version 14.8.1. 36 A pilot study on 50 HCWs of different categories found that 12% of them ever made a ME. With confidence level 99%, study power of 95% and precision of 5%. The sample size is 246. The total number of HCWs in the study locality was about 1000 eligible for the study. A systematic random sample (every 4th) of HCW was selected from each department. The questionnaire was distributed to 250 HCWs with a response rate of 98.4%.
Instrument and data collection
A paper-format structured English and Arabic questionnaire was used. The questionnaire was used in previous study. 6 The data collection instrument utilized was a self-administered questionnaire that included both open-ended and closed-ended questions. Every question was written in Arabic and English to ensure the respondents fully understand the question and thus reduce bias (see appendices). The questionnaire contains 3 sections, section one contains demographic information about the HCWs including age (<30 years, 30–39, and 40 years 7 more), gender, qualifications (Doctorate/fellowship, MSc, Bachelor, and diploma), years of experience and self-reported job satisfaction (are you satisfied with your current job?). Section two evaluated the knowledge of HCWs in terms of MEs, and also sought if they had seen or involved in a ME and what the outcomes were. Section three investigated the perceptions of HCWs about attempts to decrease the incidence while trying to prevent MEs. The permission to use the questionnaire was obtained from the developer. 6
Research assistants distributed the questionnaires to the HCWs. The completed questionnaires were collected from a point of contact in each department, who handed the questionnaires to the data collectors in the current study. The participants received a reminder from the data collectors.
Data analysis
Data were analyzed using SPSS version 27 (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp). Data were checked for completeness and accuracy. The outcomes are ever-committed ME, as well as knowledge and experience with MEs. Descriptive statistics including frequencies and percentages were used to present participants characteristics, perceptions of MEs, and experience and circumstances of MEs. Chi-squared test was used to test significance differences between groups. Monte-Carlo exact test was used when the expected frequency is less than 5. p ≤ 0.05 was considered statistically significant.
Ethical considerations
The Institutional Review Board (IRB) at the involved hospital approved the study protocol (Ref. No. 10/2023/22921). The study ensured that the anonymity and confidentiality of the respondents were maintained at all times. It was voluntary to participate in the study. After a thorough description of the study’s objectives, all participants were asked to provide their informed consent at the beginning of the questionnaire.
Results
Demographic and occupational characteristics of studied HCWs.
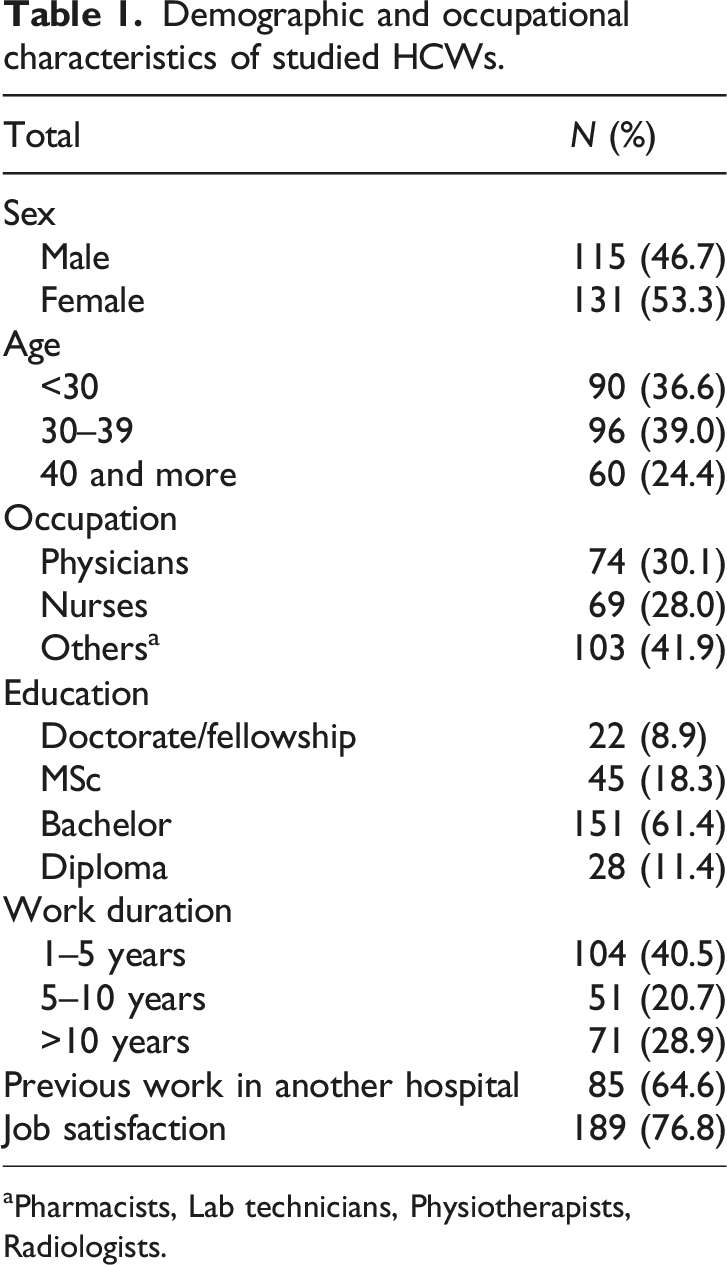
aPharmacists, Lab technicians, Physiotherapists, Radiologists.
Perceptions of studied HCWs about MEs.

• For example, providing the necessary care to treat the error as much as possible, staff training on effective communication approaches.
a For example, reducing hospital admissions.
Experience and circumstances of MEs.
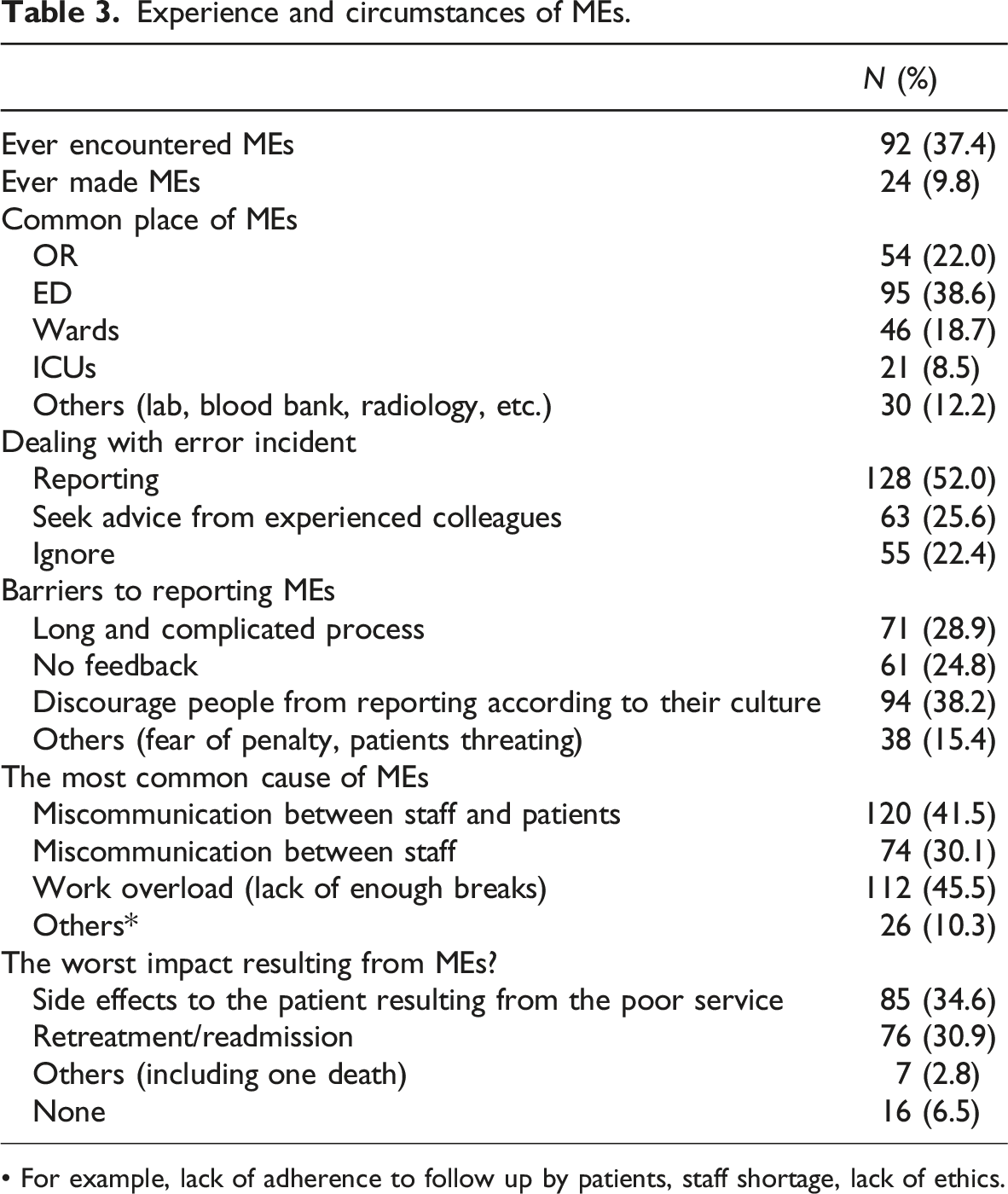
• For example, lack of adherence to follow up by patients, staff shortage, lack of ethics.
Factors associated with committing MEs by studied HCWs.
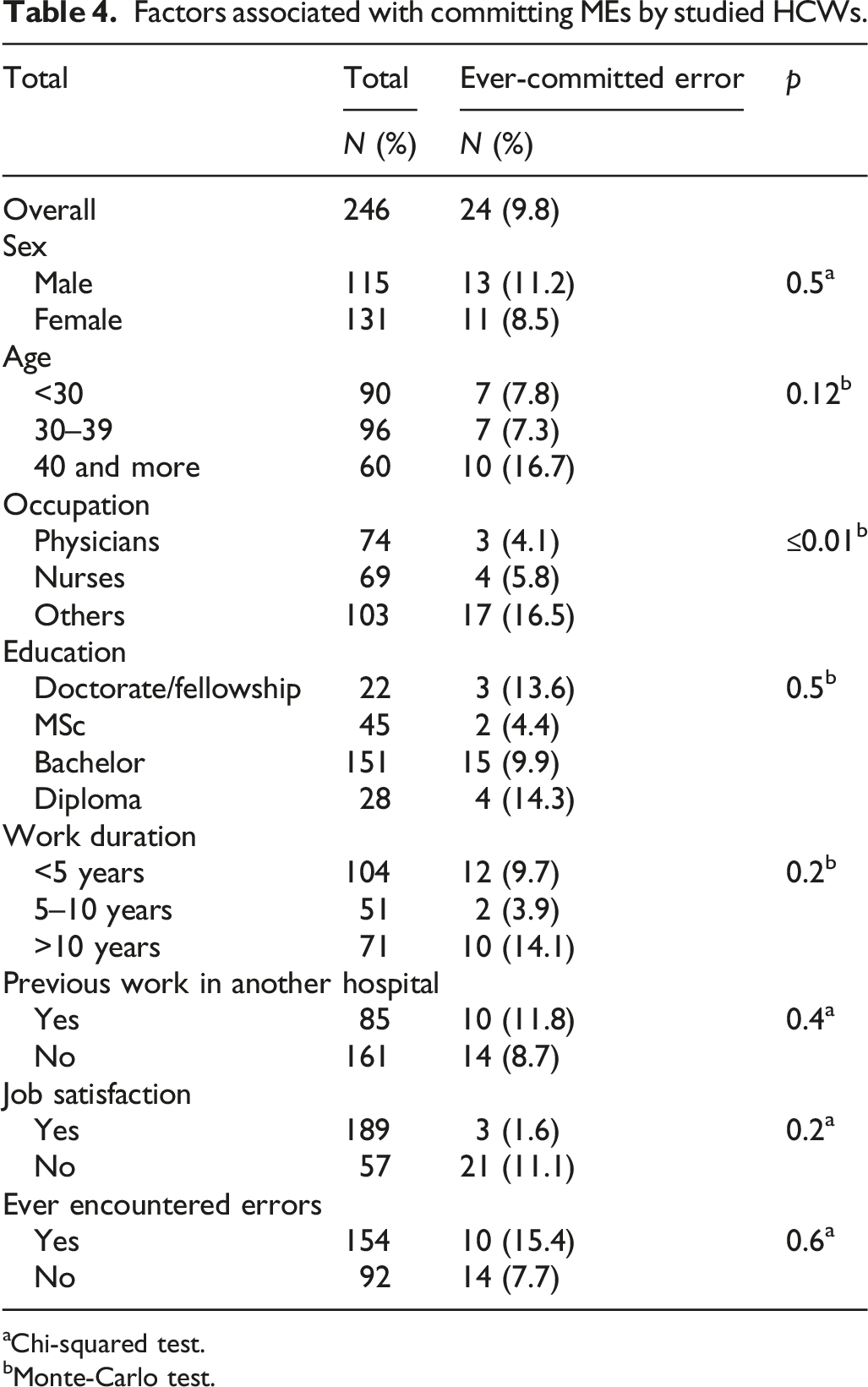
aChi-squared test.
bMonte-Carlo test.
Discussion
Medical errors pose a significant threat to public health. According to the Global Patient Safety Action Plan 2021–2030, patient safety incidents continue to rise and remain a significant contributor to mortality and disability worldwide. 37 To our knowledge, this is the first study to investigate the perceptions of HCWs about MEs in a teaching hospital in Jordan. The questionnaire was the main data collection used in the current study. The sample (n = 246) in our study included various HCWs working at the same university hospital in Jordan. The high response rate (98.4%) of the participants suggests that the results are representative of the study sample. The findings of this study revealed that the majority of the participants perceive that human error is the main cause of MEs in their healthcare facility. Previous research found that human factors such as fatigue due to hard work and lack of support were the primary contributors to medication errors. 38 Human factors and ergonomics (HFE) often lead to errors due to the mismatch between the system, technique, and human body characteristics. HFE is a scientific field that focuses on understanding the interactions between human behavior, system design, and safety. 39 Human factors emphasize the need to not only enhance individual system components like technology or tasks but also to thoroughly examine and enhance the entire system, including both its components and their interactions. 40
The findings of this study uncovered that disclosure of errors to patients is the most frequently used method to decrease the effect of MEs on patient health The disclosure of MEs to patients and their families is a crucial aspect of patient-centered healthcare. 41 Open disclosure involves engaging in transparent conversations with patients regarding any adverse events that occurred during their medical treatment. 42 An environment that promotes transparency is linked to lower mortality rates in hospitals. 26 It can alleviate patients’ discomfort without increasing legal claims, and it promotes measures to prevent future occurrences. 43 A study conducted among physicians in the United States and Canada found that attitudes towards disclosure were consistent between the two countries, with 98% of respondents believing that serious adverse events should be disclosed and 78% supporting the disclosure of minor adverse events to patients. 44 However, another study conducted in the United States among practicing physicians and the general public revealed that just one-third of individuals in each group who had encountered a patient safety incident indicated that the healthcare provider responsible for the incident disclosure. 45 Most physicians believe it is important to inform patients about MEs; however, they often experience discomfort in doing so because of concerns regarding potential legal repercussions and the implications of admitting to a mistake. 46 The “Medical and Health Liability Law” (MHLL) in Jordan, issued by the Jordanian government, stipulates that physicians are obligated to provide services that adhere to the ethical standards, precision, and fidelity of the medical profession. Additionally, their practices must align with recognized scientific standards. 47 Hence, healthcare institutions and policymakers need to work together in promoting open disclosure, protecting patients, and educating HCWs. This will ultimately result in a healthcare system that is more secure, transparent, and focused on the needs of the patients. 48
The majority of participants in the current study perceived that the role of the hospital in reducing MEs resides in raising awareness and training of staff. 49 A study found that using simulation training in endoscopy to identify hidden errors in the workplace is highly beneficial in minimizing mistakes and avoiding harm. 50 Training HCWs on Team Strategies and Tools to Enhance Performance and Patient Safety (TEAMSTEPPS) can also be used to reduce MEs and enhance patient safety. 51 In addition, training physicians on electronic health records can help to improve quality healthcare as well as maintain patient safety. 52 Furthermore, ongoing Continuing Medical Education (CME) helps HCWs remain up-to-date with the most recent evidence-based practices, thereby minimizing the likelihood of MEs stemming from outdated information.53,54
We found that ever-committed errors were the least among physicians and nurses. The findings suggest that engaging HCWs in patient safety training may enhance the patient safety environment among HCWs, although the positive impact may diminish after 1 year. Therefore, a periodic refresher training in patient safety may become necessary. 55
The findings of this study demonstrated that the most common place where MEs occurs is the Emergency Department. This is similar to previous research. 6 The high volume of patients in emergency departments, coupled with the demanding nature of the services offered, can lead to human errors due to the heavy workload. 56 Research illustrated that enhancing handover procedures between emergency care providers and healthcare professionals in the emergency department has the potential to minimize mistakes and enhance patient safety. 57
The majority of the participants perceived that increased workload as the reason for MEs. One study found that heavy workload was among the reasons that may lead to medical errors. 7 Previous research found that increased workload is linked to a higher frequency of medical errors, which can be mitigated by a positive safety culture. 58 Previous study revealed that the adoption of remote video monitoring (RVM) technology has proven to be a successful healthcare innovation, resulting in substantial enhancements in patient safety and the management of workload, particularly for nursing staff. 59
In the current study, more than 50% of the participants stated that dealing with the incident is by reporting its occurrence. However, the majority reported that the barrier to reporting is the culture that discourages HCWs from reporting incidents. This can be attributed to fear of retribution. 60 One study found that the main barrier to reporting of MEs by nurses is related to the fear of repercussions and management response. 2 A qualitative study conducted in Jordan underscores the importance of fostering a culture that encourages reporting of MEs. 61 To effectively foster a non-punitive environment for reporting MEs, it is crucial that reports remain anonymous and concentrate on systemic issues rather than pinpointing the actions of individual involved in the incident.62,63 The Swiss cheese model proposed by Reason illustrates that while human error is unavoidable, incidents often arise from a combination of several minor errors within a malfunctioning system. 64 Another study revealed that to enhance the culture of error reporting in healthcare, it is essential to focus on fostering and sustaining an environment characterized by open communication, management that prioritizes safety, and a commitment to learning and collaboration among the various units. 34 A study that was conducted in Saudi Arabia indicated that enhancing the culture of reporting of MEs can be achieved by promoting reporting through the adoption of just cultural principles, providing incentives for staff, establishing training programs focused on patient safety, and developing support initiatives for second victims. 65 In this regard, it is important to highlight that all hospitals in Jordan function within national reporting frameworks. These frameworks require the documentation of MEs and incidents to establish a uniform approach to patient safety across different healthcare sectors. The national systems advocate for anonymous reporting, which encourages healthcare professionals to disclose errors without the fear of punishment, thereby promoting a culture of transparency and ongoing enhancement in patient safety. 66
Strengths and limitations
The study’s strength lies in the minimal possibility of non-response bias due to the high response rate achieved. The topic’s relevance to the real-life experiences of HCWs in hospital may contribute to the good response rate. Moreover, the response rate on patient safety is higher in developing countries, indicating that this topic is a significant concern in such settings where adverse events are more prevalent. 67 However, the study is subject to several limitations that should be considered when interpreting the findings Firstly, the survey was carried out in a single tertiary hospital, potentially restricting the generalizability of the results to other healthcare settings, including private hospitals. Therefore, future studies could improve by conducting surveys in multiple facilities with larger sample sizes to improve the generalizability of the findings. Secondly, due to the cross-sectional nature of the study, establishing a cause-and-effect relationship between variables was not possible. Thirdly, the study sample aligns with the average age and sex distribution of HCWs in Jordan. However, there is a notable underrepresentation of nurses among the professional groups. Due to their demanding responsibilities during shifts, nurses may lack the time necessary to complete surveys and participate in research activities. 68 Fourthly, although the study tool has been previously utilized and evaluated for content and face validity in earlier research, additional assessment of its construct validity and reliability is required in future studies. 6 Fifthly, the study relied on self-reported data, which could introduce reporting bias. To address this issue, additional research should consider incident reports to examine MEs and their causes. Lastly, considering the sensitive nature of the topic, there is a chance that participants provided socially desirable responses (social desirability bias). Anonymity and confidentiality would help to mitigate this issue. Furthermore, to address this in future research, careful attention to the survey design and use of techniques to minimize social desirability bias, such as indirect questioning, should be considered.
Conclusion
In conclusion, this cross-sectional study, which included 246 HCWs practicing in a Jordanian tertiary hospital, was among the first studies to investigate the perceptions of HCWs regarding MEs. Most of the participants have not committed or encountered a ME. Our respondents identified several causes of MEs. The majority of the participants perceive that human error is the main cause of MEs in their healthcare facility. The study demonstrated a statistically significant association between MEs occurrence and professional group. The findings of this study underscore the importance of creating a non-punitive environment to enhance reporting of MEs in healthcare institutions. It seems that staff training on teamwork, using electronic health records, and encouraging open discussions on patient safety in medical curricula would help to reduce the prevalence of MEs, therefore promoting quality healthcare and patient safety in healthcare organizations.
Supplemental Material
Supplemental Material - Perceptions of healthcare workers about medical errors: A cross-sectional study in a tertiary hospital in Jordan
Supplemental Material for Perceptions of healthcare workers about medical errors: A cross-sectional study in a tertiary hospital in Jordan by Rania Ali Albsoul, Muhammad Ahmed Alshyyab, Luay Abdallah, Ghaleb Naser Eskeiker, Yazan Faisal Al-Bukhari, Rahmeh Al-Asmar, Mohammad Aljahalin, Gerard FitzGerald and Abdel-Hady El-Gilany in International Journal of Risk & Safety in Medicine
Supplemental Material
Supplemental Material - Perceptions of healthcare workers about medical errors: A cross-sectional study in a tertiary hospital in Jordan
Supplemental Material for Perceptions of healthcare workers about medical errors: A cross-sectional study in a tertiary hospital in Jordan by Rania Ali Albsoul, Muhammad Ahmed Alshyyab, Luay Abdallah, Ghaleb Naser Eskeiker, Yazan Faisal Al-Bukhari, Rahmeh Al-Asmar, Mohammad Aljahalin, Gerard FitzGerald and Abdel-Hady El-Gilany in International Journal of Risk & Safety in Medicine
Footnotes
Acknowledgements
We want to thank all participants for taking the time to complete the study survey.
Author contributions
RA: conceptualization, data curation, funding acquisition, methodology, project administration, supervision, writing-original draft, writing-review and editing; MA: conceptualization, methodology, writing-review and editing; LA, GE, EA, RA, MA: conceptualization, investigation, methodology, writing-original draft; GF: conceptualization, methodology, writing-review and editing; AE: data curation, formal analysis, writing-original draft, writing-review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Deanship of Scientific Research at the University of Jordan supported the study (1507/2023/19).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.