
Abstract
Background
Polycystic ovary syndrome (PCOS) is a prevalent endocrine disorder in women of reproductive age, characterized by menstrual irregularities, hyperandrogenism, and polycystic ovaries. Insulin resistance is central to its pathophysiology, contributing to metabolic disturbances and increased cardiometabolic risks. High-Intensity Interval Training (HIIT) has emerged as a promising intervention to improve metabolic health.
Objective
This study aimed to investigate the specific effects of HIIT on insulin sensitivity, body composition, metabolic profile, and quality of life in women with overweight PCOS.
Methods
A retrospective analysis was conducted on 107 female patients with overweight PCOS who were divided into two groups: the Regular Interval Training Group (n = 54) and the HIIT Group (n = 53). Baseline data, including insulin sensitivity, glucose metabolism, body composition, metabolic profile, and quality of life, were measured and compared between the two groups.
Results
The HIIT Group demonstrated significantly improved insulin sensitivity, reduced fasting glucose levels, lower HOMA-IR index, lower body fat percentage, decreased waist and hip circumferences, improved favorable changes in metabolic profile, and significant improvements in quality of life compared to the Regular Interval Training Group. These findings suggest that HIIT led to beneficial outcomes across various metabolic and clinical parameters in women with overweight PCOS.
Conclusion
The findings of this study highlight the potential of personalized exercise prescriptions, such as HIIT, in optimizing health outcomes in women with overweight PCOS. The observed improvements in insulin sensitivity, body composition, metabolic profile, and quality of life underscore the promising role of HIIT in addressing the multifaceted implications of PCOS and its associated metabolic and reproductive implications.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is one of the most prevalent endocrine disorders affecting women of reproductive age.1,2 This syndrome is characterized by heterogeneous clinical manifestations, including menstrual irregularities, hyperandrogenism, and polycystic ovaries.3–5 It is a complex condition with multifaceted metabolic and reproductive implications, leading to a higher risk of infertility, obesity, insulin resistance, and cardiometabolic complications. 6 Among women with PCOS, those who are overweight or obese are particularly susceptible to exacerbated metabolic derangements and an increased risk of developing type 2 diabetes mellitus, dyslipidemia, and cardiovascular disease.7,8
Insulin resistance is a central pathophysiologic feature of PCOS, contributing to the metabolic disturbances observed in affected individuals.9–11 The dysregulation of insulin action and compensatory hyperinsulinemia have been linked to abnormal glucose metabolism, dyslipidemia, and the adverse cardiovascular risk profile commonly seen in PCOS.12,13 Moreover, the presence of insulin resistance in PCOS is often associated with a higher prevalence of obesity, particularly central adiposity, further exacerbating the metabolic burden in these individuals.14–16
Exercise training is a cornerstone in the management of PCOS, aiming to alleviate the metabolic abnormalities and improve reproductive and cardiometabolic health in affected individuals.17,18 High-Intensity Interval Training (HIIT) has gained attention as a time-efficient and effective exercise modality with the potential to enhance metabolic health and physical fitness.19,20 HIIT involves short bursts of vigorous exercise interspersed with brief periods of low-intensity activity or rest, leading to improvements in cardiovascular fitness, insulin sensitivity, and body composition.21,22
While the benefits of regular physical activity in PCOS are well-recognized, the specific impact of HIIT on insulin sensitivity, body composition, cardiovascular parameters, and quality of life in women with overweight PCOS remains an area of active investigation. Previous studies have explored the effects of HIIT in various populations, demonstrating its potential to enhance insulin sensitivity, reduce visceral adiposity, and improve cardiovascular function.23–25 However, the application of HIIT in the context of PCOS, particularly in overweight individuals, necessitates further exploration given the unique metabolic and endocrine perturbations associated with this condition.
In light of the current gaps in the literature and the growing interest in personalized exercise prescriptions for PCOS, the findings of this study may contribute to a deeper understanding of the role of HIIT in optimizing health outcomes in women with overweight PCOS. Furthermore, the implications of this research may extend to the development of tailored exercise recommendations and the refinement of clinical guidelines for the comprehensive care of individuals with PCOS.
The aim of this study was to investigate the impact of HIIT on insulin sensitivity, body composition, metabolic parameters, and quality of life in women with overweight PCOS.
Materials and methods
Study population
This study retrospectively analyzed the clinical data of 107 female patients with overweight PCOS admitted to our hospital from January 2023 to December 2023, who were divided into two groups based on the training method: the Regular Interval Training Group (n = 54) and the HIIT Group (n = 53).
Inclusion and exclusion criteria
Inclusion criteria: Met the diagnostic criteria for PCOS as per the “Chinese Diagnosis and Treatment Guidelines for PCOS “ (12); Met the overweight criteria according to the “Expert Consensus on Body Management Pathway and Process for Overweight/Obese Infertile Patients in China,” i.e., BMI ≥ 24 kg/m2 26 ; Women of childbearing age between 16 and 40 years old; Good communication and literacy skills; Informed consent from both family members and patients was obtained for their participation in this study.
Exclusion criteria included: Coexisting gynecological disorders; Use of hormonal or similar drug treatments; Coexistence of severe conditions such as heart, brain, or kidney diseases; Mental abnormalities; Refusal to cooperate with the study; Presence of severe systemic diseases, sexually transmitted diseases, or urinary system infections; Presence of gynecological neoplasms or malignancies (such as ovarian tumors, endometrial tumors, cervical cancer); Presence of other metabolic disorders (diabetes, Cushing's syndrome, thyroid diseases, hyperprolactinemia, etc.).
Treatment methods
The control group received routine care including respiratory training, physical exercises (lower and upper limb abduction, lifting, and flexion), as well as moderate-intensity exercises such as stair climbing (5 min each time, with 1 to 3 min rest in between) and jogging (10 to 15 min), 3 to 5 times a day, 3 to 5 days per week, continuously for 2 months.
The exercise group received the same routine care as the control group, along with HIIT. HIIT Running Exercise Protocol: The high-intensity exercise involves 15 to 30 s of maximal sprinting followed by a 15-s rest, repeated for a total of 5 to 10 min. This is interspersed with 4 min of rest, constituting one complete exercise session. This protocol is administered 3–5 times per day, 3–5 days per week, continuously for 2 months.
Measurement methods
Baseline data
The baseline data comprised age, BMI, smoking history, alcohol intake, hypertension, diabetes, hyperlipidemia, fasting glucose, and total testosterone levels.
Blood glucose level measurement
Peripheral venous blood samples of 2 mL each were collected from both groups while fasting and 1 mL after a 2 h postprandial period. Fasting blood glucose (FBG) and 2 h postprandial blood glucose levels were determined using the fully automatic biochemical analyzer (COBAS8000, Roche, Germany), while fasting insulin (FINS) was measured using the fully automated chemiluminescence analyzer (1601, Roche, Germany) and matching reagent kits. The Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) index was calculated using the formula: (FINS × FBG)/22.5, with a normal range of 0.5–1.4.
Body fat level measurement
The participants’ waist and hip circumferences were measured using a tape measure, and their body fat percentage (BF%) was assessed using a body composition analyzer (InBody770, InBody, South Korea) with participants required to be lightly dressed, barefoot, and having emptied their bladder and bowels during the test.
Blood lipid level measurement
Before testing, participants fasted for 12 h, and 3 ml of venous blood from the mid-elbow was collected in the early morning on an empty stomach, and plasma was obtained following centrifugation using heparin anticoagulant. Enzymatic colorimetric methods were then used to determine the levels of total cholesterol (TC), triglycerides (TG), low-density lipoprotein-cholesterol (LDL-c), and high-density lipoprotein-cholesterol (HDL-c).
Quality of life assessment
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) was used to evaluate patients’ quality of life, including five functional domains (Physical Functioning/PF, Role Functioning/RF, Emotional Functioning/EF, Cognitive Functioning/CF, and Social Functioning/SF). Higher scores indicated a better quality of life, while lower scores suggested the presence of more symptoms or issues.
Statistical analysis
IBM Statistic Package for Social Science (SPSS) 26.0 (version 15.0.3; NCSS LLC, Kaysville, USA) was employed for the analysis. Continuous variables were presented as mean ± standard deviation and differences between the Regular Interval Training Group and the HIIT Group were compared using the t-test. Categorical variables were described as n (%) and differences between the two groups were assessed using the chi-square test.
Results
Baseline data and demographic characteristics
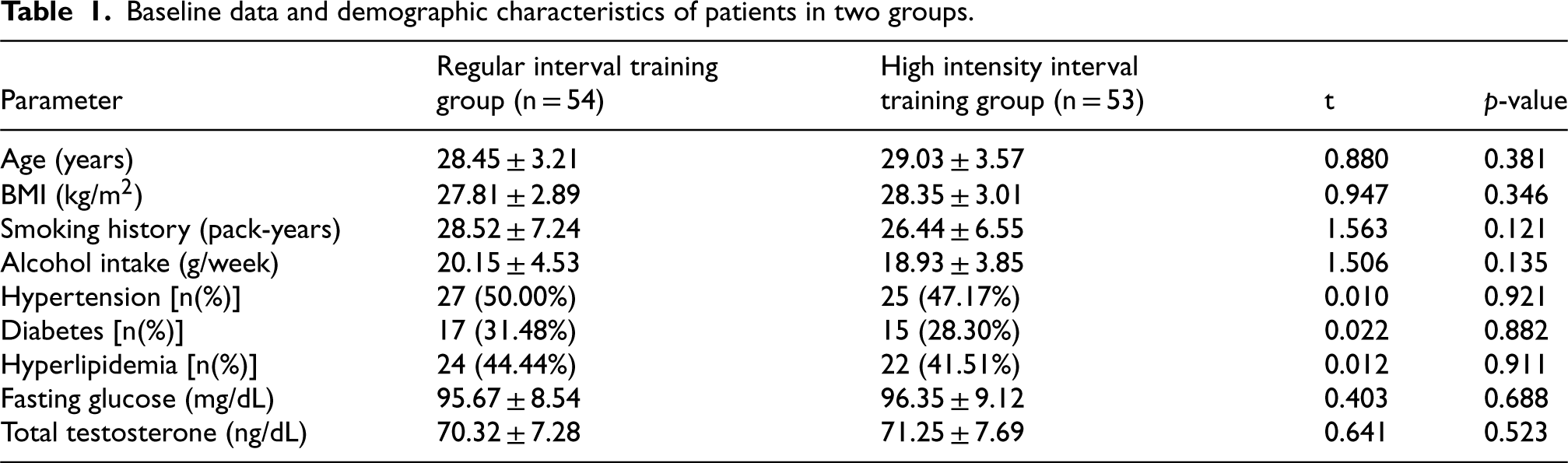
The baseline characteristics of the participants in the Regular Interval Training Group (n = 54) and the HIIT Group (n = 53) were comparable, with no statistically significant differences observed (Table 1). The mean age was 28.45 ± 3.21 years and 29.03 ± 3.57 years in the Regular Interval Training and HIIT groups, respectively (t = 0.880, p = 0.381). Similarly, there were no significant differences in BMI, smoking history, alcohol intake, prevalence of hypertension, diabetes, hyperlipidemia, fasting glucose levels, and total testosterone levels between the two groups. These findings suggest that the baseline characteristics were well-balanced between the two intervention groups, indicating that any subsequent differences in outcomes could be attributed to the HIIT intervention rather than baseline demographic variations.
Baseline data and demographic characteristics of patients in two groups.
Baseline data and demographic characteristics of patients in two groups.
The comparison of changes in insulin sensitivity and glucose metabolism between the Regular Interval Training Group and the HIIT Group in women with overweight PCOS revealed notable differences. The HIIT Group demonstrated significantly improved insulin sensitivity, as evidenced by the Matsuda index (6.23 ± 0.85) compared to the Regular Interval Training Group (5.15 ± 0.72) (t = 7.109, p < 0.001). Moreover, the HIIT Group exhibited a significant reduction in fasting glucose levels (87.41 ± 7.03) compared to the Regular Interval Training Group (90.25 ± 7.51) (t = 2.017, p = 0.046), along with a lower HOMA-IR index (2.15 ± 0.35) compared to the Regular Interval Training Group (2.82 ± 0.45) (t = 8.535, p < 0.001). However, there were no significant differences in 2 h glucose levels and total cholesterol levels between the two groups. These findings suggest that HIIT may lead to improved insulin sensitivity and fasting glucose levels in women with overweight PCOS compared to Regular Interval Training, highlighting the benefits of this approach in managing the condition (Table 2).
Comparison of changes in insulin sensitivity and glucose metabolism of patients between two groups.

Comparison of changes in insulin sensitivity and glucose metabolism of patients between two groups.
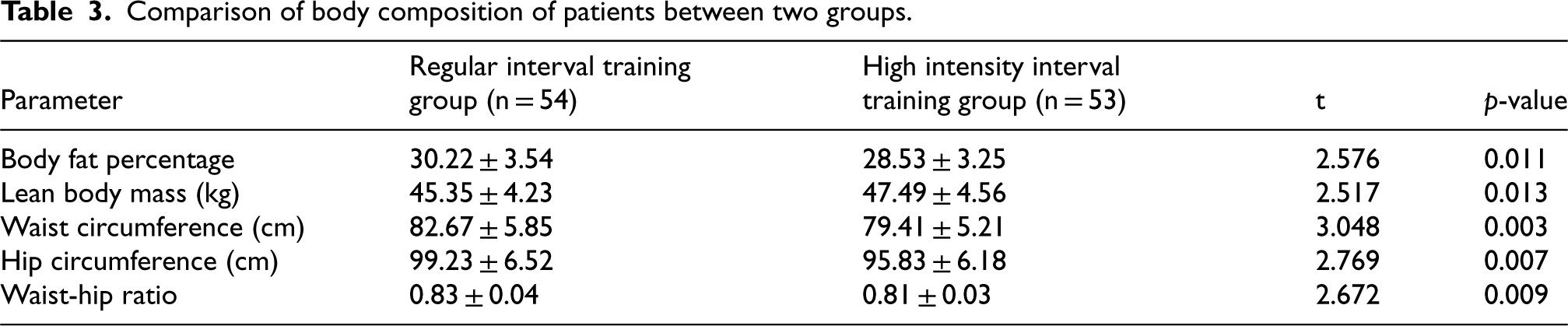
The comparison of body composition between the Regular Interval Training Group and the HIIT Group in women with overweight PCOS revealed significant differences (Table 3). The HIIT Group demonstrated a lower body fat percentage (28.53 ± 3.25) compared to the Regular Interval Training Group (30.22 ± 3.54) (t = 2.576, p = 0.011), as well as a higher lean body mass (47.49 ± 4.56) compared to the Regular Interval Training Group (45.35 ± 4.23) (t = 2.517, p = 0.013). Furthermore, the HIIT Group exhibited reduced waist circumference (79.41 ± 5.21) compared to the Regular Interval Training Group (82.67 ± 5.85) (t = 3.048, p = 0.003) and decreased hip circumference (95.83 ± 6.18) compared to the Regular Interval Training Group (99.23 ± 6.52) (t = 2.769, p = 0.007). Additionally, the waist-hip ratio was lower in the HIIT Group (0.81 ± 0.03) compared to the Regular Interval Training Group (0.83 ± 0.04) (t = 2.672, p = 0.009). These findings suggest that HIIT may lead to favorable changes in body composition, including reduced body fat percentage, decreased waist and hip circumferences, and improved waist-hip ratio, highlighting its benefits in managing body composition in women with overweight PCOS.
Comparison of body composition of patients between two groups.
Comparison of body composition of patients between two groups.
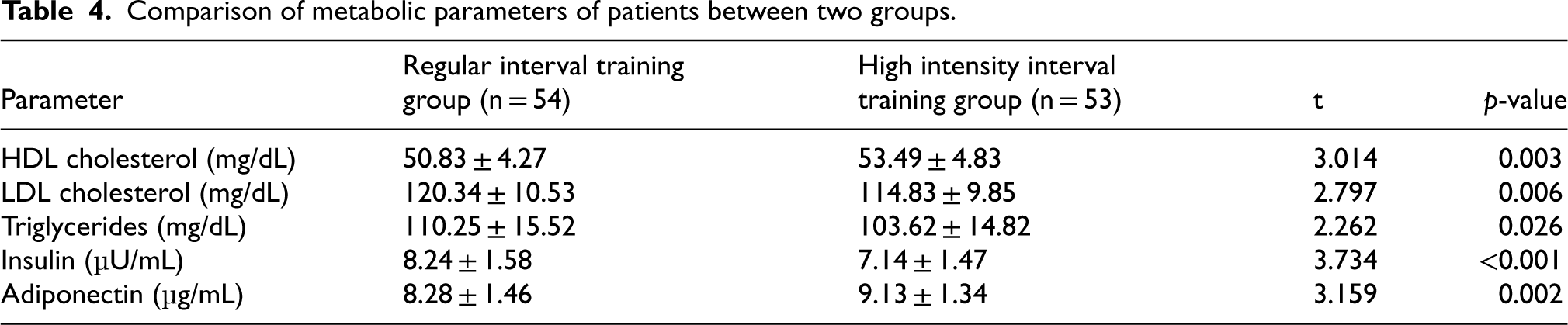
The comparison of metabolic parameters between the Regular Interval Training Group and the HIIT Group in women with overweight PCOS revealed notable differences (Table 4). The HIIT Group demonstrated higher levels of HDL cholesterol (53.49 ± 4.83) compared to the Regular Interval Training Group (50.83 ± 4.27) (t = 3.014, p = 0.003), lower levels of LDL cholesterol (114.83 ± 9.85) compared to the Regular Interval Training Group (120.34 ± 10.53) (t = 2.797, p = 0.006), reduced triglyceride levels (103.62 ± 14.82) compared to the Regular Interval Training Group (110.25 ± 15.52) (t = 2.262, p = 0.026), lower insulin levels (7.14 ± 1.47) compared to the Regular Interval Training Group (8.24 ± 1.58) (t = 3.734, p < 0.001), and higher adiponectin levels (9.13 ± 1.34) compared to the Regular Interval Training Group (8.28 ± 1.46) (t = 3.159, p = 0.002). These findings indicate that HIIT may lead to favorable changes in metabolic parameters, including improved lipid profile, reduced insulin levels, and elevated adiponectin levels, highlighting its benefits in enhancing metabolic health in women with overweight PCOS.
Comparison of metabolic parameters of patients between two groups.
Comparison of metabolic parameters of patients between two groups.
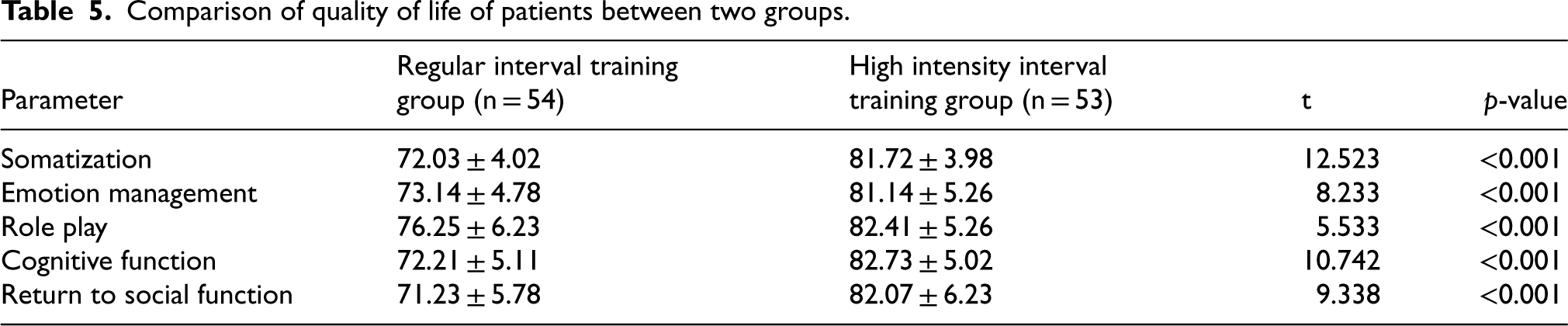
The comparison of quality of life between the Regular Interval Training Group and the HIIT Group in women with overweight PCOS revealed substantial differences. The HIIT Group demonstrated significantly improved scores across all domains including somatization (81.72 ± 3.98 vs 72.03 ± 4.02; t = 12.523, p < 0.001), emotion management (81.14 ± 5.26 vs 73.14 ± 4.78; t = 8.233, p < 0.001), role play (82.41 ± 5.26 vs 76.25 ± 6.23; t = 5.533, p < 0.001), cognitive function (82.73 ± 5.02 vs 72.21 ± 5.11; t = 10.742, p < 0.001), and return to social function (82.07 ± 6.23 vs 71.23 ± 5.78; t = 9.338, p < 0.001). These findings suggest that HIIT may lead to significant improvements in quality of life across various domains.
Discussion
The impact of HIIT on insulin sensitivity and quality of life in women with overweight PCOS has been a subject of considerable interest and debate in the field of reproductive health and endocrinology. Santos et al. also confirmed the positive impact of HIIT on the psychological well-being of women. 27 In this study, we aimed to assess the specific effects of HIIT on varous metabolic and clinical parameters in women with overweight PCOS, shedding light on the potential benefits of this exercise modality in managing the complex manifestations of the syndrome. Our findings demonstrate significant improvements in insulin sensitivity, glucose metabolism, body composition, metabolic profile, and quality of life in women with overweight PCOS following a HIIT intervention, compared to regular interval training. These results offer compelling insights into the potential of personalized exercise prescriptions, such as HIIT, in optimizing health outcomes for individuals with PCOS.
HIIT has garnered attention not only for its benefits in women with PCOS but also for its effectiveness in other patient populations and healthy individuals. For professional athletes, HIIT has been shown to enhance aerobic and anaerobic capacity, leading to improved performance and recovery times.28,29 The high-intensity nature of HIIT can increase VO2 max, muscle power, and endurance, making it a popular training modality among elite athletes. 30 Healthy individuals also benefit from HIIT due to its time efficiency and versatility. Studies have demonstrated that HIIT can improve cardiovascular fitness, increase insulin sensitivity, and promote weight loss.31,32 These benefits are particularly relevant for individuals looking to maintain optimal health and fitness without dedicating extensive time to exercise. However, it is essential to consider the potential disadvantages and risks associated with HIIT. The high intensity of the workouts can increase the risk of injury, especially if proper form and technique are not maintained. 33 Additionally, HIIT may not be suitable for individuals with certain medical conditions, such as severe cardiovascular disease, unless carefully monitored by healthcare professionals. 34
Our study revealed that the HIIT Group demonstrated significantly improved insulin sensitivity, as evidenced by higher Matsuda index and lower HOMA-IR index, along with reduced fasting glucose levels compared to the Regular Interval Training Group. These findings underscore the potential of HIIT in ameliorating the insulin resistance characteristic of PCOS, aligning with previous research suggesting the benefits of HIIT in enhancing insulin sensitivity and glucose metabolism. 35
Furthermore, our study demonstrated that HIIT led to significant improvements in body composition, as evidenced by reduced body fat percentage, decreased waist and hip circumferences, and improved waist-hip ratio in women with overweight PCOS. These findings are particularly noteworthy given the strong association between obesity and PCOS, with overweight or obese women with PCOS being particularly susceptible to exacerbated metabolic derangements and an increased risk of developing type 2 diabetes mellitus, and dyslipidemia. The ability of HIIT to induce favorable changes in body composition may have profound implications for the management of PCOS, addressing not only the aesthetic concerns of affected individuals but also the broader metabolic and reproductive implications associated with excessive adiposity. These results align with previous evidence suggesting that HIIT is effective in reducing visceral adiposity and improving body composition in various populations, underscoring its potential utility in addressing the unique metabolic burden associated with PCOS. 36
Metabolic parameters also showed marked improvements following the HIIT intervention, with the HIIT Group demonstrating a favorable lipid profile, reduced insulin levels, and elevated adiponectin levels compared to the Regular Interval Training Group. These findings are noteworthy in the context of PCOS, where individuals are at an increased risk of dyslipidemia, insulin resistance, and metabolic disturbances. The observed improvements in these metabolic parameters suggest the potential of HIIT in addressing the multifaceted metabolic implications of PCOS and its associated complications (Table 5).
Comparison of quality of life of patients between two groups.
Comparison of quality of life of patients between two groups.
Quality of life is a critical aspect of the comprehensive care of individuals with PCOS, given the multifaceted impact of the syndrome on physical, emotional, and social well-being. Our study demonstrated significant improvements in various domains of quality of life in the HIIT Group, including somatization, emotion management, role play, cognitive function, and return to social function. These findings are particularly relevant considering the significant psychological and emotional burden experienced by individuals with PCOS, encompassing aspects such as body image concerns, emotional distress, and impaired quality of life. The observed improvements in quality of life highlight the broader psychosocial benefits of HIIT in addressing the holistic well-being of women with PCOS, emphasizing the need for comprehensive interventions that extend beyond the traditional focus on metabolic and reproductive aspects.
It is important to acknowledge the limitations of this study. Firstly, the retrospective design limits our ability to infer causality and necessitates further prospective, longitudinal investigations to validate the long-term benefits of HIIT in women with overweight PCOS. Secondly, the sample size, although adequate for statistical analysis, may not fully represent the broader population of women with PCOS. Thirdly, the lack of blinding in the exercise protocols might introduce bias, and the absence of a placebo or control group makes it challenging to isolate the specific effects of HIIT. Finally, adherence to the exercise regimen was self-reported, which introduces potential reporting biases.
While the present study provides compelling evidence for the benefits of HIIT in women with overweight PCOS, several avenues for future research remain. First, larger, randomized controlled trials (RCTs) are needed to confirm the current findings and establish the long-term efficacy and safety of HIIT in this population. Additionally, future studies should explore the optimal frequency, intensity, and duration of HIIT sessions to tailor interventions more precisely to individual needs. Investigating the underlying mechanisms through which HIIT improves insulin sensitivity, body composition, and metabolic profiles could provide valuable insights into the physiological pathways involved. Lastly, integrating qualitative assessments of patient experiences and preferences would help in designing more patient-centered and sustainable exercise programs.
Overall, the findings of this study contribute to a deeper understanding of the role of HIIT in optimizing health outcomes in women with overweight PCOS. The observed improvements in insulin sensitivity, body composition, metabolic profile, and quality of life underscore the potential of personalized exercise prescriptions, such as HIIT, in mitigating the multifaceted implications of PCOS and its associated metabolic and reproductive perturbations. These findings hold clinical significance in shaping tailored exercise recommendations and refining clinical guidelines for the comprehensive care of individuals with PCOS, emphasizing the need for individualized, multidimensional interventions that address the diverse manifestations of this complex syndrome.
In conclusion, the findings of this study underscore the potential of HIIT in optimizing health outcomes in women with overweight PCOS, offering compelling insights into the multifaceted benefits of this exercise modality. The observed improvements in insulin sensitivity, body composition, metabolic profile, and quality of life highlight the promising role of HIIT in addressing the complex manifestations of PCOS and its associated metabolic and reproductive implications. These findings provide valuable evidence for the development of tailored exercise recommendations and the refinement of clinical guidelines for the comprehensive care of individuals with PCOS, emphasizing the need for personalized, multidimensional interventions that address the diverse facets of this prevalent endocrine disorder.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.