
Abstract
This paper describes and contrasts the implementation of Lean Thinking – a quality methodology that emphasises waste reduction and performing at higher levels of productivity with the same or less resources – into New Zealand’s healthcare system. As the field is relatively new, three literature-based exemplar cases were developed to provide an analysis framework to analyse the three New Zealand research sites, which had activities, teamwork, leadership and sustainability as its core themes. Each research site’s case was developed from primary data gathered through interviews, augmented by secondary data from project reports, District Health Board websites and media stories. The results highlight the benefits of a supportive quality-focussed organisational culture, executive management involvement and cross-functional teams as enablers. Further, work intensification and workplace resistance were also evident in varying levels within the sites. The study, while reiterating the problems of introducing quality methods from other domains into healthcare, presents the New Zealand context and reinforces that organisational preparedness as a significant factor which contributes to implementation success. This study goes beyond investigations of the use of Lean tools, changing improvement metrics and descriptive statistics to identify the contexts and variables which surround quality and process improvement implementations.
Keywords
Introduction
Lean Thinking is the generic label given to the Toyota Production System’s combination of management philosophy and activities 1 and it is being introduced into healthcare systems across the globe as a solution for the problems of quality and costs.2–4 In 2008, the New Zealand government introduced Lean Thinking to its health system through a series of projects, which included emergency departments (EDs).
EDs have become topical for healthcare performance and quality improvement as they signal a hospital’s ability to respond to demand within the context of the worldwide phenomenon of ED overcrowding, which is due to reasons both within and outside of the organisation. 5 Lean Thinking has been found to have positive impacts on both patient quality and safety in ED’s 6 contributing to reductions in overcrowding by enhancing patient management and flows. 7
This paper presents the experiences of three ED Lean Thinking implementations that took place in New Zealand hospitals from 2008 to 2010. Since 2008, New Zealand’s largely publically funded health care system, which delivers care to its population of 4.1 million people, has been directed to focus on frontline services, quality and service integration. Hospitals are operated by 20 democratically elected District Health Boards (DHB) to provide services to regional populations guided by a set of national performance targets. The recent changes also have resulted in the recentralisation of certain functions, including national oversight of information technology, workforce forecasting and system quality. 8
The paper contributes to the literature, first, by adding another country’s experiences to the emerging Lean implementation literature, a country whose system has reputation for regular and wide ranging system change. 8 Second, through cases developed from the extant literature that enable identification of key analytic themes, the study’s analysis extends the investigation beyond Lean tools, improvement metrics and descriptive data to include the contexts and factors that determine implementation success. 9 Thus, academic insight is offered regarding the introduction of Lean tools and techniques in healthcare and provides further evidence of the importance of organisational readiness as a precursor for healthcare organisational innovation. 10
Lean in healthcare
The term ‘Lean’ describes the manufacturing methods used by the Toyota Motor Corporation specifying value in terms of the customer and identifying elements to maximise that value through processes such as work streams and process flows. 1 Performance and quality improvement are achieved by activities or tools 1 such as Plan-Do Study-Act (PDSA) improvement cycles, the 5S visual work organisation method, A3 problem solving and value stream mapping; some of which may be used as part of structured or cyclical improvement events. 11 Although, as the tools were developed in the manufacturing environment, they may not be directly transferable to service industries. 12
Lean provides a philosophy, a management system and a toolset for healthcare organisations to use to lessen error rates, improve quality care and reduce wait-times for patients. 13 It is these processes which are credited with savings and cost reallocations. 13 Improvements can be achieved by reevaluating patterns of demand and redesigning the processes and work spaces, 14 which have been identified as viable alternatives to traditional hospital quality problem solving methods. 7 However, despite the benefits, few healthcare institutions are undertaking systematic organisation wide Lean implementations 4 with Lean many times being introduced as independent initiatives or as unconnected multiple projects. 15
Introducing Lean to a healthcare environment requires a certain sensitivity to the interplay between the operational and professional domains in healthcare. 16 Similarly, unlike value identification in manufacturing, healthcare customer value depends on who the customer is 9 and the customer’s expectation of value is then dependant on their identity and position within the health system. 17 As a result, Lean efforts in hospitals may not be directed towards organisational performance objectives, but more pragmatically to those outcomes with which most actors can align. 17 It is therefore preferable that Lean is part of an organisation’s strategy leading to sustainable continuous improvement. 18 Moreover, Lean should not be used as a cost elimination methodology, 18 particularly if the organisation is seeking cost control rather than service innovation or improvement 14 – for in times of financial constraint, it can be difficult for healthcare leaders to change their view of their workplace’s systems. 19 Managers and staff implementing Lean should receive training not only to be able to undertake the new techniques but also to prevent a return to their past behaviours. 20
Lean healthcare is generally executed by teams operating in a participative environment and organised across administrative or functional boundaries.21,22 The role and the style of a Lean team leader are required to be more functional than authoritarian utilising facilitation skills and creating a climate of encouragement23,24 by mitigating power differentials between staff to ensure inclusion, encouraging innovation and sustaining new work routines. 22 These attributes are more important since the ‘hero clinician’ is less relevant as patient pathways become the operational norm.21,24
Top management and leadership,25,18 as well as the engagement of the hospital’s senior doctors, 26 provide vital support to Lean initiatives. However, clinical engagement may be restricted to those who have been ‘converted to Lean’27,p.1339 or to occupational groups whose work organising principles are similar to Lean approaches.19,22 There are few reports that include the examination of Lean’s effects on the health workforce 23 or its contribution to the intensification of work as found in manufacturing. 28 Although O’Donnell 29 and Willis 30 found indications of work intensification in organisations following some Australian Lean healthcare implementations, Waring and Bishop 27 provide insight into the issues of social organising within a UK hospital.
Research context
As Lean Thinking has only recently been introduced into the New Zealand healthcare system, it is relevant to seek to understand how it is being implemented as New Zealand EDs. By uncovering the outcomes and by situating the implementation within the hospital’s contexts the factors for success can be determined. 9
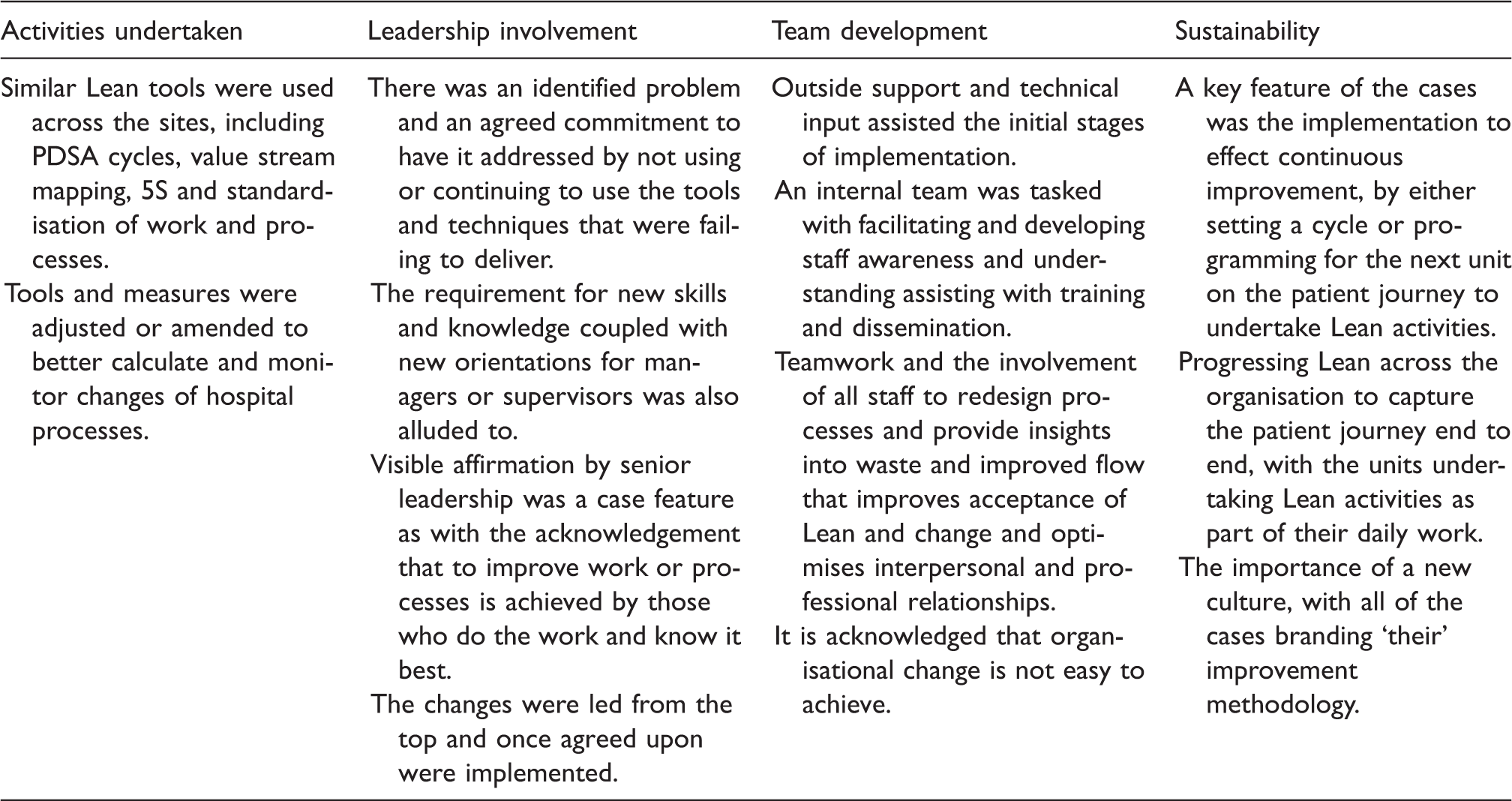
Lean implementation indicators identified from the three exemplar cases.
Research method
The case study is a methodology that lends itself to examining new phenomena, 32 using quantitative and qualitative data to develop an answer to a given research question – particularly when a ‘how’ or ‘why’ question is being posed. 33 A weakness of the case study method is the difficulty to generalise the results into other cases or situations; 33 in particular, a situation that exists for healthcare quality, 3 leading authors suggest more rigorous research to expand on the exploratory and descriptive nature of the Lean healthcare cases published so far.2,3,23
Summary of case study organisations and Lean activities.

ED: emergency department.
Secondary data were gathered from a range of sources and were used to triangulate aspects of the implementations, their foci and evidence of process improvement. Hospital statistics and population data were found in national health reports, DHB annual reports and from the respective DHB websites. Summary and periodic progress reports of the implementations provided details of the activities, timelines, outputs and efficiency measures. Internal memos and staff newsletters provided additional evidence surrounding implementation progress.
Summary of respondents.

Case theme results.

ED: emergency department.
Findings
The findings reveal that the sites had different implementation approaches that were influenced by a range of management, resource and readiness factors. There were significant commonalities found in terms of the tools and practices adopted. Reflections on the use of the problem solving and quality tools were positive, with staff commenting favourably on the results of their use e.g. ‘it has improved definitely… We’ve streamlined our documentation and the process of getting the patients up to the ward is a lot easier’ (Respondent C4). This is not too dissimilar to other reported Lean healthcare implementations, where flow, waste and patient journeys are targets for improvement projects and a similar range of effects are observed. 6
However, key differences emerged between the cases with respect to the involvement of organisational leaders. Top leadership engagement was found lacking at Sites A and C, where the respondents identified the lack of engagement quite readily, e.g. This is a huge opportunity for executive managers to come down and talk to some of the real experts, and no one ever did. They were actually offered coaching – customised to how they want it – and they didn’t take up that offer. (Respondent A5)
Site B’s leadership involvement was significantly different as it was coordinated through an oversight committee, which sought to promote organisational ownership by reframing the ED Lean work to take a wider hospital view and to be more about the quality of a patient’s journey. Site B also exhibited the devolution of authority to the primarily nurse led teams to ‘basically get on with it [and] produce outcomes’ (Respondent B6). Nevertheless, the integration of clinicians was variable across the sites, in part through the existing hierarchies or through the different engagement processes, e.g. ‘I’m not convinced that the medical input was as good as it could have been. I think if you want to drive a fundamental change then you really need to get the doctors on-board’ (Respondent C2).
While Site B seemed to have the most favourable team working, all of the sites experienced morale improvements. However, work intensification was reported by respondents and was dealt with differently by each organisation. At Site A the staff absorbed the additional workload into their own time, while at Site C, the staff prioritised tasks with what they considered to be patient-centred or care-oriented work to be completed first. Even though both of these sites had made contingencies for additional compensation or overtime hours, the organisation’s cultural cues undermined some of the staff’s confidence to enact these provisions, e.g. [the manager would say] if we need to pay [for extra time] then we can, but the innuendo from higher up says I shouldn’t be paid for doing [these] things, it should be done on your own time, or done in the time when you’re working … that’s the subtleness from the organisation. (Respondent A10)
Similarly, across the EDs, the level of staff ownership for the changes was variable. Workplace resistance manifested itself as a reluctance to engage or a de-prioritisation of Lean work, particularly at Site C where the volatile staffing levels significantly affected the ED, e.g. ‘we only had 5 staff, we don’t have 9 or 10, you take 3 of those staff away and you’re at 50%, so it was very difficult to resource or to commit time to it’ (Respondent C1). The planning, preparedness and a quality culture of the organisation seemed to be able to minimise the effects of these staff issues. At Site B their quality culture helped to localise Lean e.g. ‘we have these basic principles of quality improvement, [we’ve] just renamed to be honest’ (Respondent B7). As the implementations progressed the realisation of change and its effects became more apparent. It was at this stage that the organisational immune systems manifested themselves, e.g. It went along swimmingly for a while, until people realised that there was an expectation that they do things other than what they were currently doing: that it might need change on their behalf. I guess we weren’t well equipped to deal with the sorts of behaviours that came out, and we didn’t understand that there was real angst behind that, in terms of what people were feeling. (Respondent A2)
Case results and implementation indicators.

, evident; =, neutral; ✗, absent.
Discussion
The method which is used to implement Lean is significant for the success of an endeavour 16 and this study highlights the apparent differences of implementation method in relation to the prospect of longer term outcomes. Site A’s project management approach, while successful for delivering Lean outputs and wait-time gains, was not connected to an organisational strategy and thus, not linked to overall organisational performance. The contrast between Sites A and B points to the conclusion that organisational preparedness and an existing quality improvement strategy provide the basis for an increased likelihood for implementation success. The importance of preparedness or readiness and organisational strategy has been acknowledged6,18 and it is also prominent within the Lean implementation exemplars. There, the organisation’s leaders were committed to change and so they facilitated sets of enabling resources to achieve organisational transformation. This is similar to the environment found at Site B, while Site C’s adoption of Lean to be the organisation’s quality framework revealed its intention to prepare and hence provide for some progress. Resistance to change is a perennial problem with quality improvement, particularly when implementing Lean into healthcare. 36 Although resistance was acknowledged at the case sites, it was seen as secondary or a consequence rather than being accorded any prominence or attention in plans. 37
The cases show that implementing Lean into healthcare improves flow and reduces waste. But after the easiest and most obvious problems are addressed, sustaining gains maybe more difficult. 12 Bicheno 12 offers the solution of a phased or staged systematic implementation across the organisation, building on each successive project’s success, a process observed in the exemplar cases. This pattern is also observed in the UK by Burgess and Radnor, 15 with some hospitals beginning to implement more system type adoptions of Lean. Similarly, setting improvement metrics such as wait-times at the exclusion of the other internal customers seems to solve little. For example, Site A’s patient-streaming projects did reduce the wait-times for non-admitted patients, but the lack of synchronisation with the wider hospital found admitted patient wait-times barely improving. Admission times were the principal improvement targets at the other two sites, as these sites possessed an organisational quality strategy or policy that focussed on improving patient flow. These strategies or policies provided the direction for staff to be able to recognise the fundamental Lean tenet – understanding who the customer is – and thereby enabling a focus on synchronised flow improvement.
Conclusion
This paper reviews the performance of three New Zealand hospital ED’s implementation of Lean Thinking. The three sites implemented Lean differently, with some leveraging their existing quality culture and team processes. The different outcomes obtained by the EDs were: Site A substantively improving their non-admission patient wait-times, but failing to synchronise these improvements with the hospital; Site B improving patient admission times through ward admission synchronisation and Site C achieving reduced admission wait-times, even though their project was hampered by unstable staffing.
Lean Thinking is a quality system that appears to be able to be successfully applied to hospitals to realise waste reduction and improved patient flows. As a set of principles and techniques, its implementation is influenced by the environment in which it operates. Key influencers found from this research were top leadership involvement and visibility, an overarching programme of improvement governed by a stated strategy or policy and the existence of some organisation capacity or team culture, all of which are components of organisational readiness. Readiness factors influenced other aspects of implementation. While a project management implementation methodology may make many gains initially, sustaining the gains relies on the project’s integration and identifying what is needed for any changes to become routinised. Those sites with a quality improvement strategy or policy achieved integration or routines, in some form. Furthermore, the possibility of work intensification has the potential to derail any gains made from Lean. Therefore, any unintended consequences that the introduction of Lean may bring through role and job changes should be considered by organisation leaders.
Implementing Lean into healthcare challenges traditional healthcare delivery structures and asks that new types of skills and continuous learning become the organisational norm. The preparedness or readiness of an organisation appears to make a difference to achieve this change, particularly when taking the patient journey paradigm as the core quality value. For without this engagement, in the words of one frustrated New Zealand clinician: ‘we’re just going to end up with a temporarily tidier ED’.
Footnotes
Acknowledgements
The author would like to acknowledge the thoughtful comments of reviewers and the journal editor which helped to finalise this work, along with Richard Greatbanks for his supervisory assistance and research resources and Robin Gauld for commenting on earlier drafts.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.