
Abstract
Background
Linezolid is one of the most used antibacterials to treat resistant gram-positive infections, though its use may result in a number of toxic effects, especially in the older adults. There is lack of data derived from the real-world studies regarding safety of linezolid in the elderly.
The aim
To disclose the structure of adverse drug reactions (ADRs) associated with linezolid in patients ≥60 years.
Materials and methods
Retrospective analysis of spontaneous reports (SRs) from the Russian Pharmacovigilance database (April 2019–December 2024).
Results
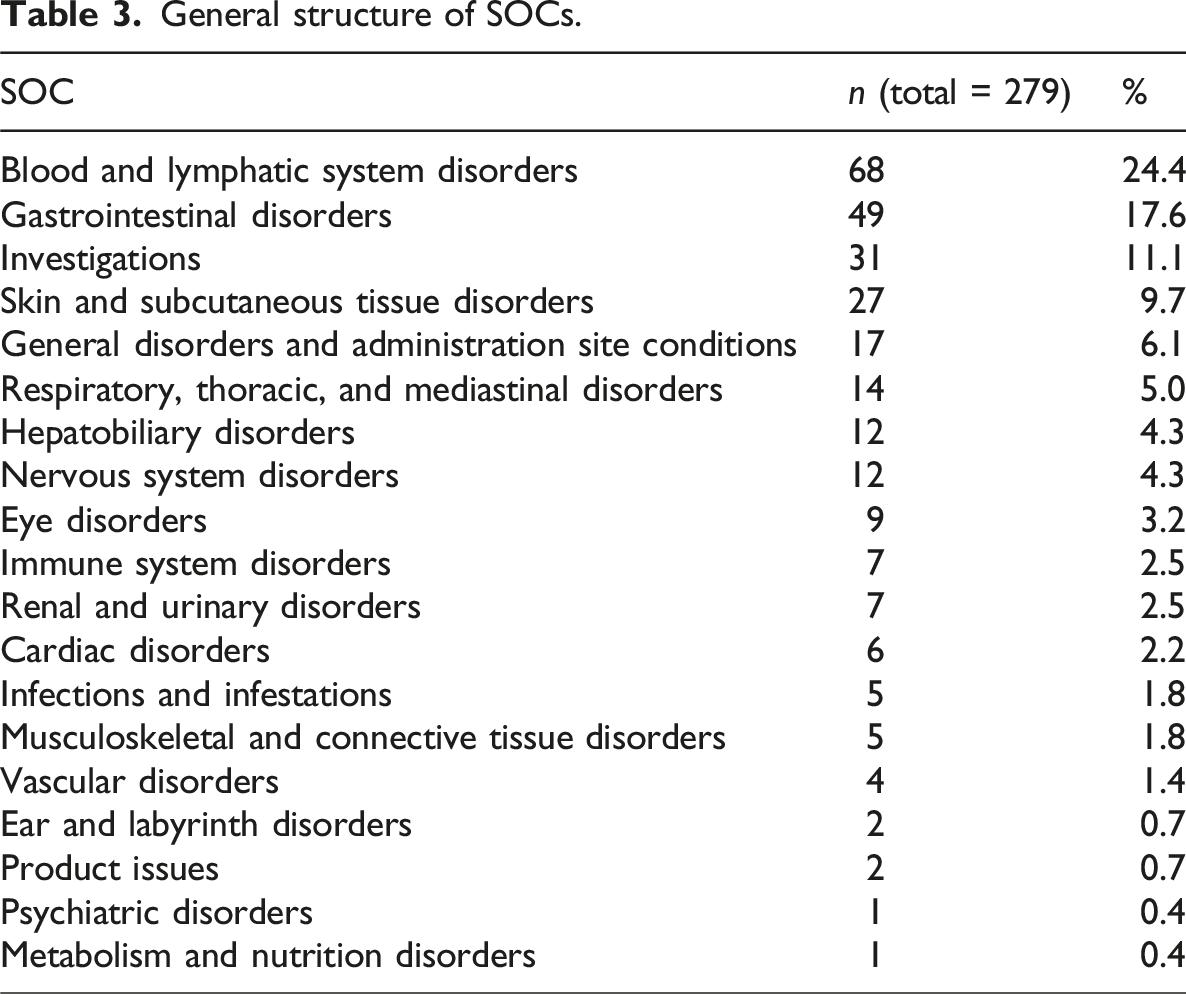
SRs of patients ≥60 years accounted up to 19.9% in the total structure of SRs. Top-5 system-organ classes (SOCs) were blood and lymphatic system disorders (24.4%, n = 68), gastrointestinal disorders (17.6%, n = 49), investigations (11.1%, n = 31), skin and subcutaneous tissue disorders (9.7%, n = 27), and general disorders and administration site conditions (6.1%, n = 17). Top-5 preferred terms (PTs) were thrombocytopenia (7.9%, n = 22), anemia (7.2%, n = 20), nausea 4.3% (n = 12), diarrhea (3.6%, n = 10), vomiting (3.6%, n = 10), and leukopenia (3.6%, n = 10).
Conclusions
Linezolid-induced myelosuppression was identified as the most significant safety concern in patients ≥60 years, underscoring the necessity for careful laboratory and clinical monitoring in this population.
Introduction
Infectious diseases remain a major contributor to morbidity and mortality in the elderly. Age-associated changes in physiology as well as presence of variable comorbidities make older adults more susceptible to infections compared with general population.1,2 Poorer outcomes represent another problem: older age is one of the main risk factors of sepsis development 3 and reduced survival rates. 4 Infections are among top-5 causes of intensive care unit admission in the elderly as it was reported by Cobert et al. (2022) who analyzed data extracted from Medicare-linked Health and Retirement Survey and disclosed information about patients ≥65 years old admitted to an intensive care unit (ICU) between 1998 and 2015. 5 Analysis of the main trends through the 17-year study period revealed stable increase in the prevalence of disability, frailty and multimorbidity among the elderly admitted to the ICU. 5 The structure of infections in the elderly was characterized in depth in the work by Karakoç-Parlayan et al. (2025). 6 In the age group 65–79 years a skin and soft tissue infections (42%) were identified as the main reasons for hospital admission while in ≥80 years patients urinary system infections (40%) and sepsis (24.6%) were among the leaders. 6 In general population of the elderly skin and soft tissue infections ranked first (32.2%). Gram-positive microflora was identified in 22.5% of patients aged 65–79 years and in 24.6% of those aged 80 years and older.
Among the most prevalent nosocomial Gram-positive pathogens methicillin-resistant Staphylococcus aureus (MRSA) poses a significant threat in the elderly population. 7 The World Health Organization (WHO) nominated MRSA as a “priority pathogen” due to the high rates of morbidity and mortality it causes, as well as the limited number of antibiotics effective against it. A representative of oxazolidinones class, linezolid is considered as a drug of choice to treat a variety of multidrug-resistant Gram-positive infections. 8 In the elderly population linezolid demonstrated a high efficacy. 9
Safety of linezolid is an important concern regarding clinical practice. There is a number of ADRs associated with linezolid use in the elderly. Hematological disorders, including linezolid-induced thrombocytopenia (LIT), are among the most common.10,11 Based on the results of different clinical trials frequency rates of LIT varies from 18.9% 11 to 28.1%. 12 Except hematotoxicity there are some other linezolid-induced ADRs affecting clinical outcomes in the elderly, including lactic acidosis, serotonin syndrome, neuropathy, myelosuppression, and hypoglycemia. 13
Several studies explain linezolid-associated ADRs by an increase of plasma concentrations above therapeutic values that is typical in the elderly due to age-associated changes of pharmacokinetics.14–16 Liu et al. (2024) analyzed age-related variations in linezolid trough concentrations and found that patients aged 65 to 80 years experienced an increase of 10 mg/L, with an additional rise of 10 mg/L for each subsequent decade of age. 17 The presence of renal impairment—a condition commonly found in older adults—has also been identified as a contributing factor to the increased risk of linezolid-induced toxicity, including LIT. 18 Hepatic impairment also may change concentration and safety profile of linezolid. 19
Considering the pharmacokinetic basis for linezolid toxicity and the comorbidity heterogeneity in elderly patients, real-world estimation of linezolid-induced ADRs in this population is essential. One of the best sources of safety data is national pharmacovigilance database. The aim of our study was to assess the structure of ADRs associated with linezolid use in the elderly population as well as demographic characteristics of patients using data of Russian National Pharmacovigilance database–Automatized Information System “Pharmacovigilance” (AIS).
Materials and methods
Data source
Pharmacovigilance is the main tool to ensure the safety and efficacy of pharmaceutical products by monitoring, detecting, assessing, understanding, and preventing ADRs. The Federal Service for Surveillance in Healthcare (Roszdravnadzor) is responsible for monitoring of drug safety and effectiveness in the Russian Federation. Russian legislation declares that all organizations engaged in the circulation of medications must provide reporting on ADRs into Roszdravnadzor. The AIS database was launched in 2008; it accumulates all SRs with ADRs data. Functioning of AIS is organized following guidelines of the Eurasian Economic Union and the International Council for Harmonization (ICH).20,21 Detection of SOCs and PTs was made according to MedDRA version 28.0. Drugs identification was made by brand names and international nonproprietary names. Causality assessment within the AIS database is performed using WHO algorithm alongside the Naranjo algorithm. Definitions were derived from 22 :
“Adverse reaction—A response to a medicinal product, which is noxious and unintended. Adverse reaction may arise from use of the product within or outside the terms of the marketing authorization or from occupational exposure. Use outside the marketing authorization includes off-label use, overdose, misuse, abuse, and medication errors.”
“Causality—In accordance with ICH-E2A, the definition of an adverse reaction implies at least a reasonable possibility of a causal relationship between a suspected medicinal product and an adverse event. An adverse reaction, in contrast to an adverse event, is characterized by the fact that a causal relationship between a medicinal product and an occurrence is suspected. For regulatory reporting purposes, as detailed in ICH-E2D, if an event is spontaneously reported, even if the relationship is unknown or unstated, it meets the definition of an adverse reaction. Therefore, all spontaneous reports notified by healthcare professionals or consumers are considered suspected adverse reactions, since they convey the suspicions of the primary sources, unless the reporters specifically state that they believe the events to be unrelated or that a causal relationship can be excluded.”
“A spontaneous report is an unsolicited communication by a healthcare professional, or consumer to a competent authority, marketing authorization holder or other organization (e.g., regional pharmacovigilance center, poison control center) that describes one or more suspected adverse reactions in a patient who was given one or more medicinal products. It does not derive from a study or any organized data collection systems.”
Study design and data selection
A retrospective, descriptive study of SRs registered in the AIS database for the period April 1, 2019–December 31, 2024 was performed. A flowchart of SRs selection is given in Figure 1. A high probability of a causal relationship (“certain,” “probable,” “possible”) was the main inclusion criteria in our study. Duplicate and invalid reports were excluded. SRs were considered duplicates in case they were sent by different reporters but contained the same patient data, the same suspected drug and ADRs. SRs with lack of data on the reporter/patient/suspected drug/ADR were considered invalid. Final analysis included SRs occurred on the territory of Russian Federation in the patients ≥60 years old. Flowchart of SRs selection.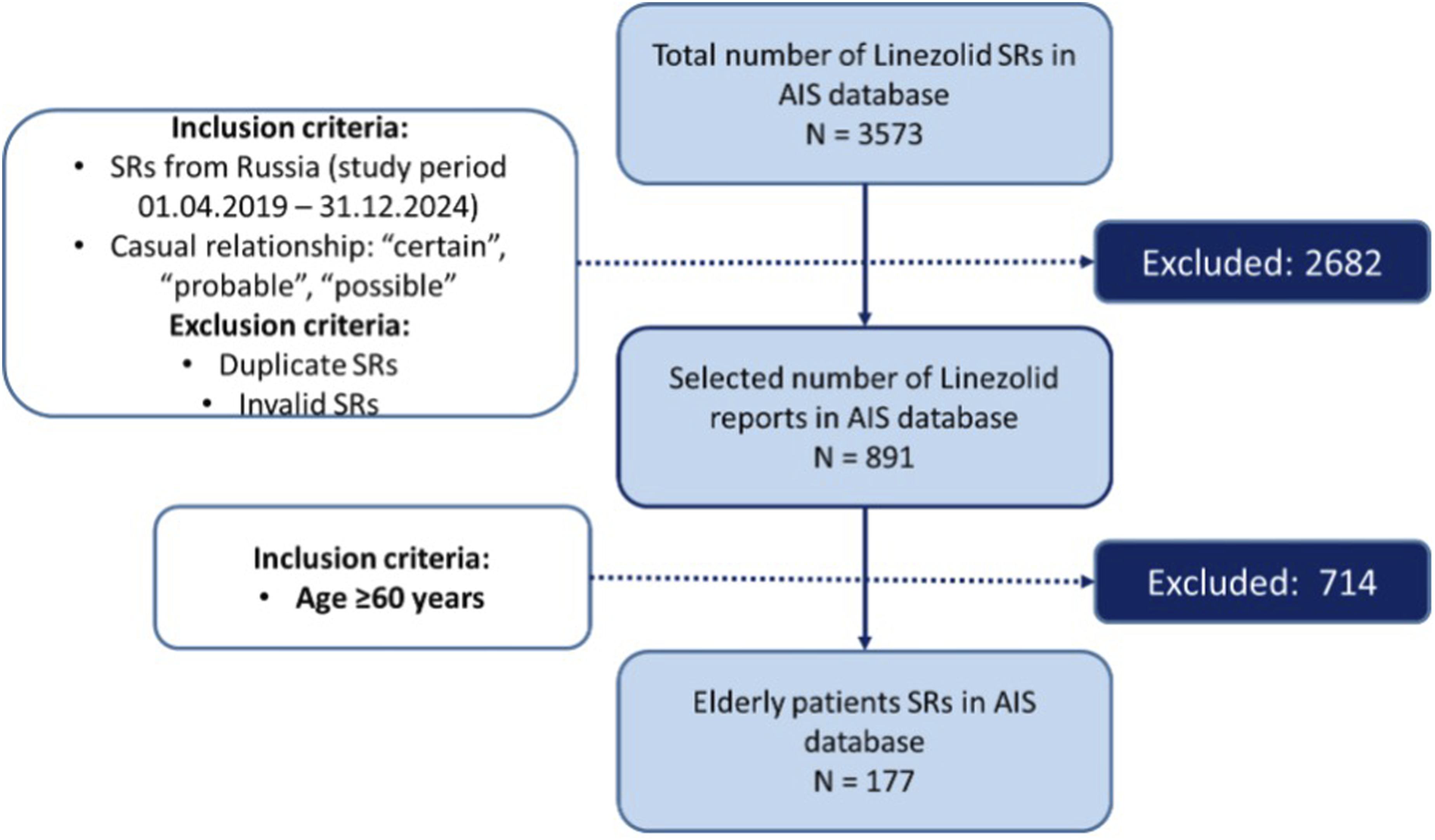
European Medicines Agency Guidelines were used to identify validity of SRs. SRs were included in the study only in case of presence of at least four essential elements: an identifiable reporter, an identifiable patient, at least one suspected drug, and at least one suspected ADR. 22 Failure to meet the specified requirements led us to deem the SRs invalid and exclude them from the study. Finally included SRs were used as a source of information about ADRs and demographic characteristics.
Statistical analysis
Descriptive statistics were used for all analyzed parameters; qualitative variables were described using absolute (n) and relative (%) values. All statistical analyses were performed in Microsoft Excel 2019.
Results
A total of 891 SRs implicating linezolid as a suspected drug were retrieved from the AIS database following application of the selection criteria “occurrence within the territory of the Russian Federation” and “high probability of a causal relationship.” The proportion of SRs in the elderly (≥60 years) accounted up to 19.9% (n = 177). Age and gender data were found in 100% of SRs. Male gender was indicated in 55.9% (n = 99) of SRs and female in 44.1% (n = 78). Mean age was 68 ± 7 (min = 60, max = 87, Median (Me) = 66, (Interquartile range, IQR (Q1–Q2): 63, 72) years.
Most patients were in the age group 60–74 years (83.6%, n = 148), and 16.4% (n = 29) belonged to the group 75–90 years.
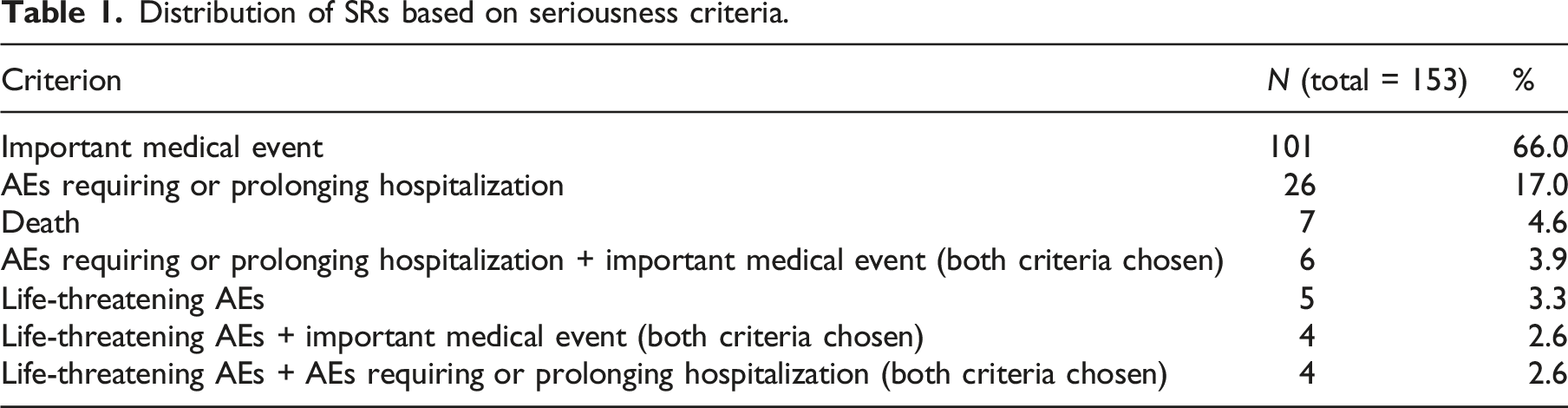
Outcome analysis revealed improvement in 41.8% (n = 74) of SRs, recovery without consequences in 25.4% (n = 45), condition unchanged in 22.0% (n = 39), unknown outcome in 6.8% (n = 12), and death in 4.0% (n = 7).
Distribution of SRs based on seriousness criteria.
The structure of indications to use linezolid in the elderly based on data indicated in SRs.

A total of 279 ADRs were detected in our study. Mean number of ADRs per SRs was 1.6 ± 1.2 (min = 1, max = 10, Me = 1, IQR: 1, 2). SRs reporting one ADR made up 70.6% (n = 125), those with two ADRs—16.9% (n = 30), SRs with three to four ADRs—9.0% (n = 16), and SRs with ≥5 ADRs—3.4% (n = 6). Figure 2 illustrates the time trends in the number of SRs regarding linezolid in the population ≥60 years. Time trends in the number of SRs containing information on linezolid-induced ADRs.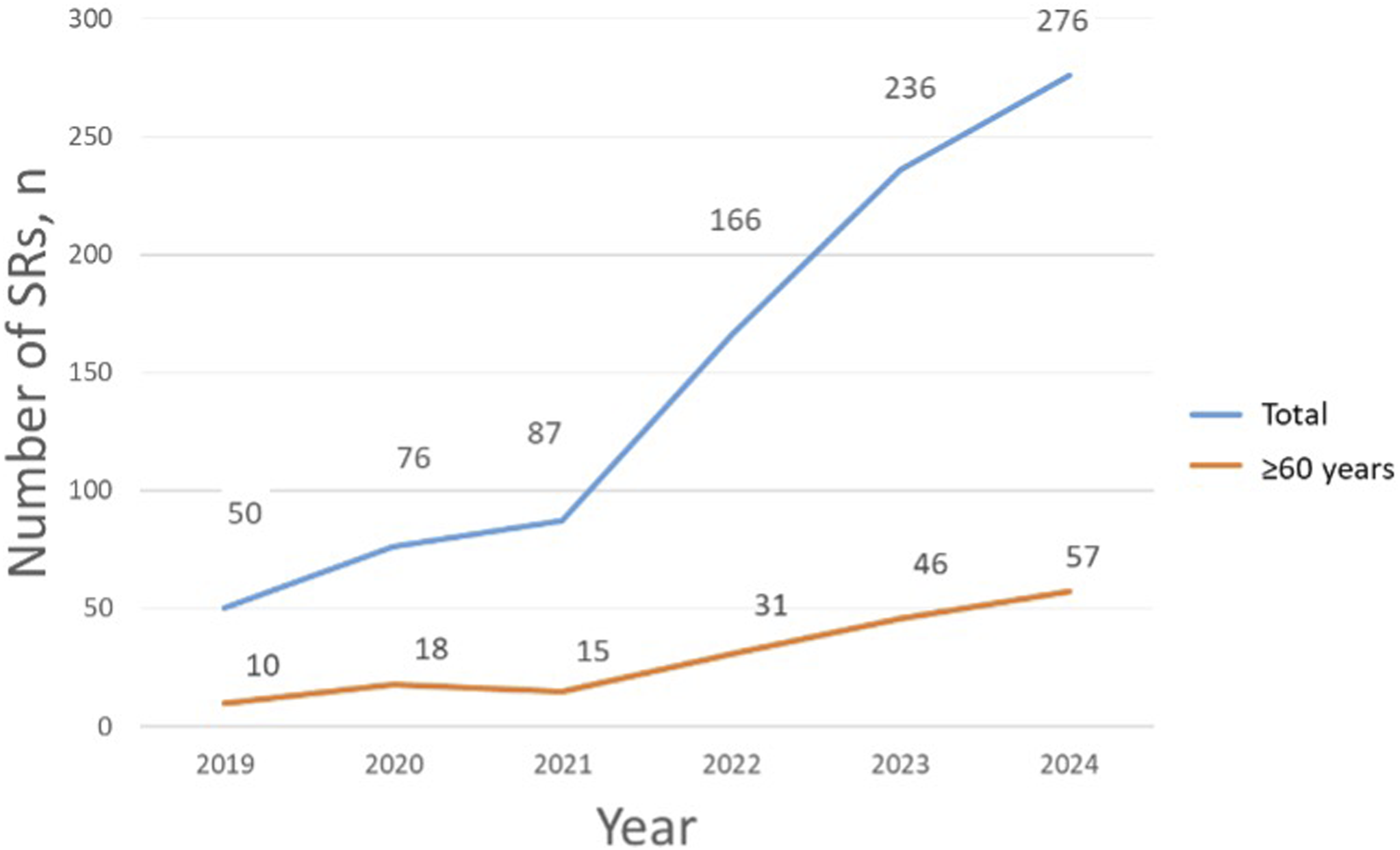
Estimating time to ADR onset we revealed no information in 11.3% of SRs (n = 20). Based on the presented data, the mean time to onset of ADRs was 41.1 ± 66.7 days (min = 1, max = 365, Me = 12, IQR: 3, 46) days.
General structure of SOCs.
The most involved SOC was “Blood and lymphatic system disorders.” 31.1% (n = 55) of SRs included PTs belonging to this SOC. Data assessment revealed male gender in 56.4% (n = 31), female in 43.6% (n - 24). Mean age was 67.2 ± 6.7 (min = 60.0, max = 86.0, Me = 66.0, IQR: 61.5, 70.5) years.
Mean time to ADR onset in the given SOC was 50.6 ± 64.3 (min = 2, max = 270, Me = 15, IQR: 10.5, 60.0) days.
Next outcomes were revealed regarding SOC “Blood and lymphatic system disorders”: condition unchanged (45.5%, n = 25), condition improved (36.4%, n = 20), recovery without consequences (10.9%, n = 6), death (1.8%, n = 1), unknown (5.5%, n = 3).
Structure of PTs in the SOC “Blood and lymphatic system disorders.”

SOC “Gastrointestinal disorders” ranked second due to our results; it was found in 20.3% of SRs (n = 36). Male gender was reported in 55.6% (n = 20), and female in 44.4% (n = 16). Mean age was 68.1 ± 7.3 (min = 60.0, max = 87.0, Me = 65.5, IQR: 63.0, 73.0) years.
Mean time to ADR onset within the given SOC was nearly twice reduced compared with that of the SOC “Blood and lymphatic system disorders” and comprised of 26.8 ± 52.0 (min = 1.0, max = 180.0, Me = 9.5, IQR: 3.8, 15.0) days.
Outcome analysis revealed negative results only in 13.9% (condition unchanged, n = 4 and death, n = 1). Outcome “condition improved” was detected in 41.7% (n = 15), “recovery without consequence”—in 38.9% (n = 14). No data on outcome was in 5.6% (n = 2) of SRs.
Structure of PTs in the SOC “Gastrointestinal disorders.”

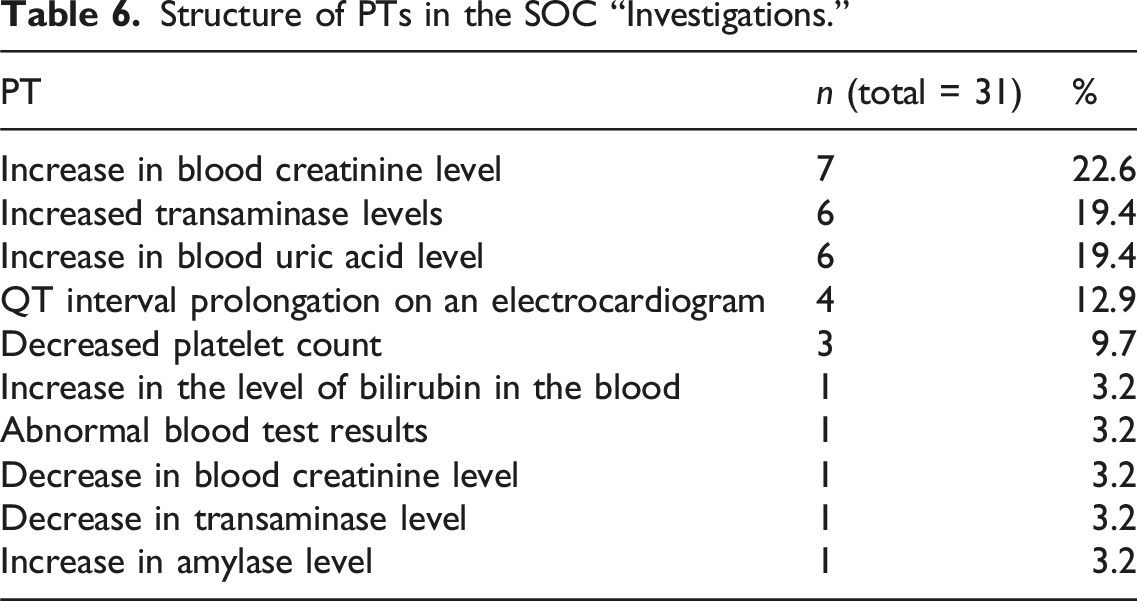
The third position in the total structure of SOCs was for “Investigations.” 13% of SRs contained data related to this SOC (n = 23). According to the data in SRs, male gender was detected in 65.2% (n = 15), female in 34.8% (n = 8). Mean age was 69.4 ± 8.1 (min = 60.0, max = 87.0, Me = 68, IQR: 62.5, 74.0) years.
Mean time to ADR onset was 74.3 ± 70.8 (min = 1.0, max = 180.0, Me = 52.0, IQR: 22.8, 112.5) days.
Structure of PTs in the SOC “Investigations.”
SOC “Skin and subcutaneous tissue disorders” was found in 14.7% of SRs (n = 26). Male gender was seen in 38.5% (n = 10) and female in 61.5% (n = 16). Mean age was 67.3 ± 6.1 (min = 60.0, max = 85.0, Me = 66.0, IQR: 63.3, 72.0) years.
Data on time to ADR onset was found in 25 SRs. There was a shortest time to ADR onset in the SOC “Skin and subcutaneous tissue disorders”. Mean time was 3.7 ± 4.1 (min = 1, max = 14, Me = 2, IQR: 1.0, 4.0) days.
Structure of PTs in the SOC “Skin and subcutaneous tissue disorders”.

The last among top-5 SOCs identified in our study was “General disorders and administration site conditions.” It was detected in 9% of SRs (n = 16). Using data in SRs we revealed male gender in 18.8% (n = 3), female in 81.3% (n = 13). Mean age was 70.2 ± 6.9 (min = 61.0, max = 87.0, Me = 70.5, IQR: 64.8, 73.0).
Data on time to ADR onset was absent in one SR (6.3%). Mean time to ADR onset was 51.7 ± 85.8 (min = 1.0, max = 270.0, Me = 11.0, IQR: 1.0, 49.0) days.
Structure of PTs in the SOC “General disorders and administration site conditions.”

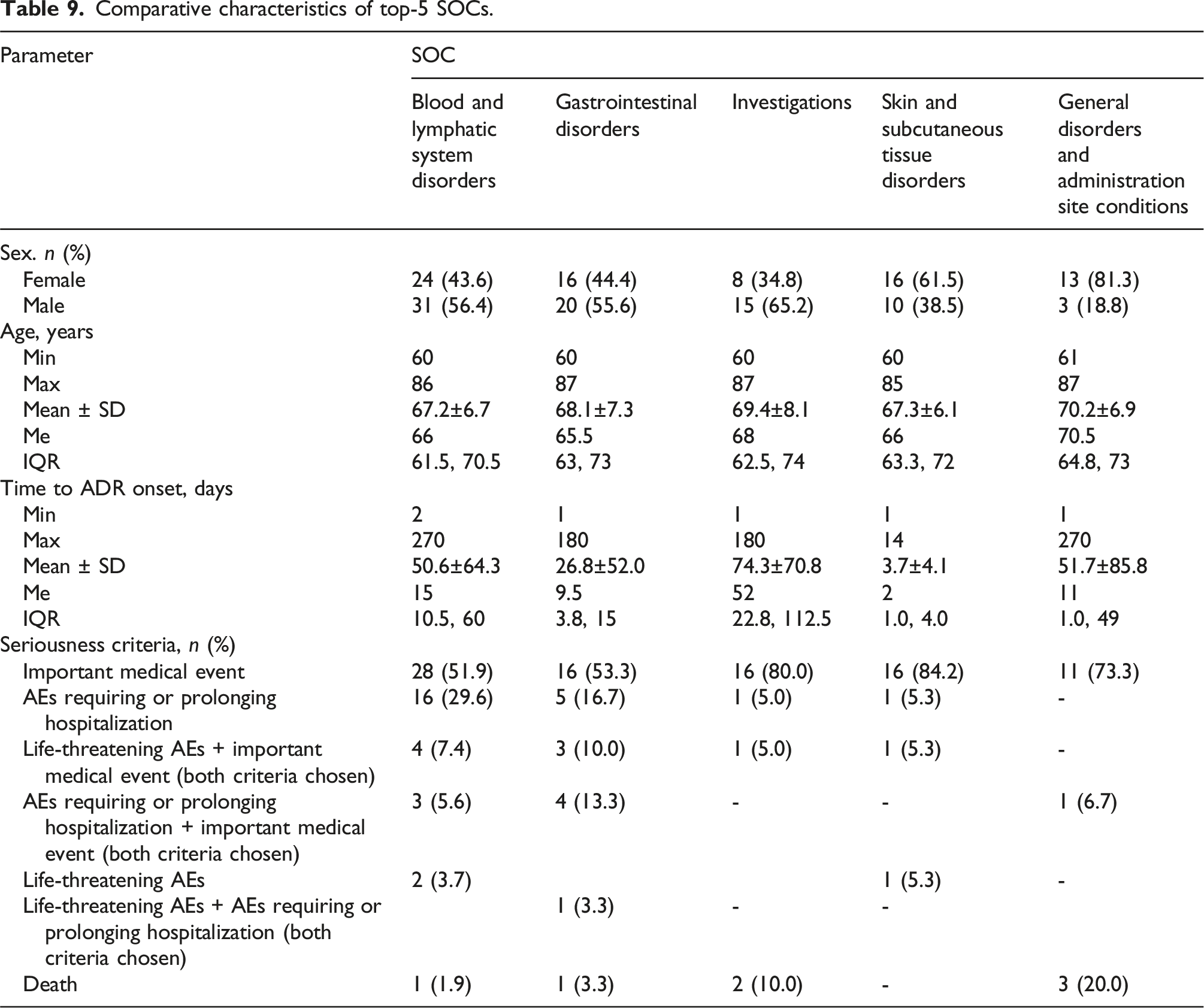
Comparative characteristics of top-5 SOCs.
General structure of PTs revealed in SRs of patients ≥60 years.
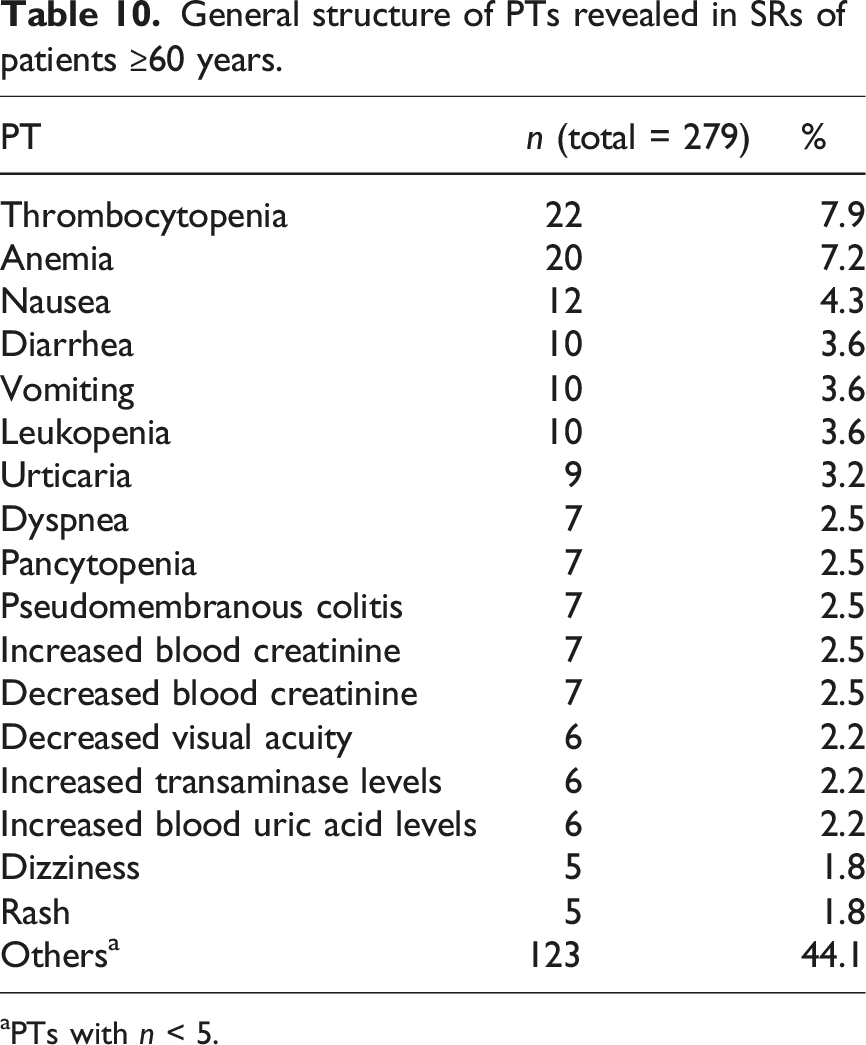
aPTs with n < 5.
Analyzing demographic data indicated in SRs with thrombocytopenia we revealed higher prevalence of female gender (females were 63.6% (n = 14), males were 36.4% (n = 8)). Mean age was 69.8 ± 7.9 (min = 60.0, max = 86.0, Me = 68.0, IQR: 63.3, 75.3) years. Assessment of time to ADR onset revealed no data in one SR (4.5%). Mean time to thrombocytopenia onset was 51.7 ± 65.7 (min = 2.0, max = 210.0, Me = 16.0, IQR: 11.0, 60.0) days.
Anemia ranked second in the total structure of PTs (7.2%, n = 20). Male gender was indicated in 80% (n = 16), female in 20% (n = 4). Mean age was 64.1 ± 4.3 (min = 60.0, max = 75.0, Me = 63.0, IQR: 60.7, 67.3) years. There was no information on time to ADR onset in one SR (5%). Using data from 19 SRs we revealed that mean time to anemia onset was 56.8 ± 67.7 (min = 2.0, max = 210.0, Me = 39.0, IQR: 7.5, 64.0) days.
The third most prevalent PT found in our study was nausea 4.3% (n – 12). Half of patients were male and half female (n – 6 for each). Mean age was 67.5 ± 8.1 (min = 60.0, max = 82.0, Me = 64.0, IQR: 61.0, 70.6) years. Mean time to ADR onset was 5.6 ± 4.8 (min = 1.0, max = 18.0, Me = 8.0, IQR: 2.5, 10.8) days.
The same contribution into the total structure of PTs was made by diarrhea, vomiting, and leukopenia (n = 10 for each). In 70% of SRs with diarrhea male gender was reported (n = 7), in 30% (n = 3)—female. Mean age was 70.7 ± 7.5 (min = 61.0, max = 82.0, Me = 70.5, IQR: 65.0, 75.6) years. No data on time to ADR onset was in 3 SRs (30%). Mean time to diarrhea onset was 7.4 ± 6.1 (min = 2, max = 16, Me = 4.0, IQR: 2.5, 12.5) days. In SRs with vomiting male gender was detected in 60% (n – 6), female – in 40% (n = 4). Mean age was 66.6 ± 5.5 (min = 60.0, max = 80.0, Me = 65.5, IQR: 83.3, 67.8) years. Mean time to vomiting onset was 8.7 ± 9.1 (min = 1.0, max = 30.0, Me = 4.5, IQR: 3.0, 12.8) days. In 60% of SRs with leukopenia male gender was reported (n = 6), and female in 40% (n = 4). Mean age was 65 ± 5.3 (min = 60.0, max = 73.0, Me = 62.5, IQR: 60.3, 70.5) years. No data on time to ADR onset was in 1 SR (10%). Mean time to leukopenia onset was 8.7 ± 18.5 (min = 6, max = 60, Me = 11.0, IQR: 9.0, 12.0) days.
Discussion
Our study disclosed the structure of ADRs induced by linezolid in the elderly in Russia. Top-5 identified SOCs were blood and lymphatic system disorders (24.4%), gastrointestinal disorders (17.6%), investigations (11.1%), skin and subcutaneous tissue disorders (9.7%), and general disorders and administration site conditions (6.1%). Due to the results of FDA’s Adverse Event Reporting System (FAERS) database analysis which included SRs with linezolid-induced ADRs top-5 SOCs were general disorders and administration site conditions (12.47%), blood and lymphatic system disorders (12.19%), nervous system disorders (10.23%), investigations (9.54%), and gastrointestinal disorders (n = 2,802, 9.21%). 13 In this study no information about age was in 97.15%, and age analysis covered less than 3% of SRs. Authors revealed close proportions of age groups 18–64 years (1.45%) and >64 years (1.23%).
SOC “blood and lymphatic system disorders” ranked first in our study. PT “thrombocytopenia” was the most prevalent both in the given SOC (32.4%) and in the total PT structure (7.9%). This stands in line with several studies dedicated to linezolid safety profile. The highest frequency of thrombocytopenia in PT structure (3.74%) was detected in FAERS database by Zou et al. (2024). 13 Clinical studies indicate a greater frequency of LIT. The results of a systematic review and meta-analysis including data from 6454 patients treated with linezolid revealed LIT in 37%. 23 Among hospitalized patients with median age 62 years LIT was detected in 43.3%, and affected cohort showed a significantly greater accumulated in-hospital mortality compared with patients without LIT (19.7% vs 8.6%, p = 0.003). 24 A retrospective observational cohort study involving 102 patients found that the incidence of new-onset thrombocytopenia among those treated with linezolid for a minimum of 5 days was 17.6%. Patients with LIT were older than that without (mean age 58 ± 17 vs 49 ± 22). 25 In the work by Zhao et al. (2024) artificial neural network model was implemented to predict risk factors of LIT development. The highest level of importance was found for urea level, followed by albumin, baseline platelet value, creatinine clearance, total protein age, history of hypertension, aspartate aminotransferase level, history of malignancy, and direct bilirubin level. 26 A strong negative correlation between linezolid concentrations, ranging from 0.5 to 14.7 μg/mL, and platelet count was demonstrated in a study that utilized ultra-performance liquid chromatography coupled with tandem mass spectrometry method to measure linezolid plasma levels followed by correlation analysis. 27
Anemia was the second most prevalent PT detected in our study (7.2%). Anemia also ranked second in the overall structure of PTs according to the results of the FAERS database analysis (2.31%). 13 Clinical trials demonstrated higher incidence of linezolid-induced anemia. For example, a retrospective study including elderly patients (Me = 79.00, IQR: 71.50, 87.50 years) revealed linezolid-induced anemia in 18.54%. 28 Another study (analysis of hospital’s electronic medical records for the period January 2014 and December 2020) demonstrated linezolid-induced anemia in 10.7%. Multivariate logistic analysis realized in this work brought to light a list of independent risk factors for linezolid-induced anemia: age ≥60 years, increased total bilirubin, estimated glomerular filtration rate <60 ml/(min·1.73 m2), duration of linezolid therapy, and ICU admittance. 29 In the cohort of patients received linezolid for more than 10 days anemia developed in 17.9% and LIT in 35.9%. 30 Authors demonstrated increased risks of haematotoxicity in patients with hepatic and/or renal dysfunction. Of interest are the data obtained in the work of Cattaneo et al. (2023), where it was shown that LIT is more common in patients with gram-positive infections, while anemia in patients with tuberculosis. 31 It is proved by the results gained by Pratama et al. (2021) on the cohort of patients with multidrug-resistant tuberculosis treated by linezolid: anemia was seen in 29.0% while LIT only in 3.2%. 32
Nausea (4.3%), diarrhea (3.6%), and vomiting (3.6%) were among top-5 PTs in our study. Their high prevalence made SOC “Gastrointestinal disorders” to be the second in the total SOC structure. Broad involvement of gastrointestinal tract in linezolid-induced ADRs was also demonstrated by the results of FAERS database analysis (2004 to 2023 years): SOC “Gastrointestinal disorders” rounded out the top-5 detected SOCs. 13 In the retrospective study which included patients who used linezolid for more than 28 days (median treatment duration was 42 days) gastrointestinal intolerance (42%) was the most prevalent safety concern. 33 Due to the results of another retrospective observational study (4 Belgian hospital centers, n = 230) gastrointestinal disorders ranked third in the overall structure of ADRs (5.2%). 11
Leukopenia, with an incidence of 3.6%, was the fifth most frequently identified PT in our study. Its presence together with LIT and anemia indicates high myelotoxicity of linezolid in the elderly. FAERS database analysis revealed leukopenia in 0.48%. 13
Linezolid-induced myelosuppression manifested with pancytopenia may be the result of mitochondrial dysfunction and impaired protein synthesis in hematopoietic cells. Mechanism of action of linezolid can give explanation to this phenomenon. Oxazolidinone antibacterials bind to bacterial 23S part of the 50S ribosomal subunit inhibiting formation of a 70S initiation complex and further mitochondrial protein synthesis.34,35 The similarity between bacterial 23S ribosomal ribonucleic acid (RNA) and human mitochondrial 16S ribosomal RNA has been proposed as a potential cause of human toxicity.34,36 Linezolid disrupts the mitochondrial respiratory chain by decreasing the enzymatic activity of cytochrome oxidase. 36 Studies demonstrated ability of linezolid to violate mitochondrial ultrastructure, inhibit expression of mitochondrial proteins and oxidative metabolism. 37 Linezolid was shown to inhibit megakaryocyte differentiation from hematopoietic progenitor cells which is considered to be an important mechanism of LIT. 38
Our study emphasizes the need for a close ADRs monitoring in the elderly receiving linezolid. Since ADRs occurrence may correlate with increased level of linezolid plasma concentration,17–19 therapeutic drug monitoring should be considered routine in the elderly with chronic kidney disease, that is supported by the results of a systematic review and meta-analysis by Liu et al. (2022). 39 The study performed by Zhao et al. (2024) demonstrated that the optimal LIT prediction in patients with renal impairment includes estimation of linezolid concentration together with PNU-142300 (metabolite of linezolid) concentration. 40 An expert consensus on therapeutic drug monitoring and individualization of linezolid dosing was published in 2022. 41 An important consensus statement regarding LIT included recommendation to monitor platelets count in patients receiving linezolid therapy. Another expert recommendation was to start LIT pharmacotherapy in patients requiring linezolid treatment for more than 1 month who exhibit trough concentrations exceeding 8 mg/L, particularly if they belong to the following categories: elderly individuals, patients with renal insufficiency, those with thrombocytopenia, and individuals with low body weight. 41
Limitations of the study
A key issue regarding pharmacovigilance studies is a fact that the quantity of SRs does not accurately represent the actual drug consumption levels within the population, meaning the incidence of ADRs observed in pharmacovigilance studies may differ from those reported in clinical trials. Since our study was based on the analysis of SRs accumulated in the pharmacovigilance database, we had no data on linezolid concentrations and renal and/or hepatic function which limits understanding of the basis of detected linezolid-induced ADRs. Next limitation of our study was absence of information on comorbidities and concomitant pharmacotherapy in most of SRs, so it was impossible to uncover the impact of these factors in ADRs development.
Conclusion
Pharmacovigilance database analysis indicates that linezolid-induced myelosuppression is the most important safety concern in patients ≥60 years. SOC “blood and lymphatic disorders” accounted for almost a quarter of cases in our study. LIT was shown to be an absolute leader in the structure of PTs.
Supplemental Material
Supplemental Material - Safety profile of linezolid in the elderly: National database analysis
Supplemental Material for Safety profile of linezolid in the elderly: National database analysis by Olga Butranova, Victoria Koval, Sergey Zyryanov, Irina Asetskaya, Elizaveta Terehina, Vitaly Polivanov, Anastasia Gorbacheva in International Journal of Risk & Safety in Medicine
Supplemental Material
Supplemental Material - Safety profile of linezolid in the elderly: National database analysis
Supplemental Material for Safety profile of linezolid in the elderly: National database analysis by Olga Butranova, Victoria Koval, Sergey Zyryanov, Irina Asetskaya, Elizaveta Terehina, Vitaly Polivanov, Anastasia Gorbacheva in International Journal of Risk & Safety in Medicine
Supplemental Material
Supplemental Material - Safety profile of linezolid in the elderly: National database analysis
Supplemental Material for Safety profile of linezolid in the elderly: National database analysis by Olga Butranova, Victoria Koval, Sergey Zyryanov, Irina Asetskaya, Elizaveta Terehina, Vitaly Polivanov, Anastasia Gorbacheva in International Journal of Risk & Safety in Medicine
Supplemental Material
Supplemental Material - Safety profile of linezolid in the elderly: National database analysis
Supplemental Material for Safety profile of linezolid in the elderly: National database analysis by Olga Butranova, Victoria Koval, Sergey Zyryanov, Irina Asetskaya, Elizaveta Terehina, Vitaly Polivanov, Anastasia Gorbacheva in International Journal of Risk & Safety in Medicine
Footnotes
Author contributions
all authors share the same contribution in terms of work with sources, statistical analysis, writing of a draft and final manuscript version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.