
Abstract
Background:
Postoperative hypoxemia is a severe complication in patients undergoing surgery for acute Type A aortic dissection (AAD), with significant impacts on recovery and clinical outcomes. Technological advancements in risk assessment models offer opportunities for early intervention and optimized care.
Objective:
To develop and validate a technology-driven predictive model for hypoxemia based on clinical and intraoperative risk factors, enhancing postoperative management strategies.
Methods:
A retrospective cohort of 242 patients was analyzed, including 77 with hypoxemia (PaO2/FiO2 ≤ 200 mmHg) and 165 without. Key clinical variables, intraoperative factors, and postoperative outcomes were examined. Spearman correlation analysis and receiver operating characteristic (ROC) curve analysis were conducted to identify and validate predictive markers.
Results:
Prolonged time from symptom onset to surgery (>48 h), aortic cross-clamp time, and deep hypothermic circulatory arrest time (DHCA) emerged as the most significant predictors (all p < 0.001). DHCA time demonstrated the highest sensitivity (0.961) and area under the curve (AUC = 0.891). Additional significant predictors included intraoperative blood product use and prolonged mechanical ventilation, with cumulative predictive value for hypoxemia risk.
Conclusion:
The integration of clinical variables into a technology-enhanced prediction model provides robust early warnings of postoperative hypoxemia risk. Implementing timely surgical interventions and refined intraoperative management can minimize adverse respiratory outcomes, improving recovery in AAD patients.
Keywords
Introduction
Type A aortic dissection (AAD) was a critical condition characterized by the spontaneous dissection of the ascending aorta, representing a critical medical emergency that requires prompt diagnosis and surgical treatment.1–3 Despite advances in medical technology and perioperative care, patients with AAD remain at a heightened risk of postoperative complications, including the development of hypoxemia, which can significantly impact clinical outcomes and patient prognosis.4–6
The etiology of hypoxemia in patients with AAD was multifactorial, involving complex pathophysiological mechanisms rooted in the pathogenesis of aortic dissection, perioperative hemodynamic alterations, and postoperative recovery dynamics.7,8 Contributing factors encompass the acute disruption of aortic integrity, subsequent myocardial ischemia, systemic inflammatory responses, tissue hypoperfusion, and the potential for postoperative respiratory compromise secondary to prolonged surgical procedures.9,10 Acute hypoxemia following surgical intervention for AAD poses substantial challenges to patient management.
Thus, there is a necessity for a thorough understanding of the risk factors related to their occurrence and the creation of effective prediction models to inform clinical decision-making. The present study seeks to identify the risk factors associated with the development of hypoxemia in patients with acute aortic dissection (AAD) undergoing surgical intervention. Additionally, this research aims to develop a prediction model that integrates these identified factors, thereby reducing the incidence of postoperative hypoxemia and enhancing patient outcomes.
Materials and methods
Sample selection
The study population consisted of patients with AAD admitted to Shaanxi Provincial People's Hospital. This study was approved by the Ethics Committee of Shaanxi Provincial People's Hospital (No: SPPH-LLBG-17-3.2), Signed written informed consents were obtained from the patients and/or guardians. This study was conducted in accordance with the Declaration of Helsinki and followed the ethical standards of China. A total of 165 patients did not experience hypoxemia, while 77 patients developed hypoxemia. This retrospective analysis focused on the clinical data of these patients to investigate the risk factors and prediction model for hypoxemia in AAD.
Inclusion criteria, exclusion criteria
Inclusion criteria: Definitive diagnosis of AAD confirmed by chest and abdominal enhanced computed tomography angiography (CTA); Underwent ascending aorta replacement, aortic valve replacement, aortic sinus repair, coronary artery bypass grafting, total arch replacement, or descending aorta stent implantation; Aged between 18 and 80 years.
Exclusion criteria: Inability to assess oxygenation status due to intraoperative or postoperative death within 24 h; Missing arterial blood gas analysis due to various reasons; Concurrent liver or kidney failure; Severe arrhythmia or heart failure; Impaired cognitive function; Hemodynamic instability; Presence of malignant tumors; Incomplete clinical data.
Grouping criteria
In line with the Berlin definition of acute respiratory distress syndrome (ARDS), a postoperative oxygenation index (PaO2/FiO2) of ≤200 mmHg within 24 h was utilized as the diagnostic threshold for hypoxemia, while the assessment of postoperative hypoxemia varied across different research centers, spanning from 24 to 72 h. This study adopted the 24-h postoperative period for evaluating the occurrence of hypoxemia. Patients were classified into the HY group if they had hypoxemia (PaO2/FiO2 ≤ 200 mmHg) based on the lowest oxygenation index within the initial 24 h following surgery. Patients without hypoxemia (PaO2/FiO2 > 200 mmHg) were classified into the NH group.
Observation indicators
A single experienced physician retrieved general data from the electronic medical record system, including gender, age, BMI, smoking history, hypertension history, diabetes history, cardiac surgery history, respiratory system disease history, time from onset of symptoms to surgery, left ventricular ejection fraction (LVEF), presence of pericardial effusion, intraoperative variables such as surgical duration, cardiopulmonary bypass time, ACC time DHCA time, and intraoperative blood product usage, as well as postoperative variables such as blood product usage, need for reoperation, reintubation, return to the intensive care unit (ICU), delirium, duration of MH, ICU length of stay, continuous renal replacement therapy (CRRT) rate, discharge from the ICU, pleural effusion rate, and positive pressure ventilation rate.
Statistical analysis
The data analysis was performed using the Statistical Package for Social Sciences (SPSS) version 25.0 software (SPSS, Chicago, IL, USA). Categorical data were represented using frequencies and percentages ([n (%)]). The chi-square test was utilized according to the basic formula when the sample size was at least 40 and the theoretical frequency (T) was 5 or greater, with the test statistic denoted as χ
Results
Demographic information and general characteristics
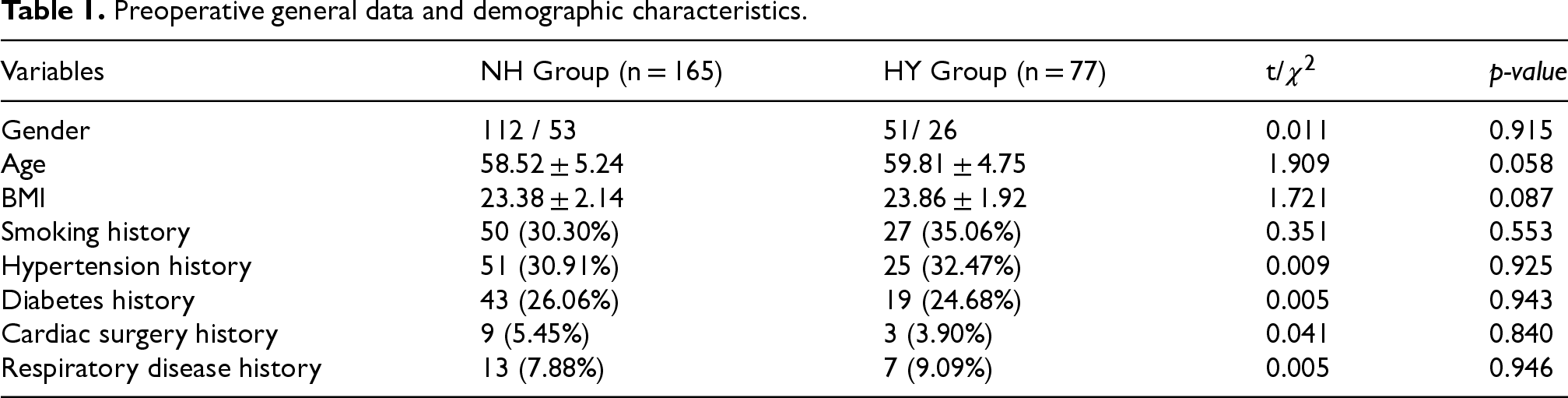
In the analysis of preoperative general data and demographic characteristics, several factors were compared between the NH group and the HY group of patients with AAD (Table 1). Based on the data provided, multifactorial differences in preoperative general information and demographic characterization comparing patients with AAD in the NH and HY groups showed no statistically significant differences between the two groups in these variables such as gender (p = 0.915), smoking history (p = 0.553), history of hypertension(p = 0.925), diabetes history (p = 0.943), cardiac surgery history(p = 0.840), respiratory disease history (p = 0.946), mean age (p = 0.058), and Body Mass Index (BMI) (p = 0.087).
Preoperative general data and demographic characteristics.
Preoperative general data and demographic characteristics.
We compared the non-hypoxic and hypoxic groups of patients with AAD in terms of several factors such as Time from Onset to Surgery as well as LVEF, presence of pericardial effusion and others (Table 2). According to the data presented, among patients with AAD in the hypoxemia group (62.58 ± 2.55 h) and the non-hypoxemia group (59.58 ± 2.31 h), the time from onset to surgery was significantly longer in the hypoxemia group compared to the non-hypoxemia group, and the proportion of patients who had been undergoing surgery for more than 24 (p < 0.001) and 48(p < 0.001) hours was significantly higher than in the non-hypoxemia group. The results suggest that preoperative hypoxemia may have an impact on the time from onset to surgery and requires further clinical observation and interventions. In addition, and the differences in LVEF (p = 0.111) and pericardial effusion (p = 0.072) were not significant.
Preoperative factors.

Preoperative factors.
In evaluating intraoperative factors in patients with AAD (Table 3), While the duration of surgery (p = 0.554) and cardiopulmonary bypass time (p = 0.591) did not exhibit statistically significant differences between the groups, our results showed significantly longer ACC time (p < 0.001), and DHCA time (p < 0.001) and higher intraoperative blood product unit (p < 0.001) requirements in the HY group compared with the NH group. These findings indicate that the HY group experienced significantly longer ACC and DHCA times, as well as a higher requirement for intraoperative blood product units compared to the NH group.
Intraoperative factors.

Intraoperative factors.
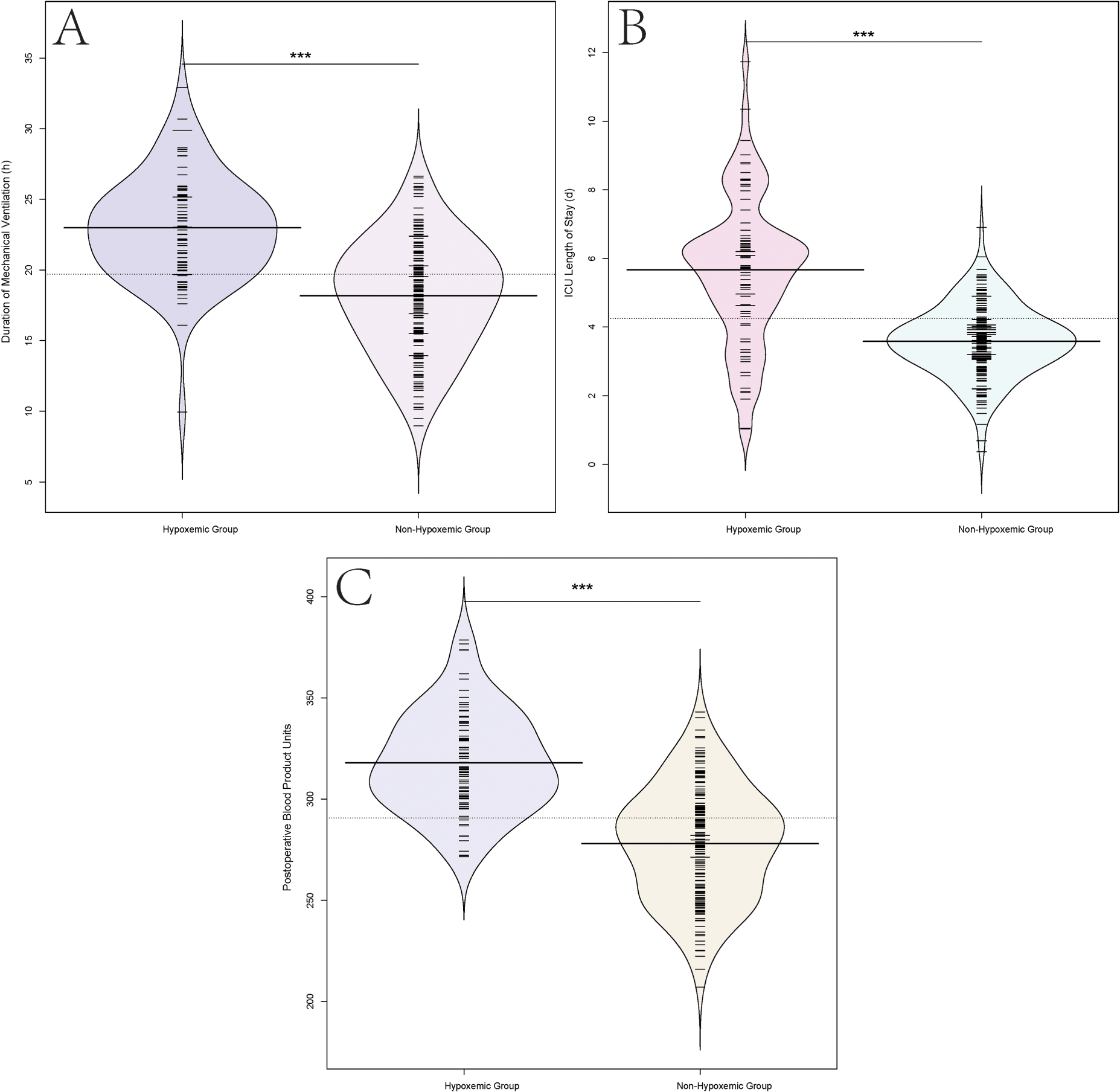
In the evaluation of postoperative factors in patients with AAD comparisons between the NH group and the HY group revealed several significant differences (Table 4). The HY group demonstrated a longer duration of MH (p < 0.001) (Figure 1(a)), an extended ICU length of stay (p < 0.001) (Figure 1(b)), and higher incidences of reintubation, delirium, pleural effusion, and the need for positive pressure ventilation compared to the NH group. Postoperative blood product units were significantly higher in the HY group compared to the NH group (p < 0.001) (Figure 1(c)). Moreover, the HY group showed a higher frequency of CRRT (p = 0.131), although this difference was not statistically significant. However, between the groups, no significant differences were observed regarding the need for reoperation, return to ICU, discharge from ICU, and the presence of pleural effusion. These findings underline the substantial postoperative complications and prolonged recovery experienced by the HY group following surgery for Type A aortic dissection.
Postoperative factors.
Postoperative factors.

In the correlation analysis between various risk factors and hypoxemia in patients with AAD, significant associations were observed (Table 5). Strong positive correlations were found between hypoxemia and several preoperative and intraoperative, postoperative factors, including time from onset to surgery, ACC time, DHCA time, intraoperative and postoperative blood product units, duration of MH, ICU length of stay, pleural effusion, and the need for positive pressure ventilation (p < 0.001 for all correlations). Notably, time from onset to surgery exceeding 24 h and 48 h demonstrated the strongest correlation with hypoxemia (p < 0.001 for both).
Correlation analysis between various risk factors and hypoxemia in patients with AAD.

Correlation analysis between various risk factors and hypoxemia in patients with AAD.
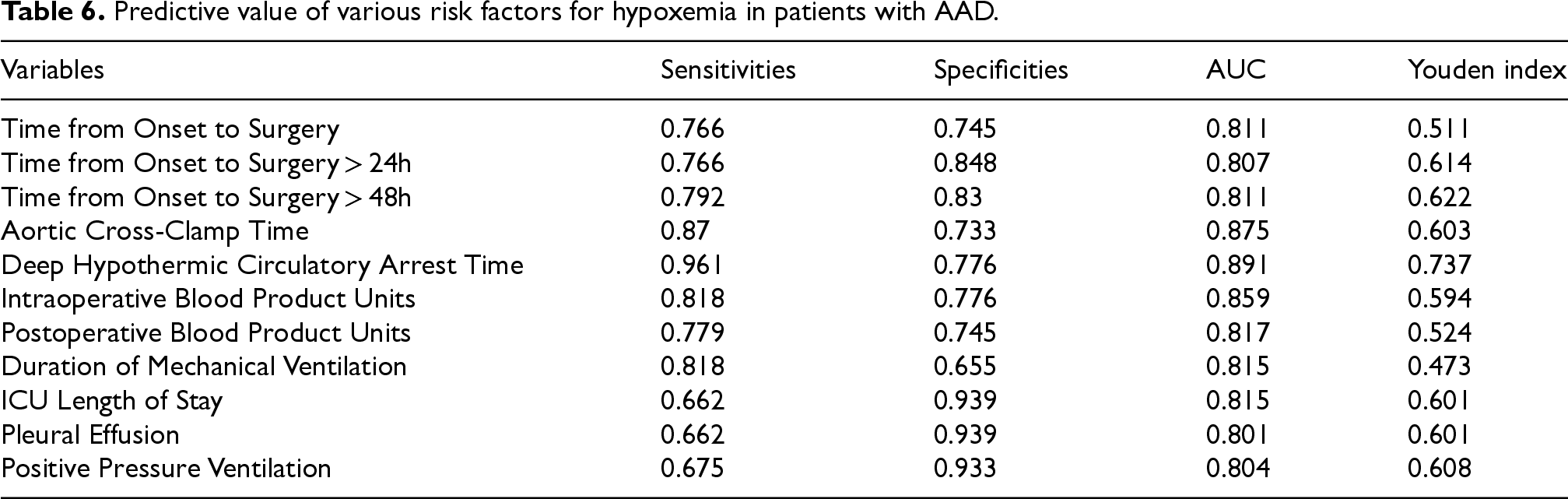
In assessing the predictive value of various risk factors for hypoxemia in patients with AAD, the sensitivity, specificity, area under the curve (AUC), and Youden index were determined (Table 6). Several factors demonstrated notable predictive value for hypoxemia, with DHCA time presenting the highest sensitivity (0.961) and AUC (0.891), indicating its strong predictive capability. Additionally, time from onset to surgery exceeding 48 h, ACC time intraoperative and postoperative blood product units, and pleural effusion, positive pressure ventilation exhibited high AUC values, signifying their potential as predictive factors for hypoxemia. Notably, based on the analysis of AUC values, we observed that all three factors, ICU length of stay, onset to surgery time of more than 24 h, demonstrated significant predictive power. These findings underscore the clinical relevance of these risk factors in predicting the development of hypoxemia in patients with AAD, illustrating the potential utility of this prediction model in identifying high-risk patients and guiding appropriate intervention strategies to mitigate the risk of hypoxemia.
Predictive value of various risk factors for hypoxemia in patients with AAD.
Predictive value of various risk factors for hypoxemia in patients with AAD.
Acute hypoxemia in patients with AAD following surgical intervention remains a concerning clinical complication, often associated with adverse outcomes.11–13 This retrospective study aimed to identify the risk factors contributing to the development of hypoxemia in these patients and develop a prediction model to aid in their clinical management. Our findings highlight several important preoperative, intraoperative, and postoperative factors that may influence the occurrence of hypoxemia in this patient population. Additionally, the development of a prediction model incorporating these risk factors provides valuable insights for predicting and mitigating the risk of hypoxemia in patients receiving surgical intervention for AAD.
Our study analysis shows that time intervals exceeding 24 and 48 h from symptom onset to surgery were linked to an increased likelihood of hypoxemia., a finding that is consistent with previous literature,14–16 suggesting that delays in surgical interventions beyond these time points may significantly elevate the risk of hypoxemia in patients with AAD. Studies have reported that prolonged AAD surgery times will increase intraoperative risk factors, such as ACC and DHCA time, as well as increased use of blood product.17–19 This study showed that prolonged ACC time prolonged DHCA time, and increased intraoperative blood product unit requirements were also significantly associated with the development of hypoxemia, and the results suggest the importance of intraoperative management for the prevention of hypoxemia. This prolonged intraoperative time can contribute to tissue hypoxia, reperfusion injury, and inflammatory responses, impacting postoperative respiratory function and predisposing patients to hypoxemia. 20 However, postoperative factors also play a crucial role in the development of hypoxemia in AAD patients. The results of the study show that the group of hypoxemic patients had a higher incidence of complications such as prolonged MH, prolonged ICU stay, reintubation, delirium, and pleural effusion. These complications may stem from hemodynamic instability, tissue ischemia-reperfusion injury, and systemic inflammatory responses linked to aortic dissection surgery, contributing to respiratory compromise and hypoxemia,21–23 these findings highlight the critical role of comprehensive postoperative management and rehabilitation for this population to improve long-term outcomes and quality of life. In addition, we observed that patients in the hypoxemia group presented a higher frequency of requiring CRRT, which further identified the potential impact of hypoxemia on renal function. Previous studies have also clearly demonstrated that hypoxemia may contribute to the progression of chronic kidney disease and adversely affect the long-term prognosis of patients.18,24 Furthermore, individual patient characteristics, such as comorbidities, preexisting cardiopulmonary status, and baseline physiological reserve, significantly influence the risk of hypoxemia. Patients with preexisting respiratory and cardiovascular comorbidities may be more vulnerable to postoperative respiratory compromise and hypoxemia. 25 Thus, individualized risk assessment and tailored perioperative management considering the patient's baseline characteristics were crucial in mitigating hypoxemia risk in patients undergoing surgical treatment for AAD. Correlation analyses performed revealed strong positive correlations between hypoxemia and several preoperative and intraoperative factors, including time from onset to surgery, ACC time to deep hypothermic circulatory arrest, intraoperative and postoperative units of blood products, duration of MH, length of stay in the ICU, pleural effusion, and need for positive pressure ventilation. These factors may play a significant role in the occurrence and severity of hypoxemia and provide valuable reference and guidance for clinical practice. From a prediction modeling perspective, our study assessed the predictive value of various risk factors for hypoxemia in AAD, the results showed that DHCA time had the highest sensitivity and AUC. Furthermore, the time from onset to surgery over 48 h, ACC time intraoperative blood product units, and pleural effusion all had high AUC values, further emphasizing their potential as predictors of hypoxemia in patients with AAD.
In conclusion, The development of hypoxemia in patients with AAD was associated with various risk factors rooted in the complex pathophysiological mechanisms of this condition. 26 The results showed that hypoxemia in patients with AAD is influenced by multiple risk factors, including time from a from onset to surgery, ACC time DHCA time, intraoperative and postoperative blood product units, duration of MH, and ICU length of stay, this study presents a prediction model of hypoxemia based on preoperative, intraoperative, and postoperative factors, the influence of multi-factor interaction among clinical variables on the development of hypoxemia was elucidated. Understanding the latent reasons for these risk factors was crucial for enhancing patient care and clinical outcomes.
This study is not without limitations. Firstly, the retrospective nature of our analysis may introduce selection bias and confounding factors that could affect the generalizability of the results. Secondly, although we have identified several significant risk factors for hypoxemia in patients with AAD, the causality between these factors and the development of hypoxemia cannot be established due to the observational design. Thirdly, the sample size, while sufficient for identifying trends, may limit the power to detect more subtle effects or interactions among variables. Additionally, all data were collected from a single center, which might not fully represent the diverse patient populations and clinical practices across different institutions. Furthermore, despite the good predictive value of our prediction model for hypoxemia, external validation in an independent cohort is necessary to assess its generalizability and robustness. Future prospective studies involving larger patient samples are necessary to further validate the prediction model and elucidate other factors contributing to the development of hypoxemia in patients with AAD.
Footnotes
Acknowledgement
The authors express their appreciation to staff in Shaanxi Provincial People's Hospital.
Ethical considerations
This study protocol was reviewed and approved by the ethic committee of Shaanxi Provincial People's Hospital. Since this study is a retrospective cohort study and the identification information of patients has anonymity, there is no need for informed consent from patients and their families.
Author contributions/CRediT
Yujie Wang: study design, data analysis, drafting the manuscript and revision of the manuscript. Qinying Wang: data collection and analysis, drafting the manuscript, investigation. Lingguo Wang, Cui Ji, Xiaoying Xing, Lu Pan: investigation and editing. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data involved in the present study can be provided under reasonable request.