
Abstract
Fetal Heart Disease (FHD) is the most prevalent root cause of infant demise which accounts for 21% of all congenital abnormalities, with most instances being catastrophic, thereby rendering the need for early prognosis. Ultrasonography is the forefront imaging modality for assessing fetal growth in four-chamber and blood vessel malformation. Clinically diagnosing the abnormality is time-consuming and requires the skill of a radiologist. In subsequent, numerous preceding research strategies ideal to meta-heuristic and deep learning's Faster Artificial Neural Network (FANN), Dense Recurrent Neural Network (DRNN), Mask-Regional Convolution Neural Network (M RCNN) and Enhanced Deep Learning-assisted CNN aid in the identification of FHD. However, the prediction models have encountered multiple challenges owing to imprecise hinders and irrelevant adhesion. Hence, we propose the automated hierarchical network-driven findings of FHD in four-chamber and blood vessels using ultrasonic 2D imaging which undergoes 3 consequential processes of Enhanced-Adaptive Median Filtering (EAMF) pre-process concerning noise variations i.e., test for SNR distortion and image enhancement i.e., visual quality, Intensified Region of Interest (IROI) segmentation for exploiting feature selection via spatial mask-labeling and Multiresolution Deep Convolutional Neural Network (MDCNN) classification in the detection of diseased pattern via confusion metrics (CM). The lesion findings of CM is determined using MATLAB R2023b with an overall substantial efficiency of 99.79% in both normal and abnormal conditions with a significant potential to assist cardiologists in the prognosis of FHD.
Keywords
Introduction
The leading category of malformations, FHD poses a significant threat to infants depicting a top cause of fetal death in accordance with the World Health Organization (WHO).1,2 The septal defect is perhaps a quite typical FHD affecting the four chamber's (FCs) atrial and ventricles and 3-vessel's blood flow (BF) 3 with the most common disorders of Atrial Septal Defects (ASDs) i.e., Aortic Stenosis and Atrial Hemangioma,4–6 Ventricular Septal Defects (VSDs), 7 and Tetralogy of Fallot (ToFs). 8 Thus, Early diagnosis of fetal heart defects is crucial for improving the prognosis of the fetus since these conditions might entail abnormalities in the fetal heart anatomy. 9 Consequently, it is important to facilitate medical treatment as soon as possible, generally within a week after delivery. Enabling prognosis, a standard prenatal ultrasound examination is screened to test for congenital vasculature throughout the fetal phase of life. The ultrasonic transducer is a non-surgical, accessible, and radiation-free medical imaging which has become an integral part of contemporary cardiology methods for FHD diagnosis.10,11 Early fetal ultrasound intervention, during the second trimester (18 to 22 weeks) of pregnancy,12,13 has been apparent to be more effective with beneficial detection outcomes in both four-chamber and blood vessels as depicted in Figure 1.
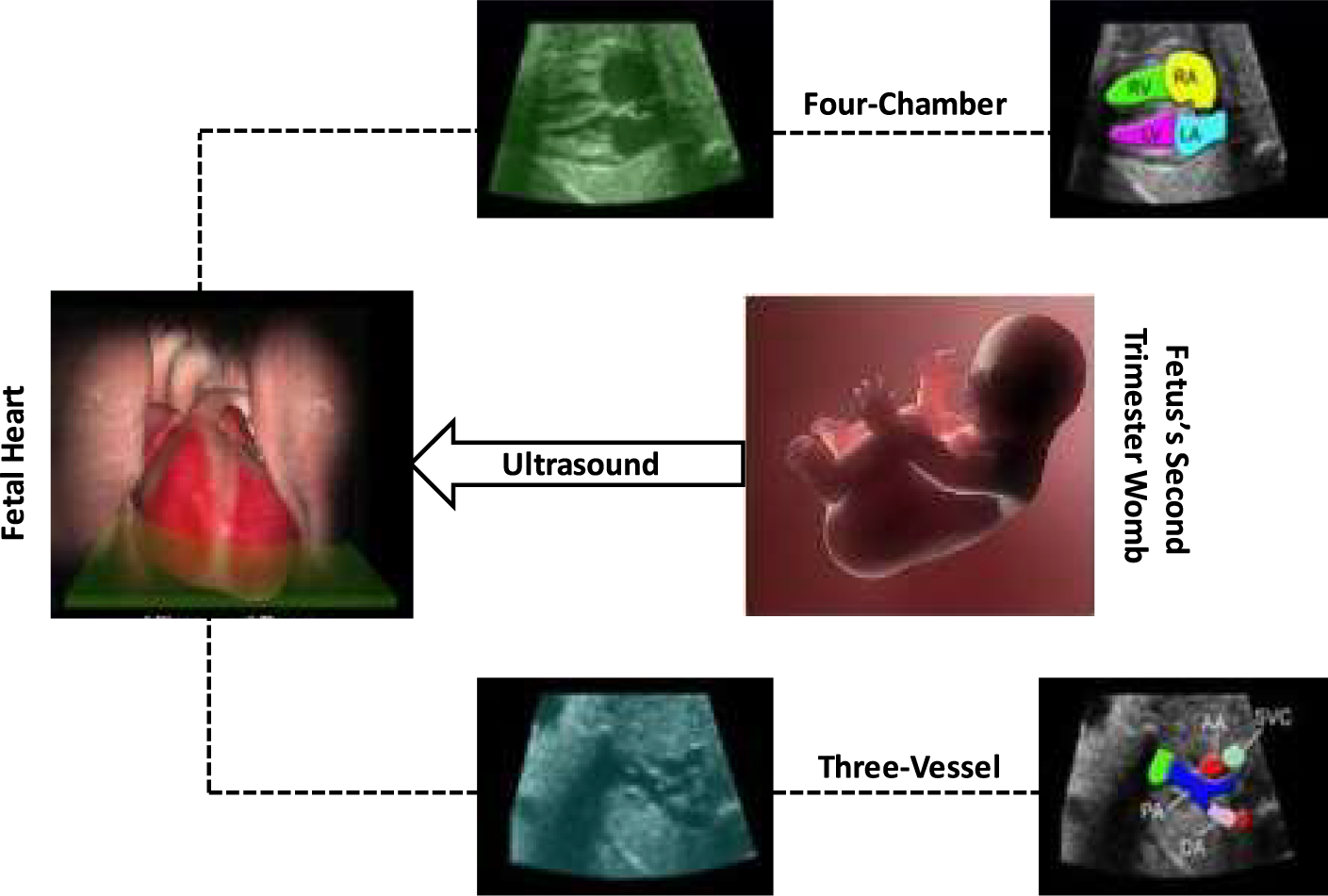
Ultrasound screening of fetal heart's four-chamber and three-vessel.
Despite, the obstetrician encounters formidable challenges in discriminating the fetal heart's dimensional proportions in four-chamber and three-vessel captured via echocardiography screening. 14 To resolve this dispute, the automated neural network-driven algorithms i.e., AI, ML and DL have pertained more precedence, enabling obstetricians to instantly recognize the congenital heart chambers and blood vessels and to optimize the reliability of FHD diagnosis rate. In topical, DL techniques have become more imperative in the FHD healthcare domain where numerous medical datasets are digitalized to streamline dense and complex clinical data.15–17 In evaluating the detection of four-chamber and 3-vessels via DL, three-phase remains constant 1. Image Pre-Processing, 2. Segmentation and 3. Classification wherein commencing, the fetal raw data is laid out as input which undergoes preliminary pre-process in transforming the raw data into a denoised and precise visual format. In subsequent, segmentation is applied where it detects the tumor region i.e., the foreground of the fetal data. In final, image classification is performed, enabling the prediction based on its defect size as pictured in Figure 2.
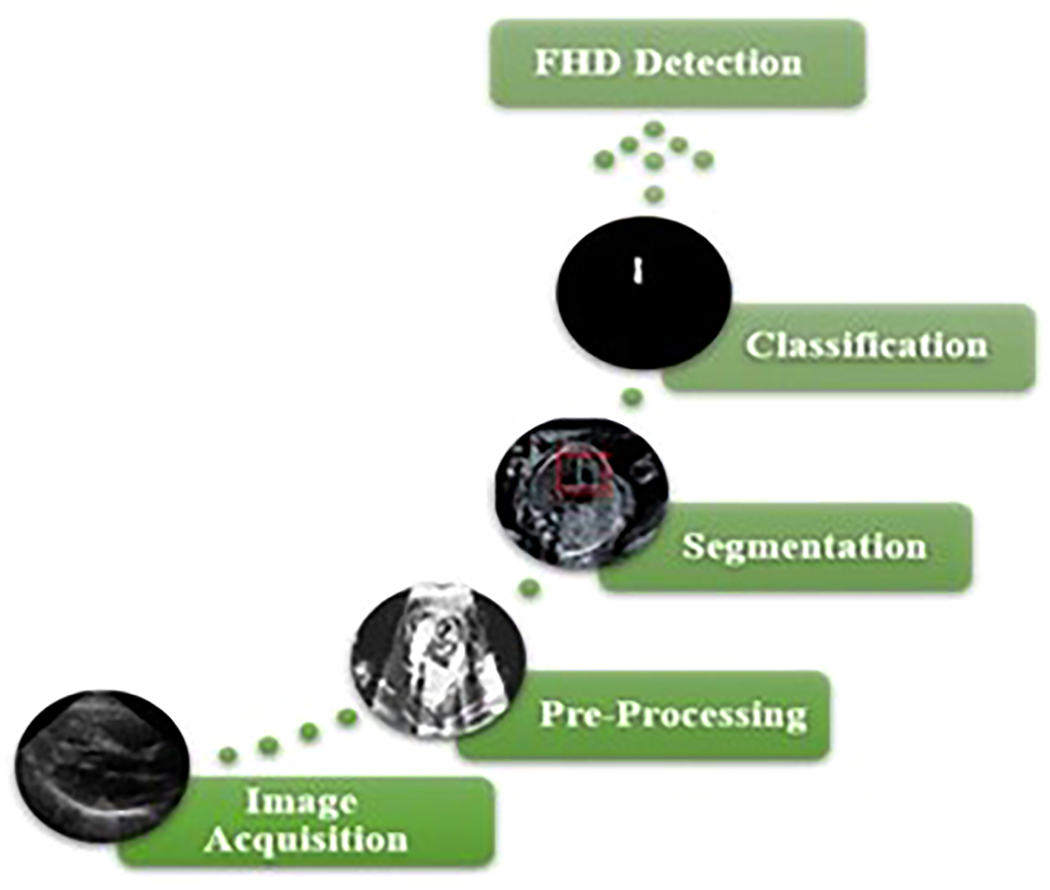
Workflow of FHD image detection.
As a result, this research seeks to diminish the risk of FHD by using the highly precise feature segmentation and classification-based prediction approach in Ultrasound images concerning fuzzy pattern matching, noise-variant interpretation and inter-functional disease i.e., Atrial, Ventricles, Aorta (AO), Pulmonary Artery (PA), and Vena Cava (VC) via medic anticipation.
The diagnostic models via computer-aided interpretation of Artificial Intelligence (AI) have showcased significant prognosis in clinical FHD echocardiography. 18 Following the advancement of AI, Multiple meta-heuristic incorporated DL methods have enabled the ultrasound examination19,20 via automated image segmentation 21 and classification 22 of fetal heart. All algorithms of DL provide a comprehensive analysis, initiating from raw data to classified images. 23 For instance, the fetus's assessment of atrial, ventricles and vessels prognosis. 24 Addressing the contribution of existing methods in recent findings, Shalini et al. 25 proffered Faster Artificial Neural Networks (FANN) in enumeration with Sequential Minimal Optimization (SMO) cataloguing large-scale datasets with multiple feature selections in detention of FHD traits. In adjoint, Khan et al. 26 deployed Minimum Redundancy Maximum Relevance (MRMR), a spatial-based ANN algorithm to screen the Cardio-Vascular Conditions (CVC) via Phonocardiogram (PCG). The MRMR has been detected with the inflated level of CVC. Ensuing the exertion of SMO and MRMR, Someshwaran et al. 27 contemplated Modified-ANN's Multilayer Layer Perceptron (MLP) integrated with preferable Principal Component Analysis (PCA) segmentation resulting in the improved feature selection and FHD classification with highly estimated confusion metrics.
Following the spadework of DL's ANN, the hierarchical learning put forth Recurrent Neural Network (RNN)28,29 in detecting embryonic dilemmas in the early 18 months via cardiotocograph (CTG) screening contraction to regulate the timely diagnosis. The model's efficacy has been tested using CTG parametric analysis of the Fuzzy Induction (FI) algorithm with temporal attentive pooling in lesion constraints delineation. Consecutively, Wang et al. 30 further deployed Dense Recurrent Neural Network (DRNN) deploying the assortment of Long Short-Term Memory (LSTM) model integrated with region-based segmentation to predict four-chamber cardiac dysfunction. By leveraging the combination algorithm, DRNN detected the congenital anomalies more precisely with 90% efficacy. In eventual, Krishnan et al. 31 propounded an integrative RNN approach utilizing Gated Recurrent Unit (GRU) and Synthetic Minority Oversampling Technique (SMOTE) in feature extraction and classification accompanied by the Framingham dataset via TensorFlow in the detection of fetal abnormalities. This integrative model was acquired with the momentous risk rate of 90.5%.
Triumphing the success rate, the heuristic optimization insights Convolutional Neural Networks (CNNs) in accordance to the advancement of RNN, where Y. Gong et al. 32 laid out DANomaly Wgan-GP and CNN (DGACNN), an innovative approach incorporating DANomaly and GACNN (Wgan-GP and CNN) for neonatal Congenital Heart Defect (CHD) detection in ultrasonography screening. This combined algorithm identified CHD with an astounding 85% success rate, resulting in an efficient foetal cardiac abnormality prognosis. Subsequently, Xu et al. 33 implemented Cascaded-CNN in enumeration with median filtering to improve the fetal image vision and region-based segmentation to pinpoint the foreground image of the fetal heart. Succeeding with the foreground segment, the CNN classifier feature maps the disease region via spatial traits. Later on, Nurmaini et al. 34 put forward multi-class delineation to automate the segmentation of atria, ventricles, valves, aorta and hole detection. Here, Mask-RCNN is incorporated with the semantic segmentation for interpreting the ultrasound data. The outcome predicts a strong correlation between expected septal abnormalities and legitimate prenatal issues. Another pertinent DL strategy put forth CNN in enumeration with the visual geometry group 35 to legitimate the Region of Interest (ROI) spatial learning of fetal features and detect the FHD via VGG 16 classified temporal traits. The resultant prognosis has been achieved with the optimal rate of 89% precision. Adjourning, Pan et al. 36 implied Enhanced Deep Learning-assisted CNN (EDCNN) with ResNet for fetal heart image analysis in ultrasound images integrating with the precise ROI segmented features in the enumeration of IoT. The test results demonstrated a remarkable efficacy of 91% in detecting the risk level of embryonic heart defects. The summarization outflow of the above algorithms is depicted in Table 1.
Summarization outflow.

Summarization outflow.
The aggregate flaw in the current prognosis models is that they scarcely segmented and classified fetal heart chambers and vessels rather than meticulous discretion. Besides, Fault diagnosis in ultrasonography provokes to be more erroneous in identifying the embryo's regional traits and spatial features. Hence, to alleviate these challenges, the prior research incorporated with the collation of multiple DL algorithms suggests that CNN-based strategies are more appropriate in prenatal revelation with high attribute features and are superior in training performance with the accreted detection of FHD.
The eminent methodology presented in Figure 3 resides in detecting the normal and abnormal septal flaws at each phase through the meta-heuristic deep learning modules. The overall FHD prognosis approach involves fetal image acquisition, image pre-processing via Enhanced-AMF, and Intensified ROI segmentation integrated with Multiresolution DCNN classification's result rendition and validation.
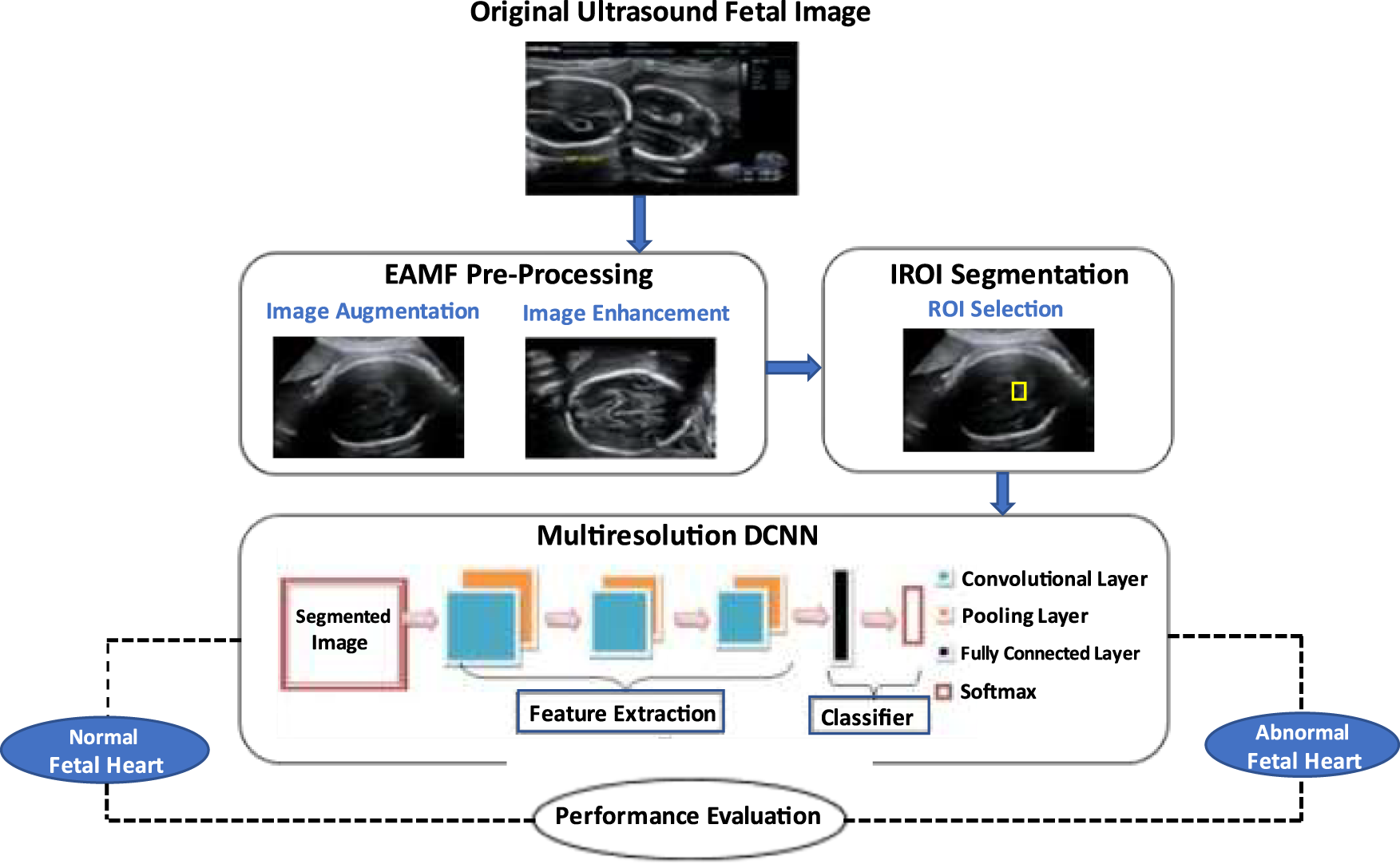
Overview of FHD's propounded prognosis.
The intent of generating legitimated medical datasets profoundly assists in network-driven heuristic algorithms to carry out the semantic test for FHD prognosis. Table 2 emphasises the antenatal fetal coronary ultrasound datasets acquired via the Indian Institute of Science Fetal Heart Sound Database (IIScFHSDB) 37 featuring both normal and anomalous data images of foetal heart planes with confidential patient consent. The collected data of 2226 images assess the impact of the proffered research work assimilated in the ultrasound using GE-Logic 400 and Voluson E6 apparatus, where the four-chamber scan of 665 and 526 image planes concerning right and left atrial-ventricles i.e., RA, RV, LA, LV and three-vessel scan of 526 and 509 image planes concerning PA, AO and SVC database framework were utilized for the prenatal FHD's diagnosis approach.
FHD image dataset acquisition.

FHD image dataset acquisition.
In the experiment, the fetal data is iterated into three category sets: training, testing and validation with the distribution of 65%, 20%, and 15% respectively. The categorized sets forth 1470 images for training, 467 images for testing and 289 images for validation. The input images are sized with 128 × 128 × 3 initially. This dimension size is used for preliminary denoising while the latter is re-scaled to 197 × 197 × 3 larger data size and enumerated to IROI and MDCNN fabrication. For training, Adaptive Moment Estimation (Adam) is utilized as the optimizer to pertain the gradient and momentum constant with an initial learning rate of 10−2. In subsequent, the batch size is set to 20 and the no. of epoch is iterated at 10.
Fetal image pre-processing
The fetal images from ultrasound contain pertinent noise, and denoising them appears to be challenging. The propounded design technique acquires pre-processing the images for multiple GUI-based diagnostic modules in the estimated FHC dataset system. The advancements in US imaging modes achieved through digital screening enumerates the utilization of the Enhanced-Adaptive Median Filtering (EAHE) algorithm38,39 to effectively denoise and improve the prognosis assessment. The EAMF pre-processing strategy in Figure 4 trounces out the traditional de-noising filtering methods via data integration, transformation and cleaning with subsequent data dimension and missing value imputation. The simulated data of EAMF adequately retains contour patterns and enables the sonographers to identify preliminary features in the screened images, with diminishing distortions of Gaussian and speckle noises in esteem with SNR in equation 1.
where w (i, j) – EAME resultant image, k (f, g) – Distorted noise of input image, and h ij – Driven integer of k, defined over the pixel intensity (f, g).
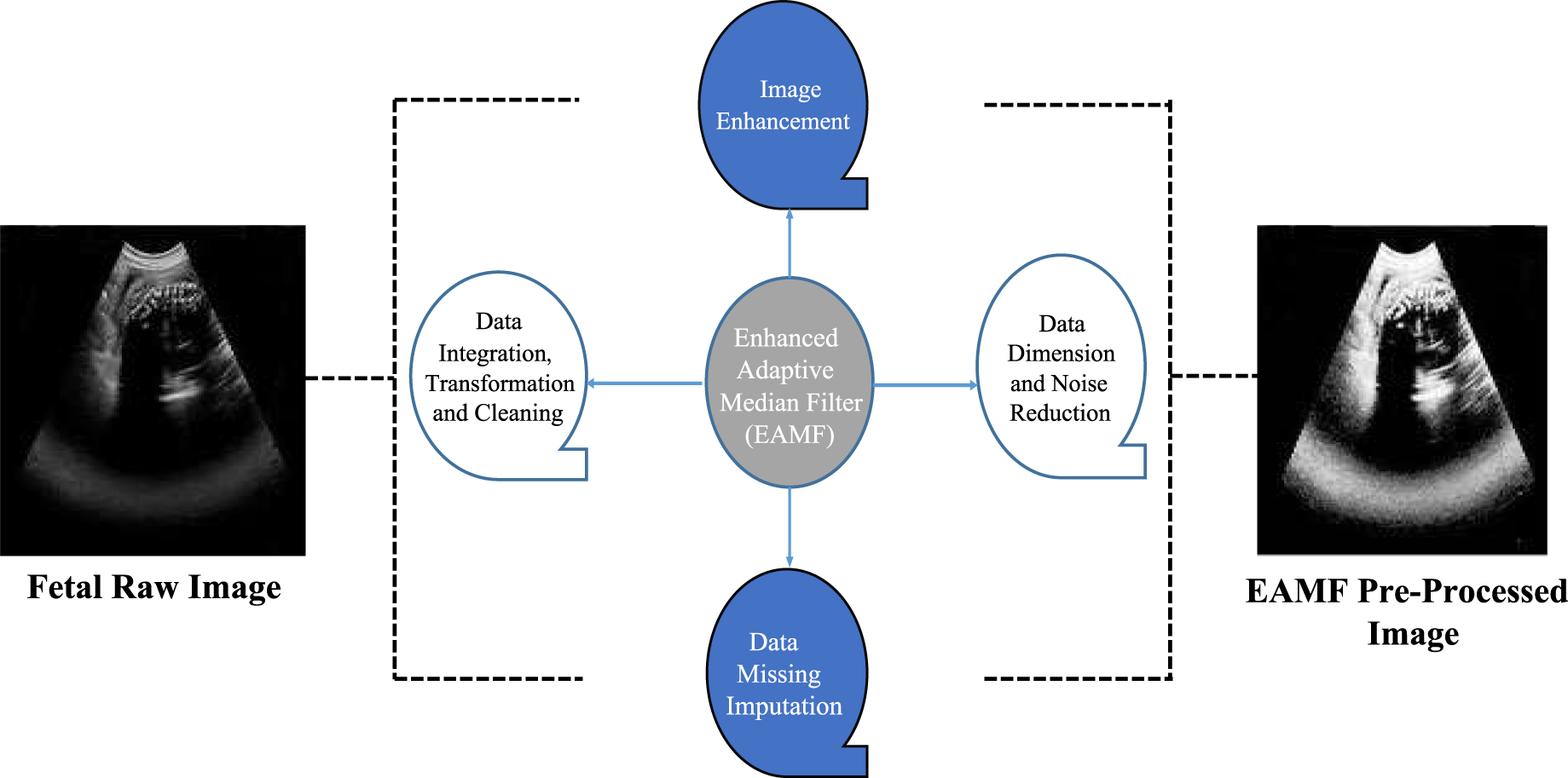
Preliminary de-noising via enhanced adaptive median filter.
The current research survey with investigative meta-heuristic learning algorithms reveals that Region of Interests segmentation yields foetal traits with an appropriate level-set,40–42 where it applies optimum entropy to segment and locate the lesion region via the bounding box with its measuring defect size. The proffered IROI task selection segments the pre-processed grey-scale foetal data by masking the fetal plane and labels via ground-truth box regression of X and Y offset, discriminating the primary features (i.e., diseased area) from the background image appended in the four-chamber and three-vessel regions as enumerated in Figure 5. In afflicted regions, IROI estimates the following parametric measures as illustrated in equations (2–4).




IROI fetal feature segmentation.

Functional design of multiresolution deep convolutional neural network in detection of FHD.
In accordance with medical imaging and heath-care processing, MDCNN is designed to optimize prenatal ultrasound-screened images improving the pixel's intensity and accuracy in the tumor region to detect and anticipate FHD abnormalities alongside risk factors. DCNN tunes the segmented image in the solution space appropriately delineating the erroneous pixels in the IROI fetal heart. This tuning strategy capitalizes the segmented pixel size and shape to cluster the aligned fetal masking and evaluates the acquired findings in extraction of the image features with high spatial and temporal traits retaining the feasible prenatal images. The propounded Multiresolution DCNN is accomplished via three distinct phases 1. Designing the feed-forward input train, 2. Calculating errors via backpropagation, and 3. Adjusting the weights. Figure 6 depicts the architectural design of MDCNN in feature extraction and classification of three pertinent layers: input, hidden, and output. The input bias neurons put forward the streamlining training process in the hidden layer which involves the Convolution Layer (CL) incorporating Pooling (PL) with subsequent ReLu activation, following the flattened resultant (output) - Fully Connected (FC) and softmax. The preliminary feature extraction is carried out by the initial convolution layer integrating 64 convolutional filters with the eventual convolutional kernel size of 7 × 7. Equation (5) showcases the CL extraction of fetal features for the appropriate kernels.

The aggregate volume of image attributes extracted based on convolution kernels fluctuates via backpropagation enumerating the matrix feature and the augmented traits are subjected to weight computation determining the target threshold. The segmented samples are then varied in a rising monotonic mode by the ReLU-stimulated activation function which mitigates the response of the convolution. The attenuated data from the interim ReLU is processed via a 3 × 3 pooling layer in striding the dimensions of the feature maps spatially and lessens the overfitting issue using the PL algorithm. Triumphing the initial stage of conv 1 and pooling, the estimated residual blocks delineate the continual workflow similar to that of the training phase. After the final residual stage, the FC layer with integrated softmax is applied depicting the final class predictions and the classification of the FHD.
The section parts the pseudocode enumeration of the MDCNN simulative design process via defined iteration, create-compilation, training and evaluation as generated below.
Define MDCNN (input_ shape): # Input Layer input_ layer = Input (shape = input_ shape) # Convolutional Layersconv1 = Conv2D (filters = 16, kernel_ size = (3, 3), activation = ‘relu’) (input_ layer)pool1 = MaxPooling2D (pool _size = (2, 2)) (conv1)conv2 = Conv2D (filters = 32, kernel_ size = (3, 3), activation = ‘relu’) (pool1)pool2 = MaxPooling2D (pool_ size = (2, 2)) (conv2)convn = Conv2D (filters = 64, kernel_ size = (3, 3), activation = ‘relu’) (pooln-1)pooln = MaxPooling2D (pool_ size = (2, 2)) (convn-1) # Flatten the output flattened = fc () (pooln-1)# fc_ layer fc1 = fc (128, activation = ‘relu’) (flattened)output_ layer = fc (num_ classes, activation = ‘softmax’) (fc1)# Create the MDCNN model = Model (inputs = input_ layer, outputs = output_ layer)return MDCNN model
Compile MDCNN Model (model):model. compile (optimizer = ‘adam’)
Train MDCNN Model (model, x_ train, y_ train, epochs, batch_ size):model. fit (x_ train, y_ train, epochs = epochs, batch_ size = batch_ size, validation_ check = 3)
Evaluate MDCNN Model (model, x_ test, y_ test):accuracy = model. evaluate (x_ test, y_ test)print (“Test Accuracy:”, accuracy)specificity = model. evaluate (x_ test, y_ test)print (“Test Specificity:”, specificity)sensitivity = model. evaluate (x_ test, y_ test)print (“Test Sensitivity:”, sensitivity)precision = model. evaluate (x_ test, y_ test)print (“Test Precision:”, precision)recall = model. evaluate (x_ test, y_ test)print (“Test Recall:”, recall)
Parametric estimation – MDCNN's confusion metrics
The classification metrics depicted in equations (6–10) evaluate the efficiency of MDCNN via Accuracy (ACC), Specificity (SPC), Sensitivity (SEN), Precision (PRC) and Recall (REC) in explicit to True Positive (TP), False Positive (FP), True Negative (TN), and False Negative (FN) of the disease detection rate i.e., lesion thrive and malignant state.






Fetal ultrasound input images: (a) and (c) four-chamber and bisectional view, (b) and (d) Three-vessel and bisectional view.
The propounded FHD detection is fabricated via MATLAB R2023b with the Indian Institute of Science Fetal Heart Sound Database (IISFHSDB) dataset findings enumerating the simulation outcome of FHD detection. Figure 7 depicts the second trimester's seismic screened four-chamber and three-vessel ultrasound input images of 6 distinct sonographic FHD patients.
Image preliminary de-noising via EAMF
In emerging with the de-noising intensity, the examined fetal heart Ultrasound images are contrasted via preliminary Enhanced-Adaptive Median Filter which envisioned the noise distortion i.e., speckle, Gaussian diminishing sub-ranged background images and improved the image intensity through pixel scaling discrepancies from the modelled fetal dataset. The results of the EAMF contrast-variant image augmentation of the fetal heart's ultrasound four-chamber, three-vessel and its bisectional view are enumerated in Figure 8.

Fetal ultrasound EAMF pre-processed images: (a) and (c) four-chamber and bisectional view, (b) and (d) Three-vessel and bisectional view.
The IROI algorithm erected out the appropriate feature and segmented the foreground disease traits i.e., lesions from the preliminary back-forth image i.e., surrounding intense. The impulsive output image segregation of the relevant structural regions is acquired in Figure 9, where the afflicted region is outlined in the yellow bounding box and the fetal parameters are fabricated from the extracted IROI.

Fetal ultrasound IROI segmented images: (a) and (c) four-chamber and bisectional view, (b) and (d) Three-vessel and bisectional view.
Succeeding with the segmentation phase, the estimated IROI images are delineated to MDRNN which classifies the target-bounded images in agitation with the disease type and efficacy enumerating the normal and abnormal fetal conditions. The MDRNNs categorized findings beneath ultrasound intensity levels in the regional and caudal femur stages with the proximal threshold of stating FHD's Atrial Hemangioma, Aortic Valve Stenosis, ASD, Eisenmenger syndrome, ToF and VSD as laid out in Figure 10 and the propounded simulation findings over the current DL strategies is depicted in Table 3.
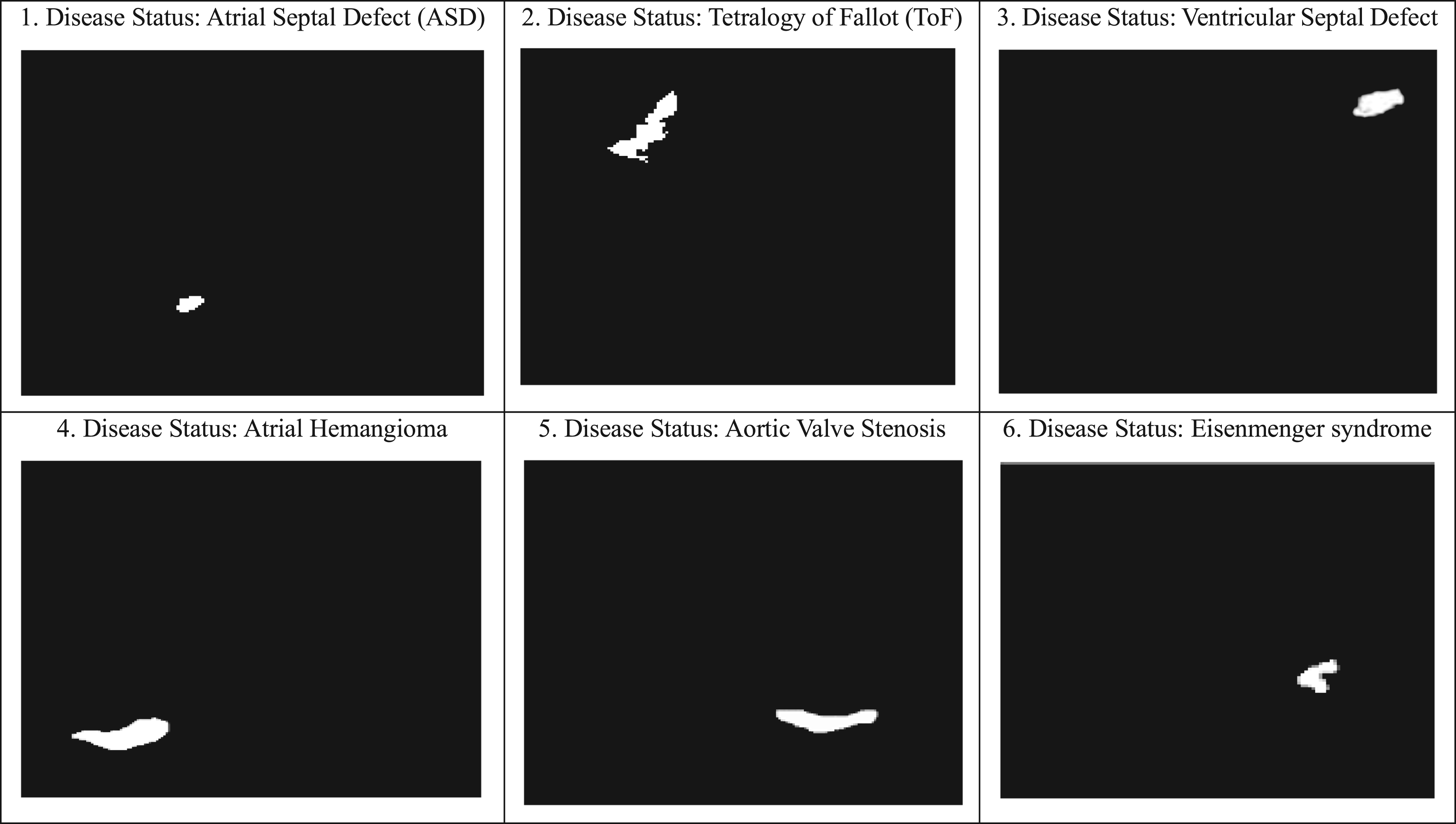
Fetal ultrasound MDCNN output/classified images: (a) and (c) four-chamber and bisectional view, (b) and (d) Three-vessel and bisectional view.
Simulation parameters of IROI combined MDCNN in 4-chamber and 3-vessel over existing algorithms.

Table 3 depicts the distinct parametric values of FHD cases through the direct implementation of the previous research detection models and the proposed system via training-validation data in accumulation to accuracy, sensitivity, specificity, precision and recall, where the Faster-ANN's SMO of FHC dataset, 25 Dense RNN-LSTM of UCI dataset, 30 Semantic Mask RCNN of CAD dataset, 34 Enhanced DL-CNN integrated ROI of CHD dataset 36 are iterated via direct test of IROI combined MDCNN-IIScFHSDB implementation which claimed to best of overall efficacy.
Leveraging the resultant dataset, MDCNN exploits the statistical findings via the parametric measures of Mean Squared Error (MSE) and the regression training rate as rendered in Figure 11(a). The regression state enumerates two sections: 1. input/output replications (i.e., no. of weights and bias length of the stipulated data) and 2. network configuration (i.e., neural systems learning estimation) over train, test and validation generating the best optimal iteration rate at 10−2 MSE approx. The stipulated graph in Figure 11(b) shows the explicit state of MDCNN training in enumeration with the inclusive three tangent functions: the gradient of 5.8929e-06, momentum constant (mu) of 1e-05 and the substantial validation check rate of 3 depicting the onset and re-occurrence of error delineated ideal at epoch level 10.
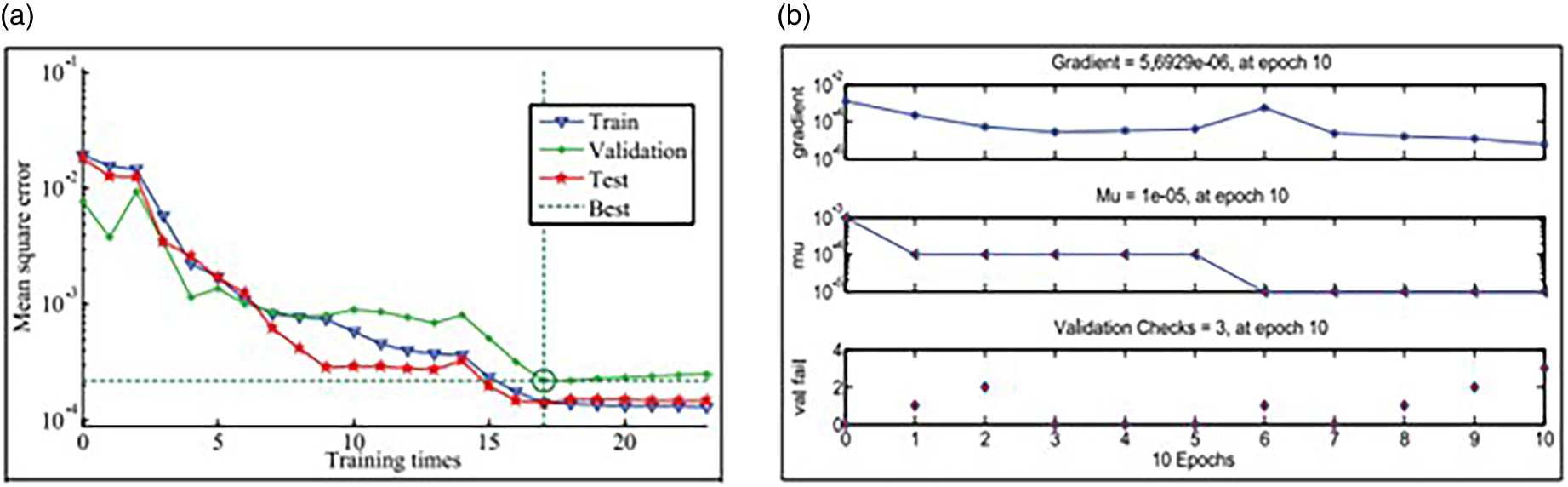
(a) MDCNN training slot. (b) MDCNN Regression Slot.

Neural network acclimation of target and output model.
This stage expedites Neural Network Acclimation (NNC) of the propounded IROI combined MDCNN model in analogue of 2226 fetal image planes classified to train, test and validation sets accommodating 824 (37%), 267 (12%), 178 (8%) 4C images and 646 (29%), 200 (9%), 111 (5%) 3 V images, respective to the prediction data in Table 4. In enumeration with NNC, Figure 12 represents the histogram interpretation of the data-driven correlation variants and coefficients. The X axis depicts the intended (target) dataset while the Y axis depicts the resultant dataset in a straight-linear equation. Inclusively, the dashed line showcases X = Y implying both the intended and resultant data are aligned fictitious with the optimal accuracy of 0.9897 regression (R) nearer to 1. In feasible, the prediction model acquired 99.9065% efficacy at the training phase for abnormal prenatal heart conditions, wherein testing yielded 98.945% efficiency and 98.672% in validation, ideally delineated as blue, red and green strips and iterated with a minimal error score of 5 Bits Per Error Rate (BER), accelerating with the less resolution time of 3 min/sec.
Estimated configuration of training, testing and validation.

Estimated configuration of training, testing and validation.
Fetal or septal heart defect is esteemed to be a grievous dilemma in infants, thus necessities for the early detection and phase-wise treatment of the fetus. In current, the meta-heuristic algorithmic modules of deep learning are one among the imaging methods deployed for embryo-cardiac disease exposure. Triumphing the succession of DL, the propounded research relied on the prognosis of FHD where the input ultrasound image acquisition is preliminarily pre-processed via enhanced adaptive median filter in enumeration with image denoising intensity and fed to the intensified region of interest segmentation which segregated the relevant feature and resolved the spatial traits via ground truth label-offsets and maps the fetal features to multiresolution-deep convolutional neural network classification therein discerned the affiliated lesion with MATLAB R2023b parametric estimation and prognosed FHD of the substantial patients with the optimal 99.715% accuracy, 97.7532% sensitivity, 98.284% specificity, 98.6% precision and 98.324% recall inclusive with IROI iterative measures of 63.192 mean, 62.9637 SD and 7.30228 entropy. The acquired performance has been collated over the current DL algorithms of FANN, DRNN, M-RCNN and EDCNN with high proximal detection. As the impact of the abnormality ailments, FHD patients will be counselled and sessions to diagnose priorly.
Footnotes
Declarations:
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.