
Abstract
Background
COVID-19-associated thrombotic complications became a major problem of pandemic. Clinical practice guidelines are meant to present approaches to preventing and managing them. In our previous studies, we found that direct oral anticoagulants (DOACs) consumption and expenditure in Russia through COVID-19 pandemic was extensive, exceeding CPGs’ recommendations in 2020 and 2021, particularly in outpatient settings.
Objective
To analyze Russian clinical practice guidelines on the use of DOACs for COVID-19.
Methods
We conducted thematic content analysis of Russian guidelines using qualitative research methods. Purposive sampling allowed including all existing guidelines on the use of DOACs in COVID-19 pandemic. The sample size was limited to the results of our previous searches of the Russian guideline and bibliographic databases. We focused on indications, contraindications, dosing regimens, monitoring, and drug interactions and compared with international recommendations.
Results
Only one guideline advised against outpatient DOAC use for COVID-19, aligning with international standards. The guidelines lacked clarity on indications, dosing, and treatment duration. Only two of six guidelines included safety monitoring recommendations, while four provided precautions.
Conclusion
We conclude that the found textual problems could potentially cause the established excessive consumption of direct oral anticoagulants in outpatients with COVID-19 on the rise the pandemic.
Keywords
Introduction
Thrombotic complications associated with COVID-19 remain a serious problem requiring adequate and timely pharmacotherapy. According to various data, the frequency of such a phenomenon is 2.6%–35.3%. 1
Cochrane systematic review 2 showed that higher doses of anticoagulants in hospitalized COVID-19 patients did not reduce mortality but increased bleeding risk.
Another Cochrane review by Santos B.C. et al. in 2023 3 showed that outpatient anticoagulation, in both individuals who did not require hospitalization and those discharged from hospital, probably reduced the incidence of venous thromboembolism (VTE) and pulmonary embolism (PE) compared with placebo or no treatment in patients with coronavirus disease. To avoid one VTE, 50 patients would need to be treated. At the same time, it was shown that these drugs appeared to have little or no effect on the number of deaths, hospitalizations, and adverse events. Prophylactic use of anticoagulants may have little or no effect on the incidence of VTE compared with antiplatelet agents.
A meta-analysis by Geng Y. et al. 4 revealed that lower doses of DOACs reduced thrombotic complications without increasing bleeding risk, whereas standard doses failed to improve outcomes while elevating the risk of complications.
These syntheses of research evidence highlight the potential harms without benefits of direct oral anticoagulant use in outpatient settings.
In our previous studies we found in the excessive use of DOACs in the first years of the COVID-19 pandemic, especially in the treatment of outpatients, the abuse of direct oral anticoagulants.5,6 We demonstrated that DOAC consumption in Russia during the 3 years of COVID-19 pandemic was extensive, exceeding CPGs’ overall dosing recommendations in 2020 and 2021.
The objective of this qualitative study was to assess the consistency of Russian clinical practice guidelines for the use of DOACs for the prevention of COVID-19 associated thrombosis by analyzing the concrete textual recommendations from six CPGs in order to understand whether CPGs were the cause of excessive consumption of DOACs.
Methods
This study employed a qualitative descriptive approach to analyze Russian clinical practice guidelines (CPGs) on the use of direct oral anticoagulants (DOACs) in COVID-19 patients. The primary objective was to assess the consistency of textual information across identified CPGs regarding indications, dosing regimens, and laboratory monitoring, followed by a comparative analysis with international recommendations.
The analyzed six CPGs G1 –; 7 G2 –; 8 G3 –; 9 G4 –; 10 G5 –; 11 and G6 –, 12 which were identified in our study. 5 The identified CPGs are presented under code names.
These guidelines were selected based on their relevance to DOAC administration in COVID-19 patients. To maintain confidentiality and minimize bias, the CPGs were anonymized and referenced using code names.
A systematic textual analysis was conducted focusing on: 1. Indications for DOAC use o Recommendations for outpatient and inpatient settings o Patient selection criteria (e.g., thrombosis risk factors) 2. Dosing regimens o Prophylactic and therapeutic doses o Dose adjustments for renal/hepatic impairment and drug interactions 3. Laboratory monitoring o Coagulation tests and anti-Xa activity levels o Frequency and methods of safety monitoring 4. Contraindications and precautions o Absolute and relative restrictions o Special patient groups (elderly, polypharmacy cases)
The extracted data were compared. - Across Russian CPGs—to identify consistencies/inconsistencies - With international guidelines (ISTH
13
)—to assess alignment with global standards
To enhance result validity, we employed. - Clear documentation—source tracking (pages, exact wording) for transparency - External benchmarking (e.g., against ISTH) to contextualize findings.
As the study analyzed publicly available documents, ethics committee approval was not required. However, to minimize bias: - CPGs were anonymized - Quotations were used verbatim with page references - Conclusions were based on objective text comparisons without subjective interpretations
This approach enabled identification of key discrepancies in Russian CPGs and their potential impact on clinical practice.
Results
Indications for the use of DOACs
G1 was the only CPG that had a clear recommendation to not prescribe anticoagulant therapy to non-hospitalized patients with COVID-19: “The use of anticoagulants for the treatment of COVID-19 at home is not recommended. There is no evidence from randomized controlled trials of benefit from routine anticoagulation in patients with COVID-19 who have not been hospitalized” (page 57).
G4 was the only CPG that did not contain any information on indications for DOAC use.
All remaining five CPGs unanimously provided more or less extensive lists of conditions and situations predisposing to deep vein thrombosis (DVT) and pulmonary embolism (PE) and recommended prevention of DVT of lower extremities or pulmonary embolism (PE) with either DOACs or low molecular weight heparins.
G2 was the most detailed and clear in specifying when and what antithrombotic therapy to use in which cases of coronavirus infection: “Prevention of deep vein thrombosis (DVT) of the lower extremities/pulmonary embolism (PE) using prophylactic doses of low molecular weight heparin should be considered for patients with a moderate form of COVID-19, who are being treated at home under quarantine conditions and have a high risk of venous thromboembolic complications, low risk of bleeding, and are not receiving anticoagulant treatment for other indications. This applies primarily to patients with severely limited mobility, a history of DVT/PE, active malignant neoplasm (MNT), major surgery or trauma in the previous month, antiphospholipid syndrome, carriers of a number of thrombophilias (deficiencies of antithrombin, proteins C or S, mutations in the factor V Leiden, prothrombin gene mutation G-20210A), as well as with a combination of additional risk factors DVT/PE (age over 70 years, heart/respiratory failure, obesity, systemic connective tissue diseases, hormone replacement therapy/oral contraceptives). In the absence of low molecular weight heparin, the use of direct oral anticoagulants (DOACs) may be considered” (page 256).
The five CPGs included recommendations for DOAC use in outpatients with COVID-19 and coexisting chronic conditions, such as atrial fibrillation or flutter.
For example, G1 recommended antithrombotic therapy in outpatient settings for certain patient groups only: “Extended prophylaxis in patients with COVID-19 after discharge is recommended if there is a continued increased risk of venous thromboembolic complications and a low risk of bleeding in cases where therapeutic doses of an anticoagulant are not required for other indications” (page 58).
There was also explicit statement on continuation of DOAC use in patients already taking them when encountering COVID-19 infections: “Prevention of DVT/PE in patients taking oral anticoagulants for other indications. Patients receiving oral anticoagulants for other indications, with non-severe manifestations of COVID-19, may continue taking them” (page 60).
Thus, all analyzed CPGs except G4 recommended DOAC use in outpatient care of COVID-19 patients without strict restrictions, though primarily as a second choice after low molecular weight heparins.
Guideline ISTH 13 recommend DOAC therapy only for patients discharged from hospital: «In select patients who have been hospitalized for COVID‐19, post‐discharge treatment with prophylactic dose rivaroxaban for approximately 30 days may be considered to reduce risk of VTE».
«3: No Benefit B‐R 2. In non‐hospitalized patients with symptomatic COVID‐19, initiation of direct oral anticoagulant (DOAC) therapy is not effective to reduce risk of hospitalization, arterial or venous thrombosis, or mortality», 13 which corresponds to the Russian clinical guidelines G1.
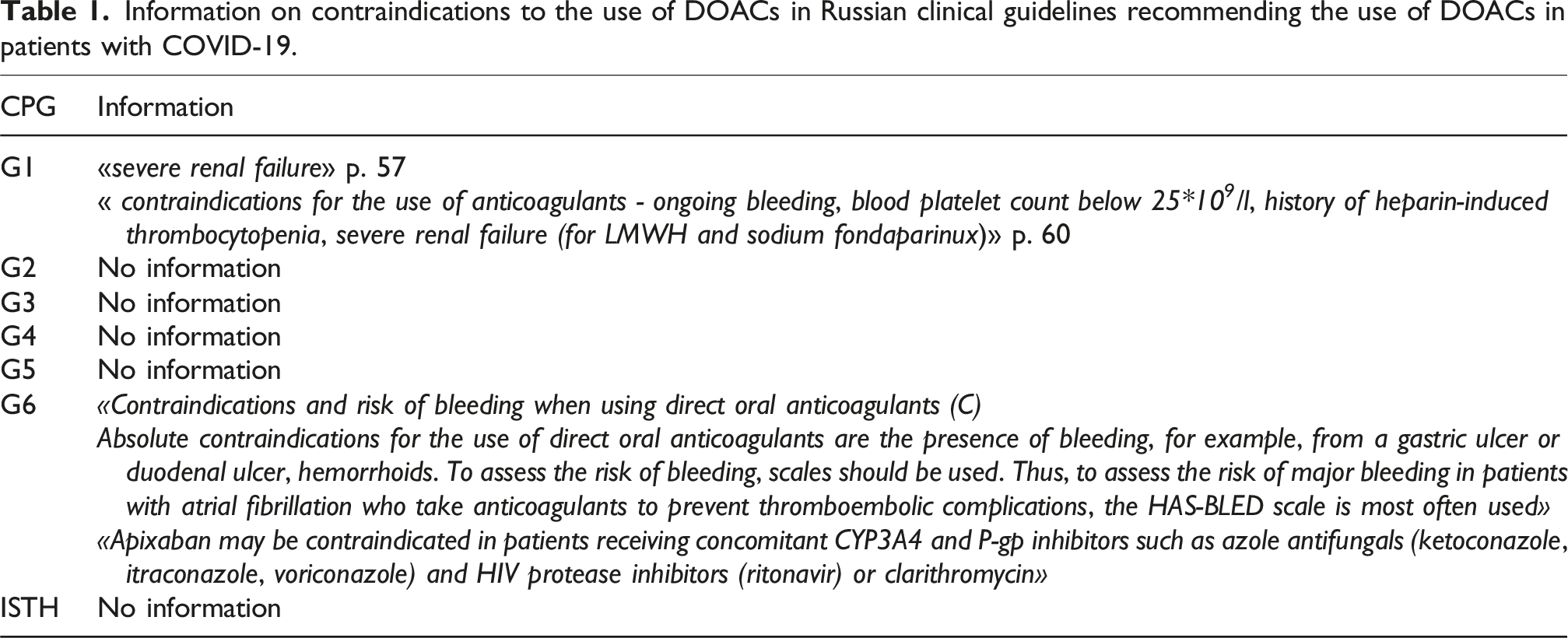
Contraindications for the use of DOAC
Information on contraindications to the use of DOACs in Russian clinical guidelines recommending the use of DOACs in patients with COVID-19.
Dosage regimen and duration of therapy
Information on recommended dosage regimens and duration of therapy with DOACs in Russian CPGs recommending DOAC use in COVID-19 patients.
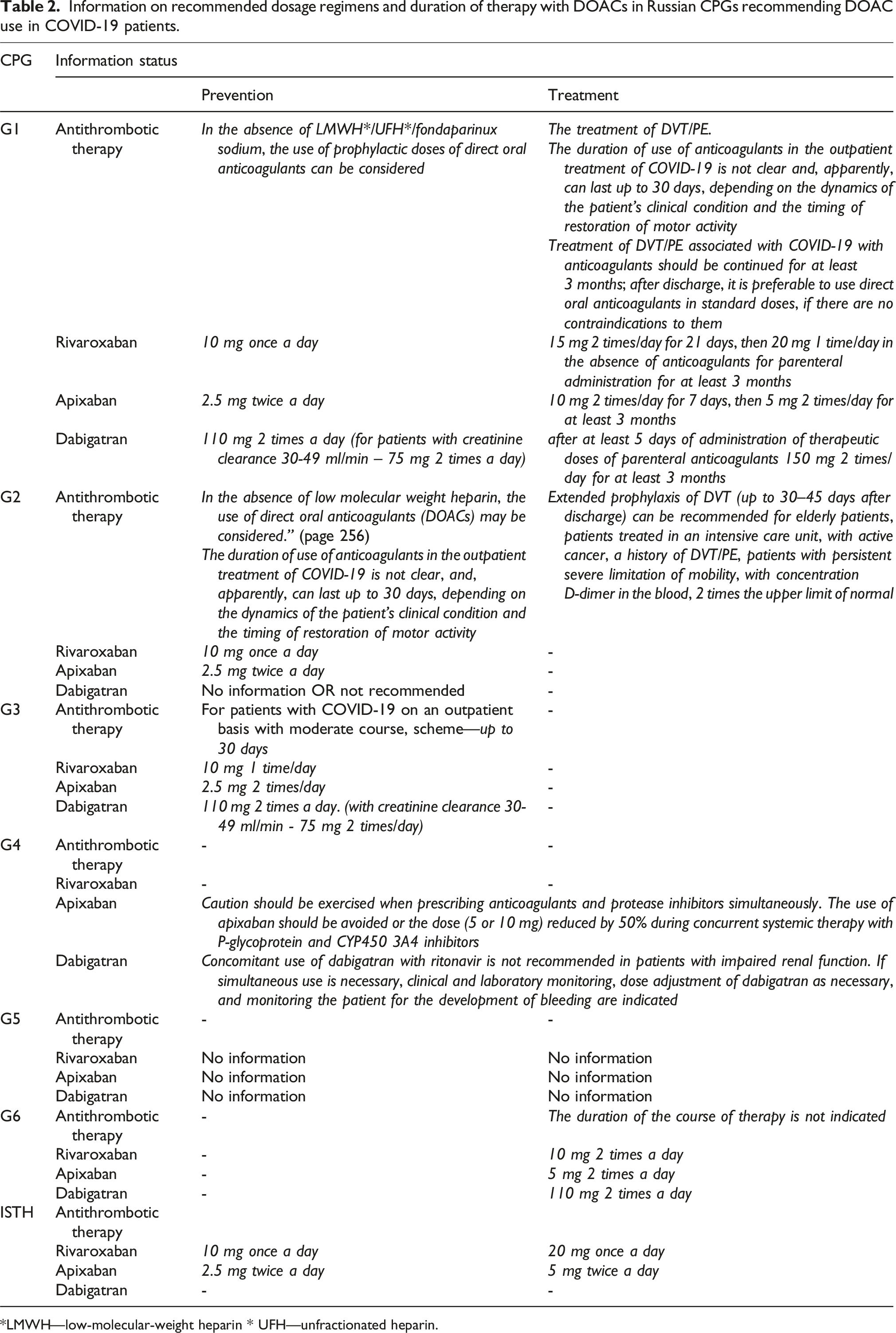
*LMWH—low-molecular-weight heparin * UFH—unfractionated heparin.
Only two of the six guidelines (G2 and G4) had a dedicated paragraph for safety monitoring of DOAC use with recommendation of clinical watchful monitoring.
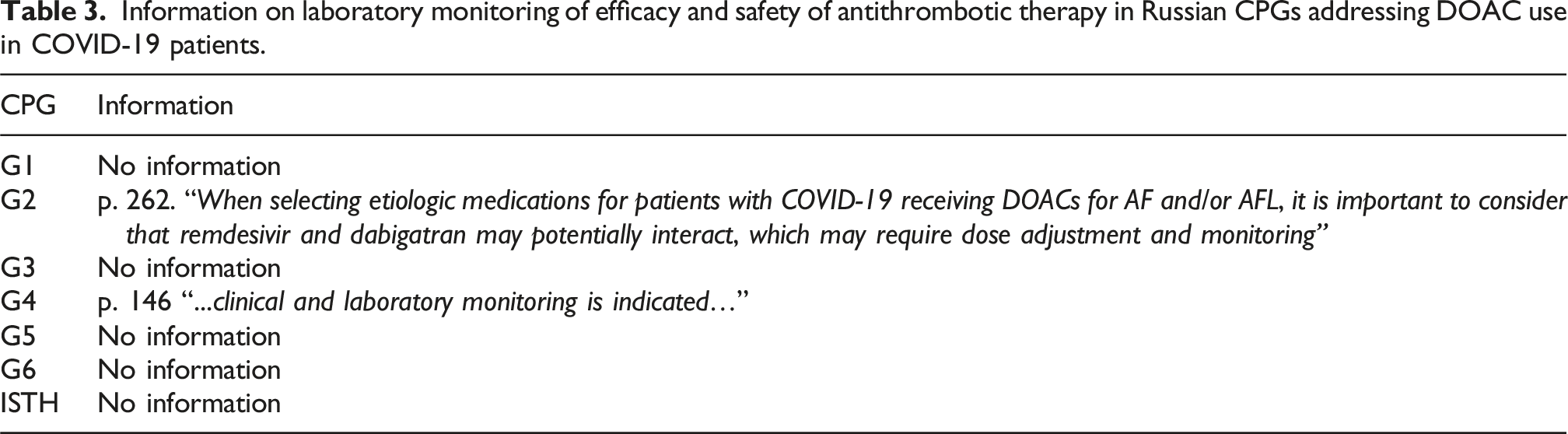
Safety monitoring and laboratory control methods and frequency
After a thorough analysis of the six clinical practice guidelines in terms of indications, dosage and laboratory monitoring methods of DOACs, we found that a clear recommendation that DOACs should not be used in outpatients with COVID-19 in community settings (at home), provided that patients do not have chronic conditions requiring stable anticoagulation, was given only in one CPG, G1: “The use of anticoagulants for the treatment of COVID-19 at home is not recommended.”
Information on laboratory monitoring of efficacy and safety of antithrombotic therapy in Russian CPGs addressing DOAC use in COVID-19 patients.
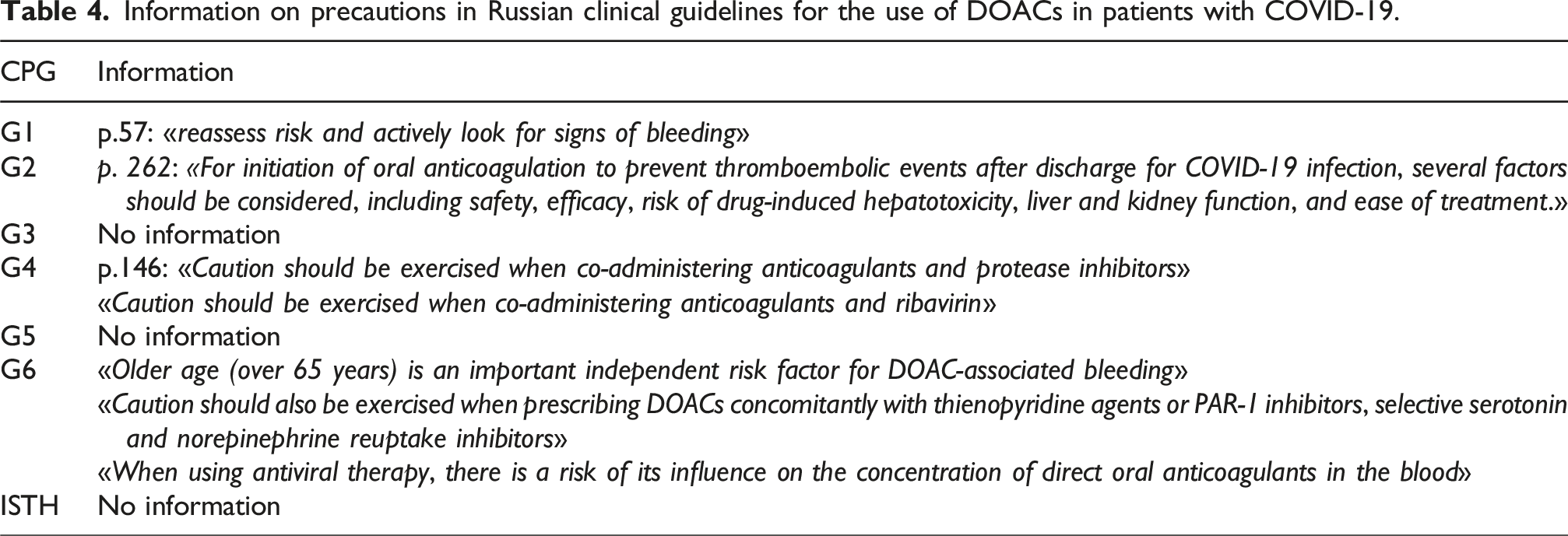
Precautions for the use of DOACs
Information on precautions in Russian clinical guidelines for the use of DOACs in patients with COVID-19.
Discussion
When comparing recommendations for the prevention of thrombotic and thromboembolic complications in patients with COVID-19 presented in Russian and international (CPG of the International Society on Thrombosis and Haemostasis (ISTH) 13 ) CPGs, we found many similarities and no significant differences in the indications, dosage and regimen, as well as the duration of DOAC therapy.
These differences are probably to the time of their development and publication. Most Russian guidelines were created at the beginning of the 2020–2021 pandemic, only G1 in 2022, as well as ISHT. During this period, experience was accumulated in the use of DOACs in outpatients with COVID-19, the results of clinical studies were obtained, systematic reviews3,4 were conducted, which made it possible to use DOAC more purposefully and rationally.
Russian clinical guidelines G1, 7 as well as ISTH guidelines, 13 note that the use of DOACs in outpatients with COVID-19 is not recommended, with the exception of patients discharged from hospital with a high risk of thromboembolic complications, as well as patients who previously took DOACs for other indications.
Russian CPGs provide more complete information on contraindications, which was reflected in recommendations G1 and G6.
Various dosage regimens of DOACs aimed at the prevention and treatment of thrombosis are presented both in ISTH and in several Russian CPGs: G1—dosage of DOACs for prophylaxis and treatment corresponds to ISTH recommendations; G2—the doses of DOACs are not indicated, the duration of the course of anticoagulant therapy and indications for extended prevention of thrombosis and thromboembolic complications in patients with COVID-19 after discharge from the hospital are described; G3—the guideline provides information only on the prophylactic regimen for prescribing DOACs; G4—the dosage is presented only for apixaban, there are recommendations for adjusting the dose of the drug in case of renal dysfunction and in combination with other drugs that are inhibitors of P450 3A4 and P-glycoprotein; G5—no information; G6—rivaroxaban treatment dose lower than ISTH guidelines. However, CPG G1 provides more detailed information on the duration of treatment with the possibility of prolonging the course of treatment, G1—rivaroxaban at doses of 20 mg once a day for at least 3 months. In addition, Russian CPGs provide the possibility of therapy with dabigatran: G1, G3, G6. The ISTH guidelines only mention apixaban and rivaroxaban.
DOACs generally don’t require routine laboratory monitoring for dose adjustment, unlike warfarin. However, laboratory testing can be helpful in specific clinical situations to assess DOAC levels or their effects on coagulation. Laboratory monitoring is noted in CPGs: G2, G4.
Only one clinical recommendation G6 contains indications about the need to evaluate the use of food and herbal supplements (horseradish, ginkgo, ginger, raspberry, etc.).
Almost all Russian clinical guidelines pay great attention to the drug interactions of DOACs.
All Russian clinical guidelines, except G3 and G5, describe situations in which DOACs should be used with caution. The risk group includes elderly patients, patients with severe renal failure, patients taking certain antiviral drugs, and others.
In general, it can be noted that the pharmacotherapy of DOACs proposed by Russian CPGs does not contradict international recommendations.
Our previous analysis of DOAC consumption by COVID-19 outpatients5,6 indicates excessive consumption of DOACs at the beginning of the pandemic. Given that some clinical guidelines contain incomplete information on the indications, dosage, and regimen for prescribing DOACs, it cannot be ruled out that this could be one of the reasons for the excessive consumption of DOACs by COVID-19 patients in 2020–2021.
The quality of clinical guidelines directly depends on the implementation of AGREE II requirements. Our previous analysis of the quality of Russian clinical guidelines for the treatment of patients with COVID-195,6 indicates, in general, their satisfactory quality but requires more complete and precise information on sections on stakeholder involvement, development rigor, applicability, and editorial independence.
Routine use of the AGREE II and RIGHT instruments in the creation of clinical guidelines and for quality control purposes will help avoid similar situations in the future and improve the quality of medical care provided to the population.
Limitations
Small sample size: we analyzed 6 Russian CPGs, which we identified in our searches of all Russian and International bibliographic databases and the Federal database/repository of all Clinical Practice Guidelines “Rubricator” (https://cr.minzdrav.gov.ru/clin-rec). The latest search was performed in May 2025.
Conclusions
1. The identified textual inconsistencies and insufficiently restrictive recommendations in Russian CPGs could have contributed to the excessive consumption of DOACs among COVID-19 outpatients during the pandemic. 2. Strengthening guideline quality, harmonizing recommendations with international standards, and promoting evidence-based prescribing practices are essential to prevent similar issues in future.
Supplemental Material
Supplemental Material - Why national consumption of direct oral anticoagulants over the rise of COVID-19 pandemic exceeded all potential recommendations: A qualitative analysis of textual details of Russian clinical practice guidelines
Supplemental Material for Why national consumption of direct oral anticoagulants over the rise of COVID-19 pandemic exceeded all potential recommendations: A qualitative analysis of textual details of Russian clinical practice guidelines by Elena A. Baybulatova, Mikhail S. Chenkurov, Sergey K. Zyryanov, and Liliya E. Ziganshina in International Journal of Risk & Safety in Medicine.
Footnotes
Author contributions
L.E.Z.: conceptualization, data curation, writing—original draft, writing—review and editing, supervision, resources, and methodology; S.K.Z.: conceptualization, supervision, resources, and methodology; E.A.B.: conceptualization, investigation, writing—original draft, and writing—review and editing; M.S.Ch.: investigation and writing—original draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The support for this project comes from the RUDN named after Patrcie Lumumba, project No 0321040000. Sponsor: Peoples’ Friendship University of Russia named after Patrice Lumumba.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.