
Abstract
Background
Drug-induced Steven-Johnson Syndrome (SJS) is a life-threatening hypersensitivity reaction and systemic steroid immunosuppressant therapy is not universally recommended. With the changing landscape of new drugs, it is important to determine emerging trends in this severe drug induced adverse event.
Objective
The objectives were to examine drug induced SJS case reports published from January 1 2003 to December 31 2023 for emerging trends of drugs implicated and systemic immunosuppressant therapy administered.
Methods
Literature search was done using PubMed (MEDLINE) database with keywords and Boolean terms, “Stevens Johnson Syndrome” AND “Case Report,” filtered for the time period of interest, articles available free and in English. Included case reports were only studies in which a single drug was implicated.
Results
Forty-nine case reports met inclusion criteria and critical analysis of quality rated studies from moderate to strong; however, causality assessment instrument was only reported for 10 (20%) case reports. There was equal distribution by sex; patient ages ranged from 2 to 95 years and 34 (69.4%) case reports originated from countries of the Asian continent. Most common drug implicated was carbamazepine, 5 (10.2%); pembrolizumab was implicated in 4 of 9 case reports involving monoclonal antibody drugs. Thirty-seven patients (75.5%) received systemic steroid immunosuppressant therapy. Two patients (4.1%) died during the clinical course.
Conclusion
The published case reports are predominately from countries known to be at higher risk of drug induced SJS and the emerging greater number of case reports implicating pembrolizumab may be an important safety concern, needing further investigation. Systemic steroid use was the preferred immunosuppressant therapy.
Introduction
Steven-Johnson Syndrome (SJS) is a life-threatening type IV hypersensitivity reaction of the skin and mucous membranes and is reported to be a rare drug induced adverse event which requires an immediate withdrawal of the associated drug.1,2 Historically, systemic steroid administration is a treatment option for immunosuppression; however, there is limited evidence of clinical benefits.3–6
In a systematic review of published case reports between 1980 and 2020, phenytoin, carbamazepine, lamotrigine and allopurinol were implicated in 3 to 5% of the drug induced SJS cases identified. 7 These small molecule drugs are also in the 2004-2021 list of top drugs associated with SJS individual case safety reports of the Food and Drug Administration Adverse Event Reporting System (FAERS). 8 Also included on the list of the FAERS are large molecule drugs, such as monoclonal antibodies. It is important to explore other sources of case reports for changes in common drugs implicated in SJS, especially with the expanding market of monoclonal antibodies. 9 Therefore, the primary purpose of this rapid review study was to describe the drugs implicated in published drug induced SJS case reports from January 1 2003 to December 31 2023. Furthermore, with the limited evidence supporting the use of systemic steroid immunosuppressant therapy, the study will explore trends in the use of systemic immunosuppressant therapy as a secondary purpose. The objectives of the study were to examine drug induced SJS case reports for emerging trends of drugs implicated and systemic immunosuppressant therapy administered.
Methodology
A rapid review search strategy was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for rapid reviews. 10 Literature search was done on May 28, 2024 using PubMed/MEDLINE database; the search was restricted to this database to ensure only case reports from peered review journals were included. Included keywords with Boolean terms were “Stevens Johnson Syndrome” AND “Case report.” The search was filtered to only include journal articles, written in English, free full text available and published between January 1, 2003 and December 31, 2023. Language and free access availability restrictions were determined by the absence of funding support for this study. No ethical approval was required for this study because it was based on secondary analysis of data obtained from peer reviewed published literature. Google Sheets on Google Documents Share Platform was used to organize and manage the yielded citations for the title/abstract screening, full paper inclusion and the data extraction phases. At least two members of the student team (GM, RC, KG, SD, and DG) independently screened title and abstract of the identified records for inclusion/exclusion; where there was disagreement, consensus was resolved by MGW. Inclusion criteria for this study were articles that involved a single case report of a patient confirmed with only drug induced SJS (with or without diagnostic confirmatory tests) and implicating a single drug. Case reports of toxic epidermal necrolysis, which represents a greater severity of SJS and erythema multiforme which may be considered as a part of the spectrum of severity, although distinct differences in the associated lesions exist 1 were excluded. Review articles and editorials were also excluded. Initial screening of record required inclusion of the term SJS in either the title or abstract; articles without abstract were passed directly to full paper review phase. Articles shortlisted for full paper review were assessed to confirm inclusion/exclusion criteria were satisfied. Articles meeting inclusion criteria were then passed to the data extraction phase.
Data extraction and quality assessment
Modified Quality Assessment Instrument for drug-induced case reports for adverse events (AEs).

* Items required of case reports of AE; but reported in less than 90% of case reports of pilot test 12 ; scoring instructions modified from a previous publication 14 ; for each item presented in case report, 0 points for ‘no’ if it was not reported in the case report, 1 point for ‘unclear’ if inadequately reported and 2 points for ‘yes’ when adequately reported. For each case report the average score (out of 12) is calculated. Based on a maximum quality rating score of 2, studies assigned a quality rating of weak = 0-0.50, moderate = 0.51-1.50 or strong = 1.51-2.00.
Data analysis
Descriptive statistical analysis using IBM SPSS Statistics 25 involved the use of means, medians, minimum to maximum values and interquartile range for continuous variables and proportions for categorical variables. The quality rating of each included article was categorically defined as previously described, 14 which required summing the scores for each item and dividing by the total number of items in instrument (n = 12). Based on the maximum quality rating score of 2, studies were then categorically assigned a quality rating of weak (score of 0 to 0.50), moderate (score of 0.51 to 1.50) or strong (score of 1.51 to 2.00).
Results
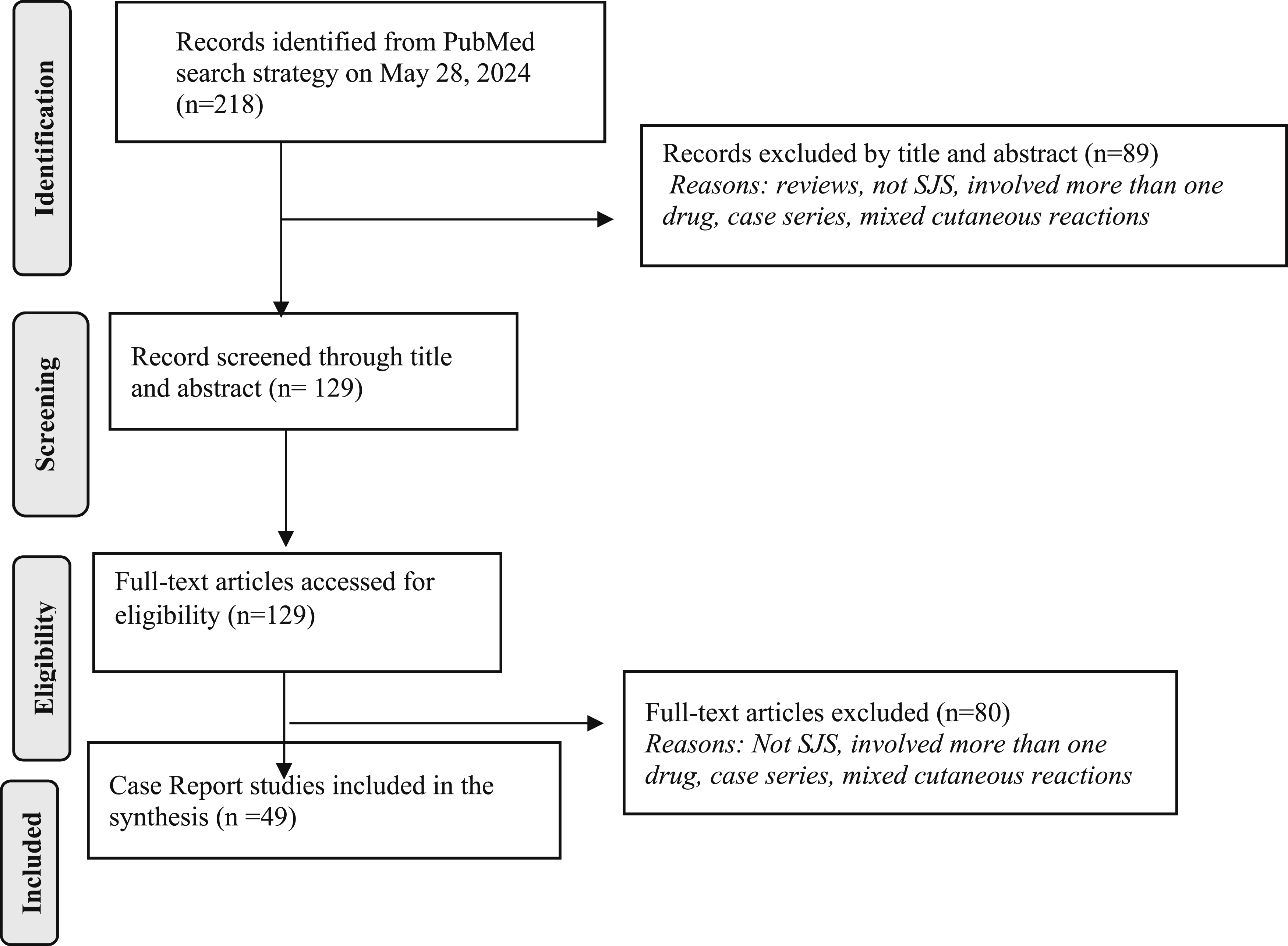
The process of the strategic search and review is depicted in Figure 1 (PRISMA flowchart adapted from Page et al.).
15
A total of 530 citations were retrieved when restricted to the years of interest once filtered for available free and only English, 218 citations remained for examination of title and abstract. The title/abstract screening yielded 129 citations for full paper assessment. Assessment of full articles resulted in the exclusion of 80 citations; reasons for exclusion included more than one drug implicated to be related to SJS; the article reported more than one patient; patient was diagnosed with mixed cutaneous adverse events. Forty-nine case reports met the inclusion criteria for this review. PRISMA flow chart; adopted from Page et al.
15
Quality assessment
Quality Assessment of included case reports using the 12 items listed in the Modified Quality Assessment Instrument (see Table 1).
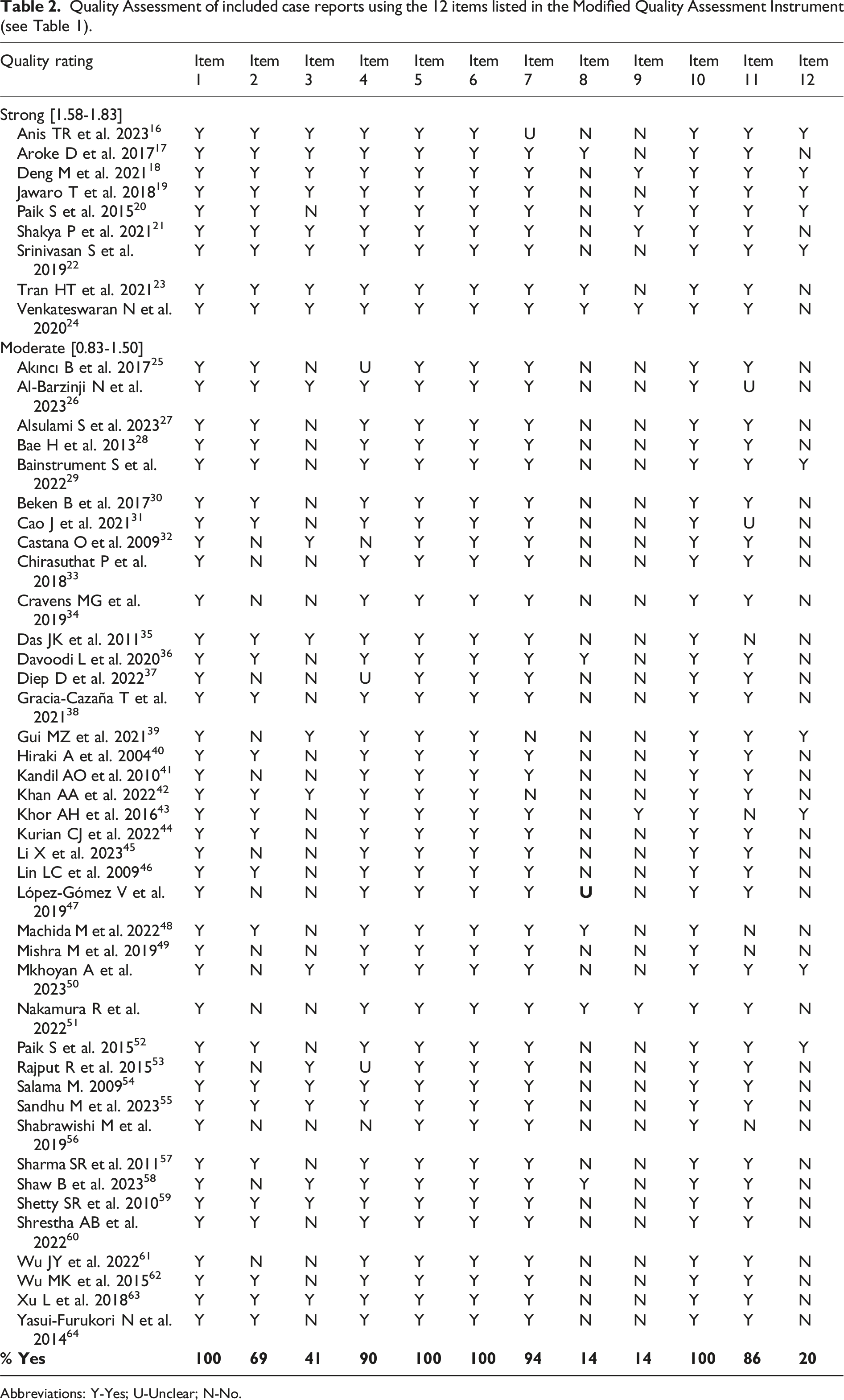
Abbreviations: Y-Yes; U-Unclear; N-No.
Large Molecule Drugs (9 case reports).

Abbreviations: USA-United States of America. All case reports involved monoclonal antibodies.
Small molecule drugs (40 case reports).
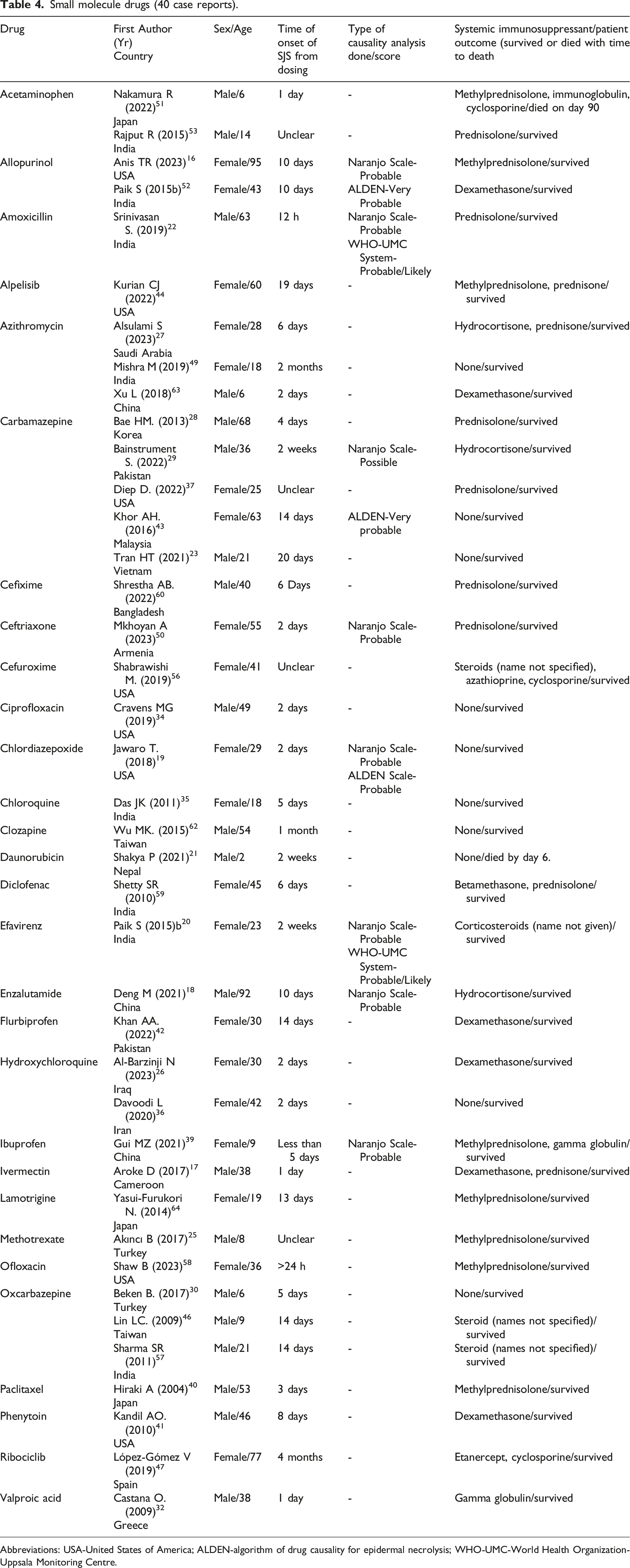
Abbreviations: USA-United States of America; ALDEN-algorithm of drug causality for epidermal necrolysis; WHO-UMC-World Health Organization-Uppsala Monitoring Centre.
Reported time of onset of SJS related symptoms from the first dose ranged from 12 h to 4 months, with 19 (38.8%) case reports indicating onset of symptoms of less than 7 days.17,19,26–28,30,32–36,39,40,50,51,58–60,63
Regarding use of a causality assessment instrument, eight (16.3%) case reports used Naranjo Scale with a rating of probable for seven reports16,18–20,22,39,50 and one possible 29 ; 2 (4.1%) case reports used the WHO-UMC System, and both reports were rated probable/likely.20,22 Three reports (6.1%) used the ALDEN instrument with two rated as very probably43,52 and one probable. 19 Seven (14%) case reports discussed possible concurrent disease as a factor in the risk of drug-induced SJS, which included positive COVID-19 status of the patients,36,58 pulmonary impairment, 51 the presence of the human immune-deficiency virus, 17 presence of giant cell arteritis, 24 nuclear receptor transcription factor 4a suppression, 48 and risk related to the Human Leukocyte Antigen. 23 Six case reports (12.2%) implicating carbamazepine, enzalutamide, daunorubicin, tocilizumab, acetaminophen and efavirenz discussed other coadministered drugs as possible factors in the drug-induced SJS. For carbamazepine, the case report explicitly stated no other drug was implicated. 43 For enzalutamide coadministered with goserelin 18 and daunorubicin coadministered with methotrexate 21 ; the second drugs were excluded based on temporal association between onset of SJS and time of drug challenge; while for tocilizumab coadministered with prednisone, 24 the second drug was excluded based on the disappearance of symptoms with tocilizumab dechallenge. For acetaminophen, the coadministered clarithromycin was excluded based on negative results using a lymphocyte stimulation test protocol 51 and for efavirenz, the coadministered tenofovir was excluded based on the absence of published literature associating tenofovir with SJS. 20
Systemic immunosuppressant therapy with steroids was reported for 37 (75.5%) case reports. Of these case reports, 30 (61.2%) indicated patients received only steroids to manage SJS; 5 patients received steroid plus globulin,24,31,39,45,61 one patient received steroid plus globulin and cyclosporine 51 and one patient received steroid plus azathioprine and cyclosporine. 56 One patient received globulin only 32 and one patient received etanercept and cyclosporine. 47 There were 10 patients who were not given any systemic immunosuppressant drug.19,21,23,30,34–36,43,49,62 Of the 49 included case reports, 2 (4.1%) patients died; in one case, the patient did not receive systemic immunosuppressant and died of sepsis 6 days post-diagnosis 21 ; the second case received systemic immunosuppressant (methylprednisolone, immunoglobulin and cyclosporine)and died from pulmonary impairment, 90 days post-diagnosis. 51
Discussion
In this study, forty-nine case reports matched the inclusion criteria and critical analysis using a modification of the ISoP/ISPE guidelines for adverse events related to drugs, rated the quality of the case reports from moderate to strong. All case reports were compliant with providing name of the implicated drug, patient’s age and sex, as well as the description of the adverse event. However, for most of the case reports, there was no use of a causality assessment instrument; neither was there discussion of the possible involvement of concurrent diseases and coadministered drugs in the adverse event.
An interesting finding of our study was that most of the case reports originated from countries of the Asian continent. This representation is possibly related to what is known of higher prevalence of cutaneous severe adverse drug reactions in these populations and may support the need for interventions to reduce patients’ risk, such as implementation of genetic screening.66,67
The most common drugs identified were carbamazepine, pembrolizumab, azithromycin, and oxcarbazepine; these results are consistent with previous case report publications and case reports of the FAERS database.7,8 A higher frequency pembrolizumab induced SJS in comparison to other monoclonal antibodies was observed. Although this may be a reflection of drug entry into the market and its increasing dominance,9,68 previous publications have also identified this emerging trend and have suggested safety concerns.69,70 Therefore, consideration should be given to the further examination of the relationship between SJS and this humanized monoclonal antibody.
Systemic use of steroids was the preferred immunosuppressant administered for most patients; although such treatment intervention remains inadequately supported by clinical evidence, including meta-analytic studies using the Cochrane Skin Specialised Registry.5,71,72 Interestingly, there is evidence of superiority of etanercept to systemic steroid therapy in promoting skin healing and reducing mortality 5 ; this drugs was only administered in one study. 47
Case reports are considered low level on the hierarchy of evidence-based medicine and therefore have limited external validity. They however provide evidence from real-world clinical practice and although most of the included drug induced SJS case reports did not utilize causality assessment, there was much information to advance discussions on minimizing patient risk. Our results are also limited by a level of publication bias, as financial constraints excluded access to articles unavailable free and publications requiring translation to English.
In conclusion, most of the case reports were of moderate to strong quality; weaknesses were related to the absence of information about patient comorbidities and coadministered drugs. The published case reports of SJS were predominately from countries known to be at higher risk of this adverse event and the common drugs identified are consistent with current trends. The emerging greater number of case reports implicating pembrolizumab may be an important safety concern. With the anticipated increase in demand for this drug, studies are required to further examine the relationship with SJS. Finally, therapy with systemic steroids was the preferred immunosuppressant, although clinical benefit of such therapy remains unsupported. With the absence of standardize treatment protocols, enriching case reports with details of outcomes of patients may provide useful clinical evidence.
Supplemental Material
Supplemental Material - Rapid review of drug induced Stevens Johnson Syndrome case reports from 2003 to 2023: Trends among monoclonal antibodies and systemic immunosuppressant therapy
Supplemental Material for Rapid review of drug induced Stevens Johnson Syndrome case reports from 2003 to 2023: Trends among monoclonal antibodies and systemic immunosuppressant therapy by Maxine Gossell-Williams, Gabrielle McLaren, Rojay Clarke, Shenae Douglas, Devonne Gayle and Kerrian Guthrie in International Journal of Risk & Safety in Medicine.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.