
Abstract
Background
Although artificial hip and knee arthroplasty has been widely used, the incidence of perioperative complications remains relatively high due to factors such as long operation time and large surgical incisions. However, the Hospital Frailty Risk Score (HFRS) clinical value for patients undergoing artificial hip and knee arthroplasty in China is not yet clear. This study aims to explore its clinical value in this population.
Objective
To explore predictive value of the HFRS in perioperative complications of artificial hip and knee arthroplasty in elderly patients.
Methods
Elderly patients who underwent artificial hip and knee arthroplasty in our hospital from March 2020 to March 2022 were selected as the study subjects. The patients were divided into the non-frail risk group (HFRS <5 points) and the frail risk group (HFRS ≥5 points) on the basis of the literature grading method. 5-factor modified frailty index (mFI-5) and Charlson Comorbidity Index (CCI) scores were assessed. General data including age, sex, ASA classification, preoperative course, and surgical time were collected through the electronic medical record system. The occurrence of postoperative deep venous thrombosis, periprosthetic infection, hematoma, anemia, and overall complications was recorded. Hospitalization days, surgical costs, and total treatment costs were also calculated for all patients.
Results
There were no significant differences in age, sex, ASA classification, preoperative course, or surgical time between the two groups (p > 0.05). The frail risk group had significantly higher mFI-5 and CCI scores (p < 0.05). This group also had a higher incidence of deep venous thrombosis and overall complications (p < 0.05), but similar rates of periprosthetic infection, hematoma, and anemia (p > 0.05). ROC analysis showed HFRS had the highest predictive value for postoperative complications (AUC = 0.851) compared to mFI-5 (0.786) and CCI (0.739). Surgical costs were similar (p > 0.05), but the frail group had longer hospital stays and higher total treatment costs (p < 0.05).
Conclusion
HFRS has better predictive value for perioperative complications in elderly patients undergoing artificial hip and knee arthroplasty compared to mFI-5 and CCI scores, and it can be used for predicting perioperative complications in elderly patients with this surgery.
Keywords
Introduction
Artificial hip and knee arthroplasty is an important surgical procedure in clinical practice for treating hip and knee joint pain, correcting joint deformities, and improving joint function. 1 It is also the most effective method for treating osteoarthritis. With the accelerated pace of social life and population aging, the number of elderly patients undergoing artificial hip and knee arthroplasty is gradually increasing. 2 Although artificial hip and knee arthroplasty has been widely used, the incidence of perioperative complications remains relatively high due to factors such as long operation time and large surgical incisions. 3 A retrospective study conducted abroad 4 showed that at least 80% of surgical patients experienced one or more complications during the perioperative period, including infection, deep vein thrombosis, postoperative hematoma, etc., which significantly affected the prognosis of elderly patients. Charlson Comorbidity Index (CCI) can reflect the overall immune and nutritional status of patients, and its application in predicting complications in surgical patients has been widely reported in clinical practices.5,6 In recent years, foreign scholars have developed a new comorbidity index scoring system called the Hospital Frailty Risk Score (HFRS), which has been proven valuable in predicting postoperative complications in orthopedic surgery in foreign populations. 7 However, its clinical value for patients undergoing artificial hip and knee arthroplasty in China is not yet clear. This study aims to explore its clinical value in this population.
Participants and methods
Research object
The elderly patients who underwent artificial hip and knee arthroplasty in our hospital from March 2020 to March 2022 were selected. Inclusion criteria were as follows: (1) age > 60 years; (2) meeting the surgical requirements for artificial hip and knee arthroplasty; (3) first-time artificial hip and knee arthroplasty. Exclusion criteria were as follows: (1) patients with malignant tumors; (2) abnormal mental status or cognitive impairment; (3) history of previous surgery on the same side of the hip or knee joint. All patients signed informed consent for the study and received approval from the hospital's medical ethics committee.
HFRS assessment
HFRS scoring is based on the International Classification of Diseases (ICD-10) in the electronic medical record system, which provides relatively standardized disease definitions and diagnoses, reducing the subjectivity in the clinical diagnostic process for physicians. 8 Gilbert et al. 9 developed the HFRS scoring system based on the ICD-10, using a modeling group of 22,139 elderly individuals and a validation group of 1,013,590 elderly individuals. By assigning scores to various clinical diagnoses in the ICD-10 and summing them up, HFRS score is obtained. 9 A higher HFRS score indicates a greater frailty risk in patients. According to the literature grading method, patients are classified into the non-frail risk group (HFRS < 5 points) and the frail risk group (HFRS ≥ 5 points).
Data collection
CCI assessment
The patients were evaluated based on 5-factor modified frailty index (mFI-5) 10 and the CCI, 11 as referenced in the literature. Both the mFI-5 and CCI scores indicate a higher frailty risk with higher scores.
Clinical data collection
Such general information as age, sex, American Society of Anesthesiologists (ASA) classification, preoperative course, and surgical duration were collected through the electronic medical record system. The incidence of complications in all patients from 1 day after operation to discharge was counted. The occurrence of postoperative deep vein thrombosis, periprosthetic infection, hematoma, anemia, and overall complications (excluding rare but severe complications such as pulmonary embolism, angina, myocardial infarction, and arrhythmias) were recorded.
The diagnosis of DVT was referred to the relevant literature, 12 lower extremity Doppler ultrasound examination combined with clinical diagnosis results as the standard..Periprosthetic infection was determined according to the results of pathogen culture, clinical symptoms and serological examination.
Hospital days, surgical costs, and total treatment costs were also documented for all patients.
Statistical analysis
The collected experimental data were analyzed with Statistic Package for Social Science (SPSS) 27.0 (IBM, Armonk, NY, USA). Normally distributed continuous variables were presented as X ± S, and independent samples t-test was used for comparisons. Categorical variables were presented as counts or rates, and comparisons were conducted using χ2 test or Fisher's exact test. The receiver operating characteristic (ROC) curve was used to evaluate the predictive value of each scoring system for postoperative complications in elderly patients undergoing artificial hip and knee arthroplasty. All statistical tests were two-tailed, and a significance level of p < 0.05 was considered statistically significant.
Results
Comparison of general information between two groups
Finally, 98 patients were included in this study,there were 56 males and 42 females. There were no statistically significant differences in age, sex, ASA classification, preoperative course, and surgical duration between the two groups (p > 0.05), as shown in Table 1.
Comparison of general information between two groups.

Comparison of general information between two groups.
The MFI-5 and CCI scores in the frail risk group were significantly higher than those in the non-frail group (p < 0.05), as shown in Table 2.
Comparison of MFI-5 and CCI scores between two groups (X ± S, score).

Comparison of MFI-5 and CCI scores between two groups (X ± S, score).
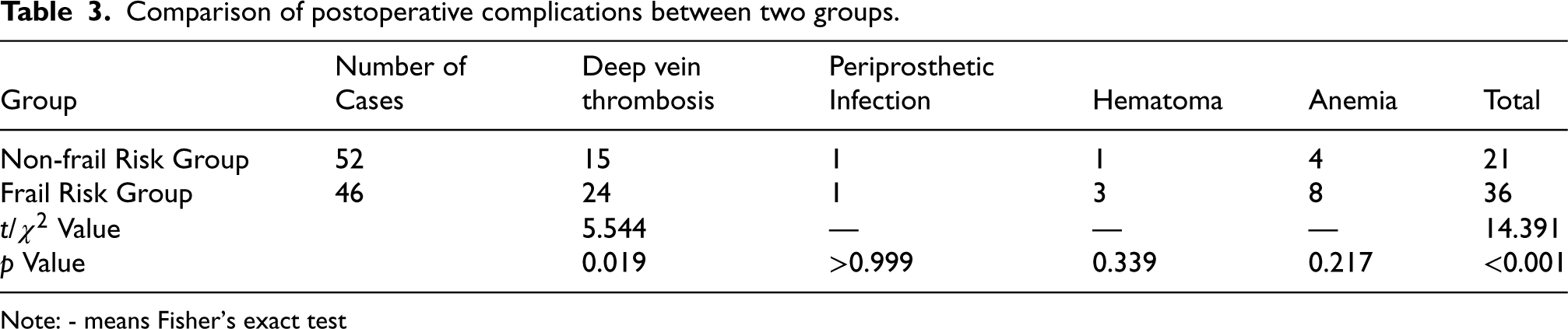
The frail risk group had a higher incidence of deep vein thrombosis and overall complications compared to the non-frail risk group, and the differences were statistically significant (p < 0.05). However, there were no statistically significant differences in the incidence of periprosthetic infection, hematoma, and anemia between the two groups (p > 0.05), as shown in Table 3.
Comparison of postoperative complications between two groups.
Comparison of postoperative complications between two groups.
Note: - means Fisher's exact test
The results of ROC analysis showed that the area under the curve (AUC) for HFRS, MFI-5, and CCI scores in predicting postoperative complications in elderly patients undergoing artificial hip and knee arthroplasty were 0.851, 0.786, and 0.739, respectively. The HFRS had the largest AUC, as shown in Table 4 and Figure 1.
Comparison of predictive value of HFRS, MFI-5, and CCI scores for postoperative complications in artificial hip and knee arthroplasty.

Comparison of predictive value of HFRS, MFI-5, and CCI scores for postoperative complications in artificial hip and knee arthroplasty.

ROC curve.
There were no statistically significant differences in surgical costs between the two groups (p > 0.05). However, the frail risk group had longer hospitalization duration and higher total treatment costs compared to the non-frail risk group, and these differences were statistically significant (p < 0.05), as shown in Table 5.
Comparison of hospitalization conditions between two groups.

Comparison of hospitalization conditions between two groups.
Artificial hip and knee arthroplasty is a commonly performed orthopedic procedure with a high utilization rate. Apart from improving joint function, it can alleviate pain and has a high acceptance rate in clinical practice, particularly among the elderly population. However, clinical studies have found that the overall incidence of postoperative complications after artificial hip and knee arthroplasty can be as high as 40% to 80%, with a severe complication rate of approximately 13.4%. 13 These complications not only impair organ function but can also be life-threatening in severe cases. Enhancing preoperative, intraoperative, and perioperative assessments of patients is of significant clinical importance for improving treatment outcomes.
HFRS has been partially applied in clinical settings. Kilkenny et al. 14 analyzed hospital data and found that HFRS had good predictive value for outcomes in stroke patients after discharge. Ramos et al. 15 demonstrated that HFRS had better predictive value for clinical outcomes in COVID-19 pneumonia patients compared to clinical frailty scores. Aitken et al. 16 found, after adjusting for various clinical variables, that HFRS could relatively accurately predict the prognosis of elderly vascular surgery patients. In this study, HFRS was used as the basis for grouping. It was found that the MFI-5 and CCI scores were higher in the frail risk group compared to the non-frail risk group, indicating that these three scores have certain discriminatory value for frailty status in elderly patients and may be correlated to some extent.
Furthermore, this study found that the frail risk group had a higher incidence of deep vein thrombosis and overall complications compared to the non-frail risk group, indicating the value of HFRS in predicting the occurrence of deep vein thrombosis and complications in elderly patients undergoing artificial hip and knee arthroplasty, consistent with the findings of previous studies by foreign scholars.7,17,18 In further analysis, this study showed that the AUC for predicting postoperative complications using HFRS, MFI-5, and CCI scores in elderly patients undergoing artificial hip and knee arthroplasty were 0.851, 0.786, and 0.739, respectively. The HFRS had the largest AUC, indicating that HFRS had better predictive value for elderly patients undergoing artificial hip and knee arthroplasty compared to MFI-5 and CCI scores. The reason for this could be that MFI-5 and CCI scores are commonly used comorbidity indices in previous studies. While they have the advantages of a smaller number of evaluation items and faster assessment, the development of these scales has been for many years, and some items may not be fully applicable to patients undergoing modern surgical treatments. 19 On the other hand, HFRS is based on the internationally-recognized ICD-10 classification, making it more relevant to the diagnosis of diseases in the current patient population.
Researchers 20 have found that the hospitalization costs for patients undergoing artificial hip and knee arthroplasty mainly include consumables, medication, examination, surgical, treatment, and anesthesia fees. The occurrence of postoperative complications undoubtedly significantly increases the hospitalization days and the cost of hospitalization. The comparative results of this study found no difference in surgical costs between the two groups. However, the frail risk group had longer hospitalization duration and higher total treatment costs compared to the non-frail risk group, indicating that assessing frailty status using HFRS not only predicts the occurrence of complications but also reflects the length of hospital stay and overall treatment costs to some extent. Therefore, targeted intervention plans should be developed for patients with higher HFRS scores to reduce their hospitalization duration and overall treatment costs.
This study has several limitations. Firstly, it is a single-center, retrospective study with a relatively small sample size, which may limit the generalizability of the findings. Additionally, the study lacks long-term follow-up data to assess the enduring impact of perioperative complications, and further prospective, multi-center studies are needed to corroborate these results.
Conclusions
In conclusion, the results of this study demonstrate that HFRS has better predictive value for perioperative complications in elderly patients undergoing artificial hip and knee arthroplasty compared to MFI-5 and CCI scores. It can be used for predicting perioperative complications in this population. Further research is needed to expand the study population and conduct larger prospective studies to refine and supplement the existing conclusions.
Footnotes
Ethics approval and consent to participate
This study was approved by the Ethical Committee of The Affiliated Hospital, Southwest Medical University (approval no. KY-20-069). Signed written informed consents were obtained from the patients and/or guardians. This study was conducted in accordance with the Declaration of Helsinki and followed the ethical standards of China.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.