
Abstract
Background
Organisational change in complex healthcare systems is a multifaceted process. The English National Health Service recently introduced a ‘Change Model’ that seeks to offer an evidence-based framework for guiding change. We report findings from a formative evaluation of the NHS Change Model and make recommendations for those developing the Model and its users.
Methods
The evaluation involved 28 interviews with managers and clinicians making use of the Change Model in relation to a variety of projects. Interviews were fully transcribed and were analysed using an approach based on the Framework method.
Findings
Participants saw the Change Model as valuable and practically useful. Fidelity to core principles of the Model was variable: participants often altered the Model, especially when using it to orchestrate the work of others. In challenging organisational contexts, the Change Model was sometimes used to delegitimise opposition rather than identify shared purpose among different interest groups.
Conclusions
Those guiding change may benefit from frameworks, guidance and toolkits to structure and inform their planning and activities. Participants’ experiences suggested the Change Model has much potential. Further work on its design and on supporting materials may optimise the approach, but its utility rests in particular on organisational cultures that support faithful application.
Background
In common with many Organisation for Economic Co-operation and Development (OECD) healthcare systems, the English National Health Service (NHS) faces a ‘perfect storm’ of challenges: increasing demand due to demographic change, the shift in disease burden towards chronic conditions and resource constraint. The need to increase throughput and quality with static or contracting resources has provoked a renewed interest in tools for improvement and change management to assist managers with the task of achieving sustainable change in challenging circumstances.
Change-management tools are not a new phenomenon. Early approaches, such as Lewin’s force-field analysis and ‘unfreeze-change-refreeze’ model, 1 remain influential today,2,3 along with several other frameworks with a grounding in organisational psychology. Models of this sort have, however, come in for criticism, particularly when applied in public service contexts. First, they are often rather linear in presentation, suggesting that the key to effecting change is stepwise application of (often behavioural) interventions.2,4 Second, and relatedly, change-management models often focus on the ‘top-down’ actions of senior managers in organisations, neglecting the acts and omissions of those lower down in organisational hierarchies – which can be crucial in initiating, modifying or stymieing change.4,5 Change, then, is constructed in overly rationalistic and planned terms; the importance of emergent influences on change arising from complex systems is underplayed. Third, most such frameworks have been developed in private sector contexts and are arguably less well suited to public services characterised by diffuse power, ambiguous aims and strong policy and professional influences.2,6,7 Application of such frameworks in healthcare systems can therefore be problematic, given the number of examples of change efforts that have been obstructed or undone by organisational challenges, professional opposition and divergent incentive structures.8–12
One attempt to overcome the limitations of existing frameworks is the recently developed NHS Change Model (www.changemodel.nhs.uk). A framework for planning, introducing and sustaining small- and large-scale change, the Change Model seeks to incorporate the most useful aspects of existing tools and frameworks in a way that is sensitive to the particularities of the English healthcare system.
13
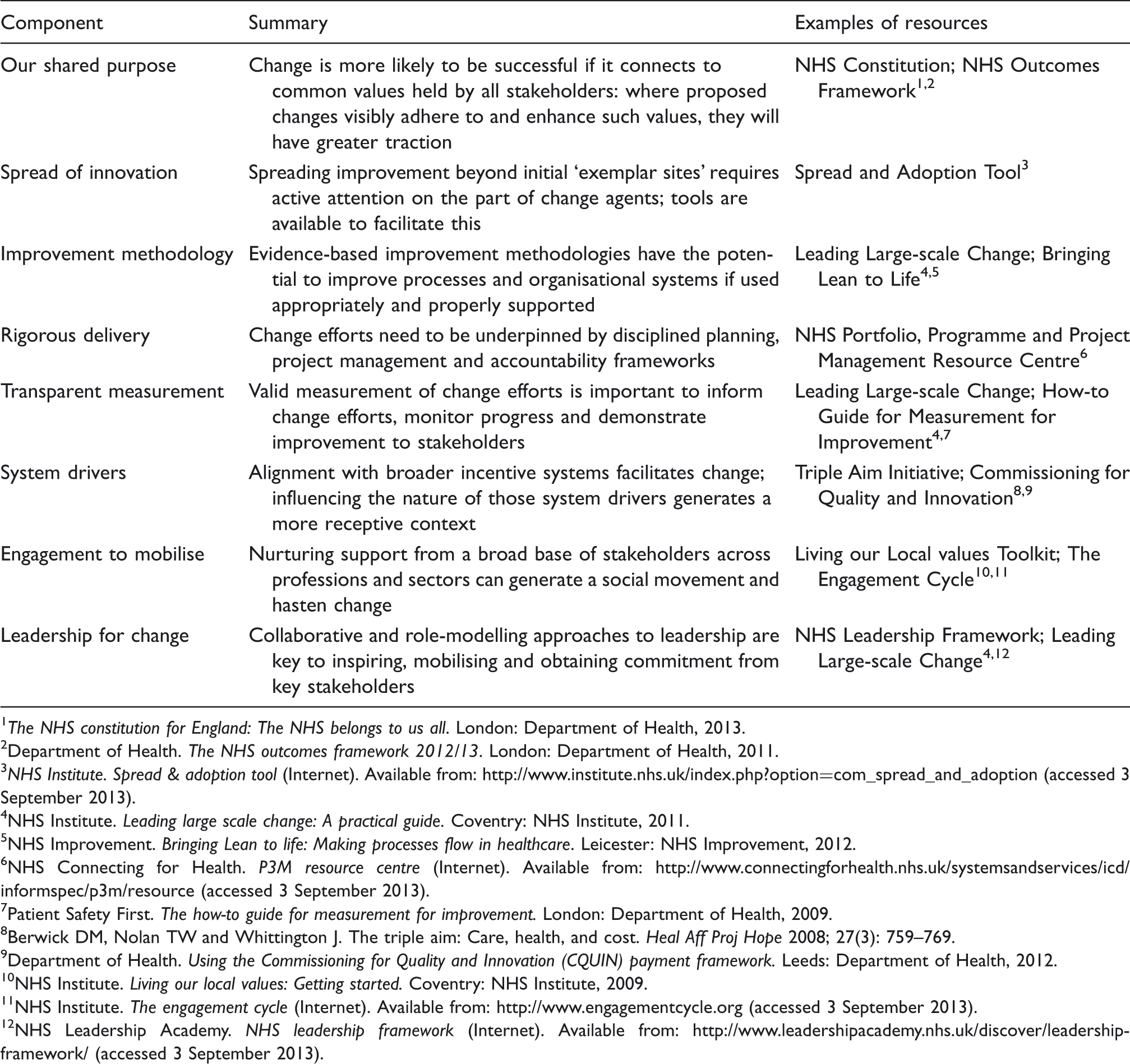
Developed by the former NHS Institute for Innovation and Improvement, the Change Model draws on evidence-derived tools and approaches from diverse fields – including organisational development, management and leadership and improvement science14–18 – to offer an approach to change that seeks to be comprehensive, multifaceted and accessible to NHS staff (see Figure 1 and Table 1). A key objective is to generate alignments between aspects of change that may be in tension – for example, the intrinsic motivations of professionals and extrinsic pushes such as financial pressures – and ensure that all change is founded on and articulated in terms of the common goals of the NHS.
16
It is explicitly presented as a non-linear model, whose eight components are interdependent, of equal importance and to be constantly revisited throughout the process of change rather than ‘checked off’ sequentially. The Change Model has been adopted by NHS England, the newly constituted body with overall responsibility for strategic development in the restructured health service, as its framework for organising improvement activities across the NHS.19,20
The NHS Change Model. The components of the NHS Change Model in sum (see also www.changemodel.nhs.uk). The NHS constitution for England: The NHS belongs to us all. London: Department of Health, 2013. Department of Health. The NHS outcomes framework 2012/13. London: Department of Health, 2011. NHS Institute. Spread & adoption tool (Internet). Available from: http://www.institute.nhs.uk/index.php?option=com_spread_and_adoption (accessed 3 September 2013). NHS Institute. Leading large scale change: A practical guide. Coventry: NHS Institute, 2011. NHS Improvement. Bringing Lean to life: Making processes flow in healthcare. Leicester: NHS Improvement, 2012. NHS Connecting for Health. P3M resource centre (Internet). Available from: http://www.connectingforhealth.nhs.uk/systemsandservices/icd/informspec/p3m/resource (accessed 3 September 2013). Patient Safety First. The how-to guide for measurement for improvement. London: Department of Health, 2009. Berwick DM, Nolan TW and Whittington J. The triple aim: Care, health, and cost. Heal Aff Proj Hope 2008; 27(3): 759–769. Department of Health. Using the Commissioning for Quality and Innovation (CQUIN) payment framework. Leeds: Department of Health, 2012. NHS Institute. Living our local values: Getting started. Coventry: NHS Institute, 2009. NHS Institute. The engagement cycle (Internet). Available from: http://www.engagementcycle.org (accessed 3 September 2013). NHS Leadership Academy. NHS leadership framework (Internet). Available from: http://www.leadershipacademy.nhs.uk/discover/leadership-framework/ (accessed 3 September 2013).
Critical to the Change Model’s ability to deliver on its goals will be how far it offers an accessible, useable and appealing framework for managers and clinicians in the NHS charged with making change happen. Early appraisal of its strengths and weaknesses in this regard can help in informing development of the Change Model and its supporting materials. In this article, we report on a formative evaluation of the Change Model. We highlight areas of promise, concern and risk in the way the Model is translated into practice, and we identify not only how the Change Model might develop further, but also lessons for those who seek to use it to guide and inform their change efforts.
Methods
The evaluation took place in two stages over the period 2012–2013. The first stage considered the design, development and objectives of the Change Model to generate a programme theory of change, 21 using interviews, document analysis and ‘virtual ethnography’ of webinars about the Change Model. The second stage focused on the application of the Change Model in practice, using in-depth interviews with NHS clinicians and managers who were using it. This article briefly summarises the findings of the first stage, then focuses on the practical application of the Change Model, as covered in the second stage.
Fieldwork for the first stage included all those identified by the NHS Institute as having been involved in developing the Change Model who consented to interview, analysis of 12 documents relating to the Model’s development and publicity materials on its website and observation of 8 hour-long webinars about the Change Model. Participants in the second stage were identified from three sampling frames: (i) ‘early adopter’ sites, which were essentially pilot sites for the Change Model; (ii) respondents to a survey about the Change Model administered by the NHS Institute; (iii) attendees at the webinars observed in stage one. We also snowball sampled from participants in each group. Our approach for stage two involved a combination of quota sampling (a minimum of two participants from each early adopter site) and theoretical sampling (continuing to recruit participants until theoretical saturation was reached). 22
Profile of participants in stage 2 of the evaluation (coded from information given in interviews).

Findings
We present our findings in five sections. We start with a summary of our stage one findings, covering perceptions of need for a Change Model and of its utility and advantage over other ways of approaching change. We then concentrate on findings relating to the use of the Change Model in practice, from stage two interviews. In the second section, we offer a summary of the views of participants on the Change Model and the ways they used it. Next, we note small – but significant – ways in which participants mediated the Change Model, adapting it for use in multiple contexts. In the fourth section, we discuss the challenges participants faced in applying the Model to the projects in which they were involved, relating to both the Change Model itself and the wider context. Finally, we examine how participants sought to overcome these challenges and what this meant for ‘fidelity’ to the Model. In interpreting findings, especially from stage two, it should be acknowledged that our sample is inevitably self-selecting and likely to include participants with a positive disposition towards the Change Model.
A theory of change for the Change Model
The perceived need for a novel Change Model among those who instigated and designed it was driven by two sets of concerns. One was the financial, clinical and social context facing the NHS and the strain of increasing demand in straitened times. The other was a developing view, whose origins predated these immediate pressures, that existing approaches to managing change in the NHS were limited – and in particular, that effective ‘micro-level’ approaches to change (such as improvement methodologies – Plan-Do-Study-Act cycles and the like – applied at local levels) were not being linked up through meso- and macro-level strategy. A key function of the Change Model, therefore, was to provide a means of co-ordinating change: There’s been some fantastic changes in the NHS so far which have improved care for so many people. As a national care system however we are not good at sharing those great improvements for all and shrinking finances make this even more important now. The NHS Change Model takes the best of what we know and gives us a checklist for the components of change necessary. (Report from ‘NHS Change Model: the Big Event’)
Moreover – and unlike other, generic change-management models – a key intended advantage of the Change Model that was identified was the way it accounted for the specific organisational context of a publicly funded healthcare system. The Change Model acknowledged explicitly the challenges this context posed to those instigating change, such as inter-professional conflict, target-based performance management and multiple accountabilities. Its eight components offered ways of mobilising resources to overcome these challenges, from ‘hard’ techniques such as transparent measurement and rigorous project management to ‘softer’ assets such as shared values and inclusive leadership. This implied ‘an evidence-based, systematic and skilled application of change management approaches’ (Official notes from NHS Commissioning Board workshop) that combined extrinsic and intrinsic motivators to maximise the chances of sustainable change. It’s to help the NHS make change at scale and pace, and to involve as many people as possible, but to make sure that that change is done in a rigorous way so that the change is sustained and people are engaged in the process and buy into what we’re trying to do. (S1-03)
This meant attending to the alignments between components, so that possible tensions between soft and hard aspects of the Model were addressed and kept in balance.
Besides its content, the format and presentation of the Change Model also sought to contribute to this purpose. Much effort had gone into ensuring that the Change Model was accessible to all, avoiding jargon; it needed to be simple to use without oversimplifying the challenge of change to the extent that it became used as a ‘checklist’: ‘I’ve ticked all of those boxes, I’m all right’ (S1-04). Another important concern was to secure ‘commitment to’, rather than ‘compliance with’, the spirit of the Change Model. Participants recognised the risk of the Model being seen as another ‘top-down’ initiative, and sought to address this both by emphasising the need to start from the values that drive intrinsic motivation, and by encouraging planned adaptation of the Change Model to local circumstance: Target-driven cultures have made people think about the deficit that they have yet to sort out. […] The Change Model doesn’t start from that position, it starts from what’s our shared purpose, what’s the outcome we’re looking to deliver, what has worked very well before, and let’s try and look at that and say, ‘How did that work?’ and start with that. (S1-05)
This different starting point, and the potential for ownership and adaptation, were seen as critical to the Change Model’s value.
The Change Model in practice: 1. Reception
As might be expected from a self-selecting cohort, the overall response to the Change Model from its early users in stage two was overwhelmingly positive. All participants, when asked, stated that they would recommend the Change Model to colleagues; all said that they had found either the whole Model or certain of its components helpful in structuring their change efforts. Several features were identified as particular assets, and as areas where the Change Model showed clear advantage over other models, approaches and frameworks.
One asset was its face validity: participants, largely experienced change agents in the NHS, found the Model intuitively sensible and comprehensive, and clearly tailored to the multiprofessional, complex context of healthcare. A second was its practical orientation: it focused on the concrete tasks required for change, and the importance of co-ordination and alignment among them, rather than offering abstract theory: It’s based in things that we’ve learned and it’s based in a ‘people reality’, rather than ‘methodology reality’. […] We’re here, we need to get there. These are the stages we’ll go through; these are the workshops we’re going to have; these are the actions we’re going to take. (S2-08/middle manager/non-clinical background)
The articulation of different aspects of change, and its links to specific tools (Table 1), meant that the Change Model was seen as something that offered clear guidance on what to consider, and pointers on what to do. Rather than simply outlining areas for consideration, it offered clear direction on the need for action.
A third, related, advantage was the Change Model’s foundation in existing evidence. Several participants said that they saw nothing particularly new in the Change Model, but added that this lack of novelty was a merit, not a flaw: I don’t think the Change Model is rocket science or something brand new, but what it does do is bring together the components of how you make change into a very simple structure, even just the visual structure. It makes you think about the component parts of it. It is not enough just to have a shared vision. You also have to have the leadership and the engagement to mobilise and the system drivers or you at least have to question yourself about whether they are there. (S2-28/senior manager/nursing background)
This basis of the Change Model in what had gone before made it more acceptable to sceptical or change-fatigued managers and clinicians than something that looked unnecessarily novel or faddish, although – as might be anticipated – participants were not all convinced of the robustness of the underlying evidence base.
These assets together meant that participants saw in the Change Model a framework particularly well suited to undertaking complicated and ambitious programmes of change that would implicate multiple stakeholder groups, cross organisational boundaries, involve decisions about resource reallocation and create winners and losers. The way the Change Model encouraged a broad-based approach to change management, and directed attention to the ‘harder’ and ‘softer’ aspects of change and the tensions between them, meant that participants saw ripe potential in the Model as a means of structuring the work of change.
Typically the change projects in which participants were engaged were ambitious and multifaceted, and often required cost savings without the loss of quality. They found the Change Model to offer an especially useful sensitising framework in planning and executing such projects: This is a multi-partnership project, so not just involving NHS ways of working: it involves a range of different providers and commissioners. But we all recognise that the tools [and] methodology within the Change Model resonated across different sectors, even though it was about the NHS. Quite often we go straight to delivery rather than actually thinking about leadership, vision, what sort of methodology we want to use, how we are going to measure it, and we don’t necessarily develop a project thinking about all the aspects that will make it work. We move quite often straight into implementation and then when we falter we don’t recognise that it’s because some of the things may not be in place. (S2-14/clinical manager/medical background)
Though most participants were at the early stages of projects, many reported that they had already found that using the Change Model enabled them to take a more considered and comprehensive approach to planning their work.
The Change Model in practice: 2. Mediation
Participants tended to find that the greatest value of the Change Model lay in informing and guiding background thinking and structuring of activity, rather than taking the foreground as an explicit model of change held in common by all concerned parties. They described using the Model to identify the dimensions of change they needed to address, and to form ideas about how to address them, and they then sought to assign particular tasks to other individuals in appropriate roles and positions. They would perhaps point these individuals in the direction of resources that could be of assistance, but rarely sought explicitly to invoke the Change Model itself: What people use it for more is a reminder, so say I’m one of the programme managers, they’re thinking, ‘Well I’m working on the urology project, these are the elements, have I considered all these elements at the outset?’ […] Whether it’s a project manager or a programme manager, they’re really key in helping clinicians to think through some of these elements, without saying, ‘And here’s a framework you must follow’, because that would turn them off. (S2-21/senior manager/non-clinical background)
Participants gave several reasons for taking this approach. The first was linked to how they managed change, which characteristically involved retaining management and responsibility for designing and implementing changes, but engaging in dialogue with others while doing so. They were concerned that, notwithstanding the efforts to make it accessible described in stage one, the language and tools of the Change Model risked alienating some stakeholder groups, especially clinicians. They therefore actively mediated the Model, seeking to ‘translate’ its domains into language that they saw as being more ‘clinician-friendly’, and they avoided presenting the Model in its entirely.
Second, participants often saw effective application of the Change Model as resting on mobilising the specialist skills of different groups of colleagues. In engaging with those with expertise in measurement, for example, participants did not feel the need to refer to the entire Change Model; instead, participants engaged with them on the specifics of the measurement challenge, having used the Model to frame their own thinking beforehand about how measurement linked to the other components: We've been dealing with the Change Model in two parts. In terms of our internal commissioning team it’s been quite useful just to help people understand what they need to consider and how are tools that we started to develop actually fit within the model has been useful. […] We haven’t been using it in the workshops or the clinicians, because what we thought that it may turn them off. (S2-19/middle manager/non-clinical background)
Third, and connectedly, this approach reflected an understanding among participants of the Change Model less as a ‘model’ per se – a process-based methodology with clear instructions that needed to be followed exactingly – and more as a framework to sensitise and inform. Several participants explicitly stated that they saw the Model not as a model at all, but as a framework or guide. This was mirrored in the way that many described their use of the Model in practice: as a heuristic set of reminders, prompts and checks that could ensure that they were undertaking change in a way that was as likely as possible to achieve the desired ends.
In some ways this might be seen as encouraging evidence of reflective use of the Change Model by participants, who recognised the risk that ‘people make the Model more important than the work they are trying to do’ (S2-13/senior manager/non-clinical background). To this extent, it was a realisation of the frontline ownership of the Change Model desired by participants in stage one. The risk that the Change Model might be conceived of as a solution in itself, whose effectiveness lay simply in its application – rather than as a set of considerations, tools and ideas that could assist change leaders – was explicitly recognised. However, such individualised use of the Change Model also meant that knowledge of the approach remained highly concentrated, and thus easily lost as individuals changed roles and organisations. It placed a heavy burden on the skills and efforts of the small teams applying the Change Model.
Further, use of the Model as a heuristic, with components pulled out and used with different groups selectively, could result in an application that was not quite faithful to its design, especially if undertaken by an individual rather than a multidisciplinary team. As noted earlier, a key principle of the Change Model was use of all components together, attending to their alignment and polarities. As we discuss next, however, there was variability in the extent to which this principle was put into practice.
The Change Model in practice: 3. Application
In drawing heuristically on the Change Model to guide change efforts, participants differed in the extent to which they addressed its eight components in a balanced way. Participants recognised the value of the comprehensive approach to change that the Model embodied, and they also saw the importance of ensuring alignment rather than tension between components of change. But in practice they sometimes struggled to achieve either of these goals. I am struggling slightly with it. It all makes absolute sense and I think the concept of the different areas that all need to be addressed as part of a change is absolutely bang on. […] We have an awareness that we need to concentrate on all of them, but I imagine that at the moment we are probably concentrating more on leadership for change and engagement to mobilise and I think some of them come at different stages in delivering change. (S2-02/middle manager/non-clinical background)
Participants often described using the Change Model to help identify particular areas of concern, but they did not necessarily embrace all its components. Some components were simply seen as more important, immediate and pressing than others, given the nature of the problem and the stage at which they found themselves in addressing it. In particular, participants found that whereas the ‘softer’ aspects of the Model – such as ‘Engagement to mobilise’ and ‘Leadership for change’ – focused on developing consensus and motivation among diverse stakeholder groups, some of the Model’s ‘harder’ aspects – such as ‘Transparent measurement’ and ‘Rigorous delivery’ – could throw into sharp relief the differences of opinion, interest and motivation among these groups: The one bit that worries me slightly is where it says ‘Transparent measurement’. Because anything that talks about measurement is going to get complicated and it’s going to get difficult and is going to get contentious because we have lots and lots of change models but we have also got lots and lots of different measurements as well within the NHS. So I think anything along those lines is going to be difficult. (S2-11/management consultant/non-clinical background)
Consequently, some participants reported that they had tended to avoid the aspects of the Change Model that they found more challenging.
More fundamentally, the ‘System drivers’ component of the Model vexed many participants. While some had undertaken a great deal of work to align change efforts with the priorities, strategic objectives and incentives of the wider NHS system, others struggled to make such connections. National priorities were seen as too fixed to be readily aligned with some of the change efforts being undertaken, while local levers were not always easily accessible, or sufficiently powerful to orient organisations and individuals towards the change desired: There are people trying to grow those levers but the system drivers aren’t there. The ones that are I have no control over, so I guess for something like that it is difficult to use if there isn’t a context to work within. (S2-12/clinical manager/medical background)
More broadly, the organisational environment of the NHS was seen by many participants as inimical to effective use of the Change Model. They described a hierarchical culture that favoured expediency over engagement in change efforts and a financial context that exacerbated this counterproductive proclivity for haste. While the major challenges facing the NHS meant that the Change Model was needed now more than ever, the urgency of resolving these challenges – and the ingrained way of dealing with change within the NHS – meant that now was probably the hardest time to put it into practice, too: ‘Often there’s a lot of pressure to get work done immediately or quickly, and sometimes that's in direct conflict with doing things the right way.’ (S2-09/middle manager/therapy background)
A particular challenge that resulted from such a context was keeping the extrinsic and intrinsic components in balance. As one participant vividly described, when extrinsic motivators – especially around cost containment, incentivisation and targets – weighed so heavily on colleagues’ minds, finding a space for mobilising for change through intrinsic motivators could prove difficult: The tension comes when we look at the systems drivers, when we look at the contracts that we’re involved in. So things like: ‘We’ll serve notice on the contract’. Or: ‘If you don’t up your game, you’ll be in the private sector and [private healthcare company] will take over’. And I’ve had to protect the engagement bit [of the Change Model] from that. […] So the last thing I want is them to be thinking they’ve got this big axe hanging over them. […] I wouldn’t want the system drivers to be involved in the engagement process, I’ve kept that away from it. (S2-20/clinical manager/medical background)
The Change Model in practice: 4. Transformation?
Given such wider pressures, some participants reported strains in remaining true to the spirit of the Change Model, particularly in relation to keeping extrinsic and intrinsic motivations in kilter, while balancing commitment and compliance. Of course, these challenges were less the product of the Change Model than of the environment to be changed. Participants highlighted the need for organisational environments that shielded change agents from these pressures and gave balanced approaches based on the Model the chance to flourish: It’s actually buy-in from the leadership. It’s all very well individuals within an organisation understanding it, but it has to become a cultural—you talk about intrinsic change as well, intrinsically the organisations need to buy into this way of working, otherwise it actually won’t have the benefits, the full benefits that people are trying to deliver. So it’s all very well middle managers or lower managers using it, but then if the chair and chief exec, directors et cetera don’t get it, then it probably won’t really deliver. (S2-17/middle manager/non-clinical background)
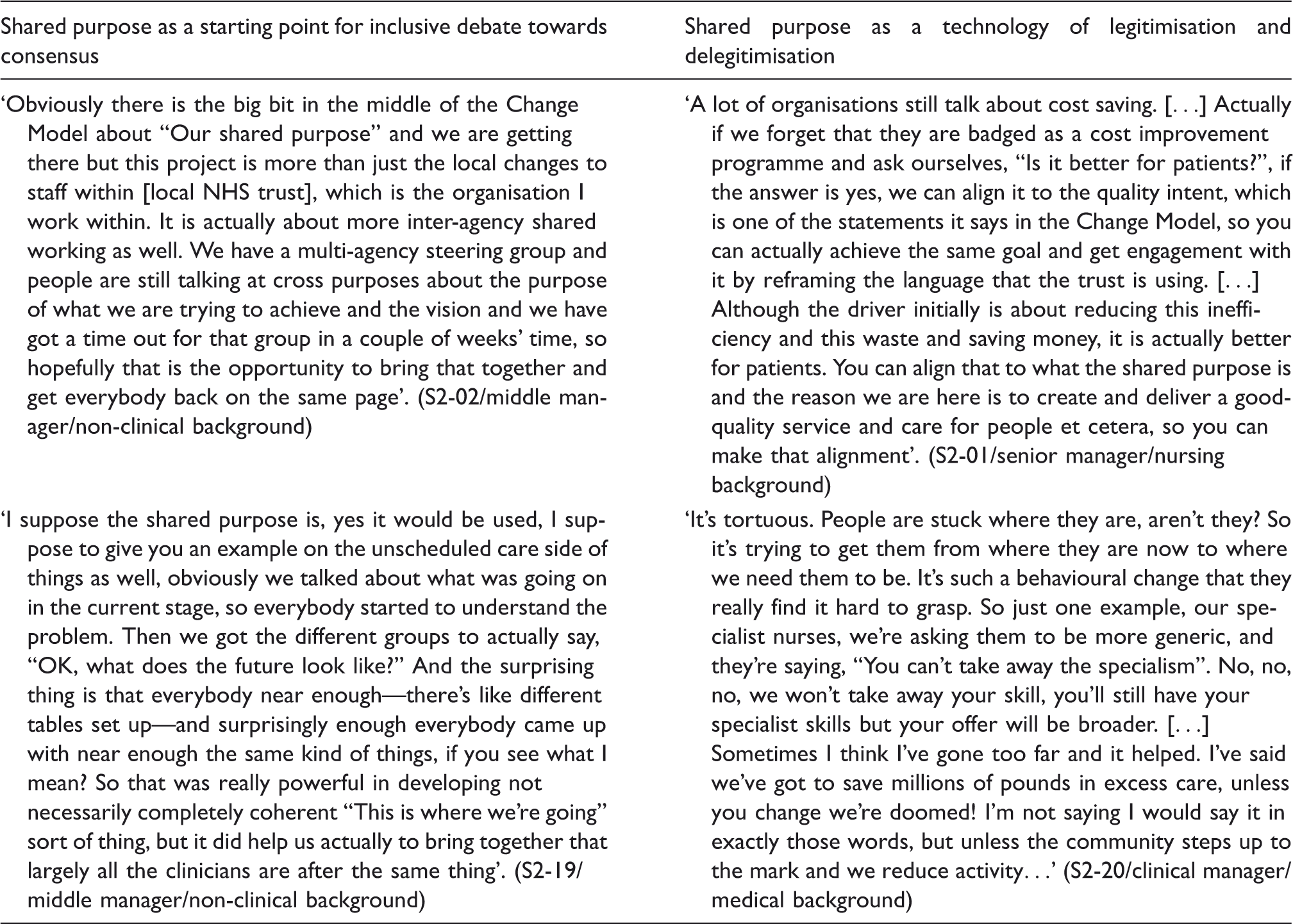
The facilitating actions of senior managers beyond ‘change teams’ were thus crucial to the Change Model’s prospects, but participants also pointed towards the potential of the tools the Model itself included in starting to deal with the challenging context. In particular, they highlighted how the notion of ‘Shared purpose’ at the centre of the Model could offer a potent resource in seeking to resolve differences of group interests, mitigate the burden of extrinsic pressures and ensure change remained true to the principles of the NHS. Where senior managers saw challenges in terms of financial pressures and frontline clinicians saw them in terms of risks to jobs, ‘Shared purpose’ could – as anticipated by the Model’s designers in stage one – offer common ground on which less polarised, less fractious conversations could take place. Discussions could be reframed instead in terms of how to deliver the best possible service to patients: We have had quite a few different people inputting into us and at one point that was getting traumatic because different people were asking us to do different things. And that has stopped now, or virtually. […] Different agendas, so different people from different areas of work. So for example, my original line managers and their general managers have obviously got an interest in the project and wanted the project to take us in one direction and get certain information and then my project manager would be saying, ‘No, I don’t want you to do that, I want you to go and get that’, and then the chaos of that made it quite difficult to keep on track. I think it has come back on track since we have the new project manager and we all talk about what our shared purpose is and what our ultimate goal is, which is the same sort of thing as a shared purpose, and we regularly talk about that. It is always talked about whenever we communicate. (S2-15/clinical practitioner/therapy background)
To this extent, users saw great potential in the ethos of ‘Shared purpose’ to make conversations that had previously been frustrated by polarised opinions more possible: a ‘platform for developing common understanding’ (S2-06/middle manager/non-clinical background). Agreeing on ‘Shared purpose’ could bring stakeholders to the table to develop solutions that did the best job possible of generating solutions that were faithful to the underlying mission of the NHS.
What was also apparent, however, was that this was not always the way in which the task of achieving ‘Shared purpose’ was undertaken. Given the scale of some of the problems faced, and the need for haste in finding solutions, ‘Shared purpose’ was often invoked more to overcome the opposition to change of groups seen as recalcitrant than to provide a shared basis for dialogue. Thus, in practice, it could be a discourse that was used to reframe stakeholder resistance, rather than to reframe the challenge faced as a common one: There’s going to be some resistance to this change and pushing harder for the change isn't going to work. We need to take some of the resistance away. So within any of the areas that we’re working in, identify where some of your resistance lies, and let’s work to try and reduce that resistance and that’s how we’re going to bring successful change. And I think that’s how I use it. (S2-03/senior manager/non-clinical background)
Examples of two contrasting approaches to ‘Shared purpose’.
This is not to suggest that these approaches necessarily represent the ‘right’ and ‘wrong’ ways of using ‘Shared purpose’, or that one is faithful to the Change Model while the other corrupts it. The resistance of some groups to change may sometimes be founded more in vested interest than in sincere commitment to quality of patient care, and ‘Shared purpose’ may constitute a useful way of challenging such resistance. However, it is perhaps useful to distinguish this from an approach in which the need for change is dealt with more democratically. It also indicates how strong an influencing factor the pressures of finance and demand represent: in such an environment – where ‘unless you change, we’re doomed’ (S2-20) – one way of using the Change Model seemed more viable than the other.
Moreover, there were signs in our study that in this environment, the Change Model itself risked becoming managerialised. One participant recounted how, in a recent reorganisation, staff had been required to reapply for their jobs – and told that, because the organisation was planning to adopt the Change Model as an operating principle, they would be asked in the shortlisting and interview process to describe how they would use it. Such stories provide another reminder of how overbearing an influence the current financial and organisational environment of the NHS could be, not just on whether the Change Model was used, but also on how it was used in practice.
Discussion and conclusion
Implications for healthcare managers.
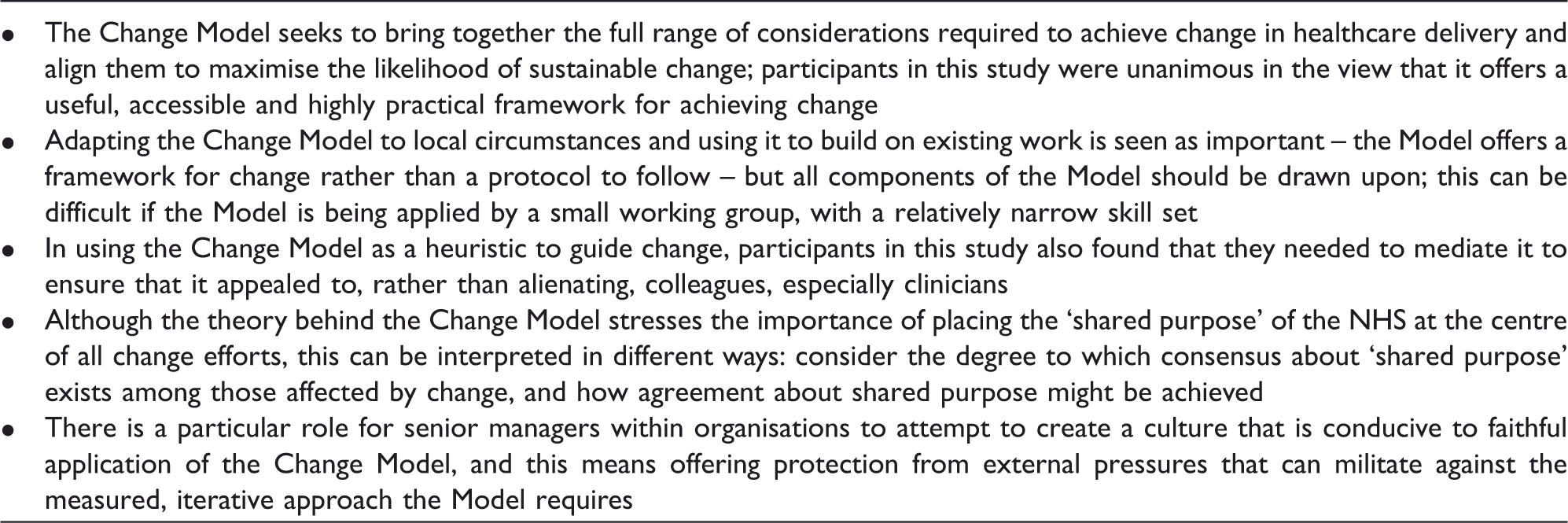
The Model was being used by some to sensitise, to broaden thinking, to inform, rather than as a recipe to follow slavishly. However, participants also tended to use the Change Model in a relatively individualised manner, keeping it to themselves or working with it in small groups rather than explicitly drawing on it as they engaged the breadth of parties with a stake in change. In some cases, this strategy was accompanied by use of the Change Model in practice that was rather more selective than intended in its design, with participants apparently more comfortable with the ‘softer’ than the ‘harder’ components of the Change Model, bringing in other stakeholders with different expertise selectively and intermittently. Although pragmatic adaptation of the Change Model by its users is, as noted earlier, part of its theory of change, crucial also is fidelity to certain essentials, including using all its components. The recognition implicit in the Change Model of the impossibility of protocolising and micro-managing change – its notion of management as being about ‘shaping capabilities’ rather than ‘control’ 4 – resulted in variable levels of both fidelity and creativity in application. One response from the Change Model’s architects might be a greater emphasis on what can and cannot be adapted, and further guidance on how to embrace the more difficult components, though this could risk sacrificing the parsimony of the Model, and generating more of a ‘recipe book’ or ‘checklist’. Ultimately such tensions may be inevitable: it is difficult to envisage a change-management model that achieves the perfect balance between detail and simplicity, 2 and certainly a model that sought to prescribe actions and proscribe judgement would be counterproductive. 7
Participants also frequently reported that some components proved very difficult to operationalise, notably ‘System drivers’. Here, the challenge seems to lie not such much in the Change Model itself as in the wider NHS system. Participants noted how the work of senior managers in organisations could do a great deal to legitimise use of the Change Model, and to foster an organisational environment in which the thorough, patient approach advocated by the Model could be protected from short-termism and haste. 24 However, organisational interest in the Change Model also risked corrupting it, turning it into a managerialist tool, 25 and prioritising compliance over commitment despite the eagerness of its designers to avoid this. There are limits, then, to the advantages conferred by the Model’s contextual sensitivity (exactly the quality claimed to be lacking in generic change-management models generated in private sector environments): the Change Model is still vulnerable to wider constraints. No framework for change, no matter how contextually sensitive, is a match for such powerful institutional forces.4,26 The adoption of the Model by NHS England as its chosen approach to achieving change offers opportunity here, but risk as well. Much will rest on what this adoption means in practice: will it create an environment in which senior managers feel legitimised in providing space for a sincere application of the Change Model approach, or will it merely act as a fig leaf for management based on diktat, target and contract?
We also found important tensions within the Change Model, most notably linked to how the ‘Shared purpose’ at the centre of the Model is conceptualised and mobilised. For some, it was a powerful means of finding common ground in previously polarised debates and initiating dialogue around challenging and contentious issues that had previously been characterised by entrenched positions aligned to particular interests. Others, however, appeared to use ‘Shared purpose’ more strategically, as a means of delegitimising opposition to change. As we noted earlier, the latter approach is not necessarily a corruption of the ethos of the Change Model – indeed it may be necessary to confront vested interests in this way 27 – but it does imply rather a different realisation. A risk of this approach is that the Change Model becomes an instrumental tool or manipulative device for imposition of change, 28 resulting in both less sustainable change and undoing its claim to providing an alternative approach.
Despite these challenges, our analysis suggests that there is much of value in the Change Model, even if its potential is contingent on the context in which it is used. If its use can be encouraged by NHS England and other bodies in a way that enables proper engagement rather than superficial compliance, it will offer at the least a useful heuristic for those leading improvement, and potentially a framework that offers a way through some of the most vexing challenges involved in changing complex healthcare systems.
Footnotes
Acknowledgements
We are grateful to the participants in the study for their time and candour. We are also grateful to an anonymous referee and the journal’s editor for very helpful constructive criticism. Funding for this study was provided by the NHS Institute for Innovation and Improvement.