
Abstract
Background
There are many types of gastrojejunostomy reconstruction after laparoscopy-assisted distal gastrectomy (LADG) for gastric cancer, each of which has merit and demerit.
Objective
In order to reduce the incidence of postoperative complications after LADG, we designed a novel method—the “Pants-shaped” anastomosis that involves the gastrojejunostomy anastomosis and evaluated its clinical application effect.
Methods
In this retrospective study, data of 630 cases of laparoscopy-assisted distal gastrectomy performed in the First Affiliated Hospital of Wannan Medical College from January 2018 to December 2022 were analyzed. The cases were divided into three groups: “Pants-shaped” anastomosis group (n = 127), Billroth II anastomosis group (n = 242), and Billroth II + Braun anastomosis group (n = 261) according to the different types of gastrojejunostomy reconstruction.
Results
The laparoscopic operations of all 630 patients were successfully performed. There were no significant differences in intraoperative blood loss, the number of lymph nodes, and complications among the three groups (P > 0.05). The “Pants-shaped” group resulted in shorter time to first flatus (P = 0.004), shorter postoperative time (P = 0.008), longer anastomosis time (P < 0.05), and lower hospitalization costs (P < 0.05) than the Billroth II group; and shorter operation time and shorter postoperative time (P = 0.008), and lower hospitalization costs (P < 0.05) than the Braun group. There were significant statistical differences in the early postoperative complications among the three groups (P > 0.05). The “Pants-shaped” group showed less reflux gastritis (P = 0.022) in the postoperative 5 years follow-up compared to the Billroth II group.
Conclusion
The procedure of “Pants-shaped” anastomosis is safe and feasible, which can be easily performed. It can be a good option with shorter postoperative time and less reflux gastritis.
Keywords
Introduction
Gastric cancer is the second-most common cancer of all malignant tumors in Asian countries, 1 and the number of new cases is increasing every year. Surgery is the only curative treatment for gastric cancer. In 1994, professor Kitano 2 was the first to report laparoscopy-assisted distal gastrectomy (LADG) for early gastric cancer. With further advancements in the past two decades, the safety and long-term efficacy of LADG are now widely recognized. Scholars confirmed the safety and feasibility of laparoscopic radical gastrectomy. 3 There are a variety of reported methods for reconstruction of the digestive tract after LADG, such as Billroth I, Billroth II, and Roux-en-Y anastomosis, among others. 4 However, each of these reconstruction methods have drawbacks, such as reflux gastritis and anastomotic ulcer. Therefore, we devised a novel method—the “Pants-shaped” anastomosis-that involves the gastrojejunostomy anastomosis after LADG.
Pants-shaped anastomosis is a new type of gastrojejunostomy technique, which is mainly used in LADG. This technology is characterized by imitating the shape of pants, through a specific anastomosis to achieve the connection between the esophagus and the jejunum. 5 In traditional gastrojejunostomy techniques, straight or curved methods are usually used for anastomosis. However, the ‘Pants-shaped’ anastomosis technique changes the direction and angle of anastomosis to form a structure similar to pants, which can better adapt to the natural course of the digestive tract and reduce the risk of postoperative complications. 6 It can improve the postoperative life quality of patients. In summary, ‘Pants-shaped’ anastomosis technique is an innovative surgical approach that mimics the shape of pants for gastrojejunostomy with aims to enhance safety, feasibility, and effectiveness of surgery.
We believe that using this technique can reduce the difficulties encountered with the anastomosis, as well as the incidence of complications. Thus, this study aimed to compare the clinical outcomes of patients with gastric cancer undergoing digestive tract reconstruction with ‘Pants-shaped’ anastomosis, Billroth II anastomosis, or Billroth II + Braun anastomosis after LADG, with a follow-up period of 5 years.
Materials and methods
General information
From January 2018 to December 2022, data were collected from 630 patients who underwent LADG in the First Affiliated Hospital of Wannan Medical College. Inclusion criteria: (1) Successful completion of laparoscopic assisted radical resection of distal gastric cancer; (2) Aged 18–85 years. Exclusion criteria: (1) other malignant tumors; (2) Neoadjuvant chemotherapy was performed before surgery; (3) complicated with serious medical disease; The patients were divided into three groups according to the type of gastrojejunostomy reconstruction after LADG: “Pants-shaped” anastomosis group (n = 127), Billroth II group (n = 242), and Braun group (n = 261). The follow-up period for all patients was 5 years. The following clinicopathological data were collected: age, sex, body mass index (BMI), histology type, TNM stage, type of anastomosis, blood loss, operation time, postoperative days, anastomosis time, postoperative complications, and cost of total surgical consumables. The evaluation of postoperative complications was diagnosed by clinical manifestations, gastroscopy, and digestive tract radiography. This study was approved by the ethics committee of First Affiliated Hospital of Wannan Medical College (No. YJSYY20180502).
The “pants-shaped” anastomosis step
All patients underwent laparoscopic lymph node dissection according to the D2 radical surgery criteria. 7 After completion of the lymph node dissection, the digestive tract is reconstructed. The Billroth II anastomosis and Billroth II + Braun anastomosis procedures were performed according to conventional methods. The “Pants-shaped” anastomosis method is as follows: First, a purse-string suture of about 2 cm was performed on the opposite side of the mesangial margin in the jejunum. About 20 cm below the ligament of Treitz, the intestinal wall was cut longitudinally. The two limbs of the stapler were inserted into the afferent and efferent loops, respectively; then, the forks of the stapler were closed and fired, achieving a side-to-side jejunojejunostomy (Figure 1a). After exiting the stapler, active bleeding of the jejunojejunostomy was sutured under direct vision. Second, the 29-mm circular stapler was inserted into the longitudinal jejunum incision (Figure 1b). Third, the anastomosis of the greater curvature of the residual stomach to the jejunum was performed (Figure 1(c)). Fourth, a 60-cm liner stapler was used to close the lesser curvature of the residual stomach. We removed the specimen through the auxiliary small incision on the upper abdomen, which completed the “Pants-shaped” anastomosis (Figure 1(d)).
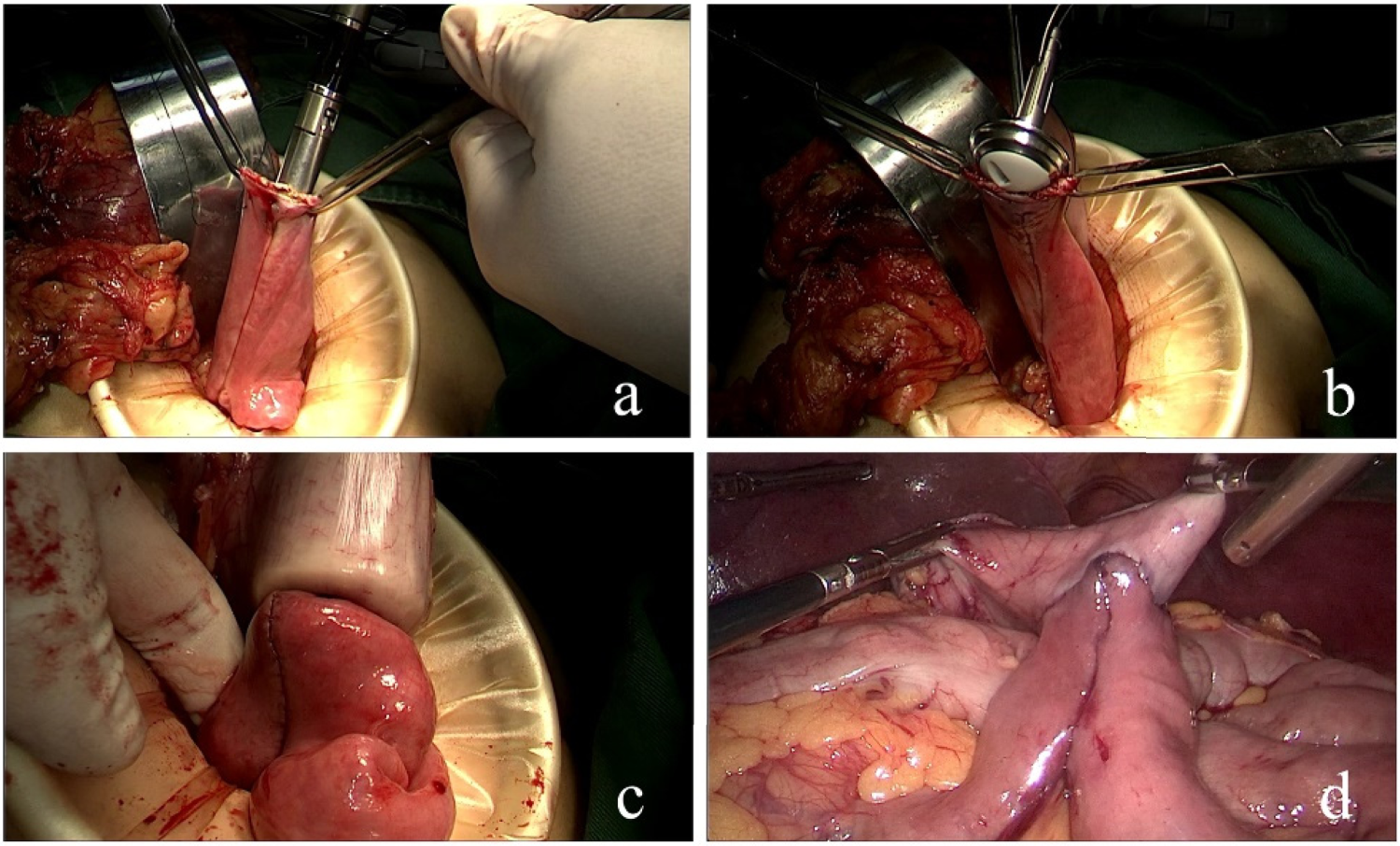
The schematic diagram of “pants-shaped” anastomosis after LADG. (a) The two limbs of the stapler are inserted into the afferent and efferent loops respectively, to achieve side-to-side jejunojejunostomy. (b) A 25-mm circular stapler is inserted into the longitudinal jejunum incision. (c) Completion of gastrojejunostomy. (d) “Pants-shaped” anastomosis is completed.
Statistic Package for Social Science (SPSS) 21.0 (SPSS Inc., Chicago, IL, USA) statistical software was used to perform statistical analyses. The t-tests were performed to compare continuous variables. The chi-square test was performed to compare categorical variables. p < 0.05 was considered to indicate statistical significance.
Results
Basic data comparison among the three groups
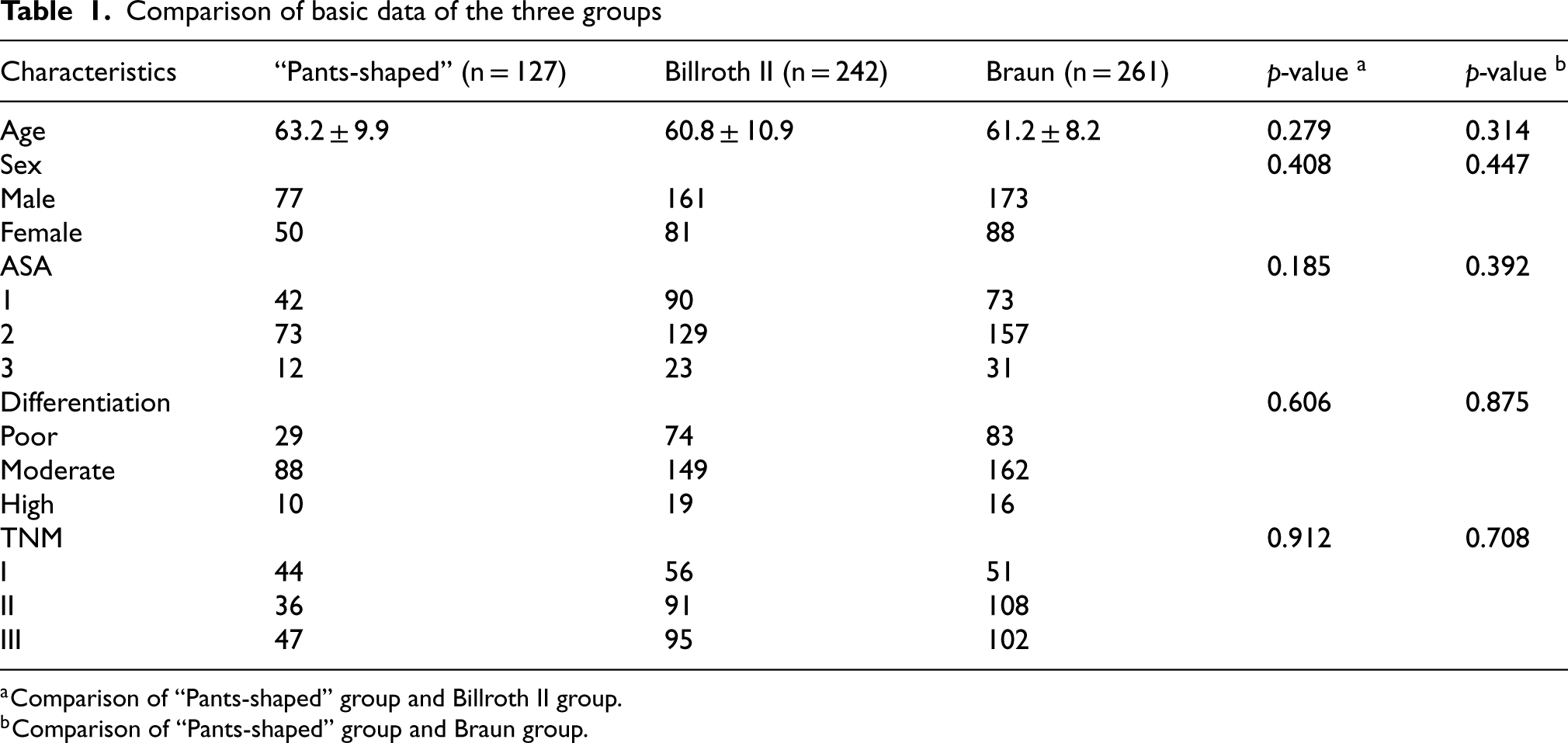
There were no significant differences in age, sex, American Society of Anesthesiologists(ASA), degree of differentiation of tumor cells, and TNM stage among the three groups (p > 0.05, Table 1).
Comparison of basic data of the three groups
Comparison of basic data of the three groups
Comparison of “Pants-shaped” group and Billroth II group.
Comparison of “Pants-shaped” group and Braun group.
The “Pants-shaped” anastomosis group showed shorter time to first flatus (p = 0.004), shorter postoperative time (p = 0.008), and lower hospitalization costs (p < 0.05), but longer anastomosis time (p < 0.05) than the Billroth II group. Moreover, the “Pants-shaped” anastomosis group showed shorter operation time (p < 0.05), shorter postoperative time (p < 0.05), and lower hospitalization costs (p < 0.05) than the Braun group (Table 2).
Comparison of surgical indicators among the three groups

Comparison of surgical indicators among the three groups
Comparison between “Pants-shaped” group and Billroth II group.
Comparison between “Pants-shaped” group and Braun group.
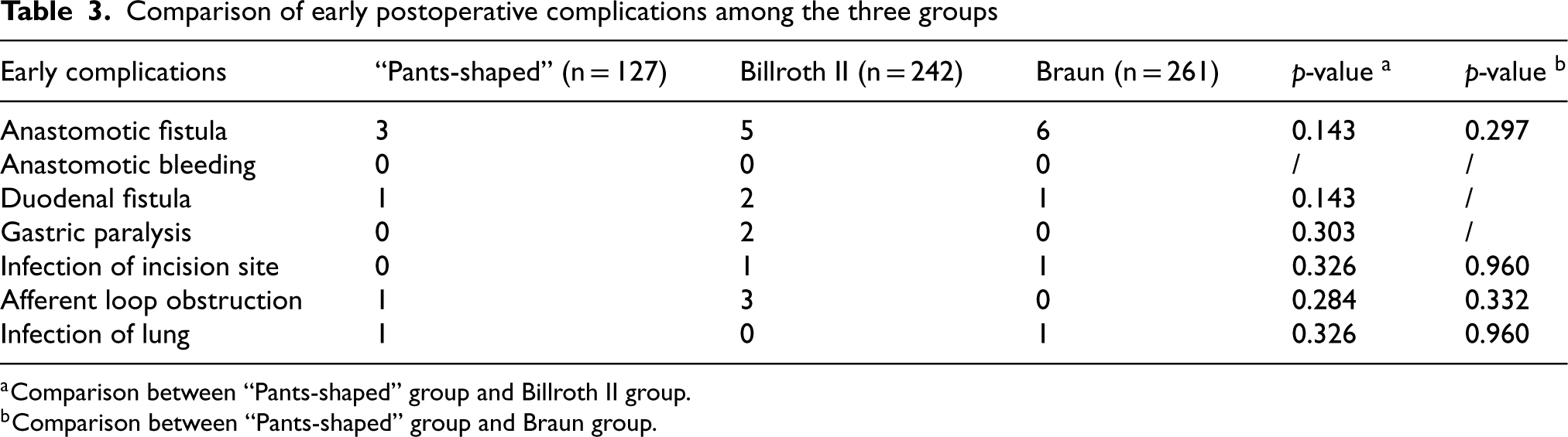
There were no significant statistical differences in the early postoperative complications among the three groups (p > 0.05) (Table 3).
Comparison of early postoperative complications among the three groups
Comparison of early postoperative complications among the three groups
Comparison between “Pants-shaped” group and Billroth II group.
Comparison between “Pants-shaped” group and Braun group.
Gastroscopy and upper gastrointestinal radiography were performed in all patients during follow-up in 5 years. The patients confirmed that there were no digestive tract symptoms such as acid regurgitation and belching after the operation. Upper gastrointestinal radiography showed that the anastomosis was unobvious and contrast medium easily entered the efferent loop of the intestine (Figure 2). There were no significant differences with respect to dumping syndrome and anastomotic ulcer among the three groups (p > 0.05). However, in reflux gastritis, the incidence in “Pants-shaped” group was lower than the Billroth II group (p = 0.022) (Table 4).

Post-operative upper gastrointestinal radiography at the 5-year follow-up.
Comparison of postoperative complications after 5 years among the three groups

Comparison of “Pants-shaped” group and Billroth II group.
Comparison of “Pants-shaped” group and Braun group.
China is the region with a high incidence of advanced gastric cancer, and the location of the gastric cancer is often the antrum of the stomach. Currently, surgery is the main method to treat gastric cancer. The procedure of radical gastrectomy for gastric cancer includes partial/total gastrectomy, lymph node dissection, and reconstruction of the alimentary tract. Since the first LADG was reported by professor Kitano, 2 laparoscopic techniques have been rapidly developed for the advantages of faster recovery and fewer postoperative complications. These benefits are reportedly attributed to the minimal invasiveness of laparoscopy and good clinical outcomes. 8 Currently, the digestive tract reconstruction methods used after LADG include Billroth I anastomosis, Billroth II anastomosis, Billroth II + Braun anastomosis, Roux-en-Y anastomosis, and uncut Roux-en-Y anastomosis. Each method of digestive tract reconstruction has its merits and demerits. Postoperative specimens need to be obtained through a small incision under the upper abdomen, and the digestive tract reconstruction is performed through this small incision after lymphadenectomy. Compared with the totally laparoscopic reconstruction of the digestive tract, the advantage of using the auxiliary small incision to reconstruct the digestive tract is simple, time saving, and cost effective. Therefore, laparoscopy-assisted radical gastrectomy for distal gastric cancer is the preferred method to reconstruct the digestive tract in China.
According to Japanese Gastric Cancer Treatment Guidelines, Billroth I was the most common reconstruction in Japan, 9 followed by Roux-en-Y. Due to the high incidence of bile reflux esophagitis, Billroth II reconstruction is rarely performed in Japan. Billroth I anastomosis is most commonly used for early gastric cancer with small tumor diameter, because it is simple to perform and closely resembles normal anatomy and physiology. However, the disadvantage is that it may result in pathological positive margin in order to reduce the tension of the anastomotic site. In China, given that most patients with gastric cancer have advanced disease, the method of reconstructing the digestive tract is typically Billroth II or others, but not Billroth I. In contrast to Billroth I, the Billroth II approach has an adequate excision range and is beneficial for the recovery of gastrointestinal function. Furthermore, the Billroth II approach reduces the incidence of anastomotic ulcer and residual stomach. Hence, a large number of surgeons choose Billroth II anastomosis for patients with advanced gastric cancer. However, with the exception of bile reflux esophagitis, Billroth II approach also has many disadvantages such as intestinal obstruction, alkaline reflux gastritis, and dumping syndrome. The reason for alkaline reflux gastritis is not only directly associated with the bile traveling directly into the residual stomach but also with the time: the longer the time, the worse the symptoms. Yang 10 reported that the incidence of alkaline reflux gastritis was high (∼72%). In the present study, there were statistically significant differences in terms of alkaline reflux gastritis, with one (2.3%) and seven (16.7%) patients, respectively, in the “Pants-shaped” group and Billroth II groups. Afferent loop obstruction is the second-most common complication of Billroth II anastomosis after distal gastric resection, which is caused by the shorter afferent loop. The incidence of duodenal stump fistula caused by afferent loop obstruction was between 30 and 60%. In the present study, the incidence of afferent loop obstruction by “Pants-shaped” anastomosis was 2.3%. In 1987, professor Braun 11 proposed the concept of the Billroth II + Braun anastomosis, and recent studies have shown that Braun anastomosis can reduce the incidence of complications of the afferent loop obstruction and bile reflux gastritis. However, the auxiliary small incision of about 5–8-cm diameter increased the difficulty to perform the Braun anastomosis. Roux-en-Y anastomosis can reduce the anastomosis tension, as the stomach contents directly enter into the distal jejunum and reduce the incidence of delayed gastric emptying and occurrence of bile reflux gastritis. 12 However, Roux-en-Y anastomosis destroys the normal intestinal electrophysiological activities, affecting the migrating motor complex (MMC) and interstitial cells of Cajal (ICC) 13 and resulting in Roux-Y stasis syndrome. The incidence of Roux-Y stasis syndrome is about 10–30%. 14 Some experts proposed the uncut Roux-en-Y anastomosis for Roux retention syndrome, but this approach has the possibility of recanalization. 15
After evaluating the advantages and disadvantages of the different approaches to digestive tract reconstruction after LADG, we designed a novel gastrojejunostomy approach—”Pants-shaped” anastomosis—named so because the shape is similar to a pair of pants after the anastomosis has been completed. Compared with the Billroth II + Braun anastomosis, “Pants-shaped” can be performed through an auxiliary small incision without lengthening the incision, and the anastomosis can be accomplished under direct vision without further complicating the procedure or increasing operation time, thereby avoiding the false injury and inaccurate anastomosis. Compared with the traditional Billroth II approach, the “Pants-shaped” procedure amounts to an increase in the diameter of the gastrojejunostomy, such that the biliary and pancreatic juice directly travel into the jejunum without through the residual stomach. Therefore, the incidence of duodenal stump fistula caused by the afferent loop obstruction can be reduced. In the present study, compared with the Billroth II and Braun groups, the “Pants-shaped” group increased the cost of an endoscopic gastrointestinal anastomosis (Endo-GIA) stapler, but the total hospitalization costs did not increase. The likely reason is that because the hospitalization time increased in both the Billroth II and Braun groups, this led to an increased total cost of hospitalization. The “Pants-shaped” group showed longer anastomosis time than the Billroth II group, but there was no significant statistical difference in the operation time. The “Pants-shaped” group showed shorter operation time than the Braun group.
Our study has some limitations. First, this study is a retrospectively designed, single-center analysis. Second, the long-term curative effects of the “Pants-shaped” anastomosis were not confirmed. Third, the sample size was small. We need to expand the sample size to observe the long-term effect of the “Pants-shaped” anastomosis. In addition, the “Pants-shaped” anastomosis makes the two anastomoses merge into one, so the final anastomosis will have a “T” shape anastomosis line, we call it the “Pants-shaped” anastomosis triangle. In theory, this is the point with the worst blood supply in the entire anastomotic area and deserves the surgeon's special attention. In clinical practice, we did find that the color of the intestinal wall in the “Pants-shaped” anastomosis triangle area was darker than the surrounding area, confirming that the blood supply in this area was the weaker. Another limitation of this study is the absence of a formal, quantified assessment of patients’ quality of life, as we relied on subjective feedback rather than an objective tool to measure QofL outcomes. Therefore, how to minimize the ischemic range and protect the whole anastomotic blood supply is the key to the success of the whole operation, and it is also a clinical problem worthy of further study. Therefore, future investigators should expand the sample size and analyze the long-term effects in their studies.
Conclusion
The “Pants-shaped” anastomosis represents a novel approach to gastrojejunostomy reconstruction, addressing key limitations of traditional techniques. By creating a more physiologically aligned anastomosis, this method reduces complications like reflux gastritis while maintaining surgical efficiency. The lower hospitalization costs observed in the “Pants-shaped” group highlight its economic advantages despite longer anastomosis times. These findings underscore the technique's potential to improve postoperative outcomes and quality of life for patients undergoing LADG.
While the study demonstrates promising results, limitations include its retrospective design, single-center scope, and relatively small sample size. Future research should focus on multi-center trials with larger cohorts to validate these findings and explore long-term outcomes further.
In conclusion, the “Pants-shaped” anastomosis has shorter time to first flatus, shorter postoperative time and less reflux gastritis. It can improve the postoperative life quality of patients. Therefore, the “Pants-shaped” anastomosis after LADG for gastrojejunostomy reconstruction is relatively simple and has faster recovery for gastrointestinal function. It is a flexible procedure to choose for gastrojejunostomy reconstruction.
Footnotes
Ethical considerations
This study was approved by the ethics committee of The First Affiliated Hospital of Wannan Medical College.
Author contributions
BW and LS designed the study and performed the experiments, ZW, GL and BL collected the data, WY and CY analyzed the data, YD and ZY prepared the manuscript. All authors read and approved the final manuscript.
Funding
This work was supported by the Key Scientific Research Foundation of the Education Department of Province Anhui (2022AH051241).Wannan Medical College young and middle-aged key subject(WK2023ZZD30).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.