
Abstract
Background
Technological advancements have revolutionized the management of acute upper gastrointestinal bleeding (AUGIB). However, the impact of endoscopic timing on treatment outcomes remains a critical area of exploration.
Objective
This study evaluated the role of endoscopic timing in improving treatment outcomes for AUGIB and introduces a predictive model incorporating clinical and technological insights.
Methods
A retrospective analysis of AUGIB patients treated between December 2020 and December 2023 was conducted. Logistic regression identified significant predictors of outcomes, and receiver operating characteristic (ROC) analysis evaluated their predictive value. A predictive model was developed based on these findings.
Results
Among 145 patients, 35 (24.1%) experienced rebleeding. Key predictors included endoscopic timing, active bleeding, shock on admission, and bleeding volume (p < 0.05). The predictive model demonstrated robust performance (C-index: 0.885, 95% CI: 0.810–0.956), emphasizing the clinical relevance of precise timing in endoscopic intervention.
Conclusion
This study underscores the importance of integrating technology with clinical practice to optimize endoscopic timing and improve AUGIB outcomes. The predictive model offers a valuable tool for risk stratification and clinical decision-making in modern healthcare settings.
Keywords
Introduction
Acute upper gastrointestinal bleeding (AUGIB) refers to sudden and severe bleeding originating from the upper part of the digestive tract, which includes the esophagus, stomach, or duodenum. It was reported that it affects approximately 50 to 150 per 100,000 people annually. 1 In addition, severity of the bleeding can lead to significant blood loss and shock, necessitating urgent intervention. With the continuous development of medical technology, endoscopic techniques have gradually attracted widespread attention and are widely used in clinical diagnosis and treatment of AUGIB.
In the present era, endoscopic examination is regarded as the gold standard for the evaluation and treatment of AUGIB.2–5 This is because the endoscopic examination is an effective method for identifying the source and cause of bleeding, and has high clinical value in providing a timely diagnosis and treatment for patients with active bleeding. Effective decision-making is crucial for timely diagnosis, precise risk evaluation, and appropriate resuscitation of patients experiencing gastrointestinal bleeding. 6 Nevertheless, the optimal timing for endoscopic intervention remains uncertain. As evidenced by clinical studies, 10% to 30% of AUGIB patients still experience rebleeding after treatment, with a more dangerous disease progression and significantly increased mortality. 7 The timing of endoscopic treatment is one of the most important factors that can lead to rebleeding after endoscopic diagnosis and treatment. 8 It is therefore of great clinical significance for patients with AUGIB to analyse the factors that affect the outcome of endoscopic treatment and to construct a predictive model of it. These analyses should be based on current recommendations from the European Society for Gastrointestinal Endoscopy (ESGE), which include risk stratification, optimal timing of endoscopy, and guidelines for pharmacological and endoscopic treatment. 9
Variceal bleeding is the main cause of upper gastrointestinal bleeding and is significantly more common in younger patients, who are hemodynamically more unstable due to severe anemia, shock, and hematochezia. 10
Nowadays, there are many risk assessment scores widely applied in clinical practice, such as Rockall score and recently described progetto nazionale emorragia digestive (PNED) score, but they require endoscopy before calculation.11,12 Meanwhile, many studies have compared other pre-endoscopic risk scores, including “admission” Rockall score, Glasgow Blatchford score, AIMS65 score, but they are all weak in predicting rebleeding or length of hospital stay, and uncertainty remains about their exact role in clinical practice.13,14 Therefore, in this study, we retrospectively studied the clinical data of AUGIB patients in our hospital, aiming to explore the relevant factors affecting the treatment outcome of AUGIB patients, and to screen high-risk groups with poor treatment outcomes through the construction of a predictive model, providing reference for clinical practice.
Materials and methods
Study design and population
This study was conducted retrospectively and included patients treated at the Taizhou Municipal Hospital of Zhejiang Province between December 2020 and December 2023. For the conduct of this study, approval was obtained from the hospital's ethics committee, ensuring that the research complies with all ethical standards and regulations, including the protection of patients rights and privacy. Since this study is a retrospective study and the identification information of the patients is anonymous, there was no need for informed consent from the patients and their families. The dataset consisted of two groups: control group and AUGIB case group. All treatment outcomes were recorded in the hospital medical record system and performed by specialists in the hospital. For every patient following information was collected: (1) Basic information: gender, age, history of diabetes, body mass index, hypertension, smoking history, drinking history, family history of diseases, history of peptic ulcers, educational level; (2) Clinical data: active bleeding under endoscopy, bleeding from the lesion, bleeding volume, shock at admission, timing of endoscopic diagnosis and treatment, systolic blood pressure at admission, heart rate at admission, endoscopy time, use of nonsteroidal anti-inflammatory drugs, use of anticoagulant and antiplatelet drugs, site of bleeding.
Inclusion criteria and exclusion criteria
The study included specific inclusion and exclusion criteria to ensure the selection of appropriate patients for analysis
Inclusion criteria: (1) Patients who meet the relevant criteria in the “Guidelines for the Diagnosis and Treatment of Acute Non-Variceal Upper Gastrointestinal Bleeding” 15 and are diagnosed with AUGIB with clinical symptoms such as hematemesis, melena, hematochezia, etc.; (2) Age > 18 years old; (3) Inpatients who underwent endoscopic examination within 24 h; (4) Complete clinical data. Exclusion criteria: (1) Patients with concomitant hematological diseases; (2) Patients with concomitant infectious diseases; (3) Patients who have swallowed bleeding from the oral cavity, nose, respiratory tract, etc.; (4) Patients in whom it is impossible to exclude whether it is lower gastrointestinal bleeding; (5) Patients whose feces are black due to ingestion of animal viscera or iron-containing food; (6) Patients with concomitant organ diseases such as heart, liver, and kidney.
Endoscopic diagnosis and treatment methods
All patients underwent endoscopic hemostasis treatment after admission, and the main treatment methods were: (1) Medication treatment, using hypertonic saline-epinephrine solution for local injection or direct spraying on the lesion; (2) Using microwave or high-frequency electric heat probe for thermal coagulation treatment; (3) Using titanium clips or hemoclips for clipping hemostasis; (4) Combining local injection or direct spraying on the lesion with titanium clips or hemoclips for clipping hemostasis (thermal coagulation treatment using microwave or high-frequency electric heat probe).
Relevant standards for successful hemostasis under endoscopy, rebleeding, diagnosis of hypertension, and diagnosis of diabetes
Criteria for successful hemostasis under endoscopy: Observing the patient's lesion under endoscopy, the bleeding stops, and no bleeding occurs within 5–10 min, and the patient's symptoms improve and vital signs stabilize. 16 Definition of rebleeding: Any of the following conditions occurring within 3 days after successful hemostasis under endoscopy are considered rebleeding: (1) Fresh blood is aspirated through a gastric tube; (2) New onset of hematemesis, increased black stool frequency, and thin stool; (3) Peripheral circulatory failure does not improve significantly after fluid replacement, blood transfusion, etc., or even worsens; (4) Decrease in hemoglobin or red blood cell count; (5) Rebleeding confirmed by endoscopic examination. 17 Criteria for diagnosis of hypertension: According to the diagnostic criteria in the “Chinese Guidelines for the Prevention and Treatment of Hypertension”, systolic blood pressure > 140 mmHg, diastolic blood pressure > 90 mmHg. 18 Criteria for diagnosis of diabetes: According to the diagnostic criteria in the “Chinese Guidelines for the Prevention and Treatment of Type 2 Diabetes”, symptoms such as polyuria, polyphagia, polydipsia, weight loss, etc., fasting blood glucose ≥ 7.0 mmol/L, random blood glucose ≥ 11.1 mmol/L. 19
Statistical analysis
Statistical analysis was performed using IBM Statistic Package for Social Science (SPSS) Statistics for Windows version 27.0 (IBM Corp., Armonk, NY, USA). Measurement data that followed a normal distribution were expressed as mean ± standard deviation (SD), and t-test was used. Data that did not follow a normal distribution were expressed as M (Q1, Q2), and z-test was used. Count data were expressed as n (%) and analyzed using chi-square test, with p < 0.05 indicating a statistically significant difference. Logistic regression analysis was used to analyze the influencing factors of treatment outcomes in AUGIB patients, and the predictive value of each factor for treatment outcomes was observed by plotting receiver operating characteristic (ROC) curves. R package “rms” was used to plot column line graphs to construct the predictive model.
Results
Analysis of treatment outcomes
According to the medical record system, 35 out of 145 AUGIB patients experienced rebleeding after treatment, accounting for 24.14% (35/145), and were assigned to the case group. 110 patients did not experience rebleeding after treatment, accounting for 75.86% (110/145), and were assigned to the control group.
Univariate analysis of treatment outcomes in AUGIB patients
There were significant differences between the two groups of patients in terms of bleeding volume, active bleeding under endoscopy, shock at admission, bleeding from the lesion, and timing of endoscopic diagnosis and treatment (p < 0.05), as shown in Table 1. These findings highlight the importance of promptly addressing the various clinical indicators in managing AUGIB, as they significantly impact the patient's recovery and prognosis.
Baseline characteristics of AUGIB patients.

Baseline characteristics of AUGIB patients.
Note: *P < 0.05, indicates a statistically significant difference.
The assignment of independent variables is shown in Table 2. In this analysis, several clinical factors were assigned as independent variables to assess their potential influence on treatment outcomes in AUGIB patients. These factors included active bleeding observed during endoscopy, bleeding originating from the lesion, bleeding volume, shock at admission, and the timing of endoscopic diagnosis and treatment. Each of these variables was considered individually to evaluate its contribution to the overall prognosis and response to treatment. The assignment of these variables allowed for a more detailed examination of how each factor interacts with the others and their collective impact on patient outcomes.
Assignment of independent variables.

Assignment of independent variables.
Logistic regression analysis was performed on the variables that showed significant differences. Active bleeding under endoscopy, bleeding from the lesion, bleeding volume, shock at admission, and timing of endoscopic diagnosis and treatment were all risk factors for treatment outcomes in AUGIB patients, with OR values > 1, as shown in Table 3.
Multivariate binary logistic regression analysis of treatment outcomes in AUGIB patients.

Multivariate binary logistic regression analysis of treatment outcomes in AUGIB patients.
Note: *P < 0.05, indicates a statistically significant difference.
As shown in Table 4 and Figure 1, the AUC values of active bleeding under endoscopy, bleeding from the lesion, bleeding volume, shock at admission, and timing of endoscopic diagnosis and treatment were 0.638, 0.632, 0.824, 0.613, and 0.809, respectively. The sensitivity was 0.657, 0.629, 0.886, 0.571, and 0.629, and the specificity was 0.618, 0.636, 0.700, 0.655, and 0.836. The 95% CI was 0.532∼0.743, 0.526∼0.739, 0.741∼0.907, 0.505∼0.721, and 0.724∼0.894, respectively. These results indicate that the above factors have a certain predictive value for the treatment outcome of AUGIB patients. Based on the above analysis results, a column line graph was plotted using R package “rms” to construct a predictive model for the risk of poor treatment outcomes in AUGIB patients, and the C-index of the predictive model was 0.885 (95% CI: 0.810–0.956), indicating a relatively high predictive value for the predictive factors, as shown in Figure 2.
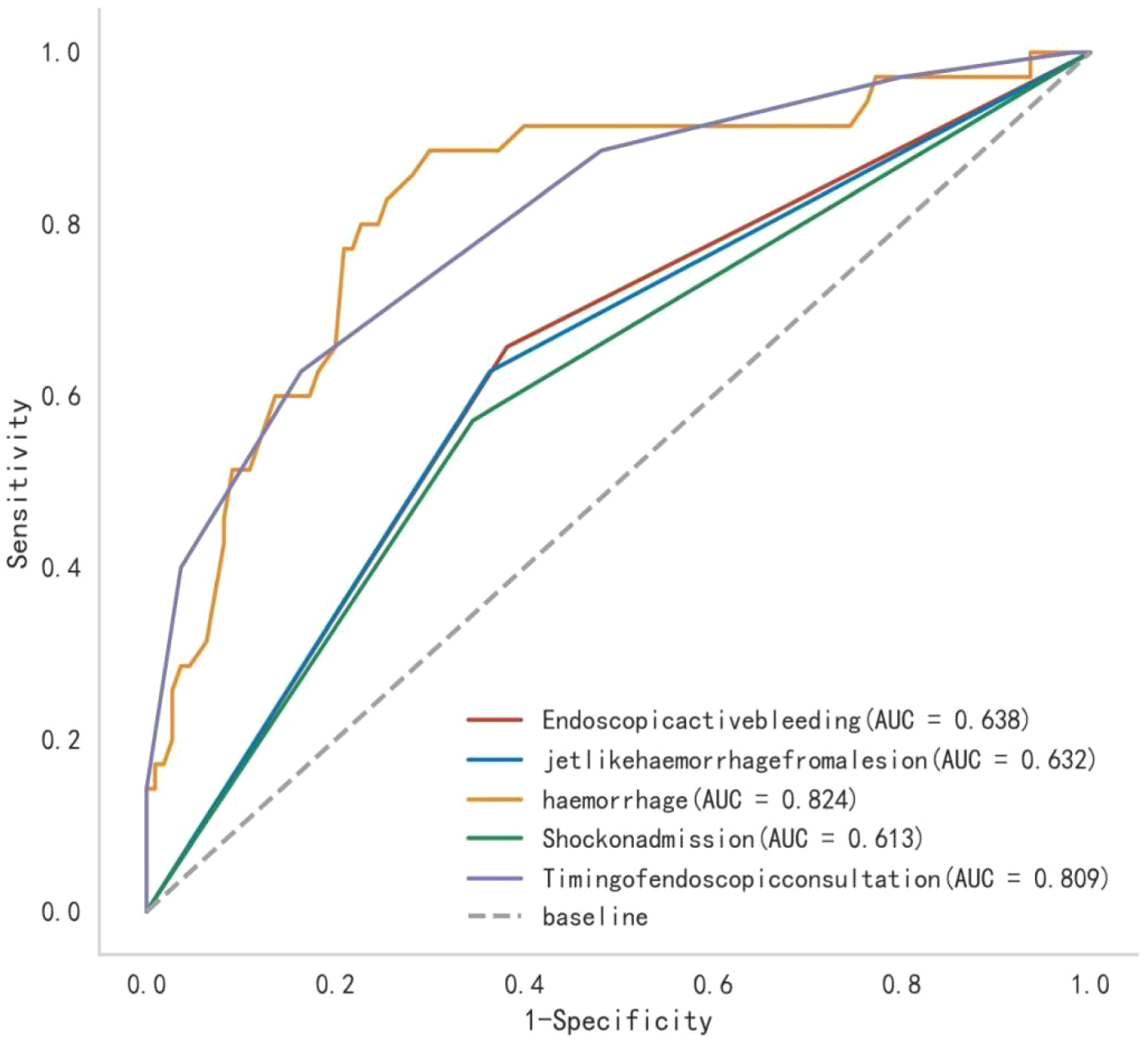
Predictive value of each factor for treatment outcomes in AUGIB patients.

Construction of the predictive model for treatment outcomes in AUGIB patient.
Predictive value of each factor for treatment outcomes in AUGIB patients.

The advantages of endoscopic technology for AUGIB have been widely acknowledged, for allowing both diagnosis and treatment.20,21 However, data shows that although endoscopic treatment for AUGIB has good efficacy, patients are still affected by some related factors, leading to poor treatment outcomes and recurrent bleeding.21,22 The data in this study showed that among 145 AUGIB patients treated with endoscopy, 35 patients experienced recurrent bleeding, accounting for 24.14%, which is consistent with other related reports. This further indicates that it is necessary to analyze the factors affecting treatment outcomes in AUGIB patients and screen the high-risk population.
There were significant differences in active bleeding, spurting bleeding, bleeding volume, and shock at admission between the two groups of patients, and all these indicators were risk factors for treatment outcomes in AUGIB patients, with OR values greater than 1. The AUC values of active bleeding, spurting bleeding, bleeding volume, and shock at admission were 0.638, 0.632, 0.824, and 0.613, respectively. The sensitivities were 0.657, 0.629, 0.886, and 0.571, and the specificities were 0.618, 0.636, 0.700, and 0.655. The 95% CI values were 0.532–0.743, 0.526–0.739, 0.741–0.907, and 0.505–0.721. This indicates that active bleeding, spurting bleeding, bleeding volume, and shock at admission are all important influencing factors for the treatment outcomes of AUGIB patients, and they have high predictive value. Cameron EA et al. 23 also found through clinical research that some AUGIB patients would experience poor treatment outcomes due to various factors during endoscopic treatment. Active bleeding during endoscopy indicates continuous and difficult-to-control bleeding, which increases the amount of bleeding and worsens the patient's condition. Spurting bleeding refers to the phenomenon of large and jet-like bleeding in the lesion area. A large bleeding volume indicates rupture of the blood vessel wall and damage to the surrounding tissues, leading to a large consumption of platelets and coagulation factors, making the patient's blood vessels more fragile during the recovery period, and the risk of rebleeding is relatively higher after treatment. Shock at admission in AUGIB patients is usually caused by insufficient blood volume, hypotension, and circulatory failure due to massive bleeding, indicating a more severe disease progression and a higher risk of rebleeding after treatment. Previous studies have shown that AUGIB patients who experience active bleeding, spurting bleeding, bleeding volume, and shock at admission during endoscopic treatment have a higher risk of recurrent bleeding, which significantly affects the treatment outcomes of patients.24,25 Therefore, combined with the above studies and the results of this study, it can be concluded that these factors are all important factors affecting the treatment outcomes of AUGIB patients, and they reflect the patient's disease progression significantly. By observing whether the above conditions occur before treatment, the high-risk population for recurrent bleeding can be screened, and timely intervention measures can be taken to effectively improve the treatment outcomes.
In our study, there were significant differences in the timing of endoscopic treatment between the two groups of patients, and this indicator was a risk factor for treatment outcomes in AUGIB patients, with an OR value greater than 1. The AUC value of the timing of endoscopic treatment was 0.809, with a sensitivity of 0.629 and a specificity of 0.836. The 95% CI was 0.724–0.894. This indicates that the timing of endoscopic treatment is an important influencing factor for the treatment outcomes of AUGIB patients and has high predictive value. Mackiewicz-Pracka A et al. 26 also conducted a study and found that endoscopy is an important method for clinical diagnosis and treatment of AUGIB patients, which has a significant impact on the treatment outcomes of patients, consistent with the results of this study. Previous studies have shown that endoscopic examination can accurately locate the source of bleeding in patients, and early endoscopic treatment can timely perform hemostasis treatment, reduce bleeding volume, prevent severe bleeding complications, and evaluate the risk of recurrent bleeding in patients by observing the bleeding location and vascular lesion causes, thereby effectively taking corresponding clinical measures to prevent rebleeding.4,27 AUGIB patients experience acute bleeding due to lesions in the esophagus, stomach, and other parts. When the timing of endoscopic treatment is delayed, the bleeding source in patients cannot be located in a timely manner, and the nature and severity of the bleeding lesion cannot be effectively evaluated, which affects the doctor's formulation of reasonable treatment and prevention measures, leading to poor treatment outcomes. Moreover, logistic regression analysis was used to analyze multiple factors, and the predictive value of each factor for treatment outcomes was found through ROC curve analysis. A predictive model was constructed by drawing a column chart, and the results of the column chart showed that the constructed predictive model had a high predictive value for the treatment outcomes of AUGIB patients, providing substantial support for clinical practice and having certain clinical significance.
However, the study is subject to the following recognized limitations. Firstly, this study is a retrospective study design, which may have potential confounding factors and information bias. Secondly, this study is a small sample, single-center design, and the research was conducted only in a specific medical institution, which may limit the generalizability of the research results to other medical institutions with different backgrounds. Finally, this study selected AUGIB patients treated in the hospital from December 2020 to December 2023, resulting in sample limitations. In future research, we can overcome the limitations of this study by using more refined designs, conducting multicenter and large-sample designs to comprehensively consider these factors, and establish more accurate predictive models. Although this study has the above limitations, it still provides substantial support for the relevant factors affecting the treatment outcomes of AUGIB patients.
Conclusion
In conclusion, several factors significantly influence the treatment outcomes of patients with AUGIB. This study highlighted five key factors: active bleeding, spurting bleeding, bleeding volume, shock at admission, and the timing of endoscopic intervention. Each of these factors independently impacts patient outcomes, providing valuable predictive information for clinicians. Active or spurting bleeding is indicative of more severe cases, while larger bleeding volumes and shock upon admission signal higher risks of complications. Early endoscopic intervention is critical for improving outcomes, as timely diagnosis and treatment reduce the likelihood of rebleeding. The combination of these factors can be used to develop a predictive model that effectively identifies high-risk patients, allowing for targeted interventions. By utilizing such a model, healthcare providers can improve clinical decision-making, enhance patient care, and potentially reduce mortality rates in AUGIB cases.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.