
Abstract
Recently, most reforms affecting healthcare systems have focused on improving the quality of care and containing costs. This has led many scholars to advocate the adoption of Health Information systems, especially electronic medical records, by highlighting their potential benefits. This study is based on a comparative analysis using a multiple method approach to examine the implementation of the same electronic medical record system at two different hospitals. Its findings offer insights into the processes of the adoption of innovation and its implementation in a healthcare context. The need to innovate, the decision to innovate, the implementation process and consequently, the results produced are quite distinctive at each study site. This comparative case study reveals that what appears to be the same can be quite different: this can be due to several conditions at the organization, the organization’s characteristics, and the process of implementation adopted. We need to understand these elements in order to be able to plan and manage such programs in the future.
Introduction
Information and communication technology (ICT) has led to improvements in efficiency and quality in many sectors of the economy and has made a considerable contribution to the modernization of public administration at all levels.1,2 This is also true in the case of health care, where technologies are helping to transform the sector with the introduction of new systems. Some studies on the adoption and the impact of technology on service delivery by public organizations3,4 have shown that the effective adoption of ICT has changed over the years as technology has evolved, and its incidence among organizations has grown and become more pervasive. 1
However, healthcare professionals and organizations have found that they do not always have adequate systems for delivering strategic change. To remain competitive, healthcare professionals and organizations are looking to information technology for help. The adoption and implementation of ICT in the healthcare sector is developing much more slowly compared to other sectors, such as finance and commerce. 5 This is due to several impediments 6 such as the continuing lack of awareness among patients of the availability of online access to specific information or the legal issues implicated by the use of electronic forms of communication in medicine. In practical terms, although there are already some ICT systems in place in the healthcare sector for the execution of administrative tasks, such as billing, scheduling and inventory management, there is scant adoption of extensive integrated clinical information systems.
Nevertheless, electronic systems for managing information about patients and care processes have the potential to enhance the quality, efficiency, and safety of healthcare delivery 7 even if technology alone is insufficient to safeguard the achievement of these benefits. Furthermore, it is essential to understand the human and organizational processes with which it interacts if efforts to implement these systems are to be optimized.
The research described in this article contributes to our understanding of how the process of adopting and implementing the same electronic health record system happens at different hospitals and the types of effects it can produce. It also reveals the importance of service planners and managers, developing a clear understanding of the mechanisms through which electronic medical records (EMR) are likely to effect change in order to engage in a meaningful evaluation of impact or cost-effectiveness. While the effects of technological innovation on organizational performance have been studied in many sectors of the economy, there is a shortage of evidence as to the impacts of EMRs in the healthcare sector.8,9 Recent analyses of existing research in this area conclude that human and organizational factors are as important, if not more so, for predicting the success of technology programs as the technologies themselves and, therefore, more research is needed in order to understand these factors. 10 This study addresses this gap in our knowledge.
The article is organized as follows: the section below discusses literature on innovation processes in the healthcare sector and presents the theoretical framework; the research method section describes the study setting and features of the EMR system adopted at the two hospitals, and considers the methods used for the empirical analysis. The results section presents the main findings of the study organized according to the main phases in the innovation lifecycle. The last section highlights the main conclusions of the study and closes with recommendations to take into consideration when adopting and implementing complex innovation systems.
The innovation process in a healthcare setting
The introduction of EMRs is potentially one of the main innovations capable of securing the clinical process and of facilitating improvements in healthcare performance and service delivery. The main goal of the EMR system is to ensure continuity of care, even if performed by different practitioners, at different times and locations. Implementing a clinical information system of this type can promote the alignment of administrative processes and clinical information. Both case studies included in this work aim at achieving the highest level of integration, although they had reached different levels of integration at the time of our data collection.
The emergence of this scenario, where clinical information is considered a strategic variable in managing daily care activities, has focused attention on theoretical models described in literature 11 leading to the practical study and design 12 of clinical information systems and their actual implementation. However, there has been little investment in the field of clinical information systems in recent years due to numerous issues, including institutional or organizational constraints, such as the lack of a corporate information system, failure to involve management, and scant opportunities to invest in IT projects. 13
Many studies have analyzed the adoption of technological innovations in health care and suggest factors focusing on the methods of adoption and implementation, and discuss the extent of any impacts. Some studies discuss the dimension of business impacts following the adoption of electronic medical records but there are few studies that have measured the actual occurrence of outcomes of such systems or that have examined the role of professionals in the implementation and evaluation processes, as this study does.
Furthermore, many studies have demonstrated that there are several potential benefits enrooted in EMR adoption.14–17 These effects are particularly important since ICT should promote integration and data sharing among different healthcare organizations. However, there is still limited evidence of the extensive adoption of IT systems in health care in most countries. According to some studies, technological immaturity, “unfriendliness” and human resistance are some of the barriers preventing adoption. Despite these, changes in government policies and increased support for the implementation of IT systems in health care suggest that successful implementation may be feasible in the near future.
Several studies reveal that an innovation process18—or a set of innovation activities19—does not resemble a simple linear model. The use of linear model is very often dominant in the more normative and prescriptive innovation models.20,21 However, it has been found that innovation processes are a rather messy and complex progress of events pointing in all directions and making use of all kinds of feedback from different stakeholders, 22 leading to the use of more sophisticated ideas. However, some patterns of similarity can be observed in the progress of these events18,19,23–25 and several studies 25 have found that there are also many powerful stakeholder groups within healthcare organizations and each of these can influence the ultimate success or failure of an overall innovation process.
One way to allow for a broader view of the innovation process could be to look at the innovation lifecycle as presented in the literature.20,23,26 This model could build on existing initiatives and expand the overview of innovations to include the main stages of an innovation lifecycle.
The framework
The innovation lifecycle.
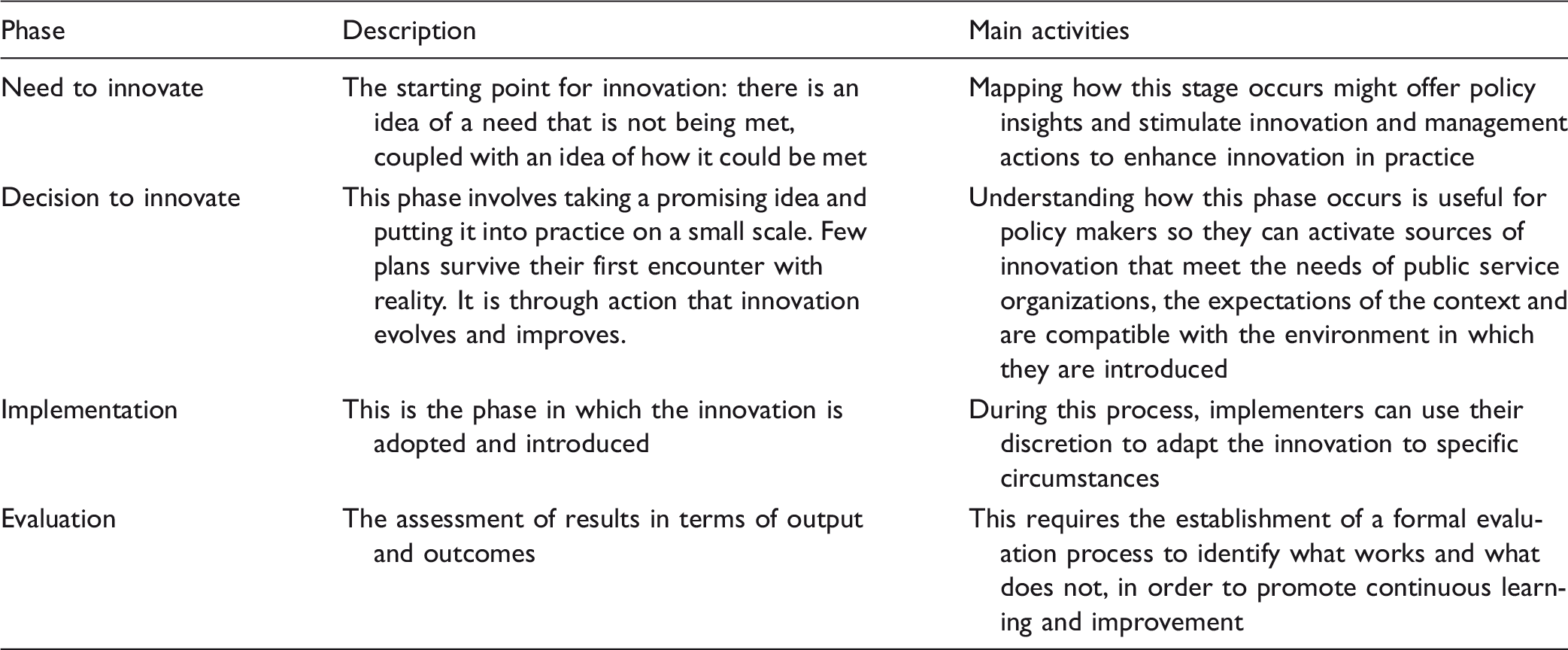
The first phase of this model focuses on the “need to innovate.” It represents the starting point for innovation: there is an idea that a need is not being met, coupled with an idea of how it could be met. Mapping how this stage occurs might offer policy insights and help stimulate innovation and management actions to enhance innovation in practice. The idea that scientific knowledge plays a dominant role in this gestation period should be put into perspective. Other sources of innovation seem to be more important, like the needs of customers.
The decision to innovate represents a second step. It can be seen as “incubating and prototyping.” 27 This describes the ways to promote the rapid and effective diffusion of innovation. It also refers to the “decision” itself 23 in which the agent tests the innovation. This phase involves taking a promising idea and putting it into practice on a small scale. Few plans survive their first encounter with reality. It is through action that innovation evolves and improves.
Understanding how this phase occurs is useful to policy makers so that they can activate sources of innovation that meet the needs of public service organizations, the expectations of the context, and are compatible with the environment in which they are introduced. It also contributes to management decisions on key performance areas allowing them to monitor, enable, enact, and evaluate the risks. The “people side” of innovations should not be forgotten: most tend to be involved on a part-time basis, have high turnover rates and experience euphoria in the beginning of the innovation process, frustration and pain in the middle, and closure at the end.
The implementation phase is when the innovation is adopted and introduced. This includes “replicating and scaling up,” referring to ways to promote the rapid and effective diffusion of innovation at a public service organization. The implementation of an innovation occurs throughout the development period by linking and integrating the “new” with the “old” or by reinventing the innovation to fit the local situation. 23 The role of the implementers of the innovation is often forgotten. During this process, implementers can use their discretion to adapt the innovation to specific circumstances. 28
The last phase of the innovation lifecycle is the evaluation phase, consisting of analyzing and learning from the innovation process. It requires the establishment of a formal evaluation process in order to identify what works and what does not, and so promote continuous learning and improvement. It consists of assessing results in terms of output and outcomes. However, it takes this a step further by integrating the innovation into the ongoing routine, and promoting it to others. 23
In order to analyze the impact produced by the EMR system at the two organizations, we referred to a specific model for the evaluation phase 16 that identifies the main impact dimensions: efficiency, organizational effectiveness, and clinical governance. In particular, (i) efficiency includes measurements of the effects of EMRs in terms of the quality of information, time, and cost savings; (ii) effectiveness includes variables that identify the contribution of EMRs to process integration, risk management, and improvement of patient care processes such as diagnosis and therapeutic activities, and (iii) clinical governance comprises a group of effects produced on clinical activities in terms of clinical audits, accountability regarding the management of access and exchange of medical information, and in terms of professional development through education and communication efforts.
These phases strike a balance between a micro- and macro-assessment of innovation initiatives. In management science, much of the micro-level research in this area has tried to identify organizational factors influencing the adoption of technology 29 without considering the external environment. Other authors focus on the relationship between internal and external factors, arguing that “ICT systems are global networks that link organizations, customers and business partners around the world.” 30 In healthcare studies focusing on the adoption and evaluation of innovative technologies, it has become increasingly important to take many elements of the social world into account.31,32 For example, it is important to draw attention to the relevance of changes in work processes, communication, and worker status brought about by the introduction of technology.
Research method
Study settings
An overview of the characteristics of the cases analyzed.
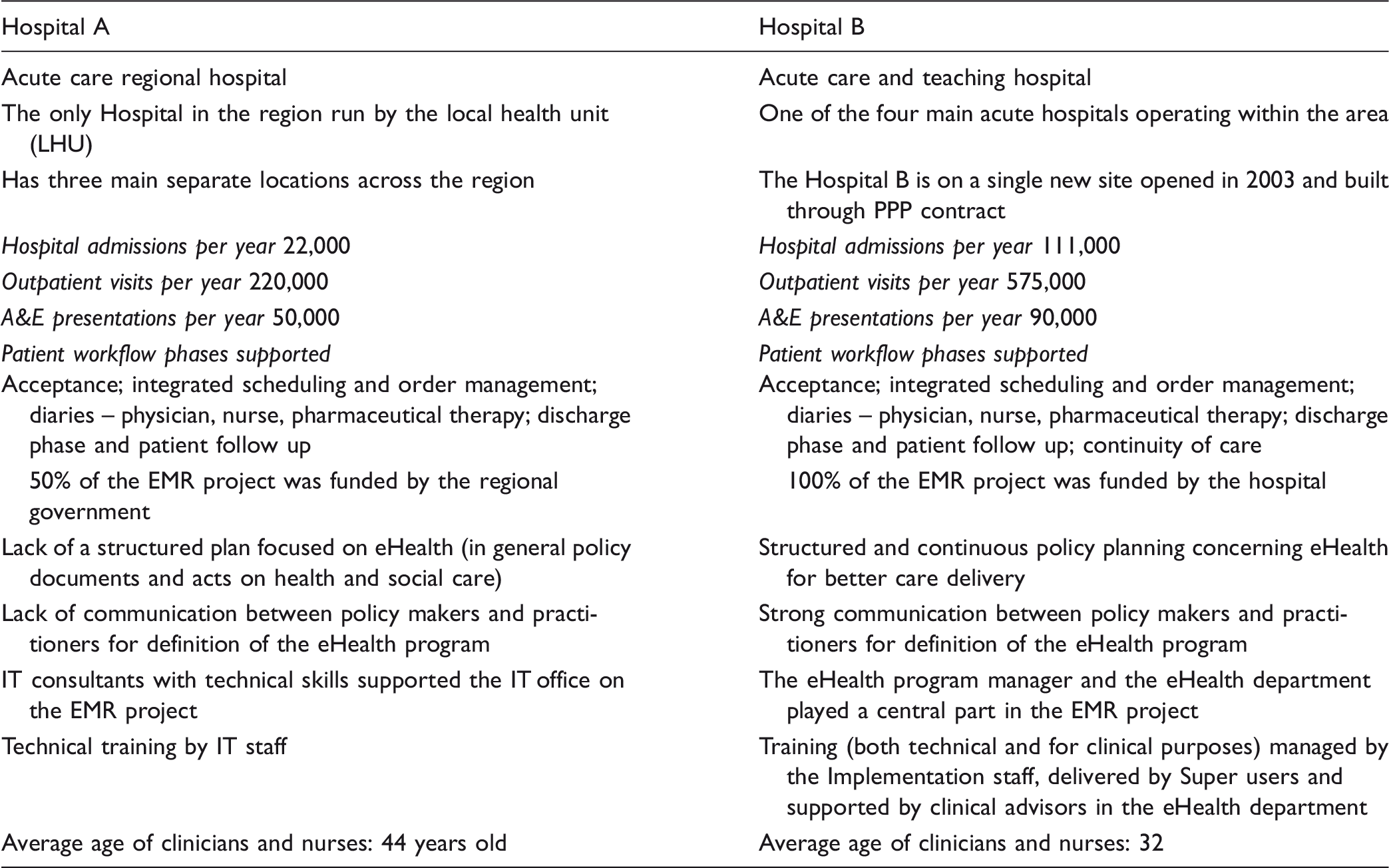
The two cases analyzed revealed some differences with regard to the hospital context, including both the hospital’s structure, culture and its way of working within a service organization:
Data collection
The research described in this article reveals how sociological and technological factors interacted during the process for the adoption and implementation of an EMR system at two different hospitals. In order to do this, the article deploys a multi-method approach to data collection in the two case study sites, offering a distinctive mode of analysis which reveals crucial factors shaping the two cases. Many studies have demonstrated that the development of information systems is also affected by the organization’s characteristics, including “soft aspects” such as social, cultural, and individual factors. As a result, great importance has been delegated to the meaning of the context as it is considered to be socially constructed by people in their environment. For this reason, several qualitative strategies were used for data collection: documentary analysis in order to identify the reasons for the adoption of the EMR system and its role, interviews, and observations.
We analyzed the main documents produced by the hospital, such as organizational documents and reports, and documents related to the EMR adoption.
The interview process initially involved approaching the eHealth/IT Director at both study sites, as the main local contact and subsequently recruiting additional participants at the hospitals through snowball sampling, including healthcare professionals (nurses, doctors), implementation team members (e.g., managers, clinical heads), and administrative staff. The initial respondents were used as informants to identify others who matched our previously defined characteristics: staff profile and number of years working for the organization (since the adoption of the EMR system at least).
Interview data was obtained from 32 participants at the case study sites and the implementation team members we interviewed included a mixture of clinical IT heads, IT managers, and training professionals. Users included a mixture of ward managers, consultants, nurses, administrative staff, pharmacists, and junior doctors. Sixteen interviews were conducted at site A (with six different types of participants), and 16 interviews at site B (with six different types of participants).
Furthermore, we also observed interaction between participants and within wards. This process entailed observing the interaction between the EMR system and clinicians, nurses and other staff, and between these and patients.
The use of observation is basically supplementary and aims to augment data resulting from interviews and documentary materials. The observation process started from the general observation of the hospital environment and then entailed observing any interaction between clinicians, nurses and other staff, and subsequently between these and patients. This facilitated the observation of different situations in several departments since modern organization “takes place in multiple fragmented contexts.” 33
Observation as a method of inquiring is a valuable means of studying relationships among people, facts and the organizational context—both at micro and macro levels. 34
We obtained ethical approval for carrying out the study and the observations were overt to the medical, nursing and administrative staff and covert to the patient. In particular, the interview phase offered us the opportunity to create the necessary rapport with interviewees so as to facilitate both access and the observation process.
Results
The results of our analysis were organized according to the different phases of the innovation lifecycle analyzed above.
The two hospitals involved in the study had a different approach to the introduction of the EMR system.
Hospital A and B: the four phases of the lifecycle model.

At Hospital B, the main driver for adoption came from the clinical staff, not the business staff, and the preferred system was chosen from two potential systems during a workshop attended by clinical staff. The eHealth Director was a key actor in the overall adoption and implementation process, and he maintained that if it wasn’t for the clinical staff, they would not have the system. The decision to innovate was characterized by “consensus” on the need for the introduction of the system and on the system selected.
A clinical advisor working for the eHealth Department and in charge of supporting and supervising the Maternity unit, said that the clinical staff wanted to have more information about their patients. At Hospital A, however, the Medical Director said that the General Director made the decision to adopt the system, starting with a pilot program in line with the region’s strategy for Innovation in Health care in 2006. One factor behind this was funding: the Regional Government funded half of the total investment (as stated in the proposal document). This may be because this is the only hospital in the region, resulting in a strong relationship between the hospital’s Strategy Board and the Regional Government. This relationship is typical, unique, in the Italian healthcare context. All of the interviewees stated that there was no participation in the decision process at this initial stage.
At Hospital A, the decision to innovate was characterized by a “top down approach,” without promoting the participation of personnel in the process at the selection phase.
35
The opposite was true at Hospital B, as the hospital proceeded to select the system in an inclusive way. The project manager said that a number of systems were considered, but finally: We undertook the usual evaluation: supplier presentation, discussion, cost—benefits analysis. We had to produce a case study for submission to the Scottish Government. The preferred option was chosen halfway through a workshop we organized and I think we had about 60 people at that workshop. The majority were clinicians and all the clinical staff put their hand up for that system. (Hospital B, Interview with the Head of Clinicians)
Looking at the implementation process in greater detail, the clinicians at Hospital A only received external support from an IT consulting company since they stated there were no courses on the strategic relevance of adopting integrated information systems. Furthermore, the nurses maintained that few events were held to introduce the new system and no technical courses were organized to support the implementation phase.
At Hospital B, some very interesting data concerning the implementation process emerged from the interviews with several actors in our sample. According to the information we collected, new roles were identified within the hospital in order to manage the implementation of the EMR system. At Hospital B, the implementation started in December 2005 (first go live) and the EMR system was implemented throughout the hospital by June 2008. One clinical advisor said: In that period we had an agreed implementation plan that said what we are implementing, when we are implementing it and how. For example, in December 2005, we were implementing hospital-wide functions at Hospital. (Hospital B, Interview with a Clinical advisor on the General Medicine Ward)
The system implementation was managed by the “Information System Implementation Team” and was overseen by a “Program Board,” that is, a group that initially met once a month and still meets on a monthly basis to oversee the implementation, formulate advice, verify if any help is needed, and provide it. Other key roles were identified during the implementation process and people were appointed to these new positions. Clinical advisors were identified for the implementation of the system in a specific ward. They worked on a specific ward but held different positions at the time of the adoption. This means positions were created to support the implementation of the system within units. No external people were taken on by the hospital to support the implementation process but people were recruited for the new positions who already knew the services provided by the hospital and by these specific wards. This included the clinical advisor—a new role created during the implementation phase after the EMR system was adopted. He or she has close links to the eHealth office.
Furthermore, a team of “Implementation staff” was set up to carry out the EMR system implementation. Initially, this support team was quite informal and the role of the new team, consisting of three people, was defined later according to the Clinical Advisor in charge of coordinating the Implementation Staff. The implementation staff members are employees working in the eHealth Department who have an operational management job. They work full time and report both functionally and hierarchically to the eHealth Director. Furthermore, a “Key Users Group” was identified at each hospital site: about 200 people (both medical and nursing staff) with a particular interest in the EMR system and its strategic development were involved in several meetings. We were looking for people who were interested in the EMR system, and wanted to ask questions and find out new things about it; every second month, they have meetings, they come along, and we tell them new things that are happening, and they bring issues they have got, to get it right and we find out how to solve the problems they encountered. (Hospital B: interview with the Clinical Advisor in charge of coordinating the Implementation Staff)
The impact of their work is essential, especially for the wards where they work. As mentioned by the interviewee, the number of key users is significant, and their role is extremely relevant for obtaining information about what happens on the wards in terms of the use and acceptance of the system, and any problems encountered during the implementation process.
The Implementation Staff does not only use this type of meeting to keep in touch with clinical staff. We went round, we asked what the regular routine was, and we identified some issues to debate for each site … . Then we went around the departments to find out people’s feelings, and help with the system. And so we did that, until they got to know it … . (Hospital B, Interview with the Clinical Advisor in charge of coordinating the Implementation Staff)
The role of “Super User” was also defined: in each ward, people were identified capable of training other people. These people work on the ward and are very motivated so they act as “local facilitators” for each department, supporting staff and training new staff. They are a communication tool, first by putting out any information to the Support Staff and then doing the same in reverse order, giving out information about function updates and answering any questions.
The Implementation group set up a skill-based system in collaboration with the eHealth Department to train the super users on training techniques. The Implementation Staff also checked their knowledge of the EMR system and issued a Super User certificate so they can operate on a specific ward. We have it all down on paper, with check boxes, until it’s electronic and then they’ve got jobs they can do with their staff and their departments, to make sure they’re competent. (Hospital B, Interview with the Clinical Advisor in charge of coordinating the Implementation Staff)
Super Users are very interested in the EMR system; they are often already conversant in ICT so their experience is a sort of “knowledge tool,” meaning they have developed good skills in the past by attending training programs held by the Implementation Staff. They offer themselves as volunteer “Super Users” for their ward.
It may happen that a unit manager identifies who can be a Super User, however according to the Chief of the “Implementation Staff”: Ideally, we’d like people to volunteer to do it … . (Hospital B, Interview with the Chief of the Implementation staff)
However, not all people reacted as enthusiastically as the Super Users. Based on what the staff said during the interviews, and according to eHealth Department advisors, many people were skeptical because they were asked to do something that they didn’t do before. It’s like any change, people automatically say, oh … They’ve got a fear of change. For the majority of them, when they realized all they had to do was a few clicks on a screen, then, most of them thought well, is that it? Okay, we can do that. Another set of people was more unsympathetic to using the system and it took us a long time to convince some of them what they were doing, the way they were working with paper records was actually taking longer. And if they would just don’t do that, they have just to click on the screen, that’s a lot quicker!! (Hospital B, Interview with the eHealth Department member) We were greatly criticized for training, they felt training was, was very poor. (Hospital B, Interview with the eHealth Department member)
As regards the evaluation phase, we referred to the model described in the framework section that identifies the main impact dimensions: efficiency, organizational effectiveness, and clinical governance, in order to analyze the impact produced by the EMR system within the two organizations.
Impacts on efficiency
The Medical Director at Hospital A found that efficiency gains were the main impact. “The system produced better efficiency within each ward.” However, she added that there were no clear results regarding these improvements. ‘This benefit of ward efficiency was not widely perceived as a benefit’ she said. This may be due to the fact that the hospital management did not opt to monitor these types of impacts at organizational level and did not use an evaluation model based on certain indicators and variables, starting monitoring prior to adoption, during the implementation process, and continuing after the adoption of the EMR system. The majority of clinicians agreed that the adoption of EMRs helps save time, for instance, by reducing the waiting time for lab test results and enabling diagnostic images to be viewed in real time.
At Hospital B, as regards saving time, the respondents (clinicians and nurses) stated that they take it for granted that EMRs produce information in real time: one of most highly acknowledged benefits resulting from the adoption of the EMR system at Hospital B is related to the perception that EMRs are fast, which helps to save time. The majority of clinicians we interviewed upheld that the adoption of EMR reduces the waiting time for laboratory test results and enables diagnostic images to be viewed in real time, saving them time during their daily work schedule. The respondents also confirmed that the adoption of EMRs produces relevant results in terms of the accuracy, completeness, ease of understanding and reliability of information. A receptionist on the A&E ward, one of busiest in the hospital, also said: In this ward we admit more than 100 persons a day and … I’ve been working here for 8 years … I don’t think the most relevant effect produced by the system is time saving … . I think the main benefit is the accuracy of information. (Receptionist, Interview)
Impacts on effectiveness
At Hospital A, interviewees suggest that the main organizational impacts on people are mainly linked to risk management, due to the presence of alerts in the Italian case. This comprehensive medical information system not only provides the healthcare provider with alerts, but also information for reducing different types of errors and avoiding unnecessary, or redundant, invasive clinical tests. Interviewees found that the adoption of EMRs safeguarded the temporal continuity of the service and an effective response to the needs of clinician and nurses. Furthermore, it guaranteed access to the full patient history. However, some interviewees found that the system initially increased their daily workload.
At Hospital B, the interviewees on the different wards agreed that the most relevant effect on people working within the organization is at “communication level”, such as improvements in the interaction between clinicians and nurses on the same ward and between different units and hospital sites. Both nurses and clinicians recognize that the adoption of the EMR system helped provide all of the patient’s information relating to previous admissions and this facilitated interaction and communication between members of staff, as discussed below. It has definitely improved relationships between clinicians and nurses … in the sense that we can all access the same information without going around and asking for details, or results and information in general terms. (Head of Nurses, Interview)
Impacts on clinical governance
The most significant effect on clinical governance refers mainly to the potential offered by EMRs to clearly identify who is accessing, managing, and exchanging medical information about patients at all times. This also has a positive effect on the degree of accountability of clinical personnel, considered a fundamental component of high-quality healthcare organizations, which helps to improve patient confidence and trust in the services provided.
At Hospital B, we found some interesting results in terms of the effects on clinical auditing: clinicians revealed that EMRs helped them collect useful information for improving healthcare support services, leading to an enhanced perception of quality by patients when they are discharged from hospital.
Conclusions
As discussed above, this article investigates a specific medical system called electronic medical records. The study also examines two study settings that adopted the same EMR system, made by the same provider. This comparative study aims to analyze how EMR systems are adopted by different healthcare organizations by focusing on the antecedents of the EMR project, on the implementation processes used, and on the impacts produced.
Based on the study’s main results, we can conclude that this work builds on existing literature by providing interesting insights related to the research context and the specific focus of the adoption, implementation and evaluation of EMRs. There are few comprehensive studies about the value of hospital EMRs; to get a complete picture, one must identify, compare, and combine the results of numerous focused and country-based studies. Furthermore, many EMR studies lack a common basis for comparison, since they use different sources of data, research methods and metrics. Another contribution relates to how EMR systems influence the delivery of health care services and how these systems affect the organization and the operations of its main users and stakeholders. Previous studies36,37 have attempted to make a quantitative evaluation, whereas this study offers a more comprehensive insight into the role of people within hospitals, particularly in highlighting how people and systems interact. Furthermore, existing studies are based on single discussions of impacts. 35 In particular, the successful EMR implementation at Hospital B shows this can be largely attributed to the fact that the various stakeholders were involved in the implementation project as a shared endeavor, with the EMR like a nonhuman super actor: in this way the technology effectively became a core actor within a network of actors.
In this way, the comparative case study shows that what appears to be the same can be quite different. The evidence discussed in the results section show that the EMR system produced some results in the first study setting (Hospital A) relating to information quality and data sharing, especially in the short term. Hospital B found real and measurable benefits and impacts: indicators (such as the time saved for sending paper letters to GPs) for monitoring different types of impacts were defined prior to the adoption of the system and adjusted during the implementation phase according to needs and the evolving situation. Furthermore, the EMR system at Hospital B produced great benefits at “communication level” in terms of improved interaction between clinicians and nurses on the same ward, and between different departments and hospital sites. The main question that arises is “what is different in these two identical EMR systems that generate different impacts”?
Some organizational conditions, the organization’s characteristics, and the process of implementation adopted were found to be particularly important in this study and may help us answer the above question. First of all, organizational arrangements: the innovation project at Hospital B appears to benefit from strong support from clinical staff who drove the adoption of the system. Hospital A, however, suffered a lack of involvement among professionals (clinicians and nurses) in the development of innovation projects.
The second aspect regards the level of pre-existing expertise relating to innovation processes within the organization: this led to the focus on user needs at organizational level at Hospital B and to more technical and formal attention on the introduction of IT at Hospital A, led by external IT consultants. The adoption of the system at Hospital B resulted in the definition of new roles and responsibilities on the wards and affected the traditional way of “handling” the care process: technology affected the distribution and content of work tasks and modified the flow of information.12,38,39
The creation of multidisciplinary work groups to manage and oversee the overall innovation project contributed to acceptance of the EMR system 40 and can also enhance acceptance among the different users. Furthermore, specific training and programs were developed and delivered on the different wards in order to enhance the creation of new roles.
Finally, as regards the implementation process adopted, Hospital A opted for a “top down approach” with no promotion of participation in the process among its personnel from the selection phase. Hospital B, on the other hand, adopted a “bottom up approach” marked by a participatory process starting from the initial system selection onwards. 41 This is a specific way to generate and enhance commitment to the project within the organization that also influences the impacts produced in terms of effectiveness and clinical governance. Conversely, if this process is imposed it can generate user-frustration and can have an impact on the implementation process and on the overall use of the system.42,43
This comparative case study has provided some insights into how the process for implementing an Electronic Health care Record system unfolds at different hospitals and which types of effects can be produced, with the ultimate goal of understanding which issues are important for planning and managing such programs in the future.
Implementing changes affecting an organization’s structure and culture, work processes, behavior and communication channels, can be considered one of the most difficult and challenging tasks to overcome when conducting an innovation project at a healthcare organization. Measures and guidelines to promote active “change management” at all system levels may facilitate better implementation of HIT and EMRs in particular.
These are important considerations in order to produce a tangible response to the corporate need to identify the best way to adopt, implement and assess an organizational, cultural, technological and economic investment, and for providing objective guidelines with regard to the nature and direction in the medium and long term, which could depend on different elements linked to organizational conditions, the organization’s characteristics, and the process of implementation adopted, as this study found with regard to acute care settings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.