
Abstract
Despite well meaning initiatives over decades, the percentage of inpatients suffering adverse events remains constant in most advanced health systems. The notion of incident reporting as used in other safety critical industries has proved far less effective in healthcare. This article describes a new patient safety paradigm in the search for improved patient safety in healthcare. Underpinned by a holistic use of human factors the Safer Clinical Systems programme involves a proactive, risk-based approach seeking to eliminate or control risk before it is converted to patient harm. The tools and techniques applied by healthcare professional in real-life settings are described along with the outcomes of a significant reduction in risk and improvement in safety culture as measured by the Safety Culture Index. The challenges of applying the approach are discussed but it is argued that important progress could be made if a critical mass of healthcare staff were helped to acquire skills in human factors.
Introduction
Patients continue to be harmed in hospital systems across the world. Estimates suggest that perhaps 10% of inpatients suffer an ‘adverse event’. 1 There is less clear data from community settings but there is no reason to assume it is less of a problem. Hogan et al. 2 suggested that as many as 3.6% of hospital deaths are avoidable. In terms of understanding this situation, the article by Kohn et al. 3 is significant in suggesting that the majority of adverse events are due to systemic faults rather than to individual incompetence. Hollnagel et al. 4 provides a very good overview of this situation and argues that the causes may be found in the contextual pressures upon health systems, citing a fast increasing demand for care from ageing populations, rapid advances in technology producing greater complexity, rising costs of health putting pressure on the adequacy of staff resources. We would concur with the general thrust of this argument adding that much of the healthcare delivery has evolved in a piecemeal, common practice style where new technologies, drugs, etc., are incorporated as they emerge producing layers of delivery systems that attempt (and do) improve health outcomes but obscure the fundamental design of the underlying system to be as safe as it can be.
Any patient, member of the public or newcomer to this topic might well be thinking that clearly a response to rectify the situation is needed. And of course there have been considerable and well meaning efforts. However, it is the case that the picture described above has been known about for some 15–20 years and despite all efforts persists. The focus of these efforts has been driven by a fundamentally reactive approach bound up in the perception that systems are safe until they are not, i.e. something goes wrong so it must actually have been unsafe. The reality is that we didn’t really know whether it was safe or not but assumed or hoped it was, and then it wasn’t. It is this construction of safety that leads to the emphasis upon retrospective approaches such as incident reporting. This type of data collection is almost universally applied and does provide useful retrospective data on what happened, where responsibilities lay and in theory what we might do about it. Such a reporting system is in itself a transfer in approach to safety from other industries, aviation usually being quoted as the source. However, there is accumulating evidence that health sectors do not use such reporting systems effectively. They tend to emphasise an individual blame culture, they quickly become bureaucratic and there is little focus on the learning or interventions that might follow.5,6 A very recent (2016) report from the National Reporting & Learning System Research and Development team rehearses yet again that we don’t use these systems as well as we might and provides more guidance as to how use might be improved. It is undoubtedly good advice from a highly respected team, but it is also clear that despite the use of such reporting systems, however well or poorly actioned, the harm persists. Crudely, this retrospective accumulation of descriptions of past events is not achieving the greater safety for patients being sought.
The fundamental issue here is that virtually all approaches to improving patient safety are predicated on retrospective analysis. Despite their application, the percentage of in-patients suffering adverse events remains constant and therefore they are not achieving their aim. The premise here is that by refocusing patient safety initiatives on proactive identification of risk in the system and its elimination greater progress can be made. The article provides an account of just such an application.
A need for change: A new patient safety paradigm
In advocating a change in approach, we are not alone. Hollnagel et al. 4 have sought to move on from current thinking by redirecting attention to how we can learn from what works well, functions safely and therefore should be the basis of learning in the future. They refer to this as moving from Safety I (essentially looking for what went wrong) to Safety II where the search is for factors that made the systems safe and resilient to increasing pressure. This is an important insight since most healthcare delivery is safe most of the time often due to the positive and skilled efforts on staff. There is undoubtedly much to learn and implement from this refocusing on the positive.
However, we feel that this may be slightly premature in the context of the health system, which palpably has made limited progress in its current approach. Safety II admirably seeks to learn from the positive performance of clinical staff. As Braithwaite et al.
7
say Rather than counting incidents, hoping to drive out errors and focusing on the negative, we should strive to ensure that things go well, and accept that ‘safety is better measured by how often everyday work goes well than by how often it fails’. This shifts the efforts from reactive and protective patient safety to proactive and productive patient safety.
In the account of a Safer Clinical Systems project given here, we seek to learn and apply approaches from other sectors and to understand the challenges that implementation may bring to the health sector. It seems reasonable to ask, if the health sector has not improved its safety as much as one would have hoped, what might it learn from industries that have made such improvements.
As we have said current approaches are fundamentally retrospective, in building for safety this means that the first thing that has to happen to trigger the system is that we harm a patient. There are two absolutely key principles to be learned from other safety critical industries that the health sector must incorporate in order to change its approach – the first is to be proactive and not to wait for the problem/error to manifest itself, and second is to seek out the risk that exists within the delivery system and eliminate or control it before it results in harm.
In the U.K., for example, before a chemical plant is opened or a new aircraft brought into service, it must be demonstrated to the appropriate authorities that it will be safe (within certain acceptable and agreed limits). The risks are expected to be known in advance, as well as their consequences: how often will this piece of equipment fail to perform? How likely is operator error to create risks? What has been done to eliminate, reduce or mitigate risks? Can the risk and likely safety of the enterprise be quantified? What is an acceptable level of risk? Healthcare as a sociotechnical system with heavy reliance on human resources adds a further and very unpredictable aspect of uncertainty to understanding the system risks. Nonetheless, we believe that these proactive, risk-based approaches can be applied to healthcare and indeed that they must if radical improvement in patient safety is to be achieved.
The Safer Clinical Systems programme is an integrated, holistic application of various key concepts from other safety critical industries. Before describing the process of application, it may be useful just to provide a brief comment on each of the elements, so that when applied it is clear how they are being used and how they contribute to the overall programme. As mentioned earlier, the overall intention is to shift the approach to safety from reactive to proactive. But contributing to this goal and the total Safer Clinical Systems programme are the following concepts.
Human factors
Human factors are a hybrid discipline encompassing elements of psychology, social psychology, risk and ergonomics. This discipline has been central in building safety in other safety critical techniques. Though human factors is often understood as the set of non-technical skills that underpin safe human performance – such as communication, situational awareness, decision-making and leadership – there is another aspect of human factors that focuses on the identification of risk within a system and the development of interventions and strategies to eliminate, reduce or mitigate risk. These two aspects of human factors are sometimes referred to as ‘person-based human factors’ and ‘system-based human factors’. These two approaches find common ground in the importance that they assign to human behaviour and how it is influenced by context. They are usually called ‘performance influencing factors’ and include distractions, communication factors, information provision and support for key tasks. Both elements of human factors have been important in developing Safer Clinical Systems.
Russ et al. 8 working in the U.S. health system emphasise the design changes to health systems that can both improve efficiency and patient safety. They make the interesting point that misunderstanding of Human Factors in healthcare, which is widespread, is reinforced by statements about human failure. Of course, these exist but the application of human factors is as they argue more about system re-design with a focus on the organisational level rather than individual.
Catchpole 9 reiterating the issue of a misinterpretation of human factors suggests that the identification Crew Resource Management (CRW) as applied in the aviation industry has led many to see human factors as a training-based solution. It is in reality a much broader perspective and it is this broader approach that is employed within SCS.
Risk in clinical systems
Formally, we define risk as the combination (usually multiplicative) of the likelihood of occurrence of a hazard and the severity of the consequences of a hazard (frequency × severity). In practice, this really means the chance of something going wrong for patients. In many industries, the estimation of risk may be precise and quantitative – how likely is this valve to fail or this pilot to press the wrong button? – but in healthcare, our estimated risk is usually derived through a highly subjective process using crude metrics such as ‘highly likely’ or ‘moderate’. Despite this, we believe that these methods and estimates have real value. This is especially true when the knowledge and estimation of risk are carried out by teams of involved professionals through consensus.
A chief characteristic of the Safer Clinical Systems approach is a focus on managing clinical risk. This is achieved through a proactive focus on risk and its identification in a patient pathway, in contrast to the traditional focus on counting things that have already gone wrong for patients. This is because, as in other safety-critical industries, there is a recognition that safety depends upon the management of risk.
The focus on patients outcomes that runs through healthcare systems is not necessarily a reflection of good safety management practice, but of the need of managers, and, indeed, political systems, to identify and highlight simple, easily understandable measures. It is a great deal easier to talk about numbers of patient deaths or numbers of pressure ulcers than about the factors that influence them – factors relating to risk, or culture or care process reliability. Numbers of patient deaths, for instance, easily identified through comparing mortality ratios from hospital to hospital, are not a reflection of quality of care or patient safety within the hospitals for a number of well-known reasons. 10
At the heart of Safer Clinical Systems is a new approach to safety in the healthcare sector – an approach based on learning from excellence in other industries and also on the special needs of healthcare. We believe that the approach, the tools and techniques, the emphasis on culture and context and the prominence of human factors in this work constitutes a new paradigm for patient safety.
Systems thinking
Systems thinking is a way of understanding how individual elements in a greater whole influence each other. It is a process of understanding the inter-relatedness of system components and seeing all those components as part of the common process with a particular common purpose. In practical terms, it recognises that reacting merely to a specific, often small, part of a problem not only frequently fails to solve the problem but also brings the danger of unintended consequences. Our approach to systems thinking in healthcare is probably best understood as a conceptual framework, a body of knowledge and a toolkit that has been developed to try to make larger patterns clearer and to help researchers and improvement teams to determine how to change them most effectively.
All things exist in systems. In healthcare, individual system components include the patient, the clinicians, the equipment and the environment in which the care takes place. Systems thinking, in general, is a process of understanding the interrelatedness of the system components as part of a common process with a common purpose. In several public services, there has been a growing recognition that improvements in quality and safety need to occur at a so-called ‘systems’ level in order to be widespread and sustainable. In healthcare, this requires focusing not only on the clinical care of the patient but also on the many systems that support and enable clinical care.
The systems approach in healthcare was perhaps most visibly introduced following the inquiry into infant cardiac surgery at the Bristol Royal Infirmary. 11 In this inquiry, though individual error or lapses in performance were identified, there was an attempt to see them as the product of systems that had failed to work properly. The inquiry adopted an approach that effectively began with an examination of the organisational context and practices before considering the performance of individual events and clinicians.
Culture and context
Safety culture is a quality of the wider organisation describing how individuals, teams and systems understand and manage safety. It is based on individual attitudes, beliefs and behaviours. Most workers believe that safety culture has a material effect on human performance and that it is a critical element in the context of practice. A safe clinical system would therefore exist in a cultural environment that supports safety through openness and fairness, and has a shared understanding of such factors as risk, reliability and error.
Many safety or quality improvement initiatives fail. Imposed ‘solutions’ developed from outside the clinical microsystem often fail to engage clinical staff and lack sustainability as a result. Interventions that look perfectly sensible from the outset can be difficult to implement if the wider organisational context doesn’t support them, or if the prevailing culture unwilling to embrace the changes. We believe that understanding the organisational context and factoring this into the design of safety interventions is essential to building sustainable change, and the Safer Clinical Systems approach seeks to address this through starting the programme with a contextual assessment.
An organisational ‘safety culture’ is inevitably a component part of a wider culture of the organisation in which it is embedded. The term ‘culture’ is itself slightly abstract and difficult to define. Nonetheless, it is very widely used and often as an explanatory concept as to why some form of organisational failure may have occurred. This is exemplified in the recent Francis Report 12 on the multiple care failures at Mid-Staffordshire NHS Trust. There are many aspects that may to go make up organisational culture (attitudes, values, beliefs, language, traditions, practices, processes, symbols) are just some.
Effective management of safety and consequently incident attribution has shifted focus from the individual to the organisation and typically includes organisational factors such as norms of behaviour, management style and organisational culture.
13
As Leonard and Frankel
14
comment ‘highly reliability environments deal with risk and hazard on a daily basis, yet maintain impressive levels of safety culture and continuous learning’. This systems approach and the key cultural factors involved are nicely summarised by Leape and Berwick
15
The combination of complexity, professional fragmentation and a tradition of individualism, enhanced by a well entrenched hierarchical authority structure and diffuse accountability, forms a daunting barrier to creating the habits and beliefs of common purpose, teamwork and individual accountability for successful interdependence that a safe culture requires.
Singer et al.
17
identified some important elements of patient safety culture:
Leadership commitment to safety Organisational resources for patient safety Priority of safety versus production Effectiveness and openness of communication Openness about problems and errors Organisational learning
The responsibility of organisational leaders to develop and build such aspects is emphasised by Leonard and Frankel 14 who suggest important aspects such as creating a psychologically safe environment in which teamwork can flourish; organisational fairness that allows different issues to be discussed openly; a learning system that enables leaders to demonstrate active support and interest in the problems encountered by frontline staff. The Safety Culture Index (SCI) as used in the Safer Clinical Systems programme has the great and unique advantage of such tools of both measuring the organisation’s safety culture as well as identifying implications for leadership.
Safer Clinical Systems programme: A patient safety improvement initiative based on learning from other sectors
Safer Clinical Systems was a programme funded by the Health Foundation to explicitly examine the notion of whether the constructs outlined above could be successfully applied to a healthcare setting. The programme was supported by the authors working with eight hospital sites from within the U.K. The participating sites were invited to apply outlining their area of focus for safety improvement and the clinical team supporting the delivery. Following documentary review, eight sites were selected having a wide geographical range as well as distinctly different patient and service groups as the focus of the work – from renal patients, severely disturbed children, Parkinson patients or admission units. The programme was run as a collective with the teams from each site coming together throughout the 3 years of the programme to share the underlying concepts of the approach, be given training in the use of particular tools to represent the application of the concepts and then implement both these tools and techniques as well as the safety improvement initiatives derived from them. The programme had three key aims:
to introduce NHS staff of various background to the core concepts (proactively, risk, applied human factors, systems thinking and culture/context). to understand how best to present these concepts (as quite new to many participants) as well as gauge how best (and how long) transfer of skills in the use of associated tools and techniques might be achieved. to assess the impact of the implementation of Safer Clinical Systems (concepts, tools and techniques) on the safety on the particular area of focus.
Programme structure
The overall programme was structured into five steps (see schematic outline below).
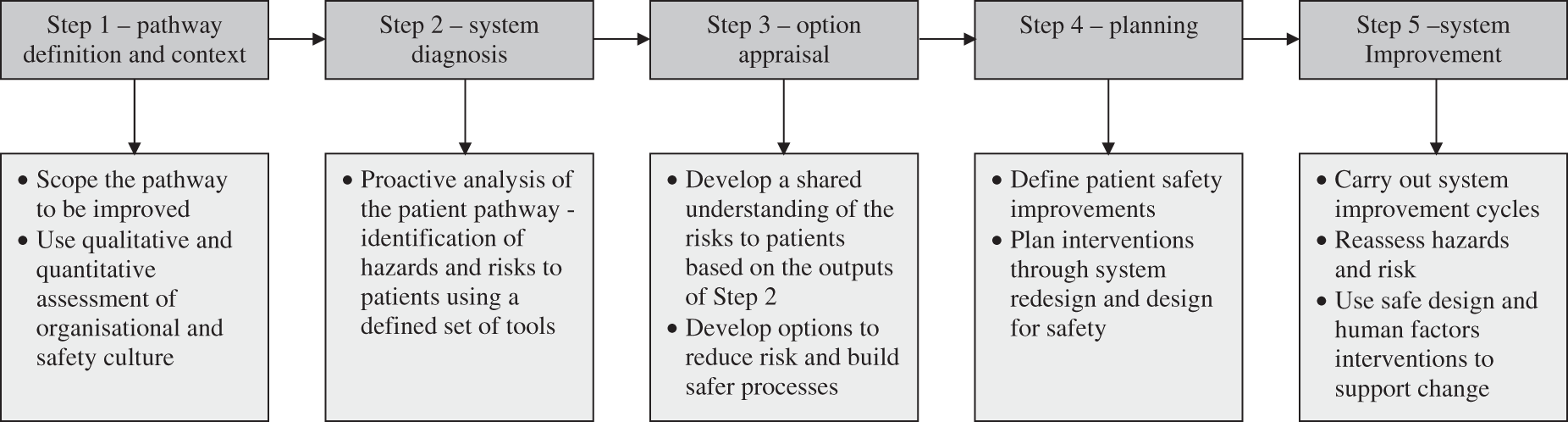
The structure and flow are, in part, inherent in the sequence of understanding and identifying risks in the system through to implementation, but it was also used to pace each collaborating site through the learning events. In this way, all sites proceeded to the next in a coordinated fashion with a ‘sign off’ on the previous stage before moving on. This was important to maintain control but also to enable learning about each stage to be captured systematically.
A full account of each stage and detail of how to use the tools and techniques is provided in the report of the programme (Safer Clinical Systems Report 2016) published by the Health Foundation. 18 A few brief comments here on each stage reflecting the critical aspects of each:
Step I: Pathway definition and context
The purpose here is to define the pathway boundaries and to develop a deep understanding of your culture and context. A pathway is defined as a patient journey incorporating the wider context of the system flow as well as the specific focus of care tasks. Typically historic data from Reporting Systems, known harm events will form the first part of this supplemented by both qualitative and quantitative measures of culture and context.
The SCI was used to assess the existing patient safety culture at each site within the specific area of patient care. The SCI consists of 60 items that form 12 scales grouped under four core cultural dimensions.
Task focus: Coping with work demands Purpose and direction Role clarity People focus: Participation in decision-making Working in collaboration Staff motivation Control focus: Checking and accountability Sharing information Standards monitoring Change focus: Commitment to learning Blame-free climate Vision and mission
They measure culture at three levels – individual, team and organisational, and have previously been shown to be reliable and valid in describing safety – relevant aspects of working practices.
Step 2: System diagnosis
This is a crucial step involving a detailed diagnostic assessment of the tasks within the pathway, the reliability, the associated risk levels and the process/outcome measures linked to knowing where risk (and therefore potential harm to patients) can be reduced. Various tools and techniques of human factors (Process Mapping, Hierarchical Task Analysis, Failure Mode and Effects Analysis) are used here to present the main challenges to NHS staff in acquiring expertise in their use. A consequence of this process is often awareness amongst clinical staff of risks to patients that they had not previously recognised and also a clear ranking of the priority of risks to patients to be tackled.
Detailed training in the technical aspects of each technique was provided in the programme and is described in the full SCS programme report. For example, McElroy et al. 19 debate various scoring methods for use with the Failure Mode and Effects Analysis Tool.
Step 3: Option appraisal
Having established the risks and where located in the delivery process, it is at this point that potential interventions are identified, considered and appraised. It is important that all risks are entered into the appraisal process and that ‘practical’ options are not over-emphasised too quickly otherwise more significant improvements, but also more difficult to put in place, are discarded too readily.
Step 4: Planning
This is essentially planning to implement the safety changes previously prioritised. This may involve both the technical content, i.e. the nature of the change to the system, as well as the more human aspects of engaging staff to seek their support in the process of implementation. The latter can be time consuming but is absolutely vital to success.
Step 5: System improvement
The purpose of this phase is the conduct of improvement cycles based upon your prior analysis. A key here is clear, focused measurement that allows a baseline to be set and change properly monitored such that it can be unambiguously attributed to the changes made. In addition to changes in risk levels, it may also be good practice to reflect changes in safety culture as a result of the involvement in the Safer Clinical Systems programme.
Results
System risks
As part of the methodology described above all eight participating sites conducted an analysis of hazards, risks and existing risk control measures within the diagnostic phase. The risks were categorised as high, medium or low. These same risks were reassessed by the same clinical teams 9 months after the implementation of the changes. Each risk was unique to the particular site and patient area involved.
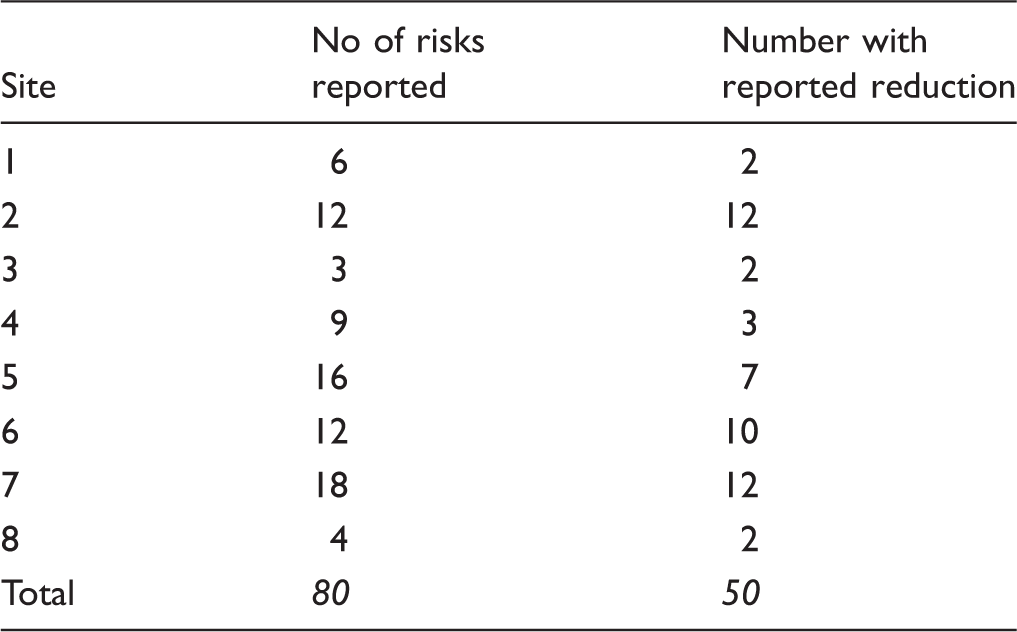
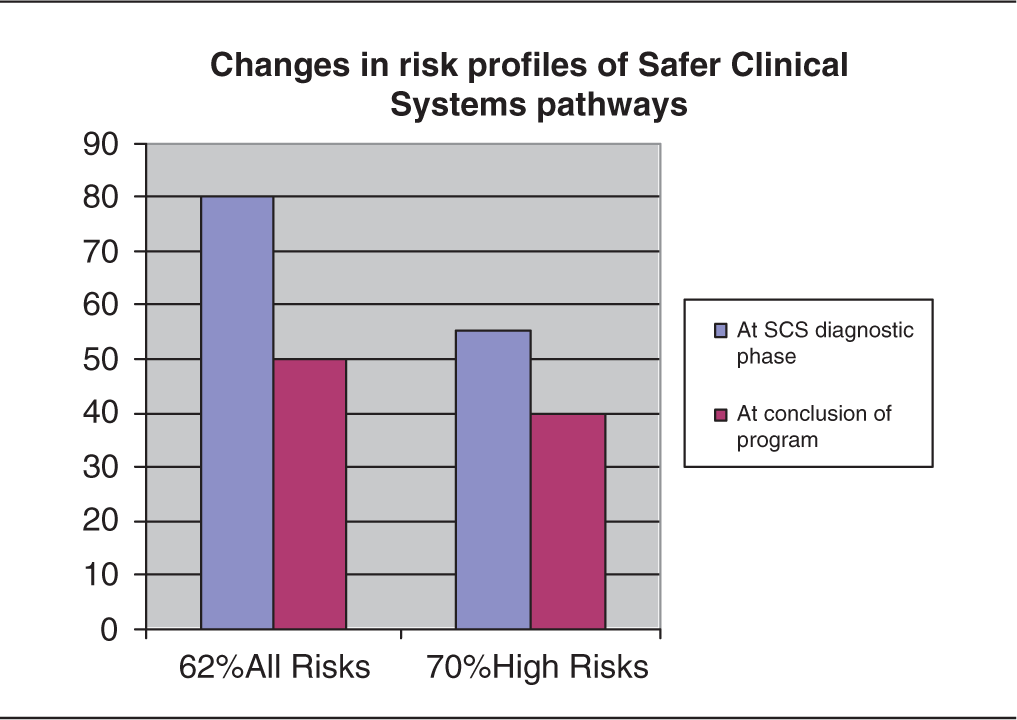
Overall the eight sites that took part in this exercise reported a total of 80 systematically identified risks where existing control measures were weak or absent and where interventions were designed and introduced to reduce risk to patients. Of those 80, the sites reported that 50 had been reduced.
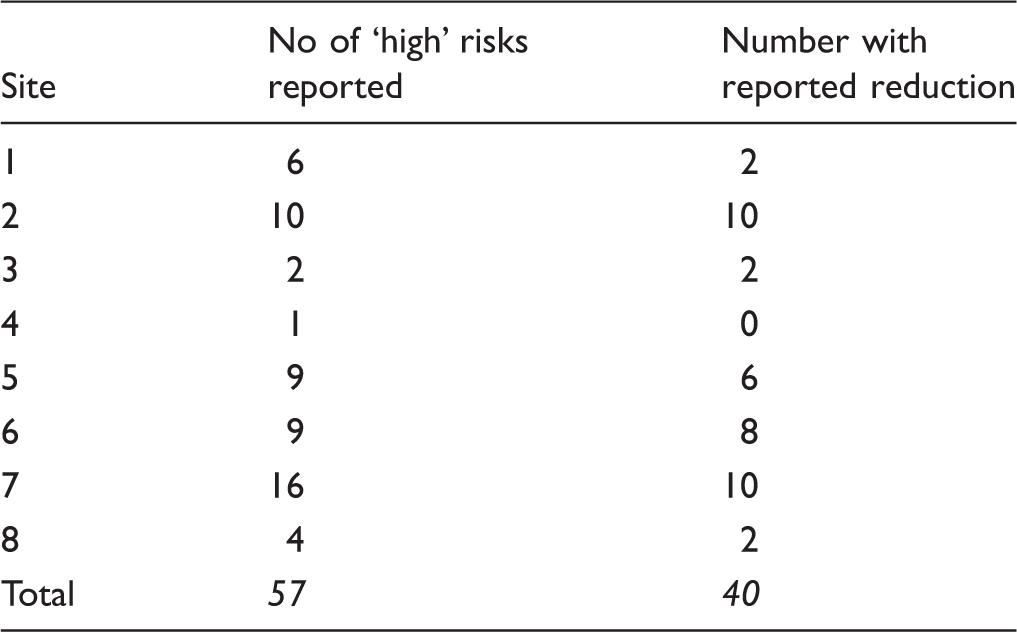
Looking only at risk categorised as ‘high’ during the diagnostic phase, and excluding any ambiguous current risk evaluations (where a risk was categorised as high/medium, for example), the sites identified a total of 57 risks where control measures were inadequate. Of these, sites reported a reduction to either ‘low’ or ‘medium’ in 40 cases. Of these, 12 key risks were currently evaluated as ‘low’.
The risks described by sites as having been reduced were identified during the diagnostic phase of the programme, and included incorrect prescriptions for acute medicines, accuracy of information provided for critical handovers and key patient evaluations prior to surgery.
Site risks identified by each site using FMEA.
High risk areas identified by each site using FMEA.
Percentage risk reduction across all eight sites.

Safety culture
The SCI is a culture assessment tool based upon a psychometrically rigorous framework. It is a comprehensive survey tool derived from a number of research studies. The first version of the measure was described by Spurgeon and Barwell 20 and was further developed by Spurgeon et al. 21 The SCI scales have been shown to be reliable and to have content and criterion-related validity across a variety of healthcare contexts.
The Scale assesses norms in 12 key attributes of organisational culture. The tool was used across eight NHS trusts on two occasions – during Step 1, defining the pathway and assessing the organisational context, and again after progressing the Safer Clinical Systems programme.
Highest percentage improvement levels on SCI scales across all sites.

Using the SCI following the implementation of the Safer Clinical Systems programme, significant improvements in safety culture were identified in six out of the eight participating trusts. The following are examples of the positive changes and levels achieved.
In this context of the Francis Report and its exhortations to the NHS to changes its safety culture, this is a critical outcome.
Conclusion: A new perspective on safety
Harm persists and we believe that despite all the progress that has been made in the technology of medicine over the past 20 years, a new approach is needed to build patient safety. It is certainly true that the science of medicine will continue to develop interventions that are life-saving and that will improve the quality and extent of people’s lives. That is not the issue: the issue is that these technologies are delivered within a complex system and that the system too often fails its patients.
We do have a safety management system: it began in 2000 with the report An Organisation with a Memory. Since we have had the establishment of the National Reporting and Learning System, the many reports into safety and quality following events at Mid Staffordshire, numerous reports and reviews of hospital safety, countless calls for openness, transparency and whistleblowing, and the setting up of an external investigating body for when things go wrong for patients.
What do all these things have in common? The answer is simple: they are reactive. They only swing into action after a patient has already been harmed. The result is that interventions are specific to the clinical microsystem in which the error occurred. They tend to ignore human factors and give no assurance that the underlying causes of harm and error (which will often transcend the microsystem) are being addressed. Risk management is too often a bureaucratic process designed more to assure the regulator than to manage either patient risk or enterprise risk, and as such, rarely contributes to system-wide improvements in safety.
There is a clear need for a proactive approach to safety. This may not be easy; unlike engineers who build a new power station or launch a new model of aircraft, clinicians and managers are operating in a living, breathing system where patients cannot simply be placed on hold while we transform our processes. This doesn’t make things easy, but nor does it make things impossible: we have shown how system risk can be reduced and patient safety culture materially changed by the interventions of Safer Clinical Systems. And change must come because of the complex and tightly coupled nature of the healthcare system. Such systems are known to fail, regardless of the good intentions of the people who work within them.
Our existing safety management system, built on reaction to past harm, is not good enough. The bolting on of emergency planning mechanisms is necessary but insufficient. Patient pathways and high-risk areas wherever they exist must be proactively assessed for risk, and this assessment must be systematic, evidence-based, free from blame and cognisant of the organisational context. That is what safer Clinical Systems is all about.It is time to learn how to be safe before a patient is harmed. It is time to build Safer Clinical Systems.
The Safer Clinical Systems programme has been the subject of a thorough evaluation and a summary of the findings were published by the Health Foundation.
22
A brief extract from the document will perhaps underline the argument in this article. The evaluation team paint a rich and sobering picture of clinical systems that were often ‘highly unreliable’ and laden with potential for ‘harm to the patient’. For example, one team mapped 99 hazards along the shared care pathway for renal patients having a surgical intervention…….
The approach of Safer Clinical Systems offers both opportunity and challenge to those managers working within patient safety context. It is easier to continue to use existing methods and correctly report that an incident has been investigated and that steps have been taken to avoid it occurring again. The problem is that it will occur again in a different form and different sequence of cumulative causes, and therefore it is not making the system safer. For those managers willing to rise to the challenge of applying the techniques of SCS, the task is to take each delivery system – contained and across boundaries – and locate the sources of risk in the system and work with clinical colleagues to control or eliminate it so that patients are no longer harmed by the risk manifesting itself as harm.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the support of the Health Foundation in funding the Safer Clinical Systems programme.