
Abstract
The paper examines the financial and non-financial performance effects of the third sector involvement in public research hospitals. By relying on multiple data sources, the study compares the performance of an Italian public research hospital before and after the establishment of a partnership with a charity institution. The results reveal that the involvement of the charity is beneficial for both care and research activities, thus supporting the research hospital in achieving its twofold mission. Beside the advancement of the literature, the paper offers a successful example of collaboration between public and not-for-profit organizations that can be replicated to improve public health.
Keywords
Introduction
Starting from the end of the 1970s, public sector reforms have led to a growing interest in public research hospitals (hereafter RHs) as organizations of the National Health Service (hereafter NHS) that are characterized by care and research institutional purposes. Their legal regime is different from both private research institutions and public general hospitals. Unlike the former, their public status reduces the autonomy in defining research priorities and funding allocation. Different from the latter, their institutional purpose is related to both delivering hospital care and carrying out research activities.1,2
Similar to teaching hospitals, the achievement of this twofold mission makes RHs complex settings. 3 In this sense, the recent challenges of public healthcare sector can undermine the RH functioning. On the one hand, the evolution of patient requirements, the technological sophistication, and the improvement of service outcomes increase the financial needs of public hospitals. On the other hand, the financial pressures on national budget hamper public hospitals in dealing with these multifaceted needs and often lead RHs to shift their financial resources from the research to the caring process. 4
In this perspective, the establishment of alternative institutional arrangements and modes of care delivery, such as collaborations with private organizations, can address the above cited challenges as they improve the efficiency and enhance the service quality of public entities.5,6
As part of the global movement towards the managerialization process of public services, literature on partnerships has focused on several aspects, such as the collaboration settlement, the institutional determinants of collaborations, the partners’ selection criteria, as well as costs and benefits for the caring process management. However, this literature suffers from two gaps. On the one side, research investigating the effects of collaborations has mainly focused on the efficiency of public–private partnerships (hereafter PPPs), neglecting other intangible performance dimensions (e.g. quality of internal processes and patient satisfaction).7,8 On the other side, prior research on PPPs has almost neglected the performance effects of collaborations between RHs and partners belonging to the third sector and involved in the care-giving process.
Taking together both the characteristics of the RHs and the existing gaps in the literature, our research question is the following: does the PPP with a charity affect the financial and non-financial performance of care and research activities of a RH?
To address this question, we rely on a qualitative methodology based on a longitudinal case study. This approach is especially useful in early stages of research, where prior evidence is lacking and existing theory seems inadequate.9–11 We focus on the illustrative case of collaboration between the haematology department of an Italian public RH and a charity institution which raises funds to finance the delivering of homecare services for patients treated at the hospital. This is an ideal setting to explore our research question as the ongoing spending review in the Italian public healthcare sector is promoting PPPs for outsourcing several services to not-for-profit organizations.
Our findings offer contributions for academics and practitioners. In particular, our paper extends previous literature on performance advantages of PPPs, by reporting that collaborations can be beneficial for public RHs in terms of care and research activities. Moreover, unlike prior research examining the role of private for-profit organizations in PPPs, our study investigates the performance implications of involving a not-for-profit partner. Finally, our research calls the attention of policy makers in promoting partnerships with not-for-profit organizations as an effective solution to address the lack of financial resources in the healthcare sector.
The remainder of the paper is organized as follows: Section “PPP in healthcare” reviews the literature. Section “Methodology” describes the research method. Section “The study setting” sets the context of the study. Section “The case study” analyzes and discusses the case study. The last section concludes by providing theoretical and practical implications as well as directions for future research.
PPP in healthcare
A growing number of studies has explored the use of PPPs in healthcare following different approaches (i.e. policy, governance, local regeneration, infrastructure and development). Our paper adopts the governance interpretation as the natural extension of the New Public Management. According to this approach, unlike hierarchies, PPPs are governance tools to effectively manage the cooperation between public institutions and private organizations for service provisions. The governance perspective is very inclusive and incorporates a variety of forms of private involvement in the delivery of public goods and services. 12 Building on this approach, the literature review shows two main streams of research. 5
The former has explored the contribution provided by the public institution as regulator, standard setter and quality monitor.13–15 In particular, scholars have pointed out how to set up the PPPs to provide users with adequate access to services.16–20 In this sense, they have recommended that public institutions should ensure a fair and transparent selection process of partners, avoiding that private profit goals overcome public interests.16,19
Differently, a second stream of research has examined the contribution of private partners for the management of the care process. Scholars in this field consider PPPs as innovative ways of providing health services since public organizations benefit from the efficiency of the private sector.20,21 In particular, this strand of literature has investigated the effects of PPPs on the overall financial performance of public partners, emphasizing two main advantages. 5 First, the involvement of private partners reduces the pressure on public budgets and allows better procurement and efficient allocation of financial resources. Second, the refined managerial expertise and the continuous innovation of the private sector lead to better service delivery at reduced costs.21–23
While these studies have pointed out the advantages of PPPs for financial performance, there are several reasons to believe that a partnership can also provide non-financial benefits to different kind of stakeholders. They may comprise, among the other, healthcare outcomes related to patients (e.g. living longer or enjoying better health) and their satisfaction. This phenomenon occurs when the private partner not only provides financial resources to the public but it is also directly in charge of service provision. This is especially true when the third sector is involved in the agreement. A related strand of literature on public education reports case study evidence on a number of non-financial benefits arising from academic partnership (e.g. improved quality of teaching and learning, better informed community practice, more frequent and higher quality publications).24–28 Additional investigation on this setting finds that collaborations with a charity organization provide mutual non-financial benefits to partners. 29 Taken together, this evidence suggests that the PPP model based on the involvement of a charity institution may be also beneficial for other public services, such as healthcare. Indeed, in this industry, complex organizations like RHs could take advantage of the agreement with a charity in terms of financial and non-financial outcomes. In this sense, a partnership with third sector may play a pivotal role in the achievement of the RH double mission of care and research. 3
Grounding on this stream of literature, we expect that the charity involvement in the PPP with a RH has beneficial implications for financial and non-financial hospital performance related to both the care and the research activities. Indeed, the charity involvement in the PPP may support the hospital in improving the quality of care provision and the innovativeness of research also in terms of publications.24–28
On the basis of these premises, we formulate the following proposition: P1: The involvement of a charity in the PPP with a public RH improves the RH performance in terms of care and research activities.
Methodology
Our methodology relies on a longitudinal case study.30–32 A single case study contributes to existing knowledge, since it deepens or widens the current understanding of the phenomenon under investigation. 33 This approach facilitates the use of in-depth longitudinal data, which is less feasible in multiple case-studies. It is especially useful in early stages of research where prior evidence is lacking and existing theory seems inadequate.9–11 We focus on the illustrative case of partnership between a haematology division of a monospecialist RH and a charity. We have chosen this case study because it represents an extreme situation and a polar type,30,34,11 as the charity activity is completely devoted to support the RH. Moreover, we have also chosen to focus on the Italian setting, where the ongoing spending review in the public health is promoting the PPPs for outsourcing several services to private for-profit and not-for-profit organizations.35,36 More specifically, contractual collaborations with charities are playing a pivotal role in delivering homecare services.
The case study was carried out in two simultaneous steps over the observation window 2008–2014. This enabled a closer examination of the hospital performance changes.
In the first step, through a number of performance indicators, we measured the financial and non-financial departmental outcomes related to both the care and the research activities. Data for developing the indicators were gathered from the documentation provided by the charity and the hospital.
In the second step, data were triangulated with information drawn from the direct interviews in order to enhance the research reliability and to assess how the actors perceived the performance implications of the partnership. In this sense, triangulation is one of the main advantages of combining both qualitative (i.e. data provided by the semi-structured interviews) and quantitative (i.e. data gathered from the documentation provided by both the charity and the RH) information.
Following prior studies,37,38 semi-structured interviews were conducted with three distinct groups: (a) charity managers; (b) departmental clinical staff at different organizational levels (i.e. clinical director, clinicians and nurses); (c) patients. The interviews were guided by questionnaires consisting of relevant questions reported in the literature for the PMS analysis. The interviewees were randomly selected among the whole population of managers, clinicians, and patients of the department during the observation period. A total number of 66 interviews were held at the study site. To improve the clarity of data, and limit misunderstandings in interpreting responses, the researchers adopted several tactics. First, a brief introductory presentation of the research was made to the interviewees. Second, it was asked permission to rephrase the answers within the researchers’ words. The interviews were digitally recorded and then transcribed for analysis soon after the event. Where necessary, researchers made a second visit to confirm the information or to follow-up on something which had arisen in another interview. Once all the interviews were completed, the members of the research team discussed the main issues emerged during the dialogues so as to start the analysis.
Figure 1 illustrates the details of the research design.
Research design.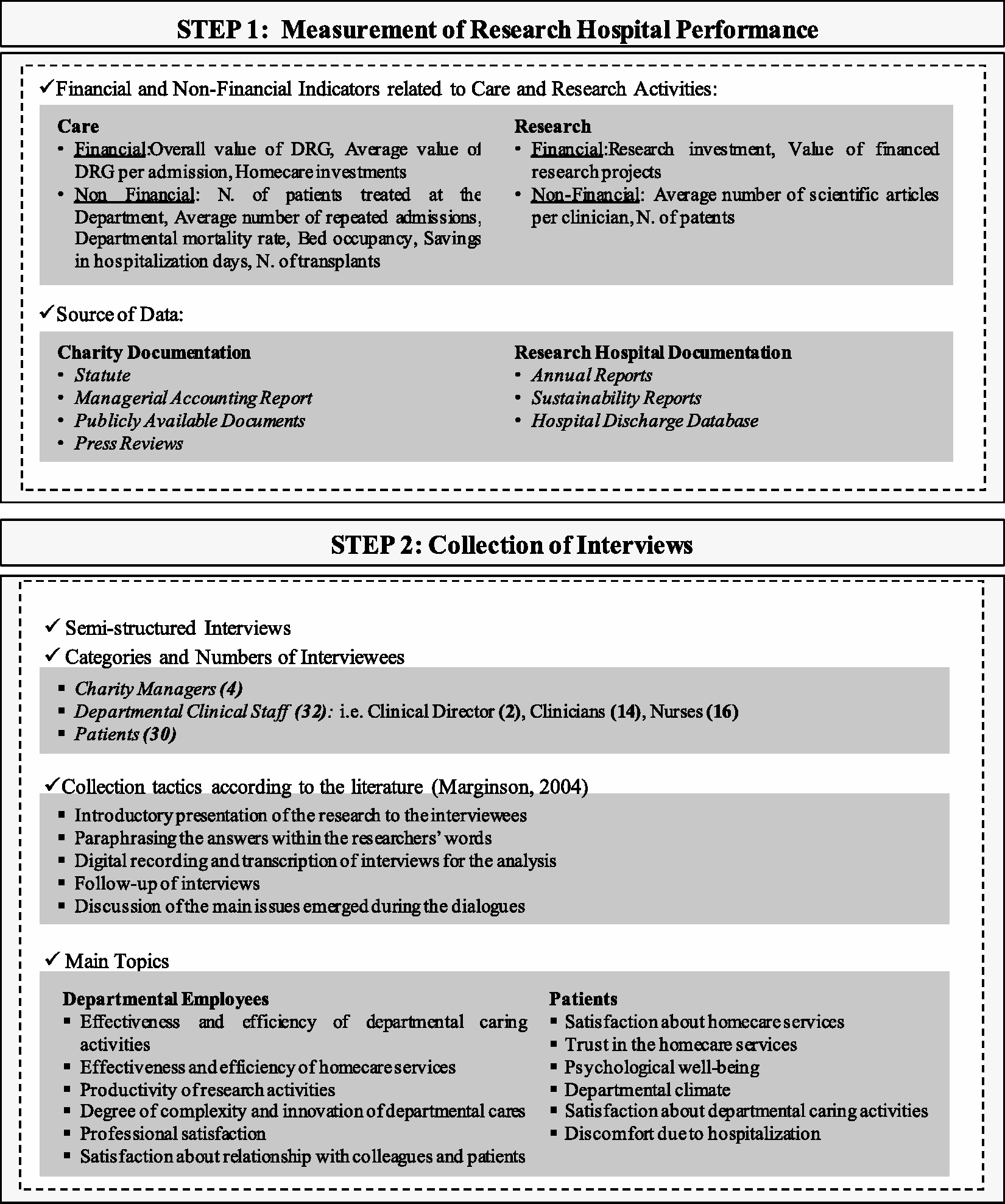
The study setting
In the Italian NHS, a vast array of public autonomous hospitals supplies cares. These entities can be general (Aziende ospedaliere), teaching (Aziende ospedaliero-universitarie) and RHs (Istituti di ricovero e cura a carattere speciale). Nowadays, 18 public RHs operate in Italy. They focus intensively on their research activity and offer limited but specialized cares to patients.3,39,40 On the one side, they provide an outstanding level of care, and on the other side they directly contribute to the research priorities of the NHS. 2 The co-presence of the double institutional aim makes RHs complex organizations 1 that can take advantages from more efficient organizational solutions like PPPs. 4
The growing use of these collaborations has been boosted by the recent reforms in the Italian healthcare sector aiming at renewing public administration (e.g. Merloni Law in 1998). Among the different forms of PPPs, contractual collaborations often aim to outsource to private companies and not-for-profit organizations the provision of healthcare services in terms of rehabilitation, laboratory diagnostics and homecare services.35,36,41
The collaboration under scrutiny involves two partners: the haematology department of a monospecialist RH and a charity.
The department is one of the centres of excellence in Italy in providing cares for haematology–oncological disorders. It presents 12 beds for ordinary hospitalization, 6 beds for transplants, a day-hospital facility, a specialist laboratory and an ambulatory for both the follow-up of discharged patients and those under experimental treatments.
The charity is an institution that raises funds to finance the delivering of homecare services for the patients affected by haematology–oncological disorders. It presents a well-framed governance model. Founders are supervised by independent auditors and cooperate with a scientific committee characterized by clinical expertise. The main channels of financing are donations, charity gala dinner and jumble sales.
In 2009, the charity signed a contractual agreement to support the haematology department by providing homecare services to its patients. Since the settlement, the homecare program is including blood transfusion and side-effect treatment, all delivered by the clinical staff employed at the hospital. Aside the homecare activity, a range of services to support the haematology department, the patients and their families is provided (e.g. infrastructure empowerment, scientific equipments and medicines). Moreover, a psychological service was founded to the benefit of both patients and their families.
The case study
This section presents the case study by discussing the hospital performance in terms of care and research before and after the settlement of the partnership with the charity.
Before the PPP
Before 2009, the haematology department was affected by several problems that undermined the research and care performance.
For what concerns the outcomes of the care activities, the performance indicators revealed an overall value of diagnostic-related groups (DRGs) equals to 4,549,103.64 €, corresponding to an average value for admission of 6425.29 €. An interview to the clinical director revealed that these values were due to the treatments of cares that make use of the division resources, even if they presented low complexity and were refunded at low DRG tariffs. Indeed, the clinical director pointed out that beds were very often occupied for caring activities with low complexity, such as the treatment of blood transfusions, side-effects of toxicity diseases and terminal illnesses that were financed by the NHS at low tariffs even if they required resources in terms of bed occupancy.
In this respect, additional information on care activities came from non-financial indicators. In particular, we report that the number of patients treated at the department was equal to 221, the average number of transplants was 31.5 and the average number of repeated admission was 3.20. In addition, the bed occupancy was equal to 78%. In this respect, the clinical director declared that the frequent repeated admissions occupied the beds to treat diseases with low DRGs, limiting the admissions for new diagnosis and the opportunity to provide more complex and innovative cares such as transplants. Moreover, a nurse added: “The treatment of not complex diseases could be more comfortable when provided at the patient home than at the department”. An overall dissatisfaction emerged from the patient interviews as they were obliged to be hospitalized for caring not significantly serious pathologies. Indeed, a patient declared: “During the last months, I was hospitalized twice for ten days just for blood transfusions”.
Another relevant issue was due to the high presence of terminally ill patients as the mortality rate was 4.14%. In this respect, having terminally ill patients at the department negatively affected the departmental mood and increased the other patients’ discomfort due to the illness.
It is worth noting that the haematology department relied on the public homecare service provided by the local health authorities. Nevertheless, the clinical director declared its ineffectiveness: “Despite the National Health Service provides homecare services, there are a number of bureaucratic issues that the department has to solve in order to start it. As a result, too much time passes before the patient is cared at home. When we attempted to initiate the public homecare service, very often the terminally ill patients passed away before completing the process.” As for the research activities, we find that research investments were 19,870.56 € and the value of the financed projects 856,000 €. Finally, while the average number of scientific articles per clinician was five, the number of patents reached seven. In this respect, the clinical director added that, despite the research mission of the department, doctors were strongly committed on caring activities and did not spend enough time on researching. Moreover, doctors involved in research activities were concerned about the scant opportunities to explore and test the effects of complex diseases as a doctor declared: “Unfortunately, I spend about 90% of my working time in treating neutropaenia. Therefore, I have limited occasions to treat more complex diseases that can inspire my research activity”.
After the PPP
Since 2009, the haematology department has settled a relationship with the charity under the convention ruled by the Framework Law on Volunteering (clause 7, law n. 266/1991).
Our analysis shows that the settlement of the partnership with the charity has produced a number of financial and non-financial performance benefits related to both care and research activities.
As for the care, we report that the homecare services investments are 92,900 €. In this respect, we find an increase of both the overall DRG tariffs and their value relative to the number of admissions. In particular, the value of the DRGs has increased by 49.08% (from 4,549,103.64 € to € 6,781,963.14 €). As a result, the average value of the DRGs tariffs for admission has increased by 45.19% (from 6425.29 € to 9328.70 €). In this respect, the clinical director emphasized a recombination effect of the DRG mix. In fact, on the one hand, the treatments of side effects of toxicity diseases and terminal illnesses are provided at home. On the other hand, they are replaced with treatments refunded at higher tariffs.
The examination of non-financial performance indicators shows that the delivering of some services at the patient home by the charity on the one side, has allowed a saving of 366 days of hospitalization for patients treated at home. On the other side, it has provided the department with the availability of 366 days of hospitalization for caring new patients. In this respect, we find that the number of patients treated at the haematology department has grown by 41.63% (from 221 to 313), while the average number of repeated admissions at the department has reduced by 27.50%. Moreover, the bed occupancy has increased by 16.67%, and the average number of transplants has reached 72.5. The interviews to the clinical staff confirm this evidence. Indeed, the clinical director declared: “Through the charity, we have the opportunity to treat the neutronpaenia at home instead of occupying the sterile area. This guarantees the availability of beds for transplants and we can also increase the admissions for new diagnosis.” A nurse added: “Older patients, that are more likely to be affected by side effects, are now treated at home. So we have more opportunities to care younger patients at the department.” For what concerns the patients treated at home, their stay also benefited from the reduced discomfort of the repeated hospitalization. In this regard, a patient said: “I am very satisfied with the homecare service as I feel surrounded by my family”. Another patient observed: “I’m happy to be treated at home by the clinicians of the department in which I trust because they already know the story of my illness.” In fact, it is worth noting that the homecare services funded by the charity are delivered by the same clinical staff employed at the department, and this feature also guarantees the continuity of cares. Indeed, the medical director noticed: “When we discharge patients, we feel more confident and safe as we know that we can trust in the homecare services.”
From a different perspective, the homecare service has decreased the departmental mortality rate (−71.01%) providing benefits to the patient stay in terms of better departmental mood. In fact, as a clinician declared, the treatment of terminally ills at home significantly improves the psychological well-being of all other hospitalized patients.
Concerning the research activities, we report that, thanks to the partnership, the research investments reach 23,435.49 €, while the value of the financed projects amounts to 1,263,000 €. Differently, as for non-financial indicators, partnership has improved the average number of scientific articles per clinician (+60%) and the number of patents (+28.6%). Indeed, the clinical director observed that, thanks to the charity investments in research, the scientific productivity of departmental researchers has increased, and the number of scientific publications in national and international journals has risen. A doctor also added: “The opportunity to treat more complex diseases, such as transplants, allows me to explore more challenging research issues.”
Figure 2 summarizes the performance changes occurred after the settlement of the partnership with the charity.
Case results.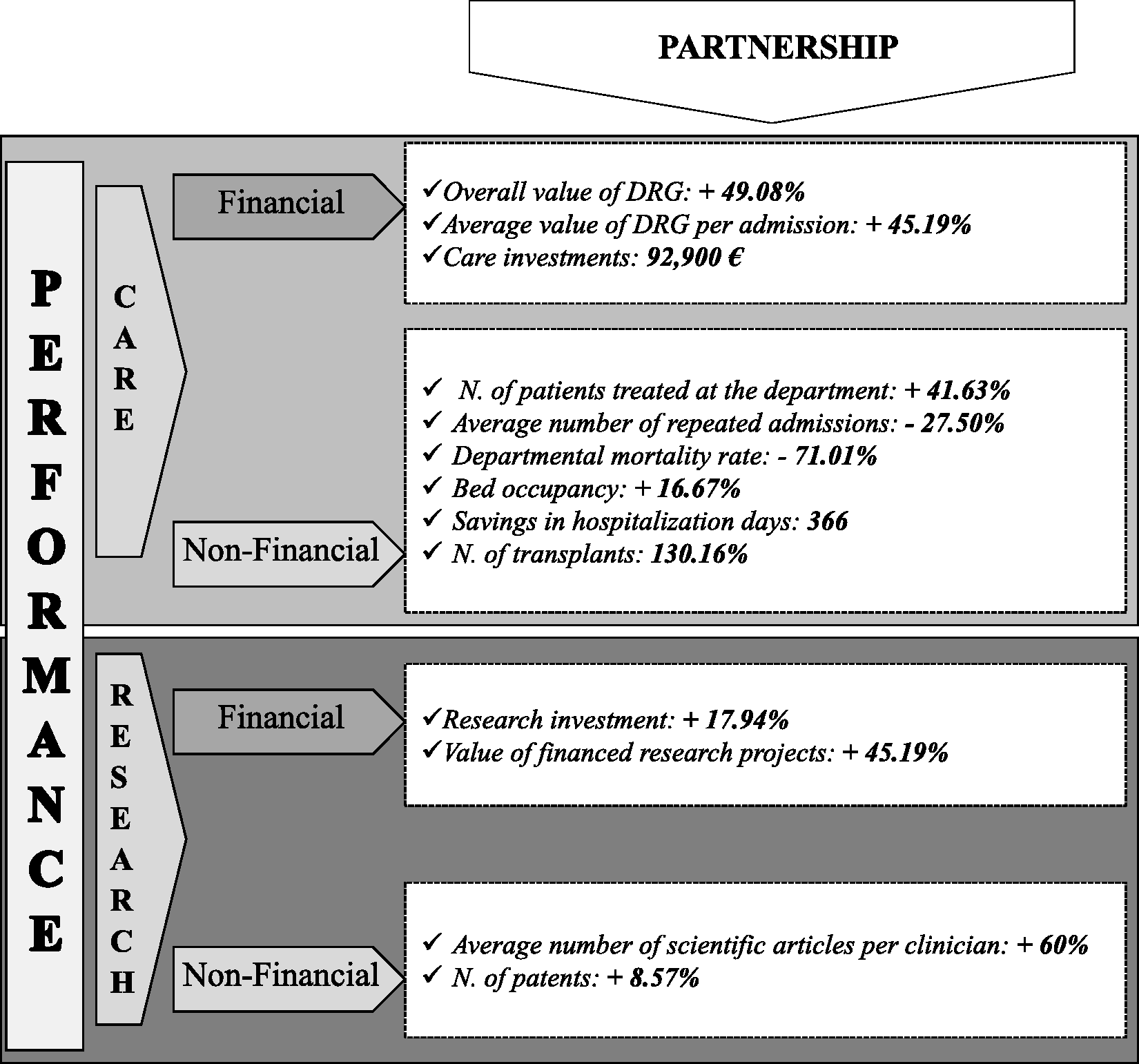
Conclusions
In this paper we aim to examine the performance implications in terms of care and research activities of a partnership between a charity and a haematology department of a public RH.
Relying on multiple data sources, we compare the financial and non-financial performance of RH before and after the settlement of the PPP. Our study shows that the collaboration can be a healthy option for the RH in the achievement of its twofold mission. In this sense, the charity supports the RH in providing an outstanding level of cares and in contributing to the research priorities of the NHS. In addition, it fosters innovative research able to deal with the need of sophisticated cares.
Our paper offers contributions for both academics and practitioners. In particular, it extends previous literature on the advantages of PPPs for the performance by providing empirical evidence that collaborations can be beneficial for public RHs.5,22,23,42–44 Differently from the studies investigating the efficiency of PPPs, our article shows that these collaborations have financial and non-financial performance implications for both care and research activities. Thereby, it addresses the research gap related with the examination of non-financial aspects of performance. Moreover, to the best of our knowledge, this article is one of the first studies that analyzes the case of an Italian PPP in healthcare where the private partner is a charity organization and it is also directly in charge of public service provision. Thereby, filling a gap in the literature, we complement the empirical studies on academic collaborations by examining a PPP model based on the involvement of a charity institution in the care-giving process. Finally, from a practical standpoint, the paper offers to policy makers a successful example of PPPs with a charity that can be replicated in settings experiencing spending review in public health.
Notwithstanding this contribution, the paper presents some limitations. Indeed, the responses to our questionnaires and interviews could suffer from the social desirability bias. 45 In addition, our paper lacks of a systematization of the different aspects of hospital performance. Therefore, future research efforts should be directed towards the employment of a multidimensional performance measurement system in order to advance the knowledge on the topic. In addition, we encourage scholars to adopt multiple case study approach to appreciate how different kind of partners affects the outcomes of partnerships with RHs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.