
Abstract
Background
TMJ disorders often involve a multidisciplinary approach, clear understanding is a must for the treatment of TMDs. This study aimed to assess the behaviour, perspective and treatment approach of Dental Practitioners towards the management of TMJ Disorders. This would help in developing the census about the knowledge level and attitude towards TMD among dental practitioners.
Methods
A comprehensive cross-sectional investigation involving 1030 dentists was conducted through the implementation of a meticulously designed survey instrument created using Google Forms. The questionnaire contained 17 closed-ended questions with the ability to mark more than one option in a few questions. the first 5 questions (Q1-Q5) determined the behaviour of Dental practitioners when they initially face TMD patients, (Q6-Q8) were asked to determine the perspective regarding cause–effect relationship in TMD disorder,(Q10-Q17) determined the treatment approach of Dental practitioners. Dichotomic answers were compared using a binomial test and multiple answers were evaluated using a Clopper-Pearson test with significance set at p < 0.05.
Results
77.7% of participants reported that they receive potential TMD patients in their office most frequently found aetiology for the pain was occlusal discrepancy (48.5%) followed by trauma (39.8%). The most commonly referred specialities were maxillofacial surgery (57.3%) and Prosthodontics (29.1%). The majority of the Practitioners treated their TMD patients with occlusal splints.
Conclusion
The management of TMJ disorders requires a comprehensive and interdisciplinary approach. Practitioners clarified that TMD patients were mostly treated with conservative measures using occlusal splints. However, the dentist should have cooperative behaviour and a clear perspective for the proper management of TMDs.
Introduction
Temporomandibular joint (TMJ) disorders refer to a group of conditions that affect the jaw joint and the muscles controlling jaw movement. 1 Temporomandibular disorders (TMDs) are a class of musculoskeletal and neuromuscular conditions that affect the temporomandibular joints (TMJs), the masticatory muscles, and all associated tissues. This was stated in a 2010 statement published by the American Association for Dental Research (AADR).1–3
This complex joint connects the jawbone to the skull and is essential for activities such as talking, chewing, and yawning. TMJ disorders can manifest in various ways, leading to pain, discomfort, and restricted jaw movement. Diagnosis often involves a thorough examination by a dentist and treatment options vary based on the severity and underlying cause of the disorder. Some conservative approaches may include lifestyle modifications, stress management techniques, and the use of oral appliances to alleviate symptoms. In more severe cases, medical interventions such as physical therapy, medications, or, in rare instances, surgery may be recommended. 3
Managing TMJ disorders often involves a multidisciplinary approach, and patients may benefit from collaboration between dentists, physical therapists, and other healthcare professionals. Early recognition and appropriate intervention can help alleviate symptoms and improve the overall function of the TMJ. Numerous significant studies have validated the multidimensional biopsychosocial model of TMD. According to the biopsychosocial paradigm, individuals with TMD should have comprehensive assessments of their mobility difficulties, psychological distress, chronic pain, and social conditions .
For many years of diagnosis and treatment of TMDs, attention has been placed on the TMJ's viewpoint; in the results of diagnosis from MRI and tomography, in the anamnesis, and the physiological response of muscles and articulations during sound contact. Nevertheless, the dental view, namely occlusal and its relation with the treatments, is equally necessary to obtain a harmonious stomatognathic function. 4 The correct occlusal analysis provides valuable diagnostic information for TMDs. Tech-scan is incorporated as part of a new diagnostic system. The Tech-scan system, the T-scan, is a tool for measuring and recording occlusal contacts during jaw movement. The occlusal analysis is an important aspect in the evaluation of TMD treatment, and new technologies may enhance the diagnostic procedures. The occlusal discrepancies, which are high-risk factors of TMDs, could be visualised by the integration of new technologies or advanced diagnostic devices and techniques in the classical occlusal analysis.5,6
Numerous treatment options exist for managing temporomandibular joint disorders (TMDs), but the optimal treatment approach for the management of TMDs is still not clear. TMD treatments can be approximately classified into three groups: a conservative approach including educational and psychological interventions and physical modalities, pharmacological methods, and surgical intervention in terms of invasiveness. These therapeutic agents or modalities can be used alone or in combination. Splint therapy approaches can be classified roughly into non-invasive modalities that do not have a direct influence on the masticatory system and central nervous system, and invasive ones with alteration of occlusion intended by wearing occlusal appliances for cognitive occlusal adjustments. It is important to have individual patient management based on functional, behavioural, and structural aspects and geared to the pain modulatory processes that may be largely generalised dysfunction of the somatosensory modulatory system.4,7–10
DC/TMD has proposed the biopsychosocial model as one of the key tenets of clinical considerations. In daily clinical practice, it has been discovered that some dentists have very limited awareness of TMD and view it as a straightforward somatic symptom or organic lesion.11–15 This frequently results in patients receiving an incorrect diagnosis or advice regarding treatment possibilities. There are many factors which may influence the existing motivation to obtain further skills in treating TMD patients. It may be intrinsic cognitive factors, personal satisfaction, and professional pride or other extrinsic factors including positive or negative recognition by another specialist, promotion of one's own dental office by providing high quality patient care, and the very perspective of achieving financial benefits. Failure to recognise the need for psycho-social, endocrine, or anti-inflammatory treatment in dentistry, related stigmatisation of people in pain, fear of tension and defence reaction on the part of the practitioner treating TMD, loss of prosthetic or pharmacological patients, lack of investment in this treatment by the patient, and stress due to unrealistic expectations are the most influencing factors. 16 Thus, assessing dentists’ present knowledge of TMD diagnosis and treatment might aid in the development of effective educational initiatives to raise their degree of TMD-related knowledge and awareness. Numerous research involving dentistry students or practicing dentists in various countries have been conducted thus far to gain an understanding of the knowledge and attitudes surrounding TMD. 17
A cross-sectional study reported that Iranian general dentists lacked sufficient information regarding chronic Orofacial Pain (OFP), particularly about therapy. 18 Similarly, Indian post-graduate students have low confidence in their ability to manage diseases of the TMJ, according to a cross-sectional study. 19 Patients’ normal lives, money, and exposure to needless treatment will all be impacted by the dentist's incapacity to diagnose OFP.
To evaluate dental professionals’ knowledge, attitudes, and practices (KAP) on TMDs, a few surveys have been conducted globally. 20 Nevertheless, no research has been conducted in India when searched using a PubMed data base.
This study aimed to assess the behaviour, perspective and treatment approach of Dental Practitioners towards the management of TMJ Disorders. This would help in developing the census about the knowledge level and attitude towards TMD among dental practitioners in India, thus revealing the current status of TMD education and helping in framing the policies and guidelines for the same.
Materials and method
Type of study and sampling
Data for this cross-sectional study were gathered from a representative sample of the western Central India region's registered dental practitioners, who finished their studies and practised dentistry in an institution, and dental practitioners, who finished their education and became licenced dentists. The non-probability sampling method, (quota sampling) was utilised. To calculate the sample size the following formula was used - sample Size = (Z-score)2 × Standard Deviation × (1-Standard Deviation) / (confidence interval)2 (Andrew Fisher's Formula- where standard deviation 0.5, Confidence level 95%, Z-score 1.96, confidence interval 6.), 21 Considering a total of 1030 participants in the study.
Ethical considerations
This study was conducted in compliance with the Declaration of Helsinki; ethical approval (YCDC/IES-IRC/312/2023-24) was given by the ethics committee of the Yashwantrao Chavan Dental College, Ahmednagar, Maharashtra, India. The participants provided their informed consent. Participation was voluntary and there were no incentives. Data protection and anonymity were guaranteed.
Questionnaire
An online survey instrument was meticulously crafted utilising Google Forms. This digital questionnaire encompassed a spectrum of inquiries about the diagnosis, awareness levels concerning TMDs, the modalities of treatment employed, and the subsequent follow-up protocols for TMDs. The hyperlink to the Google Form was disseminated across a diverse cohort of dental practitioners using different platforms for communication, e.g., WhatsApp, e-mail., (including general dentists, Prosthodontists, Oral and maxillofacial surgeons, Orthodontists, Pedodontists, Periodontists, Oral Pathologists, and Public health dentists). The communication data of every participant was gathered and coded. Every participant received two weekly reminders to send in the completed questionnaire along with their answers. When necessary, the respondents were given the opportunity to have in-depth conversations and were given explanations about the study and its application.
A total of 1030 dentists participated in the survey. Inclusion in the sample was independent of the school of origin, age, gender, professional experience, or year of graduation. Informed consent was taken before the start of the survey.
The questionnaire contained 17 closed-ended questions with the ability to mark more than one option in a few questions. The survey instrument utilised in this investigation was analogous to one utilised by Aldrigue et al. 3 in Brazil, which relied on information from the American Academy of Orofacial Pain, the European Academy of Craniomandibular Disorders, and the AADR. They informed that a systematic review of agreements based on international recommendations for TMD and OFP management was conducted to confirm the questionnaire used in their study.
The questionnaire used in the sample survey study was revised by adding five new questions. Its validity and reliability were evaluated by 4 senior dentists and a psychometrician for vetting and remarks. The suggested changes were made to guarantee its coherence. Additionally, 115 participants in pilot research validated the questionnaire. The pilot research dataset obtained was assessed to check the consistency in reply after analysis, strong internal consistency was found with an overall Cronbach's alpha of 0.82 for the questionnaire. There were three sections to the study's questionnaire.
In the present study, the first 5 questions (Q1-Q5) determined the behaviour of Dental practitioners when they initially face TMD patients, (Q6-Q8) were asked to determine the perspective regarding cause–effect relationship in TMD disorder,(Q10-Q17) determined the treatment approach of Dental practitioners. With the exception of the yes/no choice questions, participants were allowed to select more than one response on the questionnaire.
Statistical Analysis: For all statistical tests, SPSS Software, IBM version 24.0 software was used. Descriptive statistics(frequency and percentage) and inferential statistics were calculated for all variables. Dichotomic answers were compared using a binomial test and multiple answers were evaluated using a Clopper-Pearson test with significance set at p < 0.05
Results
The results of the study can be considered under the behaviour, perspective and treatment approach of the participants. On analysing the results of the study for the behaviour towards TMD, it can be ascertained that knowledge plays an important role in developing the behaviour. Of the dental practitioners surveyed, 77.7% reported that they receive potential TMD patients in their office (p < 0.001). The majority of the participants 80% knew the diagnosis but very less cohorts had treatment knowledge for TMD. The diagnostic procedure employed, the approach toward each patient, and the place of referral were significantly different among dental practitioners (p < 0.001). A combination (78.6%) of the medical history, physical examination, radiological visualisation and Study models were the most frequently employed strategies for obtaining a diagnosis. Of the practitioners who responded, 80.6% reported that they offered treatment to the patients. Maxillofacial surgery and (57.3%) Prosthodontics (29.1%) were common specialities for patient referral. (Table 1, Figure 1 and 2).
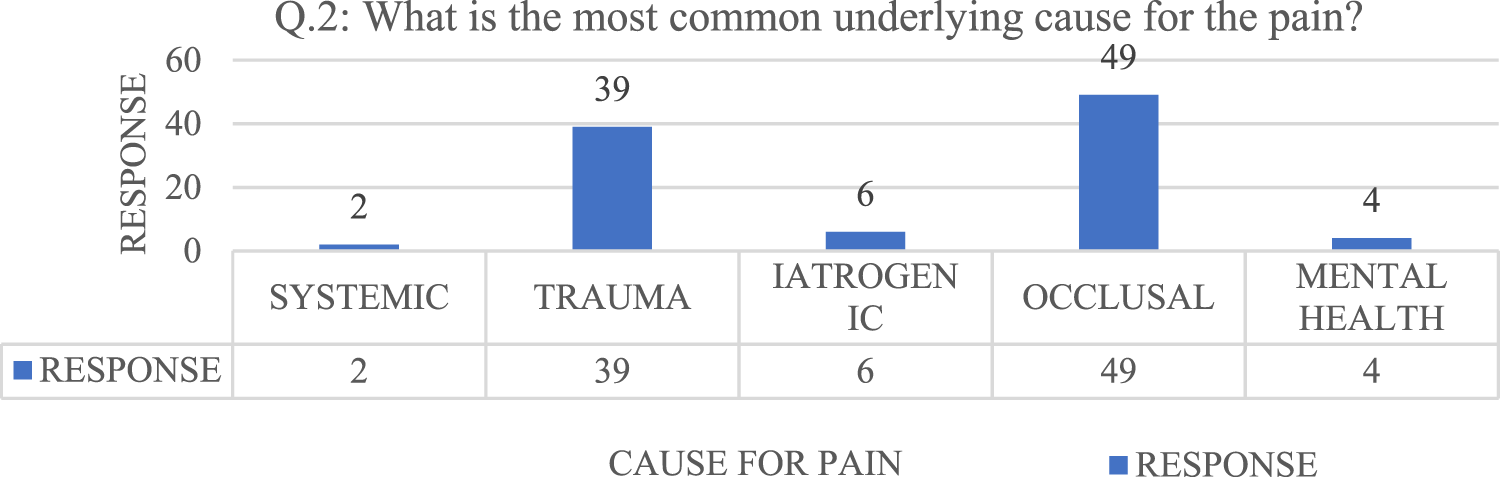
Figure depicting the responses for the cause of Pain.

Figure depicting the responses related to speciality for referral of TMD patients.
Distribution of behaviour-related questions.

The perspective of the participants overall shows positive towards the TMDs. This perspective is mainly governed by the attitude, the majority of participants feel that TMDs should be treated on a priority basis and it affects not only the stomatognathic system but also the whole body. Table 2 indicates the responses to the cause–effect relationship questions for TMD. All the practitioners were aware of the relationship between TMD and malocclusion. Half of the practitioners considered the occurrence of MPDS(52.4%) to be more common while the other half (53.5%) considered clicking and deviation to be more prevalent.
Questions regarding cause–effect relationship in TMDs.

Table 3 shows the responses to the treatment approach employed occlusal splinting(33%) followed by oral rehabilitation and prosthetic treatment(22%)were the most common treatments. 48.5% practitioners responded to the usage of soft stabilisation appliances fabricated by conventional technique(59.2%) used. During splint fabrication, 80.6% of practitioners used semi-adjustable articulators, for occlusal adjustments at the time of application. Occlusal splints were made in maximum intercuspation(30.1%) or a centric relationship by (34%) of the practitioners, with the treatment based on the features of the individual patients (p < .001).
Distribution of questions on the treatment approach employed.
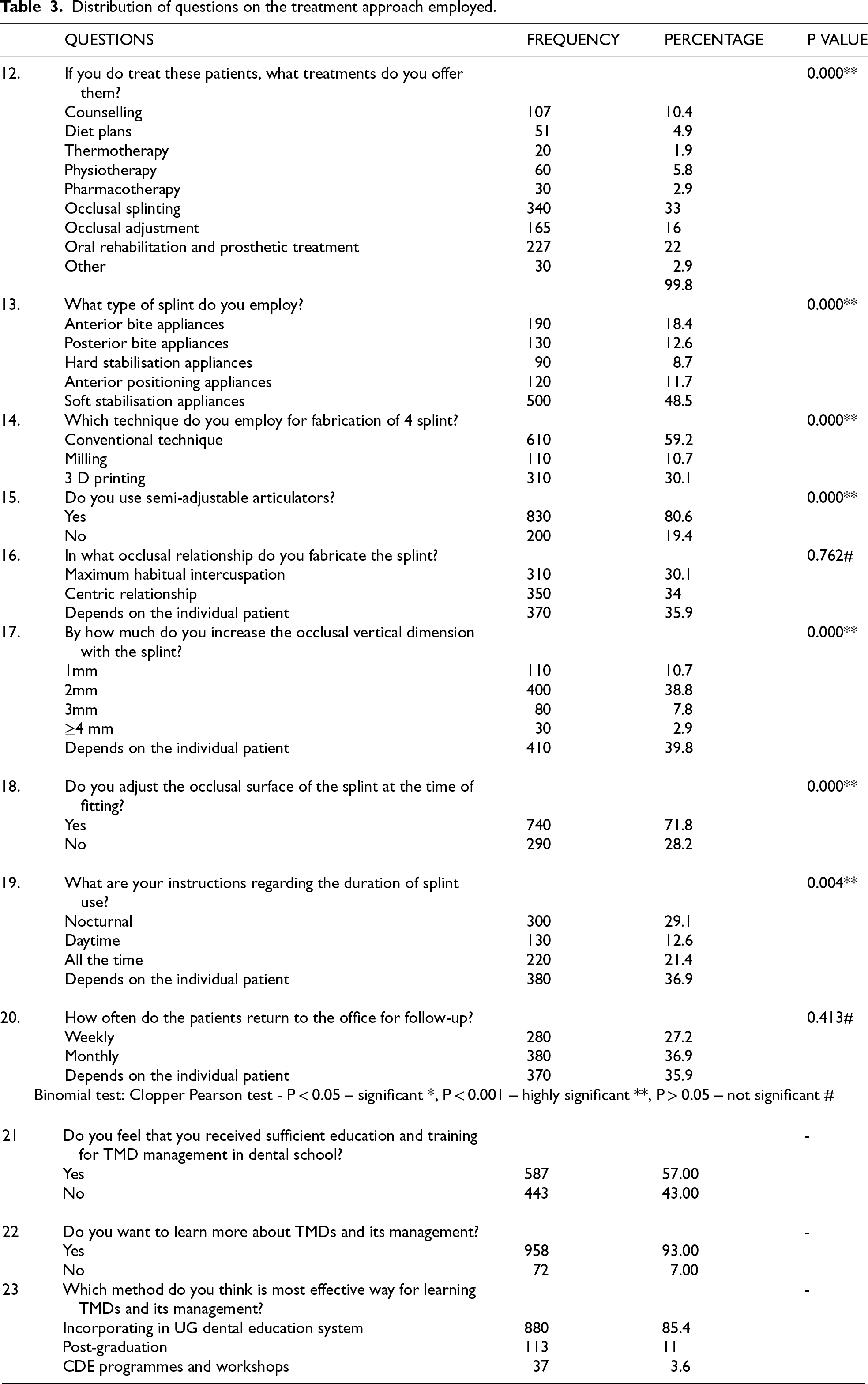
39.8% of practitioners considered that the increase in vertical dimension should done depending upon individual patient. (p < .001).71.8% of practitioners made adjustments to the splint's occlusal surface during fitting.29.1% of practitioners gave their patients instructions on how to use night-time splints. In contrast, 36.9% thought that the length of time a splint should be used depended on the patient (p < .001). A majority of practitioners (36.7%) conducted monthly follow-ups with their patients (p < .001).
Temporomandibular joint (TMJ) disorders are a complex and often misunderstood set of conditions that affect the jaw joint and surrounding muscles. The TMJ is a hinge joint connecting the jawbone to the skull, and it plays a crucial role in various daily activities such as speaking, eating, and facial expressions. When dysfunction occurs in this joint, it can lead to a range of symptoms, including pain, stiffness, clicking or popping sounds, and difficulty in jaw movement. Understanding the intricacies of TMJ disorders is vital for healthcare professionals to provide accurate diagnosis and effective management strategies.14,22–24
One of the key challenges in dealing with TMJ disorders is the diversity of symptoms and the multifactorial nature of the condition. The exact causes of TMJ disorders can vary, encompassing factors such as genetics, trauma, stress, or dental issues. 24 This complexity underscores the importance of a comprehensive approach to diagnosis and treatment. Dentists, oral and maxillofacial surgeons, and physical therapists play crucial roles in addressing TMJ disorders. A thorough evaluation, including a detailed medical history, clinical examination, and often imaging studies, is essential to identify the underlying causes and determine the most appropriate course of action.
In more severe cases or when conservative measures prove ineffective, surgical interventions may be considered. Arthrocentesis, a minimally invasive procedure involving the flushing of the joint with sterile fluids, can provide relief by removing inflammatory byproducts. Arthroscopy, another surgical option, allows for a more detailed examination of the joint and the removal of damaged tissue.13,25 For more complex cases, open-joint surgery may be necessary to address structural abnormalities or reposition the disc within the joint. The decision to pursue surgical intervention should be based on a thorough assessment of the individual's condition, considering factors such as the severity of symptoms, response to conservative treatments, and overall health.
Collaboration among different healthcare professionals is paramount in the management of TMJ disorders. Dentists and oral surgeons work hand in hand to diagnose and treat dental issues that may contribute to the dysfunction of the TMJ. A multidisciplinary approach ensures that all aspects of the condition are addressed comprehensively, leading to more effective and lasting outcomes. The difficulties in the management of TMD arise from the fact that it is a multifactorial disorder and the importance of having multidisciplinary care with various kinds of specialists. Interdisciplinary teams of dental practitioners, medical specialists, clinical psychologists, social workers, and physical therapists have been assembled for the management of TMD patients.19,20 To develop expertise in treating TMD, several factors can influence this process. Educational programmes provide most healthcare professionals with fundamental theoretical information and procedural skills. The essentials of knowledge invested in professional improvement in diagnosing and treating TMD will give them a clear understanding of the complexity and a need for collaboration in the treatment approach, amalgamating knowledge from dentistry and physical examination, communication, and cooperation with other medical specialists and psychologists. Ongoing training in this field serves as a supplementary source of new knowledge and experience. Practical professional improvement in treating TMD is also crucial, this will not only benefit the clinicians but also help in influencing the patients with jaw related problems and providing the valuable and effective treatment. 8
Patient education is an integral component of TMJ disorder management. Many individuals may not be aware of the potential causes and risk factors associated with TMJ disorders, and misconceptions abound. Providing patients with clear and accurate information about their condition, treatment options, and expected outcomes is essential for empowering them to actively participate in their care. Educating patients about self-management techniques, such as stress reduction strategies and proper jaw habits, can significantly contribute to the success of treatment plans.
Furthermore, ongoing research is critical for advancing our understanding of TMJ disorders and refining treatment approaches. The development of more targeted and personalised interventions relies on a deepened knowledge of the underlying mechanisms and contributing factors. Researchers are exploring the role of genetics, inflammatory processes, and biomechanical factors in the development and progression of TMJ disorders. By uncovering these complexities, scientists aim to identify novel therapeutic targets and refine existing treatment protocols, ultimately improving outcomes for individuals affected by TMJ disorders . Education programmes with a focus on patients’ experiences, applied through learning activities that emphasise a broad perspective on the patient, better clinical reasoning, and the development of communication strategies, may help to foster effective practice. This education should challenge dental practitioners to become curious, try new things, and put extra emphasis on the social learning environment in multiple contexts. We recommend education that stimulates learning in a community of practice in which collaboration between professionals of different backgrounds is encouraged. The ability to communicate and work together with other medical professions is important since physical care for patients with TMDs should be managed interdisciplinary. Again, this way may be conducive to practical and acute application in educational settings as well as help to guide improvements in educational content. In the long run, to enhance TMDs, dental professionals should put their efforts into policy changes in the aforementioned domains. 26
In this study, more than 75% of the participants had TMD patients in their clinical set-up and almost 65% treated them at the clinic, while 35% of dentists referred treatment to other specialists which is an important finding as participants consider the TMD to be treated with priority (96.8%) but when it comes to treating them major section is referring them. The reason may be many but the most important is the lack of complete knowledge about TMDs and its treatment. This is a fact that should be given due consideration as most of the time it is the dentist who will be approached first by the patients for any issues related to TMJ. The Council of the European Academy of Craniomandibular Disorders also recommends a basic initial examination to rule out a TMD and an assessment using oral, maxillofacial, and general histories together with relevant imaging studies to establish a workable diagnosis. This aids in the classification of illnesses including neurological, mental, and head and neck disorders as well as the detection of psychosocial variables. 27 It is recommended that dentists should be ready to learn always, and it is a proven fact that the more the dentist examines and gives treatment the more confident and skilled the practitioner gets and gain confidence.
About 78.6% of the cohort use combination methods to diagnose patients in 8.7% use physical and radiological methods mainly. Numerous research has addressed the prevalence of evidence-based clinical diagnosis techniques compared to cutting-edge technical techniques.1,20,28 It is always better to have a combined assessment modality over a particular one. This finding of the present study is in accordance with many previous studies where a physical examination and the patient's medical history are the main approaches used by GDPs to diagnose TMD, while other diagnostic techniques have also been covered in earlier research.28–31 In contrast, all GDPs diagnosed TMD based on the patient's medical history and physical examination; none used a radiological visualisation or created a study model, according to a study by Tamer et al. conducted in Istanbul. 32
The primary goal of an effective TMD treatment plan should be to reduce the signs and symptoms of TMDs. 33 The existence of joint sounds (clicking and crepitation), decreased mouth opening, and abnormal jaw motions are the most pertinent indications of TMD.34,35 However, the main issue with this condition is pain, which is usually the reason these individuals seek medical attention. Additionally, it is probably the reason why the majority of research has focused on assessing the efficacy of different intervention strategies with as the primary variable.36,37
The bar graph (Figure 1) reveals trauma (38.7%) and occlusal factors (48.6%) as predominant contributors to reported pain, while systemic, iatrogenic, and mental health factors exhibit comparatively lower impact. These findings underscore the distinct hierarchy of pain aetiology within the surveyed cohort. In the present study, Dental practitioners who referred their TMD patients to a specialist preferred to refer them to Oral surgeons (57.3%), Prosthodontists(29.1%) and Orthodontists (10.7%) (Figure 2). In the present study, choice of speciality for referral was oral surgeon which is in contrast to the practitioners of the Istanbul who preferred the Prosthodontists and Orthodontists more, also the study by Aldrigue et al. 3 indicated that most GDPs in Brazil referred their TMD patients to orthodontists. Irrespective of the speciality it should be kept in mind by the treating dentist that the TMDs should be treated with the most conservative and reversible treatment, and the same has been documented and enforced by two consensus publications, on treatment techniques for TMD patients1,27 most of the time the approach by the Prosthodontists and Orthodontists is conservative and reversible, on other hand maxillofacial surgeons are aggressive in approach but for sure each has their scientific proof to perform a particular treatment.
Of the surgical treatments available, arthrocentesis based on articular lavage with or without pharmaceutical injection and arthroscopy are the two most commonly utilised methods for internal derangements of the TMJ or degenerative disease. When comparing arthroscopy with arthrocentesis, there are no differences in terms of discomfort or mandibular function. 38 Nevertheless, there is insufficient data to suggest that arthrocentesis is a more effective therapeutic intervention than nonsurgical methods.39,40 Patients with symptomatic disc dislocation without reduction should be treated with the simplest and least invasive method 41 ; medicinal therapy or rehabilitation is preferred over other surgical options for internal derangement of the TMJ. In addition, there is mounting proof that platelet-rich plasma injections are superior to hyaluronate with arthrocentesis in treating TMJ osteoarthritis; nevertheless, additional clinical trials are required.
The cohort in the present study reported MPDS as the most common TMJ problem followed by Ankylosis and Internal derangement. Effective management of TMJ disorders requires a combination of conservative and, in some cases, surgical interventions. Conservative measures often include lifestyle modifications, such as stress management techniques, dietary adjustments, and the application of heat or cold packs to alleviate pain and reduce inflammation. Physical therapy exercises aimed at strengthening and stretching the jaw muscles can be beneficial in restoring normal function. In addition, the use of oral appliances, such as splints or mouthguards, may be recommended to help stabilise the joint and prevent teeth grinding or clenching, which can exacerbate TMJ symptoms.
The most popular treatment option provided by dental professionals in the survey was the splint (33%), which was followed by counselling, occlusal adjustment (16%), oral rehabilitation and prosthetic treatment (22%), and counselling (9.7%). According to a 2013 survey, 76% of GDPs treated patients with TMD, 97.6% provided mouthguards or splints, 85.9% encouraged self-care, 84.6% gave prescriptions for over-the-counter drugs, and 63.6% performed occlusal adjustment.
In comparison to non-occluding splints or no treatment, hard occlusal splints have shown a respectable level of success in treating temporal muscle dysfunction discomfort, according to a meta-analysis. 42 On the other hand, research has shown that the results of patients treated with active and placebo splints were comparable. Alencar and Becker 43 treated three groups of patients with hard splints, soft splints, or non-occlusal splints after randomly selecting 42 patients with myofascial pain. According to their study's findings, all three appliances helped with symptom relief, and after 90 days, there were no appreciable differences between the three groups. As a result, the current study suggests that, as a conservative measure, using splints (soft stabilisation equipment) as the initial treatment for TMD patients is reasonable regardless of the contact surfaces of the splints or the material / technique from which they are produced.
According to Terebesi et al.'s, 44 investigation into the connection between motor unit recruitment and vertical alterations in the jaws, the degree of vertical splint separation was positively correlated with the patients’ therapeutic outcomes for myofascial pain syndrome. In the current study, dental professionals (39.8%) changed the occlusal splint's thickness based on the requirements of specific patients, and 38.8% changed it by two millimetres.
Dental schools should identify pain in the orofacial region more broadly, rather than restricting their expertise to pain that is solely related to intraoral structures. They should also understand that pain is a legitimate health concern that the dentist should be handling. 3 This present study's findings are comparable to those of a study by Aldrigue RHS et al., 3 which found that 81% of GDPs are comfortable treating patients at their dental clinic, whereas 19% of GDPs are referred to another dentist or academic institution because they lack the necessary skills and expertise. However, comparable research carried out in other regions of the world revealed that GDPs felt uneasy about the diagnosis and treatment of TMDs. They also underlined the need to develop and strengthen undergraduate dental course curricula and continuing education in TMD.
Almost the entire cohort (93%) was willing to learn about TMDs in detail. Learning is a curve which will never flatten, as illustrated by the results of our study: almost all participants were ready to enhance their knowledge. They feel the amount of knowledge that they have received during education is not sufficient and the majority consider the incorporation of a detailed pain management curriculum in the Undergraduate dental education system would enhance the understanding and provide better care to patients. Also there are many factors which may influence the existing motivation to obtain further skills in treating TMD patients. It may be intrinsic cognitive factors, personal satisfaction, and professional pride or other extrinsic factors including positive or negative recognition by another specialist, promotion of one's own dental office by providing high quality patient care, and the very perspective of achieving financial benefits. The perception of opportunities for the exchange of experience with well-known experts in the field, especially during residency, for being a potential successor, or the lack of a supportive work environment are some factors that could affect the motivation of dental expert for TMDs treatment. Failure to recognise the need for psycho-social, endocrine, or anti-inflammatory treatment in dentistry, related stigmatisation of people in pain, fear of tension and defence reaction on the part of the practitioner treating TMD, loss of prosthetic or pharmacological patients, lack of investment in this treatment by the patient, and stress due to unrealistic expectations are the most influencing factors. 45
Limitations
There are some limitations in this study. The extended questionnaire length contributed to insufficient responses, and the absence of information about the participating dentists, the inherent limitation of the close-end questions, open-ended questions with the ability to express the views would give a better perspective about the topic. In the present the closed-ended questionnaires (participants may provide suggestions or ideas, simple answers may be given to complex questions, and participants may misinterpret questions), and nonprobability sampling technique (which significantly depends on the researchers’ experience) are used which is a major limitation because participants were not able to present their view. It is recommended to use open end questions in future work. We felt that the questions in the study should include the level of education, experience and training associated with the practitioners to get a clear idea about the understanding of the TMDs by the clinicians.
The small sample size and poor response rate in comparison to the covered area. Thus, it is not appropriate to generalise the results. It's important to consider the inherent limitations of cross-sectional studies (participants may not respond).
It is advised that future research be conducted nationwide, for example, in cooperation with government organisations. This would present a more comprehensive picture of TMDs among dentists in practice. It would be better to create a new curriculum that places more of an emphasis on TMDs and how to manage them. Additionally, regular continuing dental education courses should be held to improve dentists’ understanding of TMDs and their sophisticated management techniques. Additionally, dental practitioners should be taught about and inspired to use these techniques in order to give better care when necessary.
Conclusion
In conclusion, the management of TMJ disorders requires a comprehensive and interdisciplinary approach. Dental professionals must navigate the intricate web of symptoms, causes, and contributing factors to provide accurate diagnoses and effective treatments. Conservative measures, including lifestyle modifications and physical therapy, are often the first line of defence, while surgical interventions may be considered in more severe cases. Collaboration among dentists, oral and maxillofacial surgeons, physical therapists, and other healthcare providers is essential to address the multifaceted nature of TMJ disorders. They should have cooperative behaviour and a clear perspective for the management of TMDs, because operating alone has the danger of failing to notice important problems that could have a negative long-term treatment and patient outcome impact.
Footnotes
Abbreviations
Acknowledgement
This work was been done in collaboration with YCMM RDF's Dental college Ahmednagar Maharashtra (India) with College of Dentistry, King Khalid university, ABHA, Saudi Arabia.
Ethics approval and consent to participate
This study was conducted in compliance with the Declaration of Helsinki; ethical approval (YCDC/IES-IRC/312/2023-24) was given by the ethics committee of the Yashwantrao Chavan Dental College, Ahmednagar, Maharashtra, India. The participants provided their informed consent.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through a Small Group Research Project under grant number RGP 1/298/45.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.