
Abstract
Hospital average length of stay varies considerably between countries. However, there is limited patient-level research identifying or discounting possible reasons for these differences. This study compares the length of stay of patients in Japan, where it is the longest in the OECD, and Canada, where length of stay is closer to the OECD mean. Administrative patient-level data, including age, gender, co-morbidities, intervention, discharge plan, outcome and length of stay were collected from two Japanese and two Ontario, Canada hospitals for two diagnoses: colorectal cancer surgery and acute myocardial infarction. Analyses examined linkages between patient characteristics, hospitals and countries and length of stay. When controlling for patient demographic characteristics, the incidence of co-morbidities and discharge plan practices, Japanese length of stay tended to be significantly longer than that in Canada for both diagnoses. Mortality rates were not significantly different; however, the readmission rate (28 days or less) for acute myocardial infarction was higher in the Canadian hospitals. The findings indicate that non-clinical factors contribute to sustained international differences in length of stay. These factors may include professional or cultural norms, differing payment schemes and access to long-term care facilities. The study also introduces a protocol that can be used for international patient-level comparisons that can enable effective policy and management learning.
Keywords
Introduction
Hospital average length of stay (ALOS) is an important benchmark used to assess healthcare systems, as shorter stays are associated with hospital and system efficiency. 1 National ALOS figures collected by the Organisation for Economic Co-operation and Development (OECD) usefully start the process of international comparison. The most recent numbers for the 28 (of 34) OECD members who report acute (curative) hospital ALOS show a broad range, from 3.8 days in Turkey to 17.9 in Japan, and an average of 6.5 days. France (5.1 days) and the United States (5.4) are below the average, Canada (7.7) and Germany (7.9) are above and the United Kingdom is at the mean (6.5). 2
These differences give rise to an obvious question: Why does ALOS vary between countries? Extant comparative data, such as the OECD health statistics set 2 and large World Health Organization Global Health Observatory database 3 offer candidate explanatory variables such as the supply of beds and demography. These add interesting context; however, the level of aggregation does not enable analyses of links between length of stay (LOS) and patient-level variables such as age and the presence of co-morbidities.
There is a limited stream of international research comparing health services at the patient level. An early example studying patients at a Japanese and an American teaching hospital found that the Japanese LOS was much longer, and the US costs per patient higher; however, the longer Japanese LOS tended to reduce the total cost per patient gap. 4 Another contribution, that examined differences in outcomes for patients hospitalized for six diagnoses in three European countries and three American states, revealed significant variation in readmission rates. 5 Recent research comparing LOS and mortality after surgery of elderly hip fracture patients in three Japanese and two American hospitals found that while the US LOS was much shorter, mortality was significantly higher in that country. 6
This study builds on work cited earlier by comparing LOS in Japan and Canada at the patient level in order to identify or discount reasons for LOS differences. Japanese ALOS remains long, despite steps taken by the Ministry of Health Labor and Welfare to reduce it over the past 15 years. A key initiative was to reclassify some hospitals as long term or alternative level of care (ALC) facilities when data indicated that most of their beds were not being used for acute care. A second step was to introduce a form of prospective payment in hospitals. In response, Japanese ALOS has declined from 33.2 days in 1995 to 24.8 in 2000 and to the current level of 17.9 days. 2
Canada is used as the comparator because it is also a developed country with a mostly public healthcare system and has an ALOS that is close to the OECD average. The research is framed primarily by the more specific question: What factors are associated with LOS in Japan and Canada?
Methods
This study compared the lengths of stay for patients admitted for either colorectal cancer surgery or acute myocardial infarction (AMI), in four hospitals, two each in Japan and Ontario, Canada. Regional and individual hospital statistics were gathered to supply context. The Ryerson University Research Ethics Board and the participant hospitals’ respective ethics committees approved this research.
The Japanese hospitals are in two mid-sized communities. JHosp-1 is private and JHosp-2 is publicly owned. Both host medical residents, though they are not part of universities. CHosp-1 is a community teaching hospital in a large Ontario urban centre, and CHosp-2 is a large teaching hospital in a mid-sized city. The hospital-level data collected were size (bed number), LOS for all patients and the numbers of physicians and nurses. Public sources were consulted to gather numbers of acute care and long-term care beds in the hospitals’ broad service districts.
Colorectal cancer and AMI were chosen because both are reliably identifiable and significant afflictions in both countries. Cancer accounted for 32% of all deaths in Japan and 30% of those in Canada in 2004. Colorectal cancer comprised 12% of these in Japan and 11% in Canada. Ischaemic heart disease, which includes AMI, accounted for about 7% of Japanese and 17% of Canadian deaths in 2004. 7
Main analyses were performed using administrative data extracted for individual patients, aged 18 or more, using a protocol developed by three of the sites, and approved by the research ethics authorities of all four. The hospitals employ the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) scheme. 8 The colorectal sample was for ICD codes C18-C21, D010.0-D010.3 and D37.4, and who had undergone an intervention, partial or total excision. For AMI, the code was I21; subsequent AMI (I22) or old AMI (I25.2) patients were excluded.
Data were for 1 year, April 2007 to the end of March 2008 for three hospitals. JHosp-2 data are from 2008 to 2009, because it had introduced a new information system the previous year and wanted to ensure a reliable 1-year sample. There were no policy or technical changes in Japan between the two periods expected to affect hospital behaviour so the JHosp-2 information was pooled with the others.
The dependent variable, LOS, was calculated using dates of admission and discharge information, commencing with the date of admission. Therefore, a patient admitted one day and discharged the next would have a 2-day LOS. For both diagnoses the control data extracted were gender, age and incidence of diabetes (E10.0–E14.9).9–11 The colorectal patient cases also included a field indicating whether a secondary neoplasm was present. For AMI there were fields indicating whether patients had congestive heart failure (CHF, I50.0) or hypertension (I10–I15), and whether either cardiac catheterization or coronary artery bypass graft (CABG) procedure was performed.11,12
Discharge disposition and readmission information were also extracted. The destination of those discharged, particularly whether they went from the hospital to a long-term care facility, or their home.12,13 The outcome data used were whether the patients died or underwent an unplanned readmission 28 days or sooner after discharge. 12
Analysis
Chi-squared analyses were conducted to make between-hospital comparisons of patient sample categorical characteristics, outcomes, death and unplanned readmission within 28 days of discharge. Analysis of variance (ANOVA) was performed to compare LOS between the hospitals. Analyses of the patient, hospital and national factors associated with LOS were conducted using log-gamma generalized linear models (GLM) because the distribution of the dependent variable, LOS, was positively skewed.14,15 The influence of patient treatment course was assessed by testing for a link between LOS and whether the cancer patients were subject to a planned readmission. The association between discharge to a long-term care (LTC) facility and LOS was also tested by including this variable. The co-variates were employed as outlined in the previous section. To confirm the consistency of linkages between demographic and clinical factors and LOS, three models were run for each ailment, one each for the Japanese and Canadian samples, and one using the full data sets.
Results
Hospital characteristics and LOS
Profile of Japanese (J-Hosp) and Canadian (C-Hosp) hospitals and local hospital bed supply.
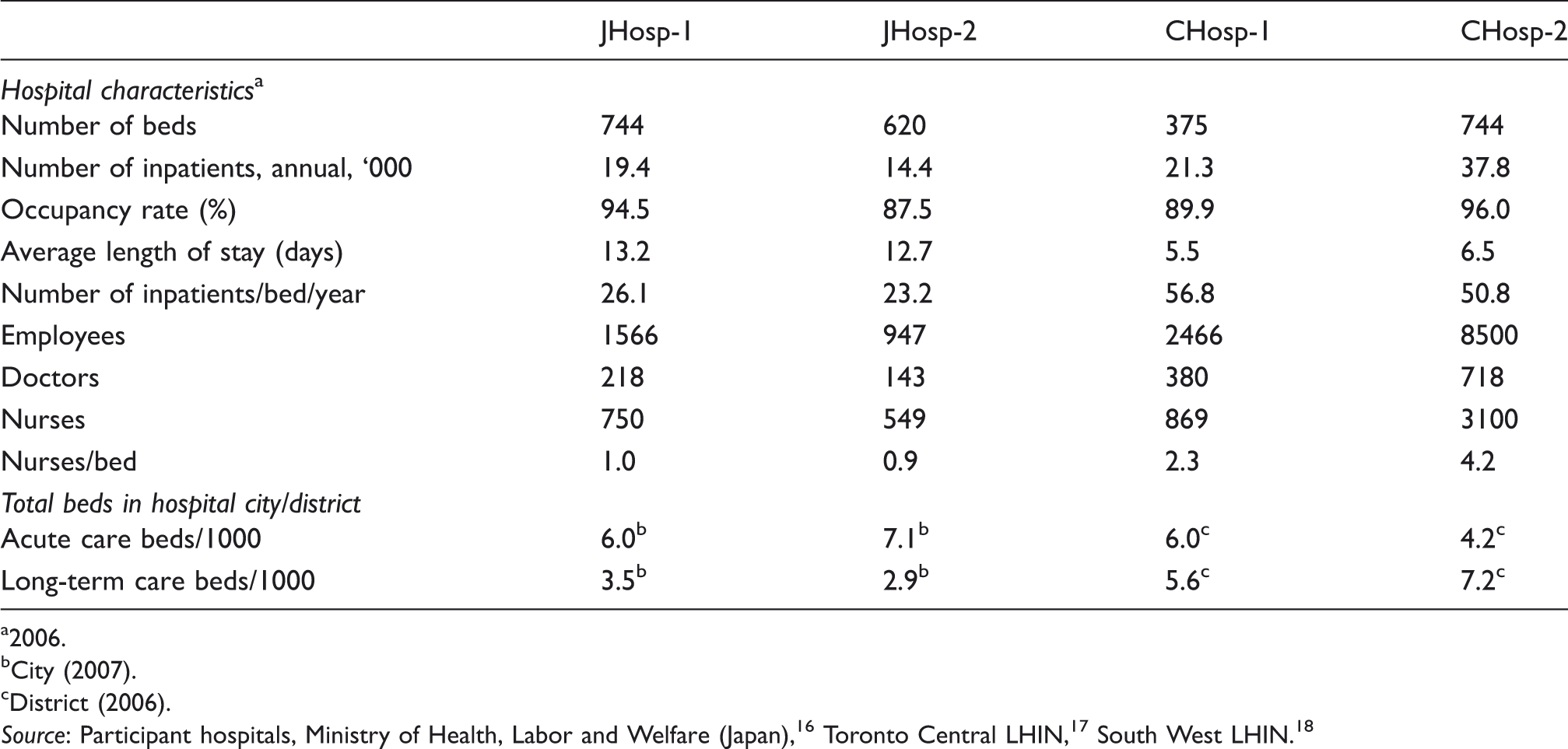
2006.
City (2007).
District (2006).
Colorectal cancer patients
Patient sample characteristics.
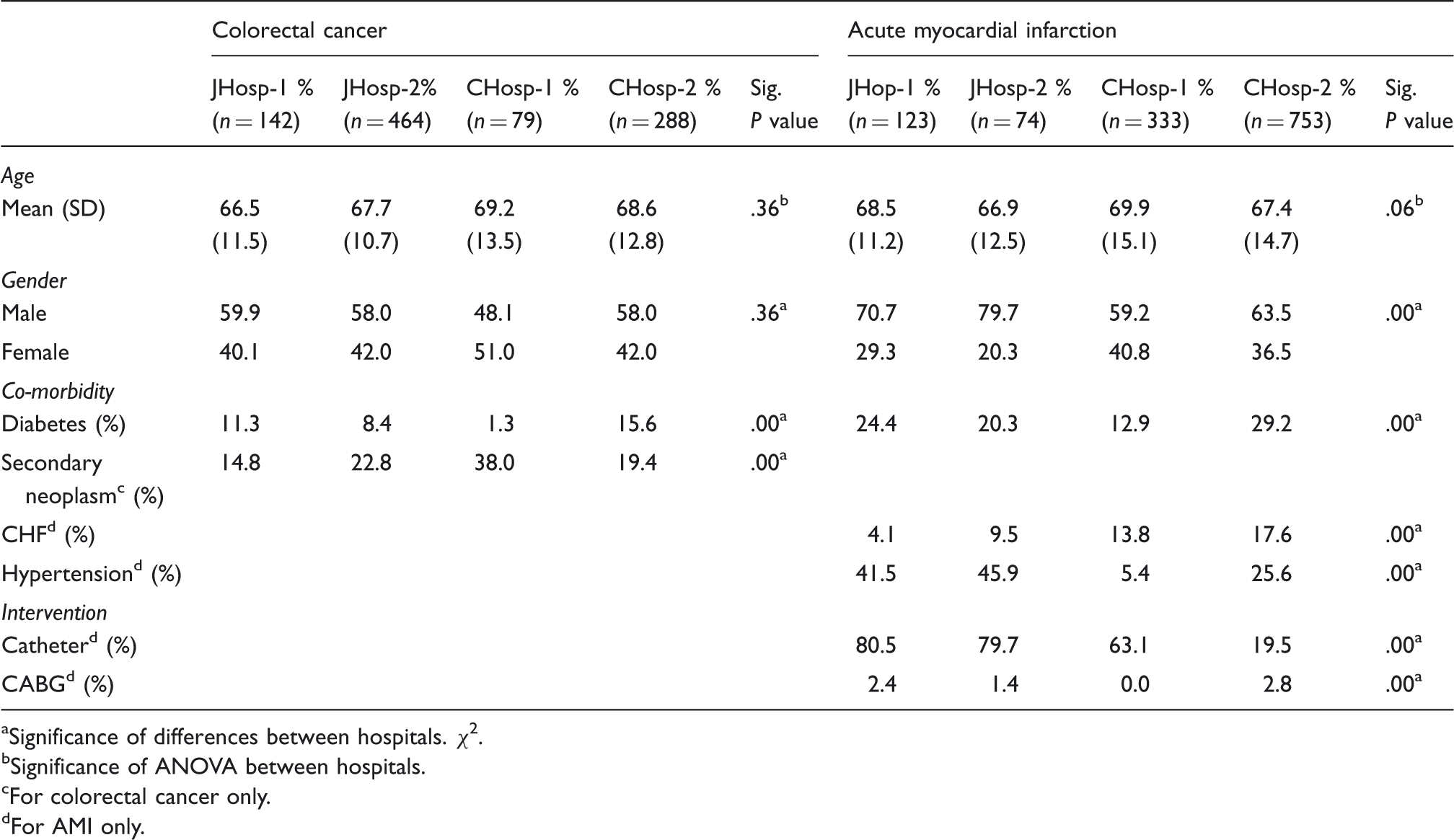
Significance of differences between hospitals. χ2.
Significance of ANOVA between hospitals.
For colorectal cancer only.
For AMI only.
Length of stay, discharge destinations and outcomes.
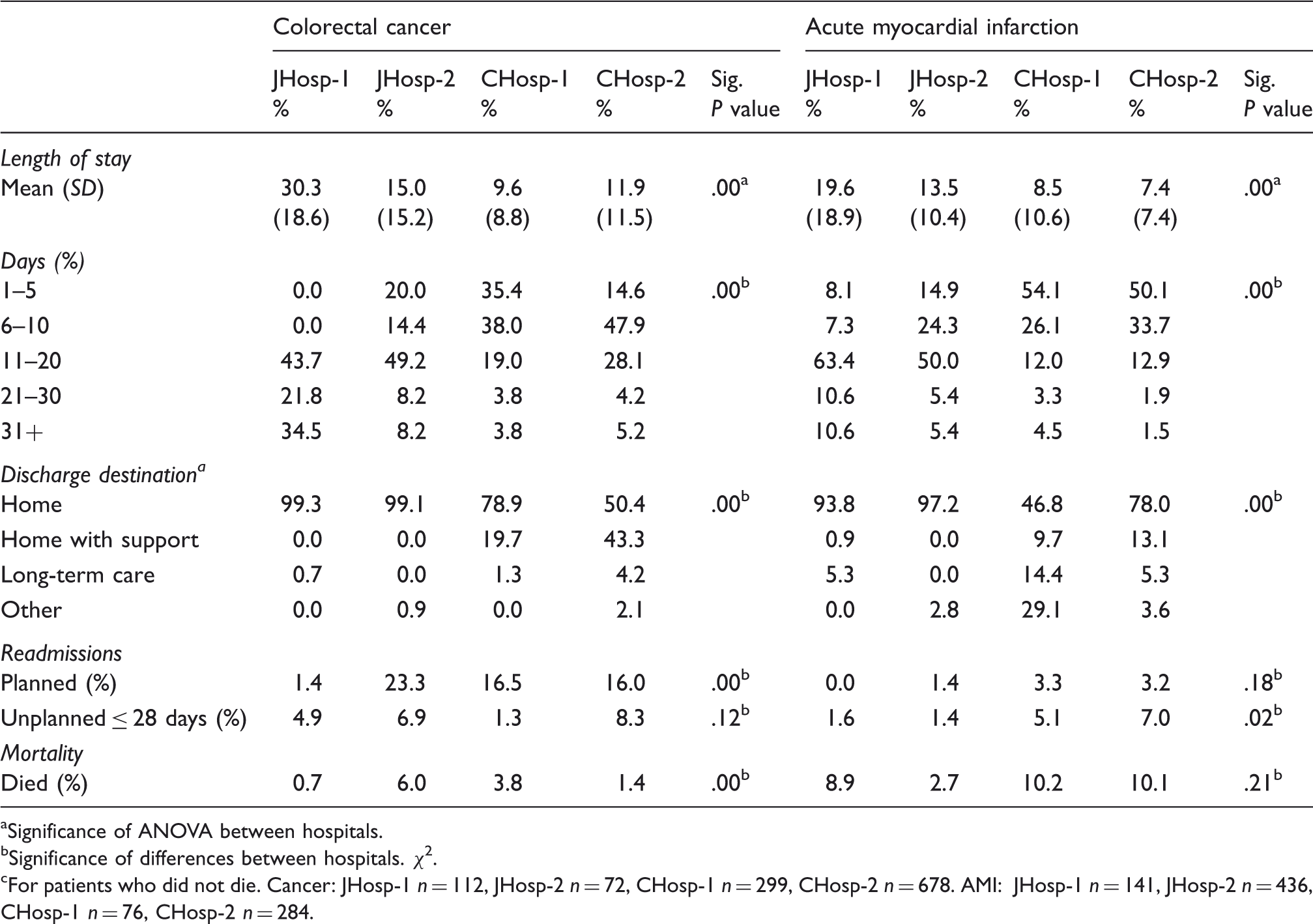
aSignificance of ANOVA between hospitals. bSignificance of differences between hospitals. χ2. cFor patients who did not die. Cancer: JHosp-1 n = 112, JHosp-2 n = 72, CHosp-1 n = 299, CHosp-2 n = 678. AMI: JHosp-1 n = 141, JHosp-2 n = 436, CHosp-1 n = 76, CHosp-2 n = 284.
Nearly all, 99%, of the Japanese hospital patients were discharged to their homes, compared to about 80% of one Ontario hospital and only about half of those from the other. Very few of the Japanese patients went to a LTC facility, while 4% of CHosp-2 patients did. In the Ontario hospitals, 20% and more than 40%, respectively, were discharged home with formal help, or to a non-LTC facility that supplied some patient support.
There was a significant difference in discharging and planned readmission of patients through the treatment course. While one Japanese hospital, JHosp-1, did this rarely, 16% or more of the other three hospitals did. Mortality rates ranged from less than 1% in JHosp-1 to 6% in JHosp-2, bracketing the Canadian hospital numbers. The unplanned readmissions within 28 days of discharge did not vary significantly between the hospitals. Taken together it would seem that the hospital country did not influence these two outcome measures.
Generalized linear model analyses of length of stay.
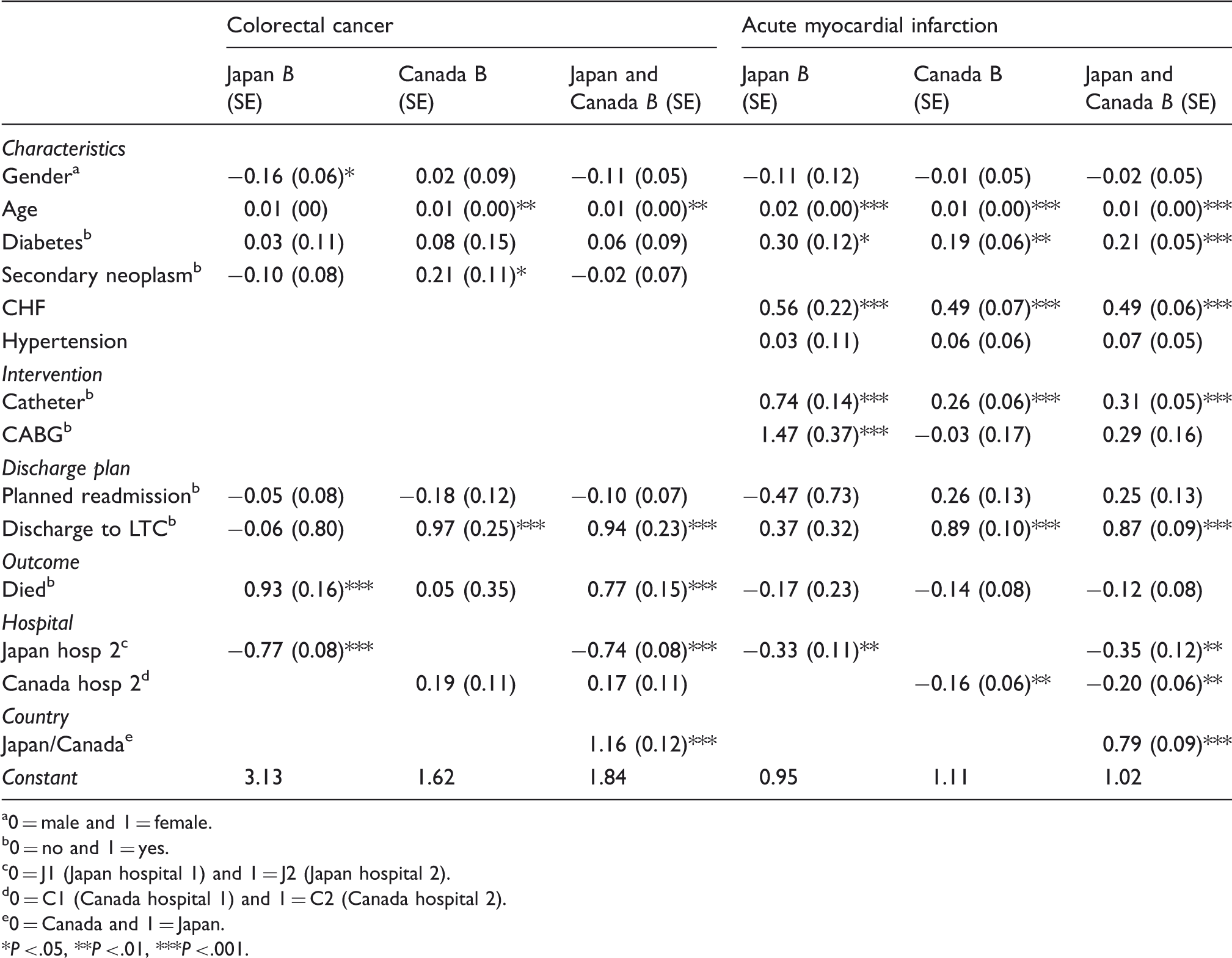
0 = male and 1 = female.
0 = no and 1 = yes.
0 = J1 (Japan hospital 1) and 1 = J2 (Japan hospital 2).
0 = C1 (Canada hospital 1) and 1 = C2 (Canada hospital 2).
0 = Canada and 1 = Japan.
*P < .05, **P < .01, ***P < .001.
The patient characteristic variables were not consistently linked to LOS in the three regressions. There was a positive link between age and LOS in the Canadian and full samples, but not the Japanese one. It is notable that patients who died in the Japanese hospitals tended to have significantly longer stays, and this effect held in the full regression. It was expected that treatment courses characterized by planned readmissions would be shorter; however, this was not borne out by the analyses. For the Canadian and full sample sets, discharge to a LTC facility was associated with longer stays.
AMI patients
Table 2 shows that of the full sample, 1283, the Canadian hospitals treated many more AMI patients. More than 70% of the Japanese AMI patients were males, significantly higher than the Canadian ratios. Average patient ages did not differ significantly between the hospitals. In both Japanese hospitals more than 40% of patients had hypertension, much higher than the Canadian ratios. However in the Japanese hospitals less than 10% had CHF, compared with 14% and nearly 18% in the Ontario sites. Diabetes incidence varied between the hospitals, but these differences were not linked to country.
The AMI patients in Japan were significantly more likely to have interventions than those in the Canadian hospitals, as presented in Table 2. About 80% of the Japanese patients were given stent or catheters, compared to 63% in CHosp-1 and 20% in CHosp-2. Coronary artery bypass surgery rates were low, less than 3% of patients.
ALOS was significantly different, about 9 and 7 days in the Canadian hospitals and 14 and 20 in the Japanese ones, respectively (Table 3). More than half of the Canadian patients were discharged in 5 days or less, compared to 8 and 15% of the Japanese hospitals. There were differences in where discharge patients went after their stays. Nearly all, more than 90%, of the Japanese AMI patients went home, compared to 78% in CHosp-2 and less than half of those from CHosp-1, where many were transferred to other acute units or hospitals. The ratio of patients that went to LTC ranged from none for one Japanese hospital to 14% in a Canadian site. There was not a significant difference in patient mortality between the hospitals. However, the unplanned readmission rates in the Japanese hospitals, less than 2%, were significantly lower than the Canadian patients.
The GLM showed consistent links in the Japanese, Canadian and full samples on factors significantly associated with LOS (Table 4). Particularly, the incidence of patient diabetes, CHF and intervention were consistently positively linked to LOS. The Japanese hospitals were associated with stays twice as long as those of the Canadian patients. JHosp-2 and CHosp-2 both had significantly shorter stays than the other hospital in their respective countries.
Discussion
The analyses confirmed that Japanese LOS was significantly longer than in the Canadian hospitals, both absolutely and when controlling for clinical factors. Further, differences in LOS between the hospitals within the two countries were apparent. Having largely discounted the influences of other factors, it is necessary to consider the significant effect of the country, Japan or Canada, on LOS. This is in effect a residual variable, capturing the effects of contextual variables, including economic incentives or disincentives associated with ownership and funding mechanisms, access to alternative care and national level professional and sociocultural variables.
The ways hospitals are paid influences their activities, though the effects may vary depending on whether the hospital is private, public, for-profit or not-for-profit. Japanese hospitals are privately or publicly owned, though all are not-for-profit. The great majority of Canadian hospitals, while not formally public, are in practice publicly controlled and operated as not-for-profit institutions. Hospitals paid through prospective schemes, such as global funding or the American Diagnosis Related Group approach, tend to have shorter stays, though ownership can matter. 19 A for-profit hospital may act to make sure stays are short; a not-for-profit institution may supply care, including more inpatient days, deemed necessary to realize sufficient care quality if fiscally feasible. 19
Since 2003, many Japanese hospitals, including the ones in this study, have been adopting the diagnosis procedure combination/per-diem payment system (DPC/PDPS) that combines prospective and retrospective fee-for-service elements. 19 While clinical procedures are compensated on a fee-for-service base, daily inpatient reimbursements depend on the LOS relative to that expected for each ailment. The effect of DPC/PDPS payments on LOS is nuanced, especially if there is otherwise excess capacity and daily costs are lower than incremental revenues.19,20 In Ontario specifically and Canada generally, hospitals are primarily funded globally. 1 The relatively short Canadian hospital ALOS shown in OECD health data is consistent with this payment approach.
The supply of ALC beds and the availability of formal and informal support for home care tend to shorten LOS by providing destinations for discharged patients. 13 OECD figures show that overall Japan has more hospital beds of all types per 1000 people, 13.6, than Canada, 3.2. 2 However, these numbers broken down show that in 2007 Japan had 7.1 acute care and 2.7 long-term care beds per 1000. 16 The comparable 2007–2008 Ontario numbers were 2.5 acute care and 8.7 long-term care beds per 1000 population.21,22 Japan’s relatively large supply of acute care beds and smaller number of LTC beds are expected to be associated with longer Japanese LOS.
In Canada, ALC patients account for about 5% of hospitalizations and 14% of hospital days. 23 Whether a patient was discharged to a formal LTC facility was linked significantly and positively to LOS in the Canadian sample and full model for both cancer and AMI. In Canada many of these patients would in effect, if not practice, be identified as ALC. In all cases, the expected positive link within the countries between LOS and the relative supply of acute beds and negative tie to that of long-term beds were not apparent.
In Japan, the hospital with the shorter stay for cancer and AMI was located in an area with a larger supply of acute care beds and smaller supply of LTC beds per 1000. This combination should in theory produce longer acute care stays. However in Japan, it could be that ownership mattered: the private not-for-profit organization perhaps was acting to fill its capacity, which was higher than its counterpart, in order to maximize revenues. Alternatively, it could be that the public hospital’s marginal costs for longer stays were higher than those of the private hospital. In Canada, the hospital with the longer stays differed for each diagnosis.
Sociocultural variables operate at multiple levels in the healthcare ‘organizational field’ as actors share understandings and logics.24,25 Clinicians and healthcare managers, embedded in national cultures, tend to share assumptions of the rules of social behaviour and hold common views on what is appropriate care. These influences are expected to be more prevalent when making decisions when information is not complete, as is often the case in healthcare. 25
Practice norms, such as patient flow procedures, discharge decisions and approaches to post-discharge treatment are socially created by professionals and policy makers. Formal approaches are expressed by Japan and Ontario’s governments support for home-based care and discharge planning by hospitals. Related are treatment courses characterized by several planned short hospital visits rather than a single unbroken inpatient stay. Within jurisdictions, organizational cultures, expressed through implicit hospital norms, also influence LOS. This is demonstrated by research showing variation in medical treatments between regions 26 and hospitals 27 within countries.
The Japanese data suggest that a long LOS is a professional norm for cases of surgical intervention for AMI. The higher rates of stent use in the Japanese patients, and the positive tie to LOS, suggest that these operations may contribute to longer LOS. Further CABG is linked to longer Japan LOS, but not for the Canadian patients. The data do not allow testing for the more general proposition that all surgeries are linked to longer LOS; all of the colorectal cancer patients in the sample had undergone surgery.
The tendency for patients who die in the hospital to have longer LOS in the Japan only and full sample regressions indicate a significant link. This suggests that in the Japan hospitals patients with very serious cancer cases were more likely to be kept in hospital until their demise, rather than being discharged and readmitted, or sent home to receive treatment as an outpatient. The latter is a more common practice in Canada.
Conclusions
This study overall validates at the patient level the macro OECD comparative LOS data showing that, despite recent reductions, Japan continues to have relatively long hospital LOS. That these differences remained apparent when controlling for patient factors suggests the minimum LOS norm, particularly for surgery patients, is longer in Japan than in Canada. Particularly for cancer patients, the longer LOS could be partially attributable to keeping terminal patients in the hospital. The results support the broader view that decisions on LOS are not typically evidence based; 28 rather LOS is a type of ‘choice variable’ 29 jointly determined by physicians and hospital administrations operating in broader systems and cultures which supply contextual variables. 13
One finding suggests that the shorter Canadian LOS could be linked to higher unplanned readmissions for AMI and is contrary to the general consensus that LOS is not linked to outcomes. However, it is consistent with the elderly hip fracture study cited earlier. 6 The study design though did not allow determining post-readmission survival rates; though inconvenient and perhaps risky for patients, survival rates may be comparable in the hospitals studied, after patients are readmitted.
The degree to which the findings can be generalized is limited by the small sample of hospitals, two in each country, and limited number of diagnoses, also two. The differences in the LOS practices between the Japanese hospitals particularly call for study of a broader sample of hospitals.
For policy makers, particularly those in Japan, it would appear that although clinical factors suggest that LOS could be reduced, there is a possibility that this may be associated with more readmissions. From the Canadian perspective, it is apparent that though LOS is relatively short already, LTC capacity shortages contribute to longer Canadian stays for some patients. However, this finding could be because Canada’s relatively short LOS offers limited temporal slack that can absorb differences in certain patient situations, such as those associated with waiting for LTC.
At the system level, the overall lower costs in Japan seem to be despite, not the result of, longer LOS. Japan’s government has controlled expenditures largely by curbing in the national medical fee schedule. 30 There is evidence that the new DPC/PDPS system has reduced resource use, including LOS.
The study contributes to developing a protocol for comparing hospital performance between countries at patient levels and serves to build on the few studies of this type mentioned earlier. The widespread adoption of the ICD system and the use of data that are as objective as possible enable hospital- and patient-level comparisons. These can lead to better understanding of the reasons for differences, or confirming that other factors do not matter. Adding treatment data across the whole patient experience, including primary care costs, would provide a clearer view of both economic and clinical efficiencies. This type of knowledge could facilitate more effective international policy and management learning that can better inform decision-making, at system and hospital levels.
Footnotes
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
The study received funding support from the Pfizer Health Research Foundation (Japan) and the Social Sciences and Humanities Research Council of Canada.