
Abstract
Background
Orthodontic clear aligners are a technologically advanced treatment modality that improves aesthetics and comfort while impacting patients’ oral health-related quality of life (OHRQoL).
Objective
This study assessed and compared the OHRQoL of adult orthodontic patients receiving clear aligners and fixed appliances (metal and ceramic brackets) during orthodontic treatments.
Methodology
One hundred and five orthodontic patients were recruited and classified according to the treatment received. Group 1 clear aligners, group 2- fixed appliances/metal brackets, and Group 3-fixed appliances/ceramic brackets. The patients were surveyed using an Arabic version of the Oral Health Impact Profile 14 (OHIP- 14) questionnaire before (T0), 1-week (T1), and 3-months (T2) after the start of orthodontic treatment. Data was analysed using SPSS software at a significance level set at ≤0.05.
Results
The mean OHIP scores showed no significant difference between the 3 groups at T0 (p = 0.09) and T2 (p = 0.41) time intervals. On the contrary, the mean OHIP scores at T1 significantly differed between 3 groups (p = 0.03). The mean OHIP scores within the groups at different time intervals was significantly different. Multiple comparison within the groups showed significant reduction in the mean OHIP scores from T0 to T1 and T2 period and further from T1 to T2 period, and the mean differences were statistically significant (p < 0.001).
Conclusion
Adult patients treated with clear aligners had significantly higher OHRQoL than those who underwent conventional fixed bracket-based treatment after 7 days of treatment but OHRQoL was similar after three months of treatment.
Introduction
Malocclusion is the second most prevalent oral health concern that impairs dentofacial aesthetics and affects speech in addition to influencing functional needs and general psychological health.1,2 This can have a profound impact on an individual's ability to express themselves and relate with others. Thus, the oral cavity is regarded as a significant landmark that influences the overall quality of life. 3 Malocclusion-related dentofacial concerns and patients’ psychological states during orthodontic treatment have an impact on quality of life. 4
Since the inception of the orthodontic specialty, orthodontic appliances to treat malocclusion have undergone a significant transformation, but this rate has increased sharply in recent years due to a rise in the number of adult orthodontic patients and their aesthetic demands.5,6 The most popular orthodontic appliance therapy for many years was metal brackets. 7 There is a growing need for less noticeable orthodontic appliances as an alternative to conventional fixed appliances because not all patients are comfortable with conventional metal or ceramic brackets. 8 The goal of orthodontic treatment, regardless of the appliance type, is to assist in achieving a harmonious facial appearance and a healthy, functional, and aesthetically pleasing occlusion that will be comparatively stable over time. 8 However, the clinician needs to consider the patient-centered effects of orthodontic treatment in addition to the final occlusal and aesthetic outcome. 5
Over the past two decades, contemporary orthodontics has advanced significantly owing to new materials and innovative treatment approaches. 9 The incorporation of technologies like Computer-Aided Design (CAD) and computer-aided Manufacturing (CAM) has further streamlined the direction of orthodontic treatments. 10 Consequently, orthodontic practices have embraced a more effective and cost-efficient approach to patient care. 11 Specifically, one of the latest innovations, the clear aligner, is becoming more popular since it provides a more comfortable, hygienic, and aesthetically pleasing alternative to conventional orthodontic treatments. 12 Clear aligner explicitly serves adult patients who have high regard for appliance aesthetics and inconspicuousness due to rising living standards and competitiveness in recent years. 13 These aligners are not just a trend but a personalized solution that acknowledges an individual's aesthetic demands. Over the past decade, there has been a notable increase in the demand for clear aligner therapy (CAT). 10
Kesling was the first to propose the concept of aligners in 1946 to correct misaligned teeth. 14 His pioneering work and the introduction of CAD/CAM technology played a crucial role in the evolution of modern-day clear aligners in orthodontics. In 1998, Align Technology, Inc. introduced Invisalign®, the first modern-day clear aligner. In CAT, a set of removable, transparent, flexible plastic aligners is used to generate the force necessary for tooth movement. 15 Initially, CAT was used to treat minor crowding or spacing. However, the application of clear aligners has significantly expanded in routine dental practice with the advancement of novel materials and the continued development of CAD/CAM technology. 16 Compared to the conventional fixed appliance treatment (FAT), these aligners have been demonstrated to be more comfortable and aesthetically acceptable while providing the benefits of orthodontic adjustments. 17
On the contrary, a recent systematic review concluded that the current evidence supporting the therapeutic efficacy of CAT in comparison to conventional FAT and the predictability of tooth movements is slight to moderate. The study further confirmed that although complex malocclusions can be treated with CAT, FATs typically produce more precise outcomes. 18 It is quite debatable whether clear aligners are an effective alternative for FAT. Consequently, practitioners developing treatment strategies rely mainly on clinical expertise and substandard evidence.
Oral health is no longer defined merely by the absence of illnesses and dysfunction, 19 but rather should include both a positive sense of dentofacial self-confidence and the lack of detrimental effects of oral disorders on social life.5,20 Malocclusion has a negative impact on OHRQoL, 21 but orthodontic therapy can enhance this condition, subsequently improving OHRQoL. 22 Clinicians have recently emphasized the importance of patient perception in order to understand patients’ needs, measure their level of satisfaction with the treatment, and evaluate their overall health. 23 OHRQoL assessment represents an individual's subjective viewpoint by reflecting how their oral health state interacts with social and contextual factors.24,25 The use of OHRQoL measures has significant implications for clinical practice, research, and public health. 26
The Oral Health Impact Profile (OHIP) is the most widely used tool both by clinicians and researchers to measure the OHRQoL.27,28 In 1994, Slade and Spencer 29 used the original Australian data set of people to develop and assess the OHIP, which has 49 questions (OHIP-49). The 49 items are distributed, taking into account the seven dimensions of life that were created using Locker's theoretical model. 30 Although the OHIP-49 is widely used, its practicality in epidemiologic and clinical studies is limited by the vast number of items and the time necessary to complete it. In order to address the same concepts as the full version of OHIP but in less time, specific condensed versions, like the OHIP-14, were developed.27,31 Previous studies comparing the OHRQoL of patients treated with CAT and FAT have demonstrated inconsistent outcomes,4,5,32–37 and the quality of the exploratory evidence recommends conducting more high-quality clinical studies to derive more robust conclusions.
Consequently, this study assessed and compared the OHRQoL of adult patients undergoing orthodontic treatment by CAT or FAT (metal and ceramic brackets) before (T0) and 1-week (T1) and 3-months (T2) after the start of orthodontic treatment using validated OHIP-14 questionnaire. The null hypothesis is that there is no significant difference in the OHRQoL between the orthodontic patients receiving clear aligners versus fixed appliances at different assessment times. The potential impact of our findings could provide insights into the patient's perception of CAT and FAT, which may influence the choice of orthodontic treatment for adult patients.
Methodology
This clinical observational study was conducted to assess and compare the oral health related quality of life outcomes of patients undergoing orthodontic treatment by clear aligners or conventional fixed orthodontic therapy, either by metal or ceramic brackets utilizing a standardized self-explanatory questionnaire at different treatment time.
Sample size
The sample size was calculated using the free, web-based platform (https://www.openepi.com) based on previous study. 38 Considering 95% CI, p = 0.06 and error margin = 0.05, the sample size (N) was estimated to be 86.66, which was rounded off to 90. Nevertheless, the study enrolled 105 patients to compensate for any dropout or follow-up loss of the patients. These sample size was divided into 3 groups, comprising of 35 each (n = 3).
Ethical considerations and informed consent
The study protocol is in accordance with the 1964 World Medical Declaration of Helsinki as amended in 2013. The study is also approved by the Institutional Review Board (IRB) at Riyadh Elm University (“FRP/2024/534/1112/1000”). Informed consent was obtained from all participating patients before their inclusion in the study, ensuring transparency regarding the study objectives, procedures, and potential risks.
Patient inclusion and exclusion criteria
The following patients were included; (a) adult patients (>18 years) who were medically fit and healthy with no contraindication to orthodontic treatment, (b) class I malocclusion with mild crowding (2–4 mm), (c) non-extraction cases, (d) maintaining good oral hygiene and oral health (free from caries or periodontal disease). On the contrary, any patients with an orthognathic profile, previous history of orthodontic treatment, presenting systemic disease, irregular/ uncooperative, or who refused to sign the consented form were excluded from the study.
Patient grouping and treatment information
One hundred and five orthodontic patients who required orthodontic treatment either by clear aligners or conventional fixed appliances (metal or ceramic brackets) were recruited in this study from two different centres. The patients were allocated to three groups:
Group 1: Clear aligners (n = 35 patients). Group 2: Conventional fixed appliances/metal brackets (n = 35 patients). Group 3: Conventional fixed appliances/ ceramic brackets (n = 35 patients).
Before the start of orthodontic treatment, the pre-operative diagnostic models, radiographs and photographs were obtained for all the patients and the treatment was performed by experienced orthodontists.
Group 1: clear aligners
The patients’ digital models were imported into ClinCheck® software (Align Technology, Inc., Tempe, Arizona, USA) to create a treatment schedule. For every patient, a set of personalized clear aligners (Invisalign, Align Technology, Inc., Tempe, Arizona, USA) were fabricated. The patients were instructed to change their trays every two weeks and wear their aligners for 22 h daily. Patients underwent evaluations every four weeks. If necessary, refinement aligners were provided. To ensure proper aligner fit and stable attachment, it was crucial for each patient to cooperate by following the treatment plan and attending follow-up appointments every 4–8 weeks (for 2–4 aligners).
Group 2: conventional fixed appliances/metal brackets
This group's maxillary and mandibular teeth were fitted with metal orthodontic brackets (Miniature Twin, 0.018 in, MBTTM or Roth prescription, 3MTM UnitekTM, St Paul, MN, USA). NiTi arch wires measuring 0.014 and 0.016 inches were used for alignment and levelling. Stainless steel or elastic ligatures were used to ligate the archwire to the brackets. The patients in this group were recalled every 3–4 weeks to monitor their treatment and make any required activations or modifications. Archwires were changed when crowding started to reduce, and it seemed possible to place the next archwire without unnecessarily straining the engaged teeth.
Group 3: conventional fixed appliances/ ceramic brackets
The patients in this group underwent a similar treatment procedure as in group 2 except for the orthodontic brackets used. Ceramic orthodontic brackets (Clarity™ Advanced, 0.018 in, MBT™ or Roth*, High torque prescription, 3M™ Unitek™, St Paul, MN, USA) were used for orthodontic bonding.
Oral health impact profile (OHIP) questionnaire
The OHIP-14 instrument was utilized to evaluate the effects of clear aligners versus fixed orthodontic treatment, either metal or ceramic brackets on OHRQoL. The 14 questions were developed considering the three aspects of life—physical, psychological, and social—distributed across seven domains: handicap, social disability, physical disability, psychological discomfort, physical pain, and functional limitation. 2 The participants were required to respond to the questions on a 5-point Likert scale, where 0 -never, 1 -seldom, 2 -sometimes, 3 -frequently, and 4- always. The scale measures how frequently an individual experiences the impact of oral health on seven OHIP domains. Each doamin is assigned a score from 0 to 8. The total score of the OHIP-14 ranges from 0 to 56 and is calculated by adding up the responses to the 14 questions. The individual's perception of their OHRQoL is inversely related to the score.2,27
The questionnaire was distributed to the patients during their routine orthodontic visits via free-access Google forms (Google LLC, Menlo Park, California, USA), which facilitate patient communication and data encoding. The questionnaire comprised of two parts, the first part included questions about the participant's demographic and general aspects such as age, gender, educational level, and family income.2,39–41 A family's monthly average income in Saudi Arabia is 10,000 Saudi Arabian Riyals (SAR), according to the country's general statistics authority. 39 Based on that, the income was divided into three categories: high, average, and low.
The second part contained OHIP −14 questions related to the oral health impact on orthodontic treatment. The Arabic version of the OHIP-14 questionnaire which was previously validated,
2
was used in this comparative study. The patients were requested to complete the questionnaire at three different times:
T0: Before the start of orthodontic treatment. T1: After 1 week of orthodontic treatment. T2: After 3 months of orthodontic treatment.
The patients were instructed to answer the questionnaire considering the treatment and the appliances.
Statistical methods
Statistical Package for Social Sciences for Windows v. 22, released 2013 (IBM, SPSS Inc., Armonk, NY, USA) was used for analysing the data. Descriptive analysis of the explanatory and outcome parameters was presented as mean and standard deviation (SD) for continuous variables and as frequency and proportions for categorical variables.
For the inferential statistics, Kruskal Wallis test followed by Dunn's post hoc test was used to compare the mean age and OHIP scores between the groups. Chi square test was used to compare the gender distribution, and socio-demographic characteristics between the groups. Friedman's Test followed by Wilcoxon Signed rank post hoc test was used to compare the mean OHIP scores at different time intervals in each group. The level of significance was set at p < 0.05.
Results
This comparative study assessed the impact of clear aligners versus fixed orthodontic treatment on the OHRQoL of the patients utilising the OHIP-14 questionnaire. Among the patients who were recruited to this study, one patient was lost to follow-up in group 1, one patient was lost to follow-up, one patient discontinued treatment in group 2, and two patients were lost to follow-up in group 3. Finally, the patients available for final analysis were n = 34, n = 33, and n = 33 in group 1, group 2, and group 3, respectively.
The age of the orthodontic patients in this study ranged between 18–48 years. The mean age was 27.12 ± 6.18 years, 26.85 ± 7.48 years and 26.61 ± 6.04 years for group 1, group 2 and group 3 patients, respectively. The mean age was comparable between the groups (p = 0.81) (Table 1).
Mean age of the patients in the study groups.

Mean age of the patients in the study groups.
Group 1- Clear aligners; Group 2- Metal brackets; Group 3- Ceramic brackets.
Table 2 compares the socio-demographic characteristics of the patients in study groups. The sex distribution of the patients was comparable between the groups (p = 0.07). Similarly, no significant difference was observed in the patients’ educational level between 3 groups (p = 0.30). Around 70% of the patients had completed college education, while 26% completed high school and 4% had completed secondary school. The family income of the subjects in group 1 and group 2 was predominantly average (55.9% and 48.5%) compared to those in group 3, where the family income was predominantly low (42.4%). This proportional difference in the family income between the 3 groups was statistically significant at p = 0.02.
Comparison of socio-demographic characteristics between three groups using chi square test.

Group 1- Clear aligners; Group 2- Metal brackets; Group 3- Ceramic brackets.
*Statistically significant (p < 0.05; bChi Square Test).
The mean OHIP scores of the 3 groups at different measurement intervals are presented in Figures 1–3. The mean OHIP scores showed no significant difference between the 3 groups at T0 (p = 0.09) and T2 (p = 0.41) time intervals. On the contrary, the mean OHIP scores at T1 significantly differed between 3 groups (p = 0.03). Multiple comparisons between groups revealed that the mean OHIP scores were significantly lesser in group 1 as compared to group 2 and group 3, and the mean differences were statistically significant (p = 0.01 and p = 0.04, respectively). The mean OHIP scores did not show a significant difference between group 2 and group 3 (p = 0.34).

Aspects and dimensions of the oral health impact profile 14 (OHIP-14).
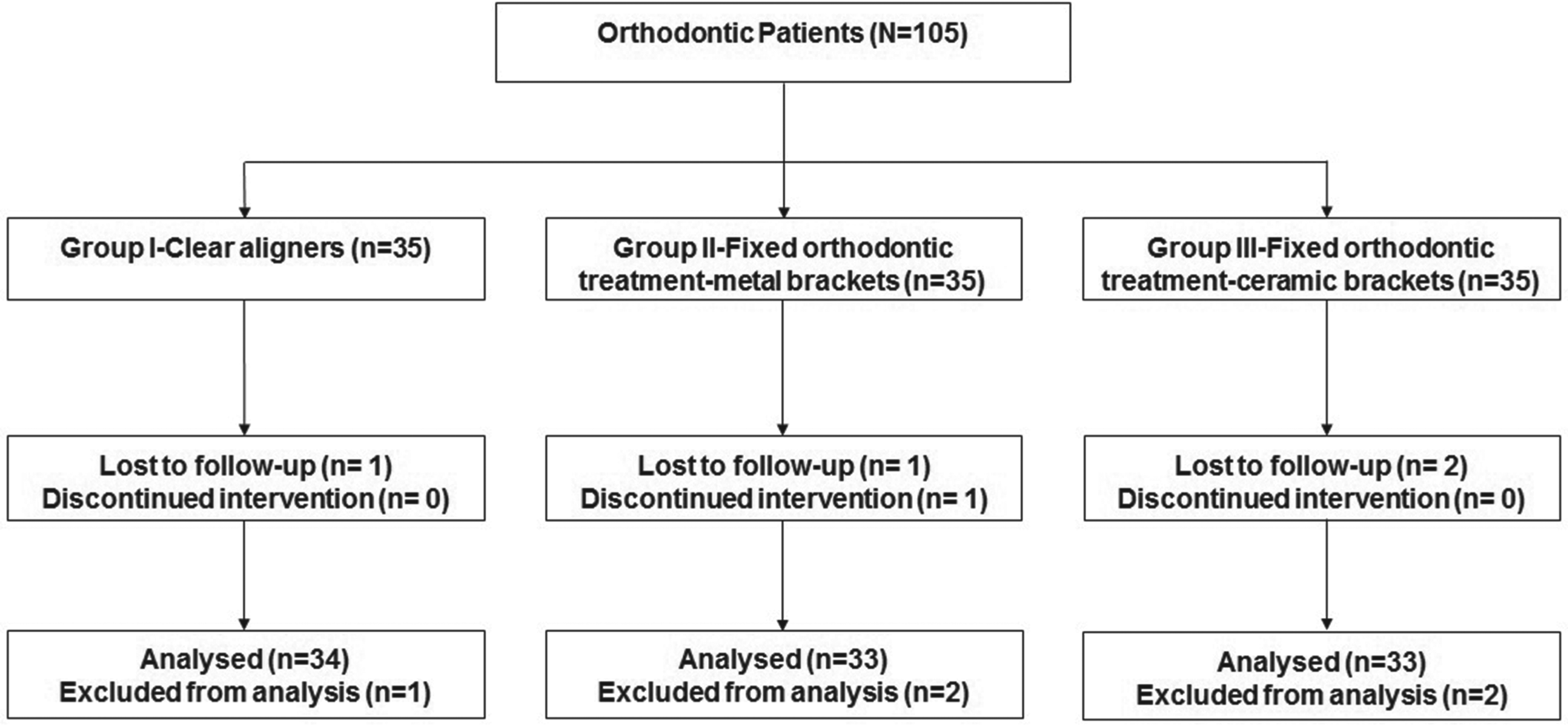
Flow chart demonstrating the study groups and the process.
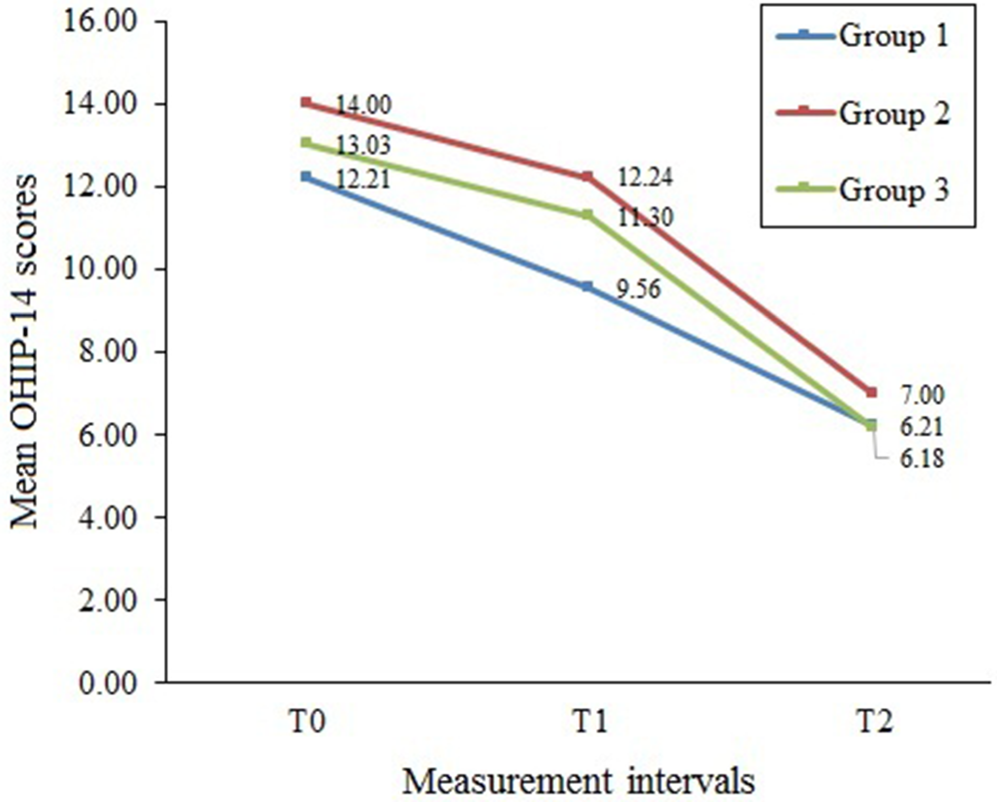
Mean OHIP-14 scores of the study groups at different measurement intervals (group 1: clear aligners; group 2: metal brackets; group 3: ceramic brackets).
Tables 3 and 4 compares the mean OHIP scores within the groups at different time intervals. For all the study groups, the mean OHIP scores showed a significant difference between 3 time intervals, and the mean difference was statistically significant (p < 0.001). Multiple comparisons between time intervals demonstrated that the mean OHIP scores showed significant reduction from T0 to T1 and T2 period and further from T1 to T2 period, and the mean differences were statistically significant (p < 0.001) for all the groups.
Comparison of mean OHIP scores between the groups at different time intervals.
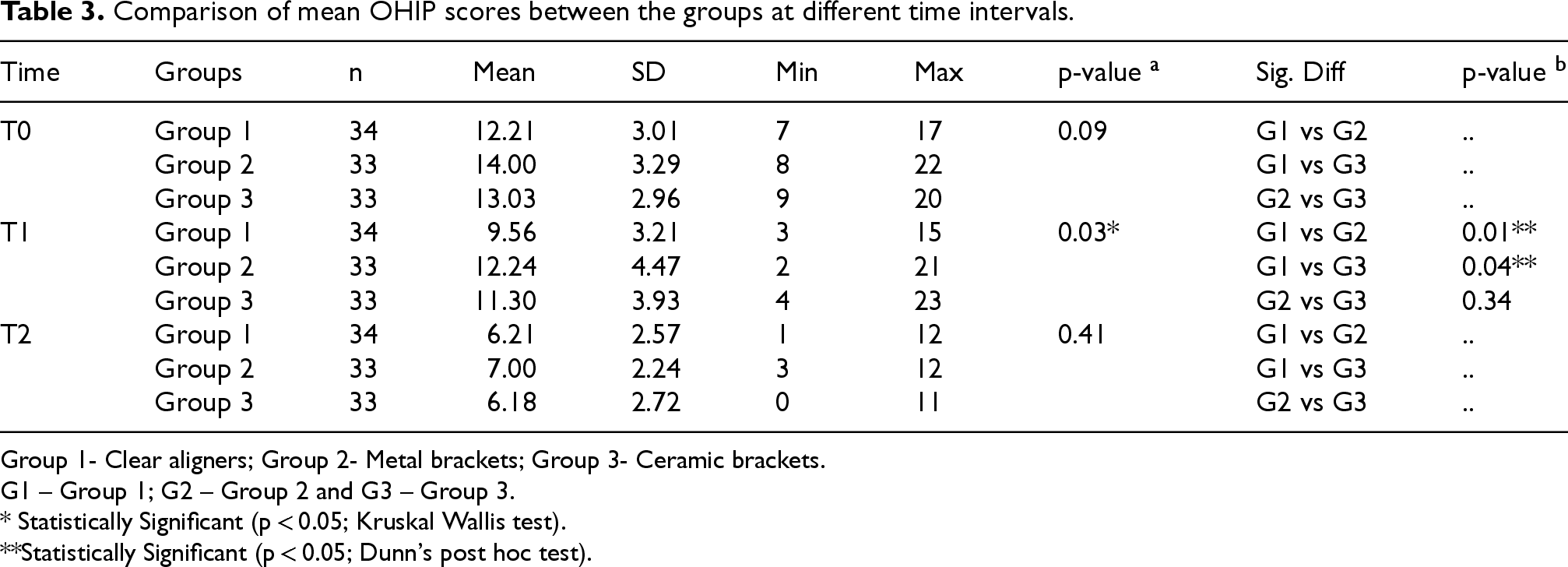
Group 1- Clear aligners; Group 2- Metal brackets; Group 3- Ceramic brackets.
G1 – Group 1; G2 – Group 2 and G3 – Group 3.
* Statistically Significant (p < 0.05; Kruskal Wallis test).
**Statistically Significant (p < 0.05; Dunn's post hoc test).
Comparison of mean OHIP scores within the groups at different time intervals.
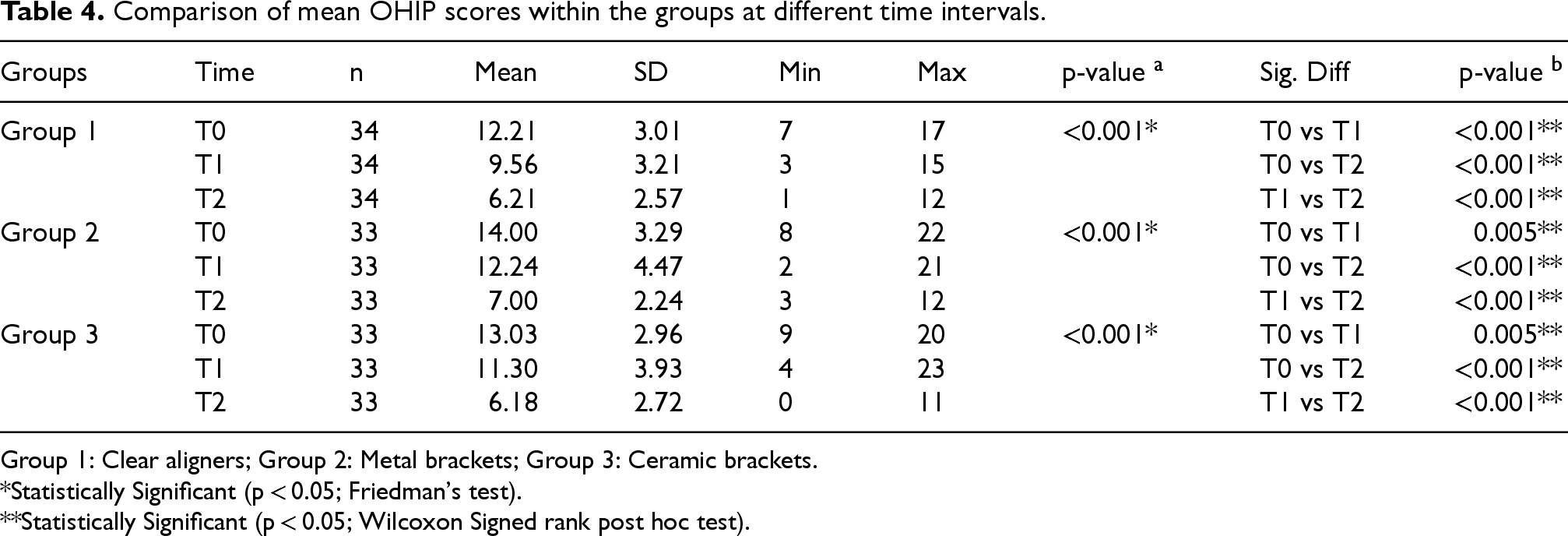
Group 1: Clear aligners; Group 2: Metal brackets; Group 3: Ceramic brackets.
*Statistically Significant (p < 0.05; Friedman's test).
**Statistically Significant (p < 0.05; Wilcoxon Signed rank post hoc test).
The current study compared the OHRQoL of adult patients undergoing clear aligner and fixed appliance treatment with metal and ceramic braces during the initial stages of orthodontic treatment using a validated OHIP-14 questionnaire. It was hypothesized that there would be a significant difference in the OHRQoL between the orthodontic patients receiving clear aligners versus fixed metal and ceramic appliances at different assessment times. The results of the study demonstrate that the mean OHIP scores showed no significant difference between the three groups at T0 (p = 0.09) and T2 (p = 0.41) but significantly differed at T1 (p = 0.03). Thus, the current study outcomes recommend partial rejection of the null hypotheses.
It is increasingly accepted that objective measurements alone cannot fully reflect the impact of malocclusion and orthodontic treatment on patient well-being. 42 In contemporary orthodontics, the OHRQoL has gained significant importance as it details the patient-perceived effects of orofacial disorders and orthodontic interventions. 34 OHRQoL is a multifaceted concept that includes psychosocial factors, functional abilities, pain, and dentofacial aesthetics. 43 Patients’ age, gender, and health, as well as their psychological state and social interactions, all have an impact on the OHRQoL. The way that orthodontic treatment affects OHRQoL varies depending on the type of malocclusion. 44 The OHIP-14 is the most widely used tool for evaluating OHRQoL due to its validity, responsiveness, and reliability. 45 The OHIP-14 questionnaire contains 14 items, which are distributed across seven dimensions: handicap, social disability, psychological disability, physical disability, physical pain, and psychological discomfort (Figure 1). 2
Clear aligners were developed to address some of the drawbacks of fixed appliances and cater to patients’ comfort and aesthetic needs. 46 As per the existing literature, orthodontic treatment with clear aligners is safe, comfortable, and esthetically acceptable. 47 In contrast to conventional FAT, patients may successfully control gingival biofilm and, hence, maintain healthier periodontal hygiene throughout orthodontic treatment since clear aligners are simple to remove during meals and oral hygiene activities. This is especially crucial for adult patients seeking orthodontic treatment since they are more likely to have periodontitis. 46 Studies on the results of orthodontic treatment with clear aligners have produced conflicting findings. In adult populations, some research found that using aligners led to much poorer outcomes than using fixed orthodontic appliances, while other studies revealed that the two treatment modalities were nearly equally effective. 48 Furthermore, CAT require 4.8 months longer to treat patients who have simple malocclusions than conventional FAT, although the occlusal results at 6 months after treatment are comparable. 44
In this study, adult patients undergoing orthodontic treatment by clear aligners had higher OHRQoL than those treated with fixed metal or fixed ceramic appliances after one week of treatment initiation. However, OHRQoL was comparable between the three groups after 3-months of orthodontic treatment. This outcome was in partial agreement with the study outcomes of Tunca et al. 4 and Hashemi et al. 17 which showed a significant difference between CAT and conventional FAT in terms of individual's OHRQoL on day 1 of treatment, but no significant difference was found on other assessment period. During conventional FAT, almost 95% of patients’ experience pain, and 8% discontinue treatment because of pain. Within 12 h of applying the archwire, the discomfort starts, peaks within a day, and then progressively subside after three days. 4 This possibly explains the significant difference in OHRQoL between the groups on day 7 and non-significant difference at day 30 in this study. Furthermore, there was no significant difference in OHRQoL between the metal and ceramic bracket appliances. This is in disagreement with the outcome of Zamora-Martínez et al. study, 49 where the authors found a significant difference in OHRQoL between metal and ceramic bracket appliance and non-significant difference between ceramic and clear aligner therapy. However, the assessment was done at 6 months, T1 and after conclusion of treatment, T2.
Previous studies comparing the quality of life associated with CAT and FAT have shown conflicting results.4,5,32–37 Gao et al. 32 and AlFawal et al. 33 reported that patients treated with clear aligners showed higher OHRQoL than those treated with FAT. Furthermore, Qi et al., 35 in their cross-sectional investigation, also reported that clear aligners were beneficial for kids and teenagers with regard to OHRQoL. Consistent with earlier findings, a recent systematic review by Kaklmanos et al. 5 also concluded that treatment with clear aligners instead of conventional metal fixed appliances was associated with higher OHRQoL scores. Clear aligner therapy is associated with improved OHRQoL, which is apparent when one considers improved eating and chewing habits as well as fewer ulcerations and pain. 50 Contrarily, CAT has been associated with lower OHRQoL with regard to speech as compared to FAT. 51
Contrary to the above findings, Shafaee et al. 37 showed that the OHRQoL in the clear aligners group was considerably lower than the fixed appliance group. In their randomized controlled clinical trial, AlHafi et al., 36 evaluated the effect of Ni-Ti spring modified CAT on OHRQoL in comparison to FAT. The authors found no discernible variation in the overall OHIP-14 score during the entire evaluation period between the FAT and the Ni-Ti spring modified CAT group. Flores-Mir et al. 52 evaluating the OHRQoL of the patients treated by Invisalign and bracket based appliance after orthodontic treatment found statistically identical outcomes across the dimensions evaluated, except for chewing and eating. Similarly, in a systematic review by Li et al., 34 OHRQoL was higher for patients treated with clear aligners than patients treated with fixed appliances during orthodontic therapy. Nonetheless, OHRQoL seemed to be comparable between the two groups at the conclusion of the treatment.
The outcome of the current study also showed that OHRQoL improved significantly within the groups at different assessment periods. This affirms that there is an association between OHRQoL and orthodontic treatment, which has also been reiterated in previous studies.44,49 Nonetheless, Curto et al. 53 found reduced OHRQoL with FAT, but that was temporary and improved over time.
The outcome of this study is not without limitation. Firstly, the fact that this study relied on questionnaires raises the risk of information bias because the findings rely on the participants’ accuracy, honesty, and memory. 46 Secondly, the participants and the clinician was not blinded which could have affected the detection bias. Finally, the study did not investigate the impact of age, gender, malocclusion type, and malocclusion complexity on the outcomes of orthodontic treatment as the study only included Class I malocclusion cases with mild crowding. Future clinical trials should include larger sample sizes and cover a wider variety of malocclusion types and severities in order to extrapolate the results of this study to a larger group of orthodontic patients. Finally, the provided data was gathered over a brief three-month follow-up period. Further longitudinal research is required to assess the long-term effect of these appliances on OHRQoL.
Conclusion
Within the study's outcomes and limitations, the following conclusion has been drawn:
The study demonstrated a positive association between OHRQoL and orthodontic treatment. Irrespective of the study groups, there was a significant improvement in OHRQoL from baseline to different assessment periods. The OHIP-14 scores showed that adult patients treated with clear aligners had significantly higher OHRQoL than those who underwent conventional fixed bracket-based treatment after 7 days of treatment initiation. However, OHRQoL appeared to be similar between the clear aligners and fixed bracket-based groups after three months of treatment. The OHRQoL were comparable at different assessment periods between the bracket-based groups (metal or ceramic).
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.