
Abstract
Objective
To explore the predictive value of the modified NUTrition Risk in the Critically ill (mNUTRIC) for patients with sepsis and acute respiratory distress syndrome (ARDS) developing into chronic critical illness (CCI).
Background
Sepsis is an important risk factor for Acute respiratory distress syndrome (ARDS), and sepsis induced ARDS accounts for 32% of patients. Patients with this subtype of ARDS have a worse prognosis than those with sepsis alone or ARDS, usually facing higher mortality rates and lower success rates of extubation, and have received more attention in clinical practice.
Methods
A retrospective observational study was conducted on 118 patients admitted to the Intensive Care Unit (ICU) of Yiwu Central Hospital from January 2020 to May 2022. Patients were categorized into two groups: CCI and rapid recovery (RAP), based on the occurrence of CCI. Age, gender, white blood cell count, C-reactive protein, albumin, serum creatinine, sequential organ failure assessment (SOFA), acute physiology and chronic health evaluation II (APACHE II), mNUTRIC score, ICU length of stay, mechanical ventilation duration, and continuous renal replacement therapy (CRRT) were compared between the two groups. The association between mNUTRIC and CCI in patients with sepsis complicated by ARDS was further examined using three models and multivariate logistic regression.The receiver operating characteristic (ROC) curve was utilized to analyze the predictive values of mNUTRIC score, SOFA score, and APACHE II score for predicting the occurrence of CCI in patients with sepsis complicated by ARDS.
Results
The age, mNUTRIC score, SOFA score, APACHE II score, ICU length of stay, mechanical ventilation duration, and CRRT ratio were significantly higher in the CCI group compared to the RAP group (all P < 0.05). Conversely, there were no statistically significant differences in white blood cell count, C-reactive protein, and albumin levels between the two groups (all P > 0.05). Multivariate logistic regression analysis identified the mNUTRIC score as an independent risk factor for CCI in patients with sepsis complicated by ARDS. The constructed models showed that the mNUTRIC score remained significant, while the SOFA score and APACHE II score did not.The area under the ROC curve analysis demonstrated that the mNUTRIC score had the highest AUC of 0.880, 95% Confidence Interval (CI): 0.808–0.933. The AUC for the SOFA score was 0.864, and for the APACHE II score was 0.825, all of which were statistically significant.
Conclusions
The mNUTRIC score is valuable in predicting the progression of sepsis combined with ARDS to CCI, and may even be superior to the SOFA score and APACHE II score.
Introduction
Acute respiratory distress syndrome (ARDS) is an acute diffuse inflammatory lung injury characterized by damage to alveolar epithelial cells and pulmonary capillary endothelial cells. It is a clinical syndrome of acute hypoxic respiratory failure. 1 In recent years, scholars have continuously proposed that ARDS can be divided into different phenotypes. Sepsis is an important risk factor for ARDS, and sepsis induced ARDS accounts for 32% of patients. Patients with this subtype of ARDS have a worse prognosis than those with sepsis alone or ARDS, usually facing higher mortality rates and lower success rates of extubation, and have received more attention in clinical practice.2,3 Despite the continuous advancement of respiratory support technology and ARDS treatment concepts in recent years, such as prone position ventilation, lung protection ventilation strategies, and the application of extracorporeal membrane lung technology, more patients have recovered from multiple organ failure (MOF) and avoided early death. However, although these patients have survived the acute phase, they still have to rely on mechanical ventilation and other organ support therapies for a long time, and continue to receive organ function support and intensive care treatment. Clinically, these patients are referred to as chronic critical illness (CCI). 4 CCI patients ultimately experience a decline in their quality of life, a significant increase in medical expenses, a noticeable extension of hospitalization time, and a significant increase in mortality rates, which have a serious impact on society, families, and the patients themselves.5–8 Therefore, early assessment of the progression of sepsis combined with ARDS to CCI has become more urgent.
At present, in clinical treatment, critical care scoring such as Sequential Organ Failure Assessment (SOFA) score is often used to reflect the comprehensive situation of circulation, respiration, blood, kidney, nerve function, etc. in critically ill patients. They are used for the evaluation and prognosis of critically ill patients. 9 The APACH II score is also a critical assessment tool, which includes age, whether emergency surgery has been performed, respiratory system, circulatory system (including vasoactive drug dosage), liver, kidney and other organs. It is used to evaluate the condition and prognosis. The above two scoring systems are to some extent related to the slow progression of critical illness in critically ill patients. 10
The modified NUTrition Risk in the Critically ill (mNUTRIC) score includes the following six items: age, number of comorbidities, length of stay before Intensive Care Unit (ICU) admission, acute physiology and chronic health evaluation II (APACHE II), SOFA. They are used clinically to assess nutritional risk in critically ill patients, reflecting some prognostic indicators related to an inflammatory reaction, organ function damage, etc. Therefore, the mNUTRIC score may be nearly linked to the development and prognosis of severe illness, 11 which can predict the possibility of CCI.
Therefore, 118 septic patients with complicated with ARDS in the Department of Critical Care Medicine of Yiwu Central Hospital from January 1, 2020, to May 31, 2022, were selected as the research objects. The general situation, mNUTRIC score, APACHE II score, SOFA score, ICU hospitalization time, and mechanical ventilation application time of the participants were aggregated and counted so as to explore the value of mNUTRIC score in anticipating the occurrence of slow and severe diseases in septic patients complicated with ARDS. Then the mNUTRIC score was compared with APACH II score and SOFA score.
Data and methods
General data
As a retrospective observational study, this study took 118 patients with sepsis complicated with ARDS admitted to the Department of Critical Care Medicine of Yiwu Central Hospital from January 2020 to May 2022 as the research subjects.
Inclusion criteria for sepsis complicated with ARDS: Hospitalized Patients meeting Berlin diagnostic criteria of sepsis 12 and ARDS 13 ; the oxygenation index (PaO2/FiO2) ranged from 150 to 200 mmHg (1 mmHg = 0.133 kPa); age ≥ 18 years old; exclusion criteria: patients who were discharged automatically or gave up treatment, ICU hospitalization time ≤24 h, patients with brain death, terminal disease or advanced tumor, and pregnant patients. CCI diagnostic criteria 14 : ICU stay of ≥ 8 days, and had at least one of the following conditions: (1) continuous mechanical ventilation for more than 96 h; (2) Tracheotomy; (3) Sepsis or other serious infections; (4) Severe trauma; (5) MOF, ischemic stroke, cerebral hemorrhage, or traumatic brain injury. According to the presence or absence of CCI, patients were divided into CCI group (59 patients) and rapid recovery (RAP) group (59 patients). This study complies with medical ethics standards and has been approved by the hospital ethics committee. Approval number: K2023-IRB-059.
Data collection
The following data of the enrolled patients were collected: age, gender, white blood cell count, neutrophil count, lymphocyte count, platelet count, lymphocyte count, albumin, C-reactive protein (CRP), alanine aminotransferase (ALT), blood creatinine, mNUTRIC score within 24 h of onset, APACHE II score and SOFA score within 24 h of admission, ICU stay days, mechanical ventilation time, continuous renal replacement therapy (CRRT), etc.
Statistical methods
SPSS 27.0 software was used for data processing and analysis. When the quantitative data conformed to a normal distribution, it was expressed as mean ± standard deviation (x ± s). Independent sample t-test was used for comparison between two groups. When it conforms to a skewed distribution, it was represented by the median (quartiles) [M (Q1, Q3)]. A non-parametric Mann-Whitney U test was used for comparison between two groups. The count data were analyzed using chi-square test. Multiple logistic regression was used to explore the risk factors for CCI in sepsis patients with ARDS. Receiver operating characteristic (ROC) curve was plotted using R 4.2.2.
Results
Comparison of clinical data between CCI group and RAP group
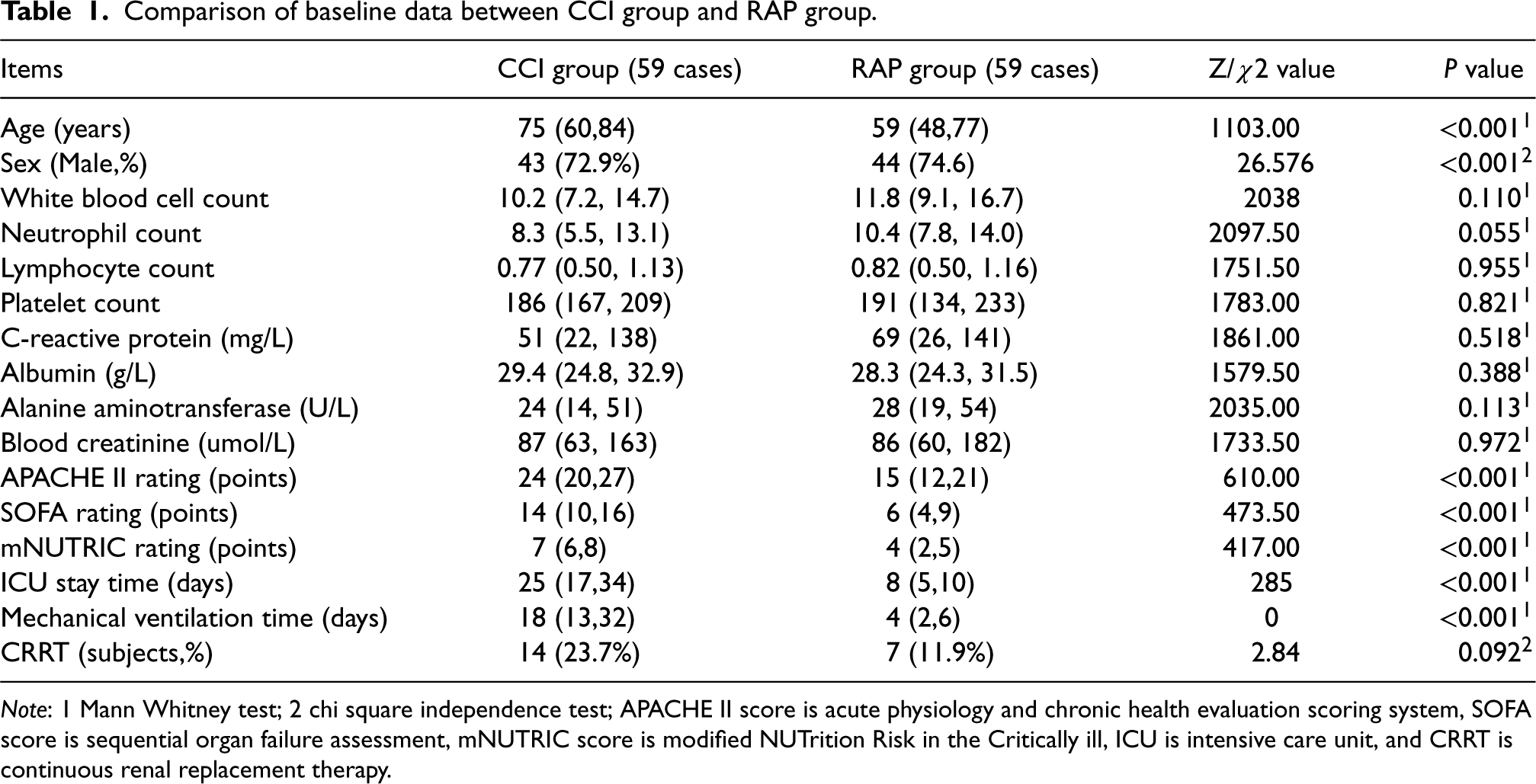
This study included a total of 118 patients, including 59 in the RAP group and 59 in the CCI group. The age, mNUTRIC score, APACHE II score, SOFA score, ICU stay time, and mechanical ventilation application time of patients in the CCI group were higher than those in the RAP group, and the differences were statistically significant (P values were <0.001, <0.001, <0.001, <0.001, <0.001, <0.001, <0.001, <0.001, <0.001). The proportion of males was lower than that in the RAP group, and the differences were statistically significant (P < 0.001). There was no statistical difference in the proportion of white blood cell count, neutrophil count, lymphocyte count, platelet count, CRP, albumin, ALT, blood creatinine, and CRRT between the two groups (P values were 0.110, 0.055, 0.955, 0.821, 0.518, 0.388, 0.113, 0.972, 0.092, respectively). (See Table 1).
Comparison of baseline data between CCI group and RAP group.
Comparison of baseline data between CCI group and RAP group.
Note: 1 Mann Whitney test; 2 chi square independence test; APACHE II score is acute physiology and chronic health evaluation scoring system, SOFA score is sequential organ failure assessment, mNUTRIC score is modified NUTrition Risk in the Critically ill, ICU is intensive care unit, and CRRT is continuous renal replacement therapy.
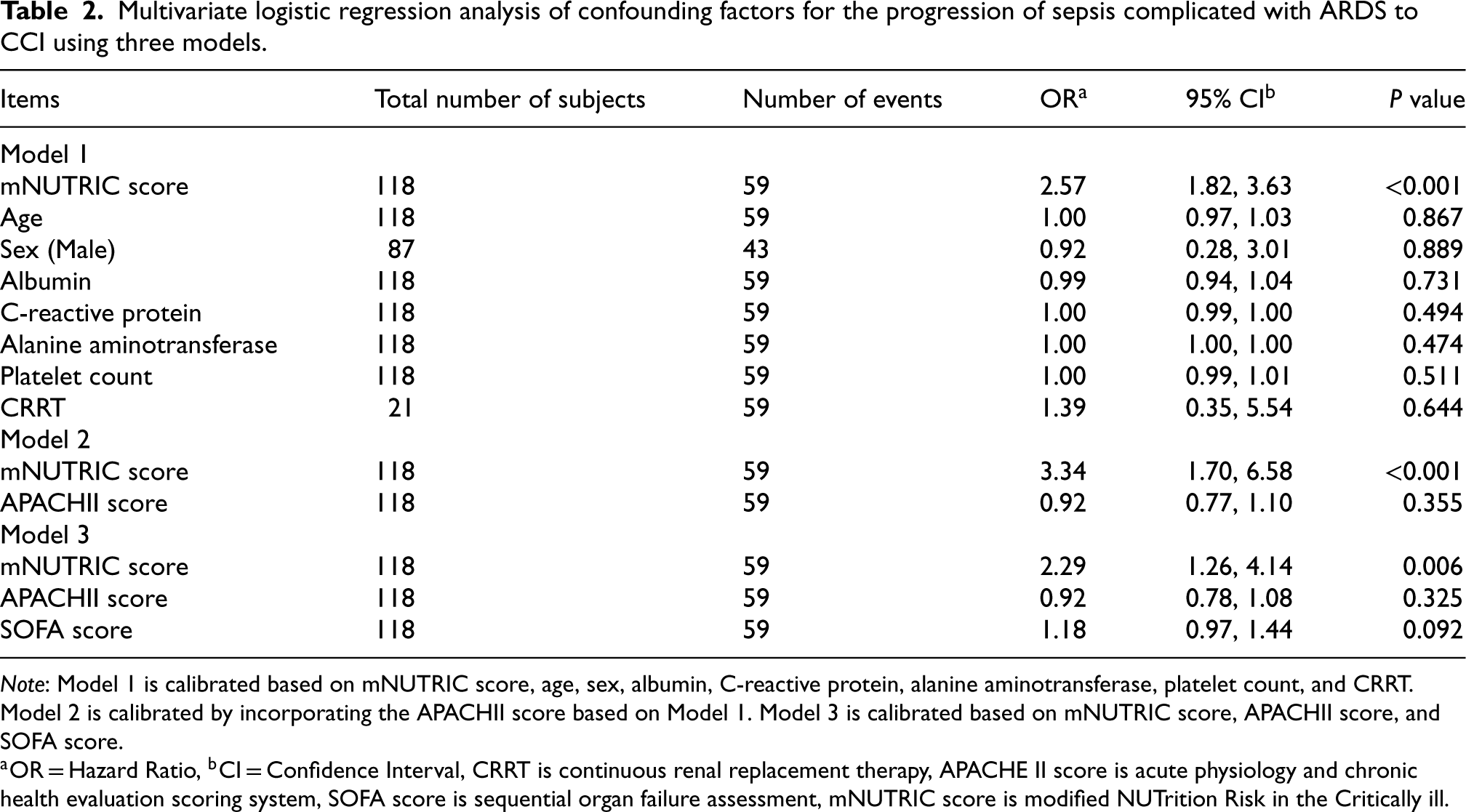
Through multiple regression model analysis, Model 1 included variables such as mNUTRIC score, age, gender, albumin, C-reactive protein, alanine aminotransferase, platelet count, and CRRT. The results showed that mNUTRIC score was an independent risk factor for CCI in sepsis patients with ARDS, with an OR of 2.57 and a 95% CI of 1.82–3.63. However, there were no significant differences in age, gender, albumin, C-reactive protein, and the use of CRRT statistics, with P > 0.05. Model 2 further adjusted the APACH II score based on Model 1, and the mNUTRIC score was identified as a risk factor for CCI with an OR of 3.34 and a 95% CI of 1.70–6.58. However, Model 3 only included the analysis of mNUTRIC score, SOSFA score, and APACHII score. mNUTRIC score remained a risk factor for CCI with an OR of 2.29 and a 95% CI of 1.26–4.14, while APACHII score and mNUTRIC score did not reach statistical significance, as shown in Table 2.
Multivariate logistic regression analysis of confounding factors for the progression of sepsis complicated with ARDS to CCI using three models.
Multivariate logistic regression analysis of confounding factors for the progression of sepsis complicated with ARDS to CCI using three models.
Note: Model 1 is calibrated based on mNUTRIC score, age, sex, albumin, C-reactive protein, alanine aminotransferase, platelet count, and CRRT. Model 2 is calibrated by incorporating the APACHII score based on Model 1. Model 3 is calibrated based on mNUTRIC score, APACHII score, and SOFA score.
aOR = Hazard Ratio, bCI = Confidence Interval, CRRT is continuous renal replacement therapy, APACHE II score is acute physiology and chronic health evaluation scoring system, SOFA score is sequential organ failure assessment, mNUTRIC score is modified NUTrition Risk in the Critically ill.
The ROC analysis results showed that the area under the AUC curve of mNUTRIC was the largest, AUC = 0.880, 95% Confidence Interval (CI): 0.808–0.933. The optimal critical value for predicting CCI occurrence is 6 points, with a sensitivity of 78% and a specificity of 93%. The AUC of SOFA score is 0.864, 95% CI: 0.789–0.920. The optimal critical value for predicting CCI is 12 points, with a sensitivity of 71% and a specificity of 90%. The AUC of APACHII score is 0.825, with a 95% CI: 0.744–0.889. The optimal critical value for predicting CCI is 22 points, with a sensitivity of 64% and a specificity of 83%, as shown in Table 3 and Figure 1.

Predictive value of age, NUTRIC score, APACHE II score and SOFA score for CCI in patients with sepsis complicated with ARDS.
ROC Summary of mNUTRIC Score, APACHE II score, and SOFA score for CCI progression in sepsis with ARDS.

Sepsis combined with ARDS is one of the subtypes of ARDS, which is more complex than other subtypes, with longer ICU stay and mechanical ventilation time, and higher mortality rates at 28 and 60 days. The cause of its onset may be that the inflammatory cells in septic patients produce a large number of inflammatory factors and cytokines. The inflammatory reaction involving inflammatory factors destroys the alveolar capillary vascular barrier, and the permeability of hair vessels increases, resulting in capillary leakage, which leads to the leakage of protein-rich fluid into alveolar cavity, and finally makes septic patients complicated with ARDS. 15 With the development of critical care medicine, the updating of ARDS treatment concepts and the progress of medical technology, many individuals with sepsis combined with ARDS can survive death, but survivors often need long-term monitoring and persistent organ dysfunction and stay in ICU. 16 An epidemiological survey on CCI in the United States found that about 63.7% of septic patients developed into CCI. 14 CCI is the product of the technological progress of intensive care. It originates from critical illness and is different from critical illness. Patients with CCI need longer hospital stays, which is consistent with the results of this study. Patients with CCI need comprehensive support treatment, including mechanical ventilation, nutritional metabolism treatment, rehabilitation treatment and other organ support measures, 17 which makes the mortality rate and medical expenses of patients increase significantly, and increases the burden on individuals, families and society.7,16
In order to identify CCI early, there were multiple studies: A Marchioni et al. analyzed 100 patients with acute respiratory failure requiring mechanical ventilation, and multivariate analysis found that high APACH II scores and septic shock were risk factors for CCI. 18 Studies by Sérgio H Loss et al. have shown that high APACHII scores and high SOFA scores are factors contributing to the occurrence of CCI. 19
This study showed that patients in the CCI group were older and had higher mNUTRIC score, APACHE II score, and SOFA score than those in the RAP group. This indicated that the more severe the organ dysfunction, the more difficult it is for patients to recover, and they are more likely to develop chronic complications and even progress to CCI. At the same time, the application time of mechanical ventilation in the CCI group was longer, which was more likely to lead to ventilator dependence. The study by Wang Linling et al. showed that the mNUTRIC score, APACHE II score, and SOFA score were higher in elderly sepsis patients who progressed to CCI compared to the RAP group. 16 The patients in the above study were elderly sepsis patients, indicating that early monitoring of mNUTRIC can help detect the tendency of sepsis combined with ARDS to progress to CCI. Through Model 1 calibration, it was found that there was no significant difference in initial biochemical indicators between the two groups of patients in the early stage, such as CRP levels, liver and kidney function, albumin, etc. Monitoring these non-specific indicators is of little significance for early assessment of CCI.
After adjusting for confounding factors based on mNUTRIC score, it was found that mNUTRIC score can effectively distinguish the possibility of sepsis complicated with ARDS progressing to CCI. Model 1: OR 2.57, 95% CI: 1.82–3.63, Model 2: OR 3.34, 95% CI: 1.70–6.58, indicating that mNUTRIC score is an important risk factor for evaluating and predicting the occurrence of CCI. SOFA score and APACH II score have value in predicting the occurrence of CCI. However, Model 3 compared the three indicators and found that mNUTRIC still has important value, OR 2.29, 95%CI: 1.26–4.14. There were no statistical significance in SOFA score and APACH II score, with OR 1.18 and 95% CI: 0.97–1.44, OR 0.92 and 95%CI: 0.78–1.08, respectively.
It is crucial to use individualized prevention and treatment strategies early for patients with mNUTRIC scores ≥ 6, to improve the incidence and prognosis of CCI. Comparing the ROC curves, the optimal cutoff value for mNUTRIC prediction of CCI in sepsis complicated with ARDS patients was 6, with a sensitivity of 0.79 and a specificity of 0.93 (95% CI: 0.808–0.933). At the same time, APACHII and SOFA scores also have certain predictive value, but the area under the mNUTRIC curve was larger and the specificity was higher, which once again proved the important clinical significance of mNUTRIC score in predicting CCI in sepsis complicated with ARDS patients. However, this study also has certain limitations: (1) It used a single center and had a relatively small sample size. The study focused on sepsis patients with ARDS and cannot represent other sepsis or ARDS patients. Further research will be conducted in the future. (2) mNUTRIC and other indicators were scored on the first day of ICU admission, and dynamic monitoring was not conducted during ICU stay. So we look forward to larger sample sizes and multicenter clinical studies to further confirm the predictive value of mNUTRIC score for sepsis complicated with ARDS patients.
Conclusion
In summary, the mNUTRIC score prediction has good clinical significance in predicting the occurrence of CCI in sepsis patients with ARDS, and is worthy of early attention and application in clinical practice.
Footnotes
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Yiwu Central Hospital (Approval No. K2023-IRB-059). Signed written informed consents were obtained from the patients and/or guardians.
Funding
This study was supported by the Public Welfare Project of Zhejiang Science and Technology Department (Project No.: LGF21H150001), the Scientific Research Project of Yiwu (Project No.:24-3-277), the Major key Science and Technology Project of Jinhua City (2024-3-130).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.