
Abstract
As patient autonomy and consumer sovereignty increase, information provision is considered essential to decrease information asymmetries between healthcare service providers and patients. However, greater availability of third party information sources can have negative side effects. Patients can be confused by the nature, as well as the amount, of quality information when making choices among competing health care providers. Therefore, the present study explores how information may cause patient confusion and affect the behavioral intention to choose a health care provider. Based on a quota sample of German citizens (n = 198), the present study validates a model of patient confusion in the context of hospital choice. The study results reveal that perceived information overload, perceived similarity, and perceived ambiguity of health information impact the affective and cognitive components of patient confusion. Confused patients have a stronger inclination to hastily narrow down their set of possible decision alternatives. Finally, an empirical analysis reveals that the affective and cognitive components of patient confusion mediate perceived information overload, perceived similarity, and perceived ambiguity of information.
Keywords
Introduction
Increased patient autonomy and consumer sovereignty confront patients with a higher degree of responsibility and more involvement in health decision-making processes. 1 To fulfill their expanded role, patients need information about health service providers, diseases, and different treatment methods to decrease information asymmetry. Therefore, the provision of precise and up-to-date information is essential 2 to allow patients to make informed choices. There is an ongoing discussion in health policy research on how patients can be provided with more information and how access to quality information can be facilitated.3,4 However, thus far, health policymakers have not considered potential problems that arise from the increased availability of quality information. 5 Authors such as Arora et al. 6 report that the majority of patients are overwhelmed by the sheer quantity of health information available. Patients increasingly need experience and expertise to understand the available health information. 7 Patients can experience psychological dissonance and frustration in making decisions regarding treatments 8 because the accuracy, quality, and quantity of information may be inconsistent. 7 These negative side effects of greater information availability may cause confusion among patients seeking medical treatment. In turn, patient confusion may cause behavioral reactions among patients such as hastily narrowing down their set of possible decision alternatives. 9 Although not intended by health policymakers and other information providers, these side effects should be taken into account when providing information because they contradict the primary goals of allowing patients to choose the best health care provider and encouraging competition among providers. 3 To analyze these challenges in information provision, the present study applies the concept of consumer confusion, which is discussed in the consumer behavior literature (e.g. Mitchell and Papavassiliou 10 ). The current study focuses on confusion and its importance in patients' decision making.
In the next section, we describe the concept of consumer confusion, discuss the topics of health information and patient choice, and combine those considerations into a model of patient confusion. An empirical study is carried out to validate the postulated patient confusion model. The concluding section includes a summary, a discussion of the study's limitations, implications for health policymakers, and avenues for future research.
Conceptual considerations
The consumer confusion concept
The concept of consumer confusion was first developed to explain consumer reactions in the context of brand similarity (Mitchell and Papavassiliou 10 ). This concept postulates that consumers misinterpret the information given or fail to understand it. 11 Consumer confusion can impact consumer behavior. For example, it can decrease consumer satisfaction (e.g. Wang and Shukla 12 and Shukla et al. 13 ) or affect brand loyalty 14 or the time consumers take to make their decisions. 14 While experiencing confusion, consumers may reevaluate their opinions on products and services. 15 Mitchell and Papavassiliou 10 discuss different strategies consumers can use to cope with their confusion. For example, as a beneficial coping strategy, consumers can seek the opinions of experts. However, confusion may also cause consumers to narrow down their set of alternatives quickly just to be done with the process.
The definition of consumer confusion is now shifting to a multidimensional construct (e.g. Mitchell and Papavassiliou, 10 Mitchell et al., 15 and Schweizer et al. 16 ) because researchers understand that confusion is triggered not only by similarity stimuli. Several studies assess consumer confusion as a multidimensional construct and address various aspects in areas such as consumer goods (e.g. Wang and Shukla, 12 Schweizer et al., 16 Drummond and Rule, 17 Leek and Kun, 18 and Chen et al. 19 ), services (e.g. Shukla et al., 13 Ashton, 20 and Drummond 21 ), cause-related marketing, 22 and the use of the internet in acquiring products or services (e.g. Matzler et al.23,24). In current research, the three-dimensional approach is widely accepted. 18 It posits that information overload, perceived similarity, and ambiguity lead to confusion and affect the decision-making ability of the consumer. 10 First, consumers have limited cognitive resources for processing information. The consumer may face a mass of information or products, which he or she often cannot handle, and may encounter difficulties in the decision-making process. These cognitive challenges can lead to confusion based on information overload. 15 Second, consumers may not be able to differentiate between different products or services. The consumer perceives them to be similar despite the fact that they are different in quality or function. 14 Third, confusion can be caused by the ambiguity and complexity of information concerning a product or service. 10
Health information and patient choice
Patients have become more active in provider choice25,26 as more demand-driven healthcare systems emerge; this encourages competition among providers and thus makes care more responsive to patient needs while improving efficiency and quality. 27 Patient participation in the choice of a hospital for an inpatient stay is restricted to elective surgery because in situations requiring emergency treatment the time frame and the health conditions of the patient do not allow for the consideration of alternative providers. 28 According to the German Federal Census Bureau, the majority of all surgeries (63%) in Germany are elective. In their literature review, Dietrich and Grapp 29 state that in 30–40% of cases of inpatient treatment in Germany and the US, patients act as single decision makers when choosing a provider. For elective surgery, patients seek reliable, meaningful, and transparent information to make health choices. 30 According to the literature review of Victoor et al., 3 patients' previous healthcare experiences are the most important driver of the future choice of a provider.
However, patients usually face a rarely occurring or entirely new situation when making choices regarding providers. Consequently, they usually cannot refer to their own treatment experiences and commonly lack knowledge to judge provider quality. Therefore, patients rely on third-party information sources and access multiple information sources to evaluate and choose a hospital within the context of non-urgent care or elective surgeries.
31
Figure 1 gives an overview of third-party information sources available regarding provider choice.
Overview of third-party information sources and their impact on patient confusion.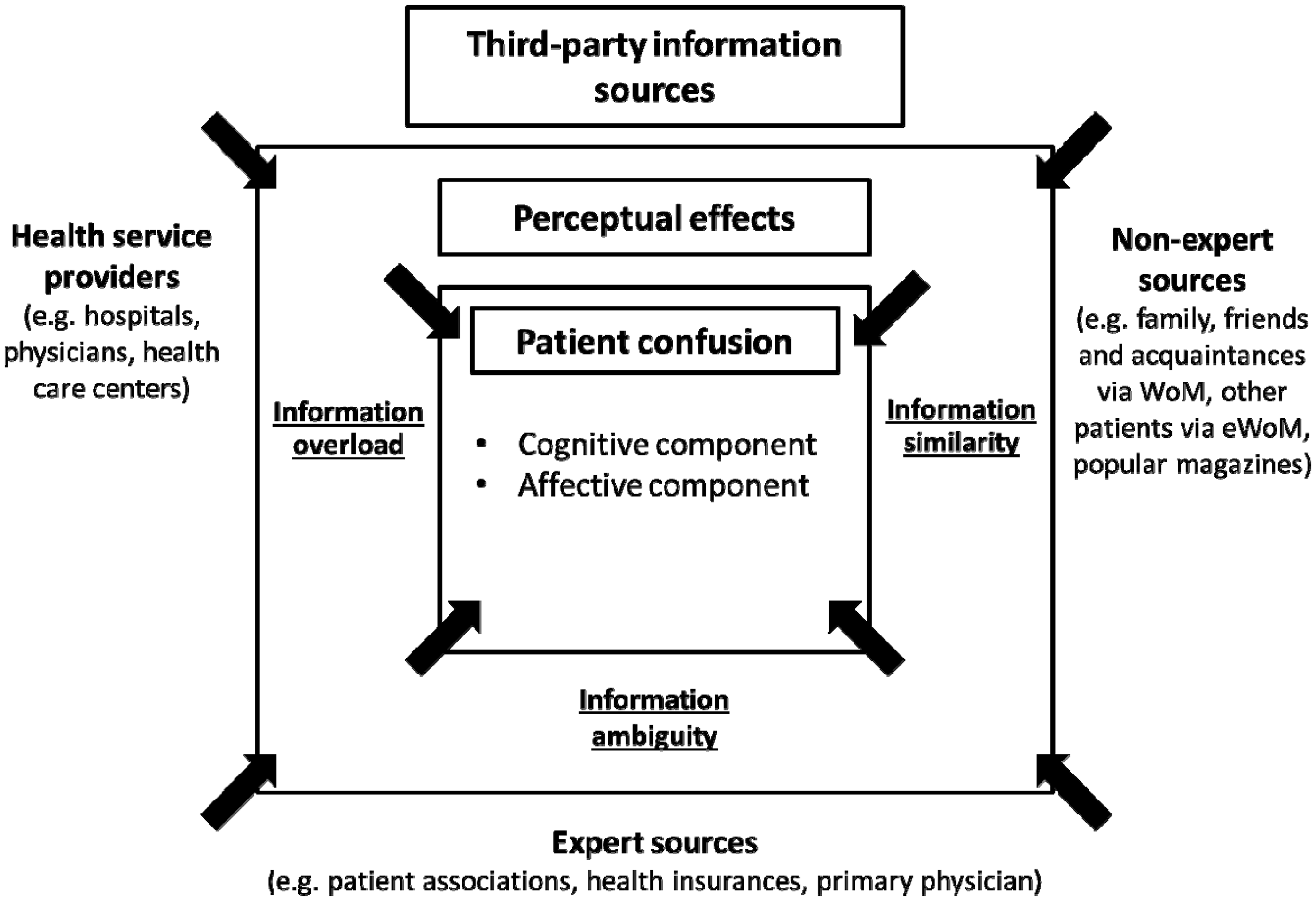
In particular, in gatekeeper health care systems, recommendations by the referring primary physician remain the primary informational third-party expert source. 32 For several diseases and types of surgeries, patient associations exist as expert sources, providing patients with the latest treatment options and allowing them to exchange service experiences. 33 Health insurance companies can act as agents for patients and may be added to list of third-party expert sources; they provide patients with quality information and give them recommendations. Provider-related information such as hospital quality reports or hospital marketing communications represent another third-party information source. 34
Word-of-mouth from relatives and acquaintances 35 is said to be the main non-expert source, providing patients with simple recommendations. New information channels are available that allow better access to the specified information sources due to the emergence of online media. 36 Internet access allows patients to assess reviews of hospitals using online-rating platforms; this functions as electronic-word-of-mouth. 37 In their reviews, patients write about personal experience and judge the quality of the medical treatments and services provided. These patient reviews have gained importance as a new non-expert source for information related to provider quality. 32 Andreassen et al. 37 show that over 70% of users search the internet for health-related information at some point.
According to Drevs, 4 an ongoing discussion in health services research continues regarding which of these information sources patients actually use for provider selection and how they interpret information on quality. Policymakers assume that patients make rational choices based on the information available, weighing and balancing relevant attributes and values. 3 However, based on empirical analyses of provider choice decisions, we know that patients often use shortcuts or intuitive heuristics due to a lack of interest and difficulty in interpreting the extensive and sometimes contradictory information regarding quality. 9
Few patients seriously consider an alternative to their nearest provider when undergoing surgery. 3 Additionally, patients use informational cues, such as ownership status, teaching status, and hospital size, when choosing a hospital. 4 Although these data may be less precise or even inaccurate as quality indicators, patients consider these informational cues to be easy ways to make provider choices. 38 It seems that patients show a lack of awareness, interest, comprehension, and acceptance of information on health provider quality. 39 Consumer confusion may be a negative side effect resulting from the quality and quantity of information and may be the reason that provider choice relies on little factual information.
The patient confusion concept
In Figure 1, we illustrate how third-party information sources can cause patient confusion. In the review of Victoor et al., 3 we find clear evidence that the quality and quantity of available information on health provider quality meet the three criteria for consumer confusion, namely perceived similarity, information overload, and complex, contradictory or ambiguous information. Fotaki et al. 27 show that patients may perceive little difference in provider quality, so they are unwilling to get involved with the set of possible alternatives; this indicates confusion related to information similarity. A lack of competent health knowledge as well as an insufficiently clear presentation of the information regarding quality further enforces the perceptions of marginal differences between providers. 40
Information overload among patients deciding among health care providers has been associated with greater information availability in studies by Damman et al. 41 and Hibbard et al. 42 Arora et al. 6 report that the majority of people are overwhelmed by the sheer quantity of health information available. Information overload decreases decision-making ability, leading to confusion (e.g. Malhotra 43 ). Some researchers argue that less rather than more information could help patients decide more easily (e.g. Damman et al. 41 and Peters et al. 44 ).
Patients are confronted with contradictory information when assessing different informational sources, 3 leading to more confusion. The referring physician may recommend choosing a certain health provider while patient reviews on a rating platform suggest the opposite. Conflicting information does not necessarily originate from multiple sources. Even within the same information source, patients can be confronted with divergent information. Quality records from hospitals, for example, are a potential source for informational ambiguity. In these records, the patient may be confronted with divergent provider-related quality indicators, some indicating a high quality provider and some suggesting low quality. In this context, Hasler 45 concludes that giving the patient scientific and complete health information can lead to confusion, which may be explained by perceived ambiguity in the information. 10
Although antecedents of patient confusion have already been identified as barriers that patients encounter while assessing quality information, thus far, studies have not analyzed these side effects of information availability conjointly with the consumer behavioral model of consumer confusion.
For an analysis of these identified negative side effects of information availability, the aforementioned consumer confusion concept, discussed in consumer behavior literature (e.g. Mitchell and Papavassiliou
10
), can be applied to the context of health provider choice. Figure 2 shows the proposed patient confusion model, grounded in the consumer confusion concept of Mitchell et al.
15
Overview of the patient confusion model.
Based on the work of Mitchell and Papavassiliou, 10 we define the following antecedents that cause patient confusion: (1) perceived similarity, (2) information overload, and (3) complex, contradictory or ambiguous information about the quality of health service providers. A literature review by Mitchell et al. 15 demonstrates that, in addition to the aforementioned antecedents, three different components of confusion exist, which we adopt for the patient confusion concept: a cognitive dimension, an affective or emotional component, and the behavioral consequences (i.e. conative component). The cognitive dimension states that the consumer or patient fails to interpret information about products and services, which presumably influences decision-making and consumer information processing (e.g. Mitchell and Papavassiliou 10 ). These cognitive challenges caused by confusion can lead to poor decisions that a consumer otherwise would not have taken. 46 Mitchell et al. 15 introduce an affective component of confusion in their model. Schweizer et al. 16 note the importance of emotion in consumer confusion as well. Walsh 47 describes this dimension as an uncomfortable state of mind. This emotional reaction is task-induced and caused by the three dimensions of perceived similarity, perceived information overload, and perceived ambiguity of information. 15 Confused people can experience negative emotions, such as anxiety, frustration, anger, and irritation. 15 Wang and Shukla 12 demonstrate in their study that negative affect caused by the antecedents of confusion reduces consumer satisfaction. Based on their findings, the current study also refers to the affective component of patient confusion as negative affect. The third component is the behavioral dimension. 15 When confusion exceeds a certain level, the consumer tries to reduce it. 18 Therefore, the behavioral component can result in strategies applied by the individual to cope with confusion. This component is illustrated by the strategy of “narrowing down the choice set” in Figure 2.
Mitchell and Papavassiliou 10 discuss different strategies for coping with confusion, such as postponing, abandoning, sharing, or delegating the decision. The consumer confusion literature proposes “narrowing down the choice set” as a further strategy to cope with confusion. 15 Decreasing confusion by reducing the choice set can help the patient alleviate distress by perceiving their decisions as easier and less confusing when the set of alternatives is smaller. However, narrowing down the choice set can have negative implications, too. Mitchell and Papavassiliou 10 propose several ways consumers can reduce the choice set. The authors adapt those strategies for patients in the context of health care. Patients can consider specific criteria, such as popular brands or other product characteristics they have experience with; they can use stereotypical quality perceptions to reduce their choice set 4 ; or they can reduce the choice set without further consideration just to get the decision over with. However, an ill-considered, hasty and rash reduction of alternatives could negatively impact patient health, especially if the patient is unable to distinguish between the alternatives, e.g. the quality of a service or effectiveness of a treatment method.
From a health policy perspective, this style of decision-making challenges the concept of patient sovereignty, and health policymakers need to understand whether and how patients reduce their set of alternatives due to confusion.
Taken together, these considerations lead to the following hypotheses: H1: The cognitive component of patient confusion has a direct and positive effect on narrowing down the choice set. H2: The affective component of patient confusion (i.e. negative affect) has a direct and negative effect on narrowing down the choice set. H3a: Perceived similarity of information has a direct and positive effect on the cognitive component of patient confusion. H3b: Perceived similarity of information has a direct and positive effect on the affective component of patient confusion (i.e. negative affect). H4a: Information overload has a direct and positive effect on the cognitive component of patient confusion. H4b: Information overload has a direct and positive effect on the affective component of patient confusion (i.e. negative affect). H5a: Perceived ambiguity of information has a direct positive effect on the cognitive component of patient confusion. H5b: Perceived ambiguity of information has a direct and positive effect on the affective component of patient confusion (i.e. negative affect).
Additional determinants
Bandura's social cognitive learning theory 48 identifies self-efficacy as an important factor in individual health behavior. A strong perception of general self-efficacy is, in particular, based on the experience that one is capable of dealing with challenging situations. People with high self-efficacy perceptions strive to achieve higher goals, are more persistent and are more willing to cope with challenging issues. Self-efficacy leads to a greater capacity to deal with new situations. Against this background, it can be assumed that patients with strong self-efficacy perceptions are less inclined to narrow down their choice set hastily.
Another factor that affects health behavior is health involvement. Foxman et al. 49 stress the importance of involvement in the context of confusion. A high degree of involvement increases individual activation and the ability to process information. As a consequence, higher levels of health involvement should decrease the perceived cognitive challenge connected with decision making. In the context of health decision making, high involvement should lead to a stronger effort to cope with confusion. Thus, highly involved persons should feel less inclined to narrow down their choice set.
Thus, hypothesis H6 and H7 read as follows: H6: The lower the degree of self-efficacy, the stronger the inclination for patients to narrow down the choice set. H7: Health involvement has a direct and negative effect on the inclination to narrow down the choice set.
Study design
Procedure
To the best of our knowledge, the current study is the first empirical paper to investigate the antecedents and consequences of patient confusion. Hence, the primary focus of our research is exploratory in nature. Thus, instead of calculating unbiased parameter estimates, the current study primarily aims to generate initial insights regarding the mechanisms underlying patient confusion. These insights may then provide researchers with a basis for the development of more detailed models of patient confusion. Against this background, the empirical study described here considers a mid-sized sample (i.e. n = 198), which was drawn via quota sampling. The quota sample is based on the criteria of gender and age. Appendix 1 shows the sample characteristics of the subjects surveyed.
A challenge in designing this empirical study was to evoke patient confusion while simultaneously creating a realistic situation. The chosen decision-making scenario had to induce perceptions of similarity, ambiguity, and information overload as confusion antecedents. We decided to use the scenario technique, in which respondents had to imagine choosing a hospital for a knee arthroscopy after a sports accident with the help of an online survey. The respondents were offered online information on three existing German hospitals; the information consisted of extracts from published quality reports from the hospital itself and patient assessments of the hospitals through online review portals. Three different decision-making scenarios with slightly varied hospital quality reports and patient reviews were considered. The 198 subjects included in the quota sample were randomly assigned to one of the three decision-making scenarios.
The rationale for choosing this procedure was not to facilitate hypothesis testing; rather, we wanted to prevent the data from being biased by a statistical artifact induced by a single decision-making scenario stimulus presented to the interviewees. The resulting data were based on the group mean-centered values of the responses to the question items from all three decision scenarios (see Note 1) combined into one data set. The model was validated with the help of SMART PLS 2.0, 50 and the assessments of the structural equation model and the measurement model were based on Hair et al. 51 recommendations.
Measurement
All considered items were based on measurement scales used in past research except for the cognitive component of the patient confusion scale. To measure the different confusion antecedents, the scales proposed by Walsh et al. 14 were applied. A two-item scale reduced and adapted from Mitchell and Papavassiliou 10 was used to measure the inclination to hastily narrow down the choice set as the behavioral consequence of confusion.
We used the self-assessment manikin (SAM) scale 52 to measure the affective component of patient confusion (i.e. negative affect). The SAM scale is based on figurative representations that depict varying emotional states. Based on Russell and Mehrabian's 53 Semantic Differential Scale, the SAM scale consists of three dimensions, namely, valence, arousal, and dominance. First, the arousal dimension alludes to the individuals' level of affective or physical arousal. Second, the valence dimension measures the extent to which the felt affect can be classified as negative or positive. Finally, the dominance dimension relates to the degree to which the individuals feel either in control of or overwhelmed by a specific situation. The current study considers only the valence and arousal components of the SAM scale. This is because a high level of negative affect is correlated with a high degree of excitement and strong negative feelings, 52 and therefore, negative affect can be regarded as a combination of valence and arousal.
The scale measuring the cognitive component of patient confusion was developed by the authors using four items describing the accordant construct. Involvement was measured using the scale of Laurent and Kapferer. 54 Four items based on Sherer et al. 55 were used to measure general self-efficacy. The exact wording of the question items are in Appendix 3. Descriptive statistics on all reflective constructs are in Appendix 2.
Assessment of reliability and validity
Average variance extracted (numbers in bold), composite reliability, and squared inter-construct correlations. a

AVE and composite reliability cannot be calculated for formative measures.
Contrary to the remaining constructs, the SAM scale is a formative construct. The variance inflation factors of two items in the SAM scale are distinctly below 5.0; thus, an absence of collinearity can be assumed. Moreover, both SAM scale weights are significant (valence: weight = .718***, arousal: weight = −.362*). The higher the individual arousal and the more negative the affective reaction, the higher the latent variable scores of the formative construct are. Thus, higher values of the formative construct represent higher levels of negative affect.
Study results
Figure 3 depicts the path coefficients for the proposed model of patient confusion. The R2 of the cognitive component of patient confusion (R2 = .34; Q2 = .25), affective component (i.e. negative affect) of patient confusion (R2 = .20; Q2 = .16), and the behavioral intention (R2 = .32; Q2 = .26) demonstrate that the proposed model is suitable to explain patient confusion. All of the Q2 values exceed zero and the predictive relevance of the model can be assumed for all endogenous constructs.
Overview of study results. Note. PLS results (path coefficients) levels of significance are based on 5000 bootstrapping runs (sign changes: construct level changes). *p < .1, **p < .05, ***p < .01.
In addition to the significance of path coefficients (see Figure 3), the effect size f 2 and the relative predicted relevance q2 should exceed .02 for weak, .15 for moderate and .35 for strong effects. 24 In accordance with hypotheses H3a, H4a, and H5a, the results demonstrate that perceived similarity (f 2 = .03, q2 = .01), perceived ambiguity (f 2 = .03, q2 = .01) and information overload (f 2 = .18, q2 = .12) have a significant direct effect on the cognitive component of patient confusion. In line with hypothesis H5b, the affective response is only triggered by the perceived ambiguity of the patient (f 2 = .07, q2 = .05). There is no affective reaction based on perceived similarity or information overload (see Figure 3); therefore, H3b and H4b must be rejected. The results also confirm that the cognitive and affective (i.e. negative affect) components of patient confusion have an impact on behavioral intentions. Confirming hypotheses H1 and H2, the cognitive (f 2 = .05, q2 = .08) and affective (i.e. negative affect) (f 2 = .01, q2 = .01) components of patient confusion have a significant impact on the inclination to narrow down the choice set. The affective component of patient confusion (i.e. negative affect) decreases behavioral intentions to narrow down the choice set, whereas the cognitive component of patient confusion increases the individual's inclination to narrow down the set of alternatives. The study results indicate that the perception of self-efficacy and health involvement affect behavioral intention as well. Confirming hypothesis H7, the stronger the health involvement, the lower the willingness to narrow down the choice set (f 2 = .13, q2 = .13). In accordance with hypothesis H6, the inclination to narrow down the set of available decisions decreases with perceived self-efficacy (f 2 = .16, q2 = .10).
In addition to the partial least square (PLS) analysis, bootstrap-based mediation analyses were conducted. 56 The cognitive and affective (i.e. negative affect) components of patient confusion were considered as mediating variables. With respect to the affective component (i.e. negative affect) of patient confusion, our analysis reveals a significant indirect effect of perceived ambiguity (−.04, p < .10). Because perceived ambiguity has a significant direct effect on individuals' action tendencies, the accordant mediation should be classified as partial mediation. When the cognitive component of patient confusion is considered as a mediator, perceived similarity (.04, p < .10) as well as perceived information overload (.10, p < .01) have a significant indirect effect on patients' behavioral intentions. Due to the non-significance of both direct effects, the mediation can be classified as total mediation.
Conclusions
Summary of study results
Patients need information to retain their sovereignty and to decrease information asymmetries in the health sector. However, as the present study shows, this notion should not be accepted without further consideration. A simple increase in information may result in patient confusion. Patients can perceive health information as too similar and too ambiguous and thus feel confused. The quantity of health information may lead to cognitive confusion as well. In contrast, adverse affective reactions to health information are caused only by complex and ambiguous information. Cognitive and affective reactions to information, in turn, influence the decision-making process and may result in unfavorable behavioral consequences. These cognitive and affective (i.e. negative affect) components of confusion increase the inclination of patients to hastily narrow down their set of possible decision alternatives. However, perceived self-efficacy decreases individuals' tendencies to apply this strategy. People with high self-efficacy apparently trust their cognitive abilities and deal better with information-induced confusion. Health involvement decreases behavioral intentions to narrow down the choice set as well. Highly involved patients seemingly do not want to make a premature decision and reduce their choice set hastily.
Practical implications
The findings of our study have implications for public policymakers. They must reduce confusion by focusing on its antecedents, which will decrease the cognitive and affective (i.e. negative affect) components of patient confusion. A couple ways to reduce patient confusion might involve introducing labels indicating that a patient is dealing with reliable information or offering websites for lay people to provide a trusted and reliable source to simplify the information search, information processing and the decision-making process. Our findings support Scammon et al., 1 who conclude that health policymakers should guarantee that the right information is accessible to the patient in the right way to simplify the decision-making process. Health policymakers could intervene with public health campaigns to reduce perceived information overload, similarity, and ambiguity. They could introduce unambiguous and understandable quality indicators and ensure that patients are not using the “narrowing down the choice set” strategy to cope with their confusion.
Furthermore, health policymakers must increase health involvement. Patients must be aware that patient sovereignty implies responsibility, and decisions about health issues have to be made carefully. Increased health involvement would decrease the inclination to narrow down the choice set. Moreover, self-efficacy could play a critical role in coping with patient confusion. People with high self-efficacy perceptions are less inclined to narrow down the choice set as a confusion-reduction strategy, and policymakers should find ways to increase self-efficacy. To increase health involvement as well as self-efficacy, policymakers could implement interventions, including health education courses, to improve patients' knowledge regarding how to decide among different service providers and increase their sense of the importance of health issues (e.g. Greenfield et al. 57 ). Within this context, it is important to understand that actual and preferred involvement may vary across different groups of patients and, as a result, interventions have to be matched with individual preferences. 58 Moreover, previous research revealed that the use of trained educators and the involvement of significant others represent important features of successful self-efficacy-enhancing interventions. 59 Consequently, mediators such as health coaches or primary care gatekeepers (i.e. primary physicians) should be an integral part of the design and accomplishment of these health-education intervention strategies.
Limitations and avenues for future research
Any interpretation of our study results must include limitations. First, the scenario was fictional and patients may act differently in real life situations. Second, the study focuses on online information and omits more traditional sources such as physicians. The inclusion of other information sources could have an impact on perceived confusion and coping strategies. Third, only behavioral intentions were evaluated, not actual behavior; however, a strong positive correlation between real behavior and behavioral intentions exists. Fourth, only one coping strategy was used to test behavioral consequences. The use of different coping strategies should confirm the impact of the cognitive and affective (i.e. negative affect) components of patient confusion on patient behavior. Fifth, a path-modeling approach was used to assess the delineated patient confusion framework. Hence, no causal research design (i.e. experimental design) was applied, and therefore, it is not clear that the estimated path coefficients truly reflect the causal relationships proposed.
The results and limitations of this study offer potential avenues for future research. To improve the explanation of confusion, additional moderating, or mediating constructs, as discussed by Mitchell et al., 15 could be considered. Examples of additional variables are the experience of the patient with health information and recommendations from and trustworthiness of various sources. These factors can impact the choice of a health service provider. 3 Additionally, specific emotions, such as anger or despair, could be measured instead of negative affect to represent the affective component of patient confusion. The assessment of other confusion-coping strategies would be useful to further understand behavioral consequences of confusion. For a health service provider, it would be important to know whether patient confusion leads to negative word of mouth or consultations with third parties.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.