
Abstract
Background
Cardiovascular diseases are a global health concern, with coronary artery disease being particularly prevalent. Percutaneous coronary intervention (PCI) via the radial artery approach (TRA) is now preferred due to its advantages. However, post-TRA hemostasis can lead to complications like hand swelling and pain.
Objective
To investigate the effect of roller support assisted balloon compression radial artery hemostasis device in patients undergoing percutaneous radial coronary intervention.
Methods
A total of 122 patients undergoing percutaneous radial coronary intervention in our hospital from March 2022 to September 2022 were randomly divided into a control group and an observation group, 61 cases in each one. The observation group was treated with roller support assisted balloon compression type radial artery hemostasis device for compression hemostasis, and the control group was treated with balloon compression type radial artery hemostasis device (TR-Band). The complications such as bleeding at the puncture site, hematoma, swelling of the hand on the operation side, and pain in the operation limb as well as the patient satisfaction were observed in the patients of the two groups.
Results
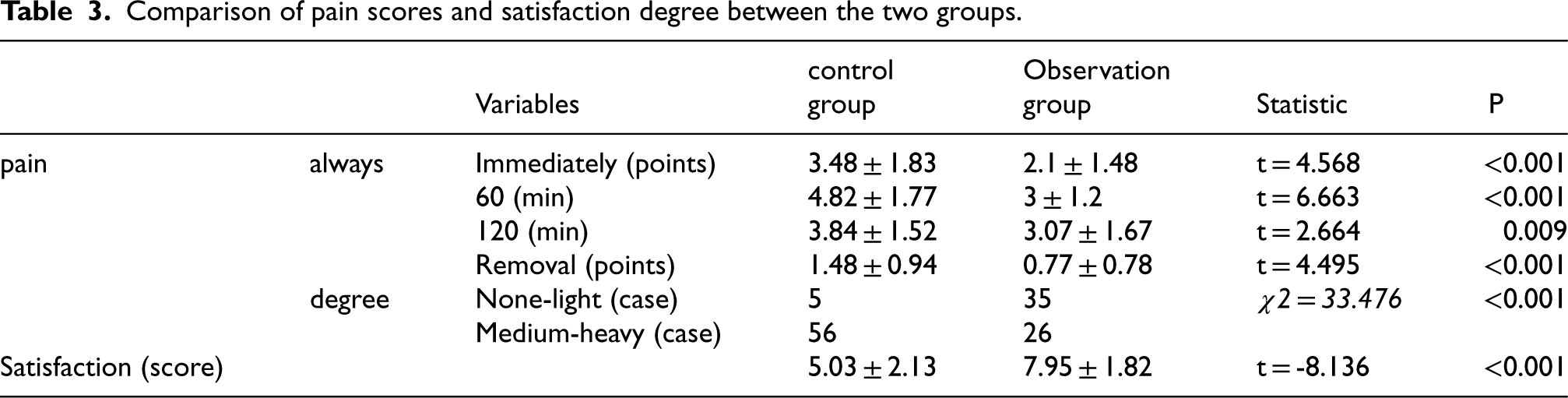
There were 10 cases of bleeding in the control group and 7 cases in the observation group, the bleeding mostly happens about 1 h after surgery. As for the pain score between the two groups of the immediately, 1 h, 2 h, and remove time were (3.48 ± 1.83), (4.82 ± 1.77), (3.84 ± 1.52), (1.48 ± 0.94) respectively, where the values in the observation group were (2.10 ± 1.48), (3.00 ± 1.20), (3.07 ± 1.67), (0.77 ± 0.78). There were significant differences in swelling, pain and satisfaction of the hand on the operation side between the two groups (P < 0.05).
Conclusion
The modified application of roller support assisted radial artery hemostat helps to reduce the incidence of postoperative non-vascular complications in patients and improve patient satisfaction, with good social effect.
Introduction
According to the Long-term Plan for the Prevention and Treatment of Chronic Diseases in China (2017–2025) and Health China 2030, it is pointed out that the prevention and treatment of cardiovascular disease is one of the important contents of health work in China in the new period. 1 In recent years, the prevalence of cardiovascular disease continues to rise in China, including as many as 11 million patients with coronary heart disease. The primary diagnosis and treatment of coronary heart disease is percutaneous coronary intervention (PCI). 2
At present, percutaneous radial artery puncture pathway coronary intervention (TRI) with the advantages of “small surgical trauma, less postoperative complications, and rapid course recovery” has been widely deployed in the world. Many hospitals in China use TR-Band compression hemostasis using balloon compression radial artery puncture site hemostasis, and after 6–8 h gradual decompression to achieve the goal of hemostasis, but there are still some patients with hand swelling, limb pain, limb numbness and other complications, 3 which increases the discomfort experience and pain of patients. Therefore, how to reduce the postoperative non-vascular complications while ensuring effective hemostasis is the focus of continuous quality improvement and also the focus of perioperative care in clinical practice. In recent years, it has been found in clinical experiments that roller support assisted radial artery hemostasis device could effectively solve the problems of patients’ hand swelling and limb pain. This research center has been granted a utility model patent: an improved radial artery hemostasis device, with the patent number of CN20819138U. The intervention effect is now reported as follows.
Information and methods
Research subjects
A total of 122 patients with coronary heart disease receiving percutaneous radial artery intervention from March 2022 to September 2022 in the Second Affiliated Hospital of Dalian Medical University were selected. The sample size for this study was calculated using a power analysis with the aim to detect a minimum clinically significant difference in the primary outcome measure, with a power of 80% and an alpha of 0.05.
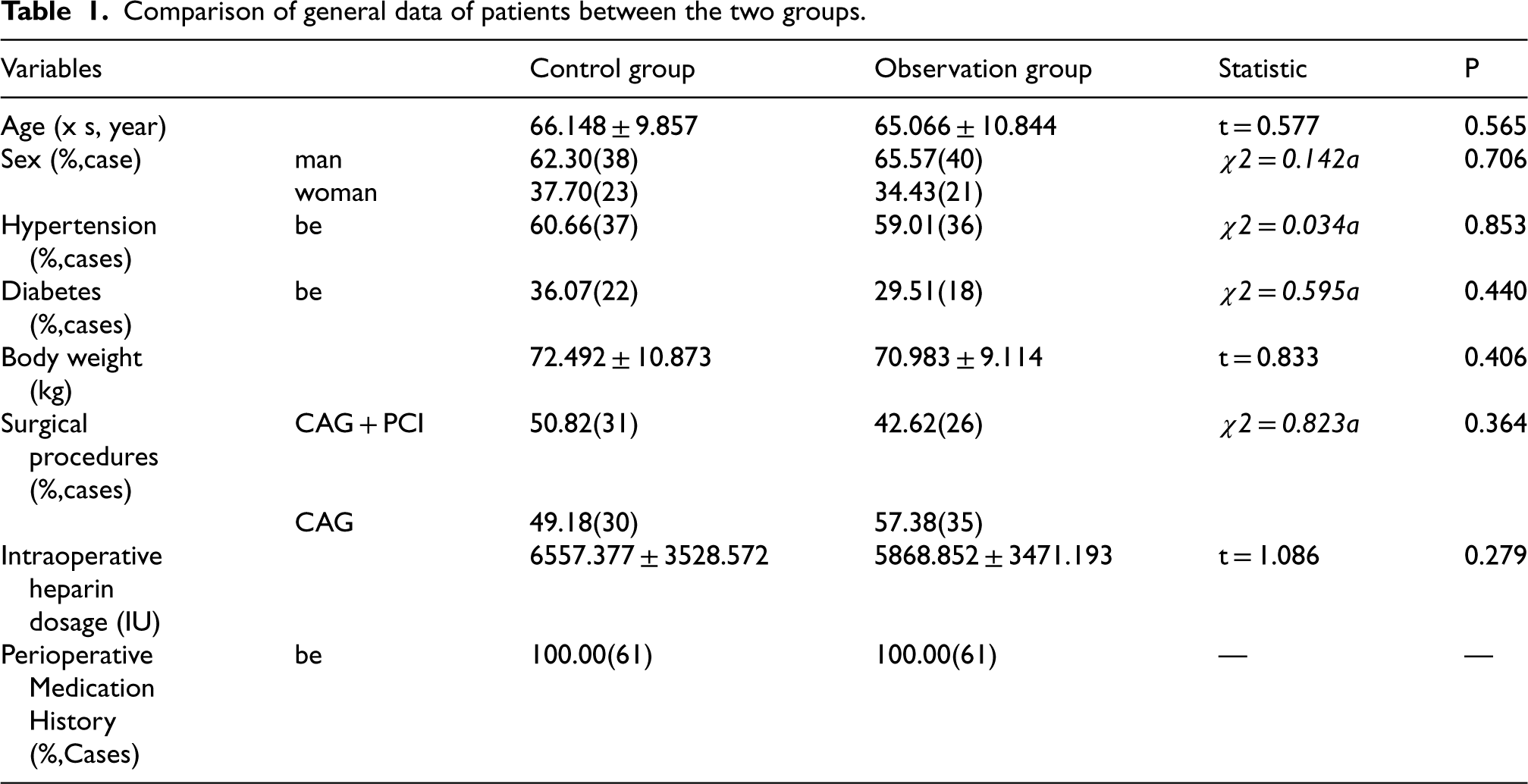
The patients were divided into the control group and the observation group by using the random number table, 61 cases in each group. The inclusion criteria were as follows: the blood supply to the ulnar and radial arteries was good, and Allen test was negative; No limb swelling, bleeding, and no skin ulceration before surgery; Clear consciousness and normal language communication; Voluntary participation and informed consent. 4 Exclusion criteria: patients with severe hemorrhagic disease; Patients who had undergone homolateral homovascular invasive surgery during the perioperative period; Unclear consciousness and unable to cooperate; Persons with mental disorders; Observer who is not stable in hemodynamics or suffers from unsustainable situations such as rescue and discharge during observation. 5 The two groups of patients were all treated by the same operation team member. There was no significant difference in baseline data such as age, gender, weight, history of hypertension, diabetes history, operation method, intraoperative heparin consumption, and perioperative medication history between the two groups (P > 0.05), as shown in Table 1. This study was approved by the in-hospital ethics committee. (The ethical batch number is: Lun Shen 2021-XJS No.122, No.2 Hospital of Great Medical Sciences)
Comparison of general data of patients between the two groups.
Comparison of general data of patients between the two groups.
Methods in the control group
Radial access switch refers to the transition from the radial artery approach to another vascular access route, typically the femoral artery, during a cardiac catheterization procedure or PCI. In the control group, when the percutaneous radial artery puncture route was used for coronary intervention, the members of the intervention operation group strictly followed the operation procedures, withdrew the radial artery sheath tube by 2.0 cm, and applied the balloon compression type radial artery hemostasis device (TR-Band, manufactured by Terme Co., Ltd, Japan) for compression hemostasis. The green mark point at the center of the compression balloon by the hemostat was aligned with the puncture point of the patient. The appropriate length was selected according to the wrist circumference of the patient, and the adjustable lock catch was fixed. Then, 13–18 mL air was injected into the balloon with the “AIR” mark using the matching syringe. Subsequently, the arterial sheath was immediately pulled out to observe whether the puncture point was bleeding. The balloon was decompressed 1 h, 2 h and 3 h after operation, with the pressure value of 5.5 N each time (that is, 1–2 mL air was pumped out of the balloon by matching syringe). Whether there was hemorrhage and hematoma at the puncture site should be observed after each decompression. The radial artery hemostat could be removed 6 h after operation without any abnormality. The puncture site should be covered with sterile gauze and then covered with elastic bandage with low tension, and aspirin were used for anticoagulation Generally, the number of attempts of radial artery puncture is less than 2 times.
Methods in the observation group
After TRI operation in the observation group, on the basis of the operating procedures of the control group, the roller was used to support and assist the compression and hemostasis of the balloon-pressurized radial artery hemostasis device (the roller was made of soft rubber, and its length was 13 cm and diameter was 1 cm). The roller was placed beside the styloid process of ulna on the hand back of the patient, and fixed at both ends of the roller with medical transparent adhesive plaster. The roller was transversely rolled for 0.5 cm every 30 min. The rolling range was in the two-thirds area of the wrist close to the ulna side of the patient, and the back area of the hand was alternately supported. The supporting effect of the roller was conducive to tissue fluid reflux and venous reflux of the hollow parts on both sides (Figure 1).

Use and structural schematic diagram of a roller support auxiliary balloon pressurized radial artery hemostasis device.
The following indexes were observed immediately after operation, 1 h, 2 h and at the moment when the hemostat was removed: ①Pain: The digital pain score (NRS) was applied to assess the pain score of the patients, with the total score ranging from 0 to 10 points; the mild pain score ranged from 0 to 3 points, the moderate pain score ranged from 4 to 6 points, and the severe pain score ranged from 7 to 10 points. 6 ②Visual observation of the puncture point around the presence of bleeding, bleeding, hematoma, if there is a bruise, puncture point around the skin protrusions occurred immediately to the corresponding hemostatic measures and the application of soft ruler to measure the scope of the bruise; The soft ruler was used to measure the forearm circumference of the patient. If the forearm circumference was increased, the clinical ultrasound results were combined to determine whether there was secondary subcutaneous hematoma. We also investigated the bleeding rate (from level 0 to 5) of patients according to the Bleeding Academic Research Consortium (BARC) criteria. ③The peripheral diameters of the second finger joint of each finger in the operated limb of the patient were measured by using a soft ruler, and the sum of the peripheral diameters was calculated. The measured results immediately after surgery were taken as the initial values of the benchmarks, and the difference between the measured results again after the hemostat was removed and the initial values was taken as the observed values. No swelling was observed when the observed value was less than 0.5 cm, mild swelling was observed when the observed value was 0.5, 1.5 cm, moderate swelling was observed when the observed value was 1.6–2.5 cm, and severe swelling was observed when the observed value was greater than 2.5 cm. 7
④ Check for the presence of allergies, ulcers, or tension blisters on the surgical limb skin; For allergies, we look for signs of skin reactions such as redness, itching, rash, or swelling that may indicate an allergic response to materials used in dressings, tape, or other products that come into contact with the skin. For ulcers, we check for breaks in the skin that are deeper than normal skin layers, which can be a result of pressure, poor circulation, or infection. Ulcers may present as open sores that are painful and take a long time to heal. As for the tension blisters, we examine the fluid-filled blisters that occur when friction causes the top layer of skin to separate from the layers below. ⑤After the hemostat was removed, we observed whether the limb had low skin temperature and abnormal sensation, and if so, we evaluated whether there were signs of radial artery occlusion (RAO) such as disappearance of vessel wall pulsation in the radial artery combined with ultrasound. ⑥To determine whether there are signs of compartment syndrome such as continuous pain, pale limbs, numbness and paresthesia; ⑦Satisfaction: patients fill in satisfaction questionnaire before discharge.
Statistical analysis
Statistical analysis was performed using SPSS20.0 (IBM). The measurement data were expressed as the mean and standard deviation. Two independent samples t test was used for inter-group comparison. The rationale for using t-tests is that they are appropriate for comparing the means of two groups when the data is approximately normally distributed and the variances are similar between groups. The specific values were given from the enumeration data. Chi-square test was used for inter-group comparison. This method was chosen because it allows us to evaluate the effects of time and group on the measured variables while accounting for the correlation between repeated observations from the same subjects. Repeated measures analysis of variance was performed for the repeated measures data, and the data were expressed as mean and standard deviation. The time factor was defined as immediately after surgery, 1 h, 2 h, and when the tourniquet was removed. The group factors were divided into the observation group and the control group. The repeated measures analysis of variance was performed for the time factor and thesignificance level for all tests was set at 0.05, which is a conventional threshold in statistical analysis to balance the risk of Type I and Type II errors.
Results
Vascular complications
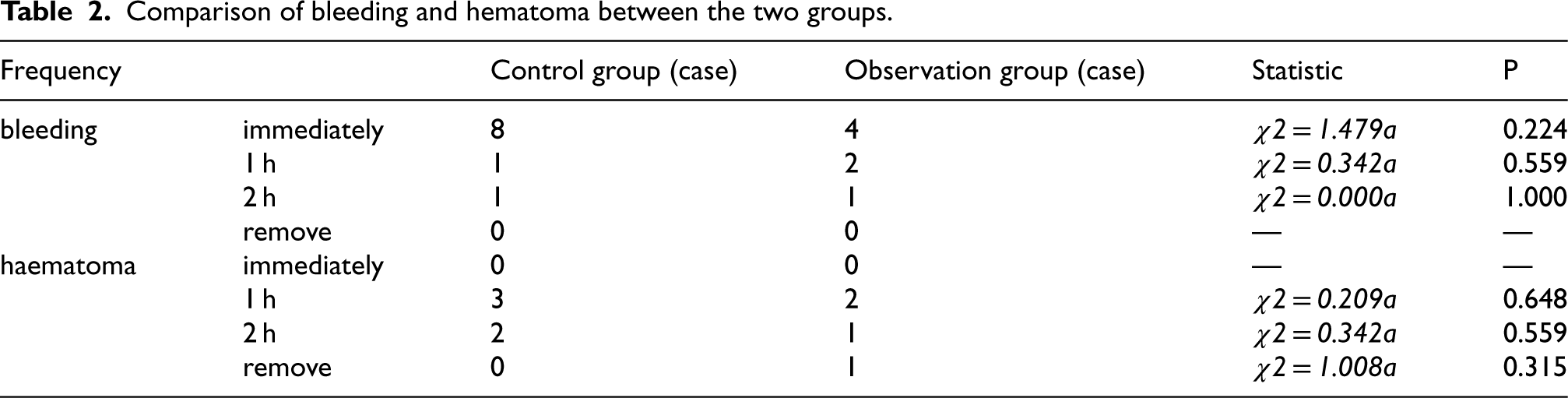
There were no cases of RAO and compartment syndrome in both groups. The bleeding at puncture site after operation was compared between the two groups. There were 10 cases of bleeding in the control group. In the observation group, there were 7 cases of bleeding, and the bleeding time was mostly about 1 h after surgery. Among the 10 cases of bleeding in the control group, there were 5 cases with level 1 bleeding and 2 cases of level 2 bleeding according to the BARC standard. Where there were 4 cases of level 1 bleeding and 3 cases of level 2 bleeding in the observation group. There was no statistic significant difference between the two groups as for bleeding. The subcutaneous hematoma of the operated limb in the two groups was compared. In the control group, there were five cases of bleeding around the puncture point and no case of increased arm circumference. In the observation group, bleeding was observed in four cases around the puncture point, and no increase in arm circumference was noticed. There was no significant difference (P > 0.05), as shown in Table 2.
Comparison of bleeding and hematoma between the two groups.
Comparison of bleeding and hematoma between the two groups.
There was no case of local skin allergy, ulceration or tension bleb in both groups. The distribution of the number of cases of limb pain was compared between the two groups. The pain scores at each time node of patients in the observation group were significantly lower than those in the control group, and the difference was statistically significant (P < 0.05). Moreover, the number of patients with moderate to severe pain was significantly lower than that in the control group, as shown in Table 3. After the tourniquet was removed, the sum of the peripheral diameters of each phalanx was measured, and the observation value was obtained by subtracting the difference from the initial value. The hand swelling situations of the two groups were compared. The results of the observation group were better than those of the control group. See Table 4.
Comparison of pain scores and satisfaction degree between the two groups.
Comparison of pain scores and satisfaction degree between the two groups.
Comparison of peripheral diameters of each finger joint between the two groups.

The results in the observation group were significantly better than those in the control group. The patients in the observation group had relatively comfortable perioperative experience, as shown in Table 3.
Discussion and conclusions
In recent years, the number of research papers and patents concerning the prevention, treatment and nursing care of cardiovascular diseases has shown a blowout growth trend. The coronary intervention technology has gradually matured and been widely used in clinical practice. However, postoperative hemorrhage, limb swelling and pain are still important factors affecting the patients’ rehabilitation and satisfaction after operation.
At present, TR Band radial artery hemostat is clinically used for compression hemostasis at the puncture point in many hospitals in China, and the pressure is gradually reduced within 6–8 h after operation to achieve the hemostatic effect. However, due to the age, past medical history, application of heparin during operation, and long-time mechanical compression, etc., the patient may suffer from postoperative swelling, pain, and other non-vascular complications. According to analysis, the pressure value of normal skin capillaries was 2.7 kpa(1 mmHg = 0.133 kPa). The radial artery hemostat used a balloon to compress the puncture point, and the spherical surface had difficulty in calibrating precision. In this case, the radial artery hemostat was required to apply pressure up to 150, 250 mmHg to the skin at the wrist to achieve effective hemostasis. However, strong high pressure and long-time blocking of the perfusion of capillaries into tissues would stagnation the blood flow in the vessels, resulting in blocked distal blood backflow and limb swelling.8,9 In addition, the hemostatic device is made of hard plastic, and the hard bandage directly compresses the skin. In addition, long-term mechanical compression hinders the return flow of tissue fluid and accumulates anaerobic metabolic wastes, which further increases the pain and skin lesion possibility of patients. 10
The results of this study showed that the roller support assisted balloon compression radial artery hemostat for postoperative compression hemostasis had good application effects on pain score, satisfaction degree and peripheral diameter observation values of each finger joint of patients, and it could reduce the swelling of hands on the operation side, alleviate the pain at the puncture site, and increase the comfort and satisfaction degree of patients without increasing the complications such as hemorrhage and hematoma. In that pressurize radial artery hemostasis device with the roller support auxiliary air bag, the roller plays a supporting role between the hard binding band and the skin of a patient, so that tissue fluid and vein in the middle hollow part cannot flow back, and the pain and swelling of the patient are reduced by dispersing the compression area and unblocking blood flow back; The transverse rolling rollers at regular intervals after operation can alternately support the back area of the hand, to avoid skin damage or even tension blisters caused by long-time compression of a part. The design has simple operation steps, the roller device can be repeatedly used after disinfection, has good economic value and social effect, and is suitable for universal promotion to continuously improve the quality and safety of nursing and improve the equalization level of nursing service. The importance of balancing the risks of bleeding and thromboembolic events in patients with AF undergoing PCI is also important in these patients, and the use of NOACs, particularly at reduced doses, is becoming more prevalent. However, better adherence to guideline recommendations regarding NOAC dosing to minimize bleeding complications is also required. 11 In addition, the evaluation of invasive cardiologist experience is also an important step, the total number of radial PCI procedures performed, the experience level in selecting the LRA for procedures, and the association between experience and patient outcomes determining the choice of radial access and its potential impact on procedural outcomes. 12 As the rapid development of large language models, such as ChatGPT, Gemini, etc., some researchers have explored the use of AI medical device.13–16 Thus, the AI-assisted roller-assisted balloon compression methods will be a promising direction in this area.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Ethical approval
Informed consent
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.