
Abstract
Background
Chatbots are increasingly integrated into healthcare, offering personalized and accessible health advice. However, the impact of factors such as chatbot authority, health information type, and interaction style on users’ decision-making remains unclear.
Objective
This study aims to investigate how these elements influence users’ willingness to adopt health advice provided by chatbots.
Methods
A 2 × 2 × 2 factorial experiment was conducted with 480 university students to examine the effects of chatbot authority (authoritative vs. non-authoritative), health information type (preventive vs. treatment-related), and interaction style (formal vs. informal). Participants’ willingness to adopt the health advice was measured before and after interacting with the chatbot.
Results
The study found that a authoritative chatbot delivering treatment-related advice in a formal style significantly increased willingness to adopt the advice. Conversely, preventive information was more effective when presented informally by a non-authoritative chatbot. These results support the media evocation paradigm, which suggests that chatbots framed as authoritative figures evoke greater user engagement and trust in health contexts.
Conclusion
The findings extend the media evocation paradigm by demonstrating that chatbot authority, information type, and interaction style should be aligned with the nature of health advice to maximize effectiveness. This study provides insights for designing chatbots that improve health decision-making by tailoring their communication strategies.
Introduction
In recent years, health communication has increasingly incorporated chatbots as a key tool for delivering health advice and guiding decision-making.1,2 These AI-driven systems are becoming integral to healthcare, providing accessible, timely, and personalized health information. 3 Chatbots have shown potential in preventive care and treatment support, helping users make informed health decisions. 4 Recent systematic reviews and meta-analyses have highlighted chatbots’ effectiveness in various healthcare domains, including chronic disease management, mental health support, and medication adherence, demonstrating their potential to complement traditional healthcare services.5,6 Studies have shown that chatbot-driven interventions can enhance patient engagement, improve adherence to medical recommendations, and promote health literacy by providing interactive and tailored health communication. 7 Moreover, the design of chatbot interactions—such as their perceived expertise, interaction style, and the type of health information they provide—plays a crucial role in shaping user trust and willingness to follow health advice. 8 With growing healthcare demands and limited professional access, chatbots provide a scalable solution for health management. 9 This makes their role in influencing health decisions increasingly important within the field of health sciences. 10
Previous research has examined chatbots’ ability to deliver accurate information, 11 support patient engagement, 12 and enhance user satisfaction. 13 Studies have demonstrated their usefulness in tasks such as symptom checking 14 and health education. 15 Researchers have also investigated how chatbots can tailor communication to meet users’ health needs, employing different interaction styles to increase the clarity and relevance of the information provided. 16 These studies have primarily focused on how chatbots deliver health advice and the quality of the interactions between users and chatbots. 17
Despite this progress, there remain gaps in understanding how chatbots influence health decision-making. Specifically, the impact of various factors such as the role of the chatbot (e.g., authoritative health expert vs. regular chatbot), the type of information provided (preventive vs. treatment-related), and the interaction style (formal vs. informal) on users’ acceptance of health recommendations has not been thoroughly investigated. Existing studies often overlook how these variables interact and affect individuals’ decision-making processes, leaving a gap in our understanding of the most effective ways to design chatbot interactions for health guidance.
To address these gaps, this study employs the media evocation paradigm and conducts a 2 × 2 × 2 factorial experiment. The experiment explores how chatbot role, type of information, and interaction style influence participants’ willingness to accept health-related advice. By examining these variables, this research aims to provide deeper insights into how chatbots can effectively support health decision-making, offering new perspectives on the design of AI-driven health communication tools.
Literature review
Evolving frameworks: From CASA to the media evocation paradigm
The computers are social actors (CASA) paradigm, developed by Nass and colleagues, has been foundational in the field of human-computer interaction. 18 This paradigm suggests that humans interact with computers and other forms of artificial intelligence as if they were human beings, applying social norms and expectations to these interactions. CASA research has shown that individuals may treat chatbots with politeness, trust, and emotional engagement, even though they know they are not interacting with actual people. 19 In healthcare, this framework has been particularly useful in explaining why users may trust and follow the advice of health chatbots, as the human-like qualities of these bots evoke familiar social responses. 20
However, the CASA paradigm has its limitations, particularly as technology and media interactions become more sophisticated. CASA tends to focus on the automatic, often mindless ways people respond to machines. 21 While this is valuable in understanding some forms of interaction, it overlooks the more complex and reflective ways that modern media, such as chatbots, influence user behavior. Chatbots in health communication are no longer simple information dispensers; they now engage users in more nuanced, context-sensitive conversations, requiring a deeper theoretical approach to fully understand their impact on decision-making. 22
This is where the media evocation paradigm becomes particularly relevant. The media evocation paradigm builds upon the idea that technology can evoke emotional and cognitive responses, challenging users to think more critically and reflectively about their interactions. 23 Unlike CASA, which emphasizes automatic social behaviors, the media evocation paradigm focuses on how media objects, such as chatbots, provoke self-reflection and deeper engagement with their content. This approach sees chatbots not merely as tools that relay information, but as evocative agents that prompt users to reconsider their relationship with technology, the nature of health advice, and the trustworthiness of AI systems in healthcare. 24
CASA, grounded in the media equation theory, posits that people mindlessly apply social rules to computers, treating them as if they were human. It emphasizes automatic, unconscious social responses to minimal cues, such as politeness or reciprocity, even when users are aware they are interacting with a machine. 25 This paradigm assumes that people's interactions with AI are primarily driven by habitual and intuitive social behaviors. 26 The media evocation paradigm conceptualizes AI as more than just passive social actors; it argues that machines can actively evoke reflection and negotiation about their own ontological status and the nature of human-AI interactions. Unlike CASA, which focuses on mindless social responses, media evocation suggests that interactions with AI can prompt deliberate cognitive and emotional engagement, leading users to critically assess the machine's role, credibility, and potential agency. This paradigm highlights how AI exists in a liminal space between human and machine, challenging traditional classifications of social actors and prompting deeper reflections on what it means to communicate with AI. 27 By shifting the focus from automatic social responses (CASA) to reflective engagement (media evocation), the latter provides a more nuanced framework for studying AI interactions, particularly in complex domains like health communication, where trust, credibility, and decision-making play a crucial role. 28
In the context of health communication, the media evocation paradigm allows for a more nuanced exploration of how different chatbot characteristics—such as their perceived authority, the type of information they provide, and their interaction style—affect users’ health decision-making. By evoking deeper cognitive processes, chatbots encourage users to engage more mindfully with the health advice they receive, reflecting on the source, relevance, and potential outcomes of the information. This paradigm shift from CASA to media evocation provides a richer framework for understanding the complex ways in which AI-driven health technologies can shape individual decision-making. The media evocation paradigm thus provides the theoretical foundation for this study.
Chatbot identity in health decision-making: Authoritative vs. non-authoritative roles
The identity of a chatbot, specifically whether it is perceived as authoritative or non-authoritative, may influence users’ health decision-making. In broader communication contexts, the perceived authority of the source providing advice has often been shown to affect the trustworthiness and acceptance of the information.29,30 When chatbots are designed to project an authoritative identity, users may view them as more credible, potentially leading to greater confidence in the advice they provide. 31 Some research suggests that authoritative chatbots, by presenting themselves as knowledgeable and professional, could enhance user trust and increase the likelihood of following recommendations.4,32
However, much of the existing research on chatbot identity has been conducted in non-health contexts, and it remains unclear how authoritative versus non-authoritative chatbots influence decision-making specifically in healthcare settings. While non-authoritative chatbots, which are often positioned as neutral assistants or general support tools, may still provide valuable information, their perceived lack of expertise may result in lower trust and reduced compliance with health advice. 33 This is particularly relevant when users are faced with complex medical decisions, where the expertise of the information source is critical to the decision-making process. 34
Despite increasing interest in the role of chatbot identity, there is limited research that directly addresses how authoritative versus non-authoritative chatbots impact health decision-making. While authority has been shown to be important in communication generally, the specific influence of chatbot identity in health contexts has not been thoroughly explored. 35 As such, further research is needed to better understand the role of chatbot identity in health decision-making and the adoption of health advice.
Therefore, we propose:
RQ1: Does chatbot identity (authoritative vs. non-authoritative) influence users’ health decision-making?
The impact of information type on health decision-making: Preventive vs. treatment advice
The type of health information provided by chatbots—whether preventive or treatment-related—may play a significant role in shaping users’ health decision-making. Preventive information includes advice aimed at avoiding health problems before they arise, such as guidance on lifestyle modifications, diet, and exercise. 36 In contrast, treatment-related information is focused on managing existing health conditions and providing recommendations related to medications, treatment plans, or symptom management. 37 Previous research in health communication suggests that the type of information users receive can influence how they process and act on health advice, with preventive advice typically encouraging long-term behavioral changes and treatment advice prompting more immediate decisions.38,39
Some studies have found that individuals may respond differently to preventive and treatment-related information based on the perceived urgency and relevance of the advice. 40 Preventive health information is often perceived as less urgent and more future-oriented. Its influence on decision-making might depend on individuals’ motivation to engage in health-promoting behaviors and their perception of future risks. 41 However, because preventive advice is not tied to an immediate health threat, users may be more likely to delay action, potentially leading to lower compliance in the short term. 42
On the other hand, treatment-related advice could be seen as more pressing and directly relevant to users’ current health concerns. Users may be more inclined to follow treatment advice when they are experiencing symptoms or managing a diagnosed condition, as the perceived urgency and personal relevance are higher. 43 In such cases, individuals may be more likely to take immediate action. However, the extent to which users follow treatment recommendations could also depend on how much they trust the source of the information and their perceived ability to comply with the advice. 44
While these distinctions between preventive and treatment-related information are well-supported in the broader health communication literature, there is limited research specifically examining how the type of health information provided by chatbots influences users’ decision-making. Existing studies primarily focus on human-to-human communication, leaving a gap in understanding whether these findings apply to chatbot-delivered health advice. 45 Given the increasing reliance on chatbots to provide both preventive and treatment information, it is important to investigate whether users respond differently based on the nature of the information presented by the chatbot.
Therefore, we propose:
RQ2: Does the type of health information provided by the chatbot (preventive vs. treatment) influence users’ health decision-making?
Interaction style and its role in health decision-making: Formal vs. informal communication
The interaction style of a chatbot, whether formal or informal, may play an important role in shaping how users engage with the information provided. Formal communication generally involves a more structured and professional tone, utilizing technical language and an authoritative approach to convey information. 46 In contrast, informal communication tends to be more conversational and approachable, using colloquial language and a friendly tone to connect with users. 47 Prior research in human-computer interaction suggests that the interaction style of digital agents can influence users’ perceptions of the agent's credibility, trustworthiness, and overall relatability. 48
In various contexts, the use of formal communication has been associated with perceptions of authority and professionalism, which may lead to higher levels of trust in the information provided. This is particularly relevant when the information being communicated requires technical precision or expertise. 49 However, overly formal or technical language can sometimes result in misunderstandings or disengagement if users find the information difficult to process or too impersonal. 50
On the other hand, informal interaction styles have been found to enhance user comfort and engagement in certain settings. By adopting a friendlier, more approachable tone, informal interactions can help alleviate feelings of anxiety or intimidation, particularly when dealing with complex or unfamiliar systems. 51 In this way, informal communication may foster a greater sense of connection between the user and the system, potentially increasing interaction and receptiveness to the information being provided. However, it remains uncertain whether informal styles are equally effective in contexts that demand professionalism and authority, such as those involving serious health concerns. 52
While these studies suggest that different interaction styles can influence user perceptions and behaviors, there is limited research on how these interaction styles impact health decision-making when delivered by a chatbot. Much of the existing literature has focused on human-to-human interactions or user experiences in non-health contexts, leaving a gap in our understanding of how formal versus informal communication affects the adoption of health advice in a digital setting. Given the growing use of chatbots in healthcare, it is crucial to examine whether the interaction style of these systems can influence how users respond to health recommendations.
Therefore, we propose:
RQ3: Does the interaction style of the chatbot (formal vs. informal) influence users’ health decision-making?
Method
Participants
We recruited 480 participants from a university in eastern China for this study. Participants had a mean age of 21.22 years (SD = 1.38), with 42.08% (n = 202) identifying as female.
This study was approved by the Institutional Review Board of the authors’ affiliated institutions, and all participants provided informed consent prior to participation. Each participant who completed the experiment was compensated with 15 RMB via WeChat Pay or Alipay.
Procedure
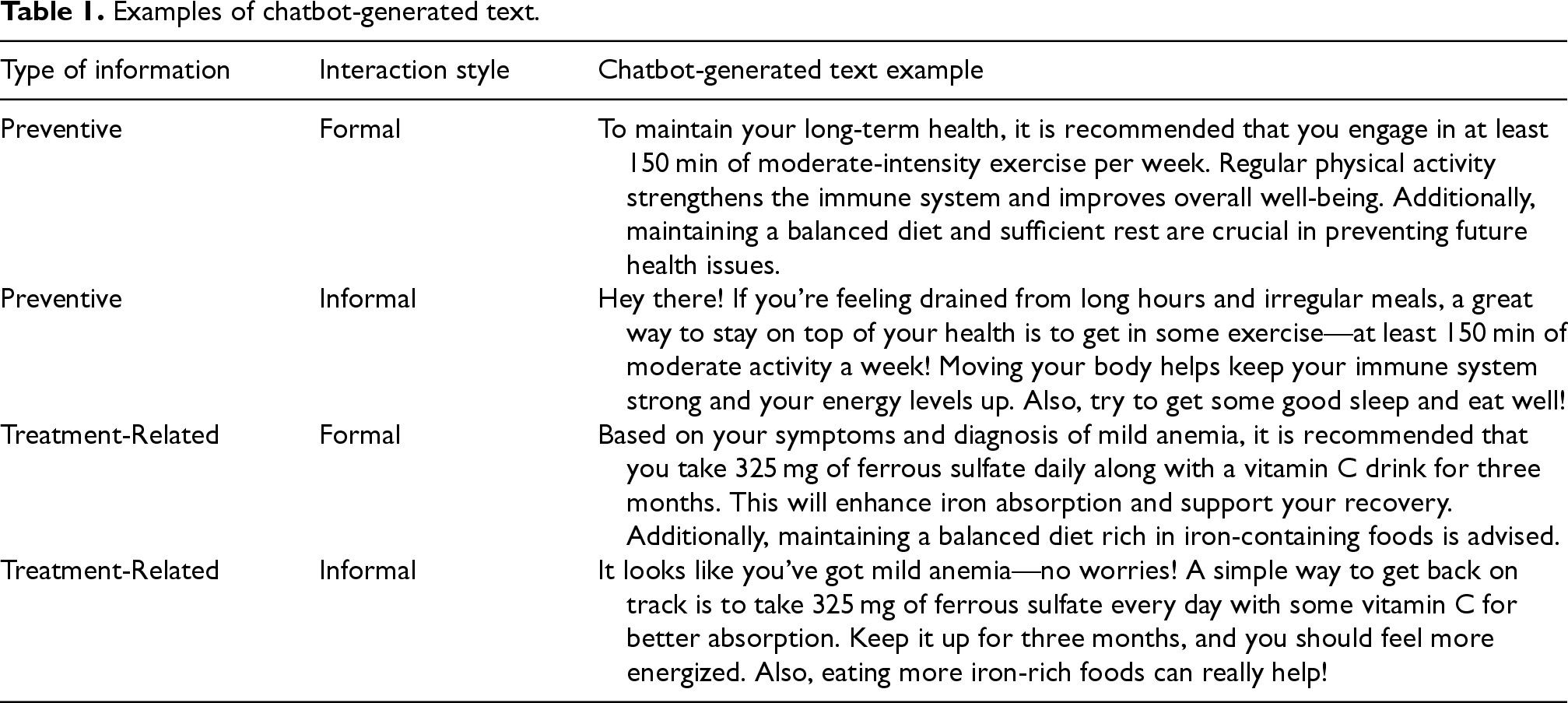
Firstly, we designed the experimental materials, which included two types of health information: preventive and treatment-related. Participants in the preventive condition were presented with a scenario where they noticed their workload increasing, resulting in late nights and irregular meals, though they were not currently experiencing health issues. They were concerned about the long-term effects on their health and wanted to adjust their lifestyle. In this situation, participants were advised to engage in at least 150 min of moderate-intensity exercise per week to boost their immune system and overall physical strength. In the treatment-related condition, participants were presented with a scenario where they were diagnosed with mild anemia after feeling fatigued and experiencing trouble concentrating. They were advised to take 325 mg of ferrous sulfate daily with a vitamin C drink for three months to help treat the condition.
Secondly, participants were randomly assigned to one of the eight experimental groups, resulting in a 2 × 2 × 2 factorial design, with 60 participants in each group. Before the interaction, participants completed a pre-test. This pre-test asked them to rate their willingness to adopt the provided health advice on a seven-point Likert scale, ranging from 1 (“not willing at all”) to 7 (“very willing”). The experiment was conducted between July and September 2024.
Thirdly, the participants initiated a conversation with the chatbot, Bennybot, which was developed by the research team and integrated with GPT-4. The experimental manipulation involved several conditions: (1) Chatbot Identity—participants were informed that they were either interacting with a health expert from a well-known hospital (high authority) or a general health chatbot (low authority). In this study, the chatbot refers specifically to a generative AI with large language models capable of processing and generating health-related advice. High authority chatbots were framed as virtual doctors affiliated with a well-known hospital, emphasizing medical expertise. In contrast, low authority chatbots were presented as general AI assistants without institutional backing, making them appear less authoritative. (2) Type of Information—participants received either preventive or treatment-related health advice based on their assigned condition. (3) Interaction Style—the chatbot was programmed with either a formal, professional tone or an informal, casual style, as determined by the experiment's conditions. Each participant was required to engage in a conversation lasting between 10 and 13 min, during which they could click “End Conversation” at any time within this time frame. The conversation began with the chatbot presenting the experimental scenario and advice, and participants were asked to input questions into the chatbox based on the role they were simulating. Additionally, to better simulate real human interaction, the response speed of the chatbot in the high authority condition was deliberately slowed to match the average human typing speed. Privacy and data protection were strictly maintained—no personally identifiable information was collected, and all interactions were anonymized. The chatbot's responses were generated based on verified health guidelines, ensuring that the provided information was consistent with established medical recommendations. To further mitigate the risk of misinformation, the chatbot did not offer diagnostic opinions or prescribe treatment beyond general health advice. Examples of chatbot-generated text are shown in Table 1.
Examples of chatbot-generated text.
Examples of chatbot-generated text.
Lastly, after completing the interaction with the chatbot, participants took a post-test using the same seven-point Likert scale to again rate their willingness to adopt the health advice provided. The comparison between pre-test and post-test responses allowed us to assess the effects of the different experimental conditions on health decision-making.
We began by conducting three manipulation checks to ensure the validity of our experimental conditions.
Firstly, we verified the effectiveness of the chatbot identity manipulation. In the high authority condition, where participants were informed that they were interacting with a health expert from a well-known hospital, post-experiment interviews revealed that none of the participants realized that the “doctor” was actually a chatbot. This suggests that our manipulation of the chatbot's perceived authority was successful, as participants in the high authority condition fully accepted the identity of the chatbot as a credible health expert. To address the ethical concerns associated with deception, participants in the high authority chatbot condition were fully debriefed after the experiment, where they were informed that they had interacted with an AI chatbot rather than a real healthcare professional. This debriefing aimed to clarify the nature of the study and mitigate any potential psychological effects of the deception.
Secondly, we performed a manipulation check on the type of information provided to participants. After the experiment, we used a questionnaire to measure participants’ perceptions of the type of information they received, asking them to rate it on a scale from 1 (Preventive) to 7 (Treatment). As outlined in Table 2, an ANOVA was conducted to determine whether participants in the preventive and treatment conditions accurately perceived the type of information. The results demonstrated a significant difference between the groups, with participants in the preventive condition scoring an average of 1.96 (SD = 0.822), while participants in the treatment condition scored an average of 6.10 (SD = 0.810), F(1478) = 3084.186, p < 0.001. These results confirm that participants could clearly distinguish between preventive and treatment information, validating the effectiveness of this manipulation.
ANOVA results for the manipulation check on the type of information.

ANOVA results for the manipulation check on the type of information.
Note: SD = Standard Deviation. Mean represents the average score of perceived type of information.
Lastly, we examined the manipulation of the interaction style. After the experiment, participants were asked to rate the chatbot's interaction style on a scale from 1 (Informal) to 7 (Formal). As shown in Table 3, an ANOVA was performed to test whether participants correctly perceived the interaction style during the conversation. The analysis revealed a significant difference between the formal and informal groups. Participants in the formal interaction condition had a mean score of 6.34 (SD = 0.896), while those in the informal condition had a mean score of 2.01 (SD = 0.765), F(1478) = 3241.479, p < 0.001. These results indicate that participants successfully recognized the intended interaction style of the chatbot, confirming the effectiveness of this manipulation as well.
ANOVA results for the manipulation check on interaction style.

Note: SD = Standard Deviation. Mean represents the average score of perceived interaction style.
Following the manipulation checks, a repeated measures ANOVA was conducted to assess the main effects and interaction effects of chatbot role, type of information, and interaction style on participants’ willingness to adopt health advice over time. The results are presented in Table 4.
Main effects analysis repeated measures ANOVA results.
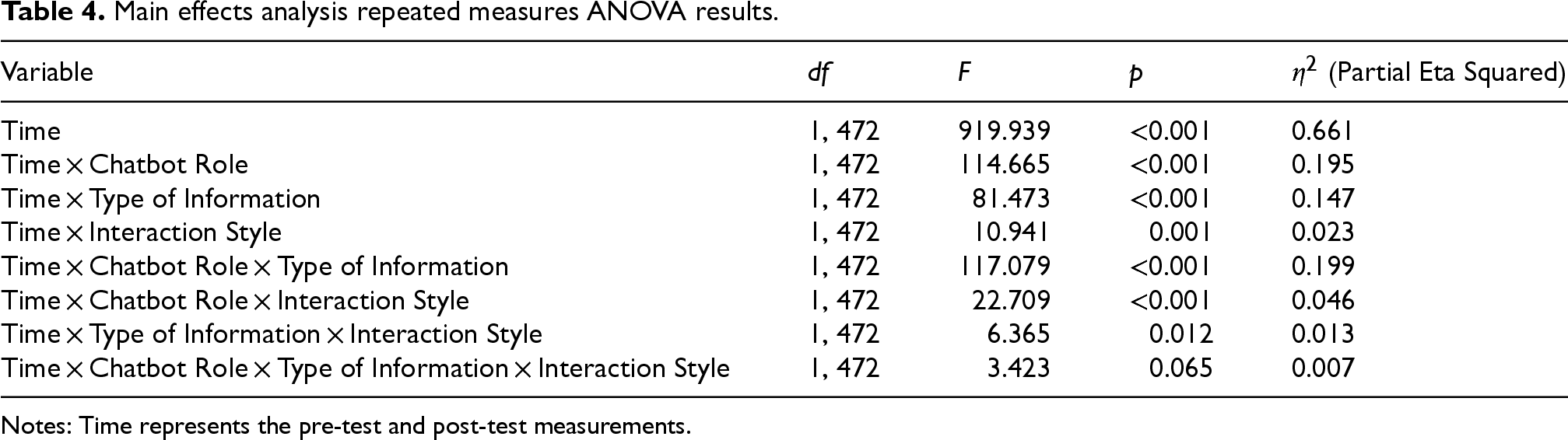
Notes: Time represents the pre-test and post-test measurements.
The analysis revealed a significant main effect of Time, F(1, 472) = 919.939, p < 0.001, η2 = 0.661, indicating a substantial increase in participants’ willingness to adopt health advice from pre-test to post-test. Additionally, a significant Time × Chatbot Role interaction was observed, F(1, 472) = 114.665, p < 0.001, η2 = 0.195, demonstrating that the effect of chatbot interaction on willingness to adopt advice varied based on whether the chatbot was framed as a general health assistant or as a doctor. Specifically, participants in the doctor chatbot condition exhibited a greater increase in willingness compared to those in the general chatbot condition. A significant Time × Type of Information interaction was also found, F(1, 472) = 81.473, p < 0.001, η2 = 0.147, indicating that the effectiveness of the chatbot interaction differed depending on whether it provided preventive or treatment-related information. Furthermore, the Time × Interaction Style interaction was significant, F(1, 472) = 10.941, p = 0.001, η2 = 0.023, indicating that participants’ willingness to adopt advice was influenced by the chatbot's interaction style.
The three-way interaction between Time, Chatbot Role, and Type of Information was also significant, F(1, 472) = 117.079, p < 0.001, η2 = 0.199, suggesting that the combined influence of chatbot identity and information type played a key role in shaping participants’ decision-making over time. Another significant three-way interaction was found for Time × Chatbot Role × Interaction Style, F(1, 472) = 22.709, p < 0.001, η2 = 0.046, indicating that chatbot authority and interaction style jointly affected how participants’ willingness evolved. Additionally, the Time × Type of Information × Interaction Style interaction was significant, F(1, 472) = 6.365, p = 0.012, η2 = 0.013, demonstrating that interaction style modulated the impact of information type on willingness.
Finally, the four-way interaction (Time × Chatbot Role × Type of Information × Interaction Style) was not statistically significant (F(1, 472) = 3.423, p = 0.065, η2 = 0.007). This indicates that while chatbot role, information type, and interaction style each influenced willingness to adopt health advice, their effects did not interact in a complex manner over time. Instead, their impact could be sufficiently explained by the three-way interactions discussed earlier.
To further analyze the impact of chatbot role, type of information, and interaction style on participants’ willingness to adopt health advice, we conducted paired-sample comparisons of pre-test and post-test scores. Table 5 presents the mean differences between pre- and post-test scores for each experimental condition.
Results of paired sample t-test.
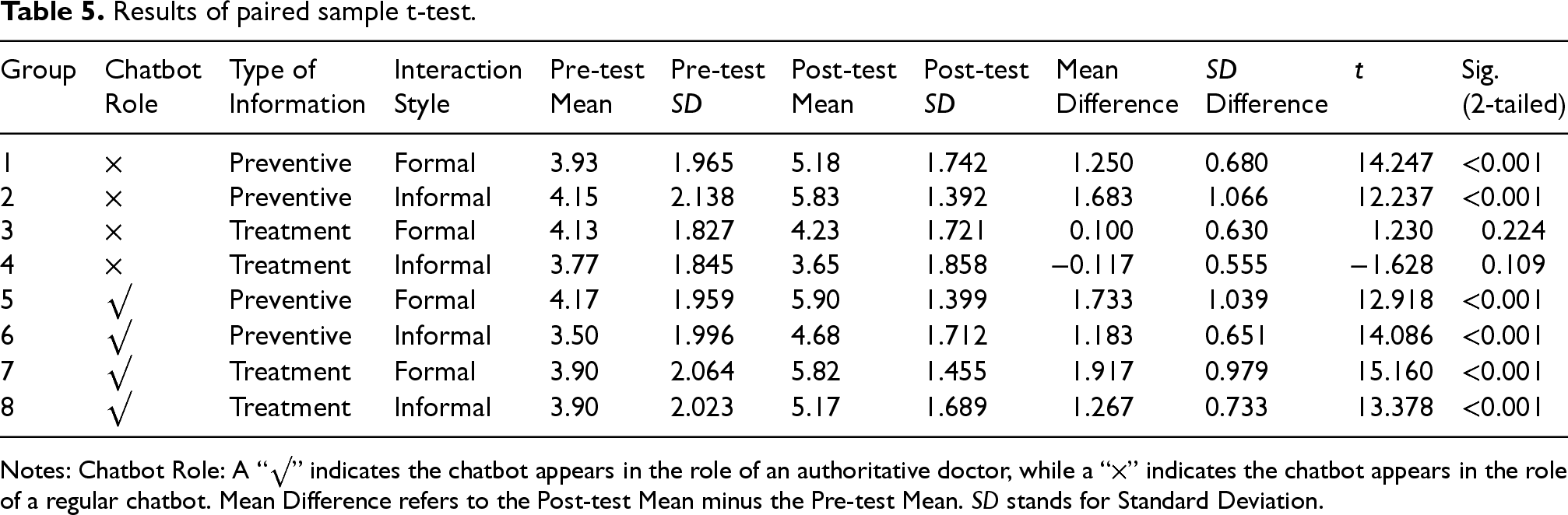
Notes: Chatbot Role: A “√” indicates the chatbot appears in the role of an authoritative doctor, while a “×” indicates the chatbot appears in the role of a regular chatbot. Mean Difference refers to the Post-test Mean minus the Pre-test Mean. SD stands for Standard Deviation.
Participants who interacted with a non-authoritative chatbot providing preventive information showed significant increases in willingness to adopt the advice. In the formal interaction condition, willingness increased from an initial mean of 3.93 (SD = 1.965) to a post-test mean of 5.18 (SD = 1.742), with a mean difference of 1.250 (t = 14.247, p < 0.001). Similarly, in the informal condition, willingness increased from an initial mean of 4.15 (SD = 2.138) to a post-test mean of 5.83 (SD = 1.392), with a larger mean difference of 1.683 (t = 12.237, p < 0.001). These findings indicate that a non-authoritative chatbot can effectively promote preventive health advice, with greater increases observed in the informal condition.
For the non-authoritative chatbot delivering treatment-related information, the changes in willingness were not significant in either interaction style (formal: t = 1.230, p = 0.224; informal: t = −1.628, p = 0.109), indicating that participants did not significantly adjust their willingness to follow the advice.
Participants who interacted with a authoritative chatbot providing preventive information also exhibited significant increases in willingness. In the formal condition, willingness rose from an initial mean of 4.17 (SD = 1.959) to a post-test mean of 5.90 (SD = 1.399), with a mean difference of 1.733 (t = 12.918, p < 0.001). In the informal condition, willingness increased from 3.50 (SD = 1.996) to 4.68 (SD = 1.712), with a mean difference of 1.183 (t = 14.086, p < 0.001), though the increase was smaller than in the formal condition.
Lastly, for the authoritative chatbot delivering treatment-related information, participants demonstrated significant increases in willingness in both interaction styles. In the formal interaction condition, willingness increased from an initial mean of 3.90 (SD = 2.064) to a post-test mean of 5.82 (SD = 1.455), with a mean difference of 1.917 (t = 15.160, p < 0.001). In the informal condition, willingness rose from an initial mean of 3.90 (SD = 2.023) to a post-test mean of 5.17 (SD = 1.689), with a mean difference of 1.267 (t = 13.378, p < 0.001), indicating that the formal style resulted in a slightly larger increase in willingness.
In summary, preventive information led to greater willingness in informal interaction styles when delivered by a non-authoritative chatbot, while treatment-related information had the greatest impact when delivered by a authoritative chatbot in a formal interaction style. Non-significant changes were observed in the non-authoritative chatbot conditions for treatment-related advice. These results answered RQ1–RQ3, demonstrating that chatbot identity (RQ1), the type of information provided (RQ2), and the interaction style (RQ3) all significantly influenced users’ health decision-making in varying contexts.
Our study aimed to explore how chatbot identity (authoritative vs. non-authoritative), the type of health information provided (preventive vs. treatment), and the interaction style (formal vs. informal) influence users’ health decision-making. By employing the media evocation paradigm, we extended beyond the traditional CASA framework to examine how different factors affect user behavior when interacting with chatbots in health contexts. The results highlight the complex ways in which these elements interact to shape users’ willingness to adopt health advice, with significant implications for both theory and practice.
Chatbot identity and perceived authority
The media evocation paradigm provides a more nuanced understanding of human-chatbot interactions compared to the traditional CASA model. Unlike CASA, which treats human-computer interactions as inherently similar to human-to-human communication, 53 the media evocation paradigm suggests that chatbots occupy a middle ground between human and machine. 23 In our study, when the chatbot was framed as a “real” doctor—through the authoritative identity manipulation—participants perceived it as more credible and trustworthy. This “real-world” tag that the authoritative doctor identity created seemed to bridge the gap between human and machine, making users more receptive to the chatbot's advice, particularly for treatment-related information.
This finding underscores the importance of framing in chatbot-mediated health communication. The media evocation paradigm suggests that by blurring the lines between human and machine, chatbots can evoke emotional and cognitive responses that increase engagement and trust. 54 In this way, framing a chatbot as an authoritative health expert, rather than a mere machine, can significantly influence users’ health decisions, a distinction that CASA does not fully capture. Users’ acceptance of chatbots labeled as health experts illustrates that chatbot authority can prompt users to engage with the chatbot on a deeper level, perceiving it as a “social actor” yet still distinct from purely human interaction. 55
Type of information: Preventive vs. treatment advice
The findings regarding the type of information provided by the chatbot—whether preventive or treatment-related—also highlight the role of context in health communication. Treatment-related advice, which tends to be more immediate and relevant to users’ current health conditions, was better received when delivered by an authoritative chatbot in a formal tone. This aligns with the literature that emphasizes the urgency and personal relevance of treatment advice.56,57 The media evocation paradigm can help explain these results by suggesting that authoritative chatbots providing critical, treatment-related advice evoke a heightened sense of importance and urgency, prompting users to take action.
Conversely, preventive information, which is more future-oriented, was more effective when delivered informally by non-authoritative chatbots. This suggests that users may respond better to informal, approachable tones when there is less immediate risk involved. The media evocation paradigm further supports this interpretation, as it argues that media objects, such as chatbots, can evoke responses that are context-dependent. Preventive advice may seem less urgent, and users may feel more comfortable engaging with a less authoritative, more casual chatbot in these scenarios. 58 Thus, framing and interaction style play pivotal roles in whether users will act on preventive health advice.
Interaction style: Formal vs. informal communication
Interaction style also significantly influenced health decision-making in this study. Formal communication was more effective in contexts where authority and expertise were important, particularly for treatment-related advice. This aligns with the broader health communication literature, which suggests that formal tones convey professionalism and increase user trust. 59 The media evocation paradigm complements this understanding by proposing that media can evoke reflective and critical engagement from users, particularly when presented in a formal, professional manner that commands authority.
On the other hand, informal interaction styles were more effective for delivering preventive advice, especially when the chatbot was non-authoritative. Informal styles seem to foster a sense of comfort and engagement, making users more likely to interact with the chatbot and adopt its advice in non-urgent contexts. This finding supports the notion that informal communication can reduce user anxiety, making the chatbot more approachable and relatable. 51 The media evocation paradigm suggests that the less rigid, more conversational tone of informal chatbots might evoke a sense of trust and openness, especially when the perceived stakes are lower. 60
Implications for health communication and public health campaigns
Our findings align with broader health communication literature, particularly research on public health campaigns and digital health interventions. Studies have shown that the effectiveness of health messaging is influenced by both the source's perceived authority and the message's framing. 61 For instance, in traditional public health campaigns, messages delivered by healthcare professionals or government agencies are more likely to be trusted and acted upon, especially when conveying urgent health recommendations, such as vaccination uptake or disease prevention measures. 62 Similarly, authoritative chatbots in our study were more effective in promoting compliance with treatment-related advice, suggesting that chatbots designed for medical guidance should integrate credibility-enhancing strategies similar to those used in public health communication.
Moreover, our results echo findings from digital health interventions where message personalization and interaction style impact user engagement and adherence to health advice. 63 Studies in mobile health (mHealth) and telemedicine platforms suggest that formal, professional tones enhance trust and compliance, particularly when addressing chronic disease management or post-diagnosis care. 64 Meanwhile, informal, conversational approaches are commonly used in health promotion campaigns targeting lifestyle behaviors, such as smoking cessation or physical activity, as they foster a sense of approachability and relatability, reducing resistance to behavior change. 65 Our study similarly found that informal chatbots were more effective at delivering preventive health advice, reinforcing the idea that message tone should be tailored to the type of health information being conveyed.
Theoretical and practical implications
From a theoretical perspective, our study extends the media evocation paradigm by providing empirical evidence that chatbots can evoke different levels of user engagement based on how they are framed. Specifically, the results show that chatbot identity, interaction style, and the type of health information provided can significantly influence how users perceive and interact with the chatbot. Unlike CASA, which primarily emphasizes automatic, mindless responses to machines, the media evocation paradigm accounts for more reflective and complex user behaviors. By presenting chatbots as authoritative figures in healthcare, users are prompted to engage more deeply with the advice provided, especially when the advice is treatment-related and presented in a formal manner.
In terms of practical implications, our findings suggest several strategies for designing more effective health chatbots. First, chatbots delivering treatment-related advice should be designed to project authority, either by framing them as health experts or by using a formal interaction style. This approach is likely to increase trust and compliance with critical health recommendations. Second, for preventive health advice, chatbots may benefit from a more informal, conversational tone, particularly if they are not framed as authoritative figures. This can increase user engagement and willingness to adopt long-term health behaviors, especially when the advice is not immediately urgent. Furthermore, our study highlights the importance of tailoring chatbot communication strategies to the specific health context. Chatbots that deliver high-stakes, treatment-related advice should emphasize authority and professionalism, while those offering more general, preventive advice may benefit from a more approachable, informal interaction style. These insights can inform the design of AI-driven health communication tools, making them more effective in supporting a range of health behaviors.
Conclusion
In conclusion, this study contributes to the understanding of how chatbot identity, the type of health information, and interaction style influence health decision-making. By integrating the media evocation paradigm, we have provided new insights into how chatbots can evoke different levels of user engagement depending on how they are framed and how they communicate. The findings suggest that authoritative chatbots with formal interaction styles are particularly effective for delivering treatment-related advice, while informal, non-authoritative chatbots are better suited for promoting preventive health behaviors.
However, several limitations should be noted. Firstly, the study's sample consisted solely of university students, limiting the generalizability of the findings to broader populations, including older adults, individuals with chronic conditions, and those with varying levels of digital literacy. Future research should explore whether these findings hold across diverse demographic groups. Secondly, the study focused on short-term willingness to adopt chatbot advice, without assessing long-term adherence or actual behavioral changes. Follow-up studies are needed to investigate whether users sustain chatbot-recommended health behaviors over time. Thirdly, while the study measured participants’ perceived willingness to adopt health advice, it did not include physiological or clinical validation, such as treatment adherence or changes in biomarkers. Future research could integrate objective health measures, such as wearable tracking or medical compliance data, to assess real-world effectiveness. Fourthly, participants were not actual patients making real healthcare decisions, which may affect the external validity of the findings. Future studies should test chatbot interventions in real healthcare settings with individuals actively seeking medical guidance. Fifthly, the authoritative and non-authoritative chatbot conditions were confounded by differences in framing—participants perceived authoritative chatbots as human doctors, while non-authoritative chatbots were explicitly identified as AI-generated assistants. This distinction may have influenced participants’ trust and willingness to adopt the advice, highlighting the need for more refined experimental manipulations in future studies. Finally, despite adherence to verified health guidelines, AI-generated misinformation remains a concern, especially for authoritative chatbots that may evoke higher trust. While the chatbot did not diagnose or prescribe treatments, AI models can still produce misleading information with high confidence. Future research should explore mechanisms for integrating expert validation and transparency measures to enhance the reliability and safety of AI-assisted health communication.
Overall, this study advances both theory and practice in chatbot-mediated health communication, providing a deeper understanding of how to design more effective AI-driven tools for promoting health decision-making.
Footnotes
Acknowledgements
Thanks to all the participants in the study.
Ethical approval
The studies involving human participants were reviewed and approved by the Ethics Committee of Shanghai Jiao Tong University (code. H20240428I). The participants provided their written informed consent to participate in this study. The study complies with the Declaration of Helsinki.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will be made available on request.