
Abstract
Italian and American hospitals, in two different periods, have been urged by external circumstances to extensively redesign their quality improvement strategies. This paper, through the use of a survey administered to chief quality officers in both countries, aims to identify commonalities and differences between the two systems and to understand which approaches are effective in improving quality of care. In both countries chief quality officers report quality improvement has become a strategic priority, clinical governance approaches, and tools—such as disease-specific quality improvement projects and clinical pathways—are commonly used, and there is widespread awareness that clinical decision making must be supported by protocols and guidelines. Furthermore, the study clearly outlines the critical importance of adopting a system-wide approach to quality improvement. To this extent Italy seems lagging behind compared to US in fact: (i) responsibilities for different dimensions of quality are spread across different organizational units; (ii) quality improvement strategies do not typically involve administrative staff; and (iii) quality performance measures are not disseminated widely within the organization but are reported primarily to top management. On the other hand, in Italy chief quality officers perceive that the typical hospital organizational structure, which is based on clinical directories, allows better coordination between clinical specialties than in the United States. In both countries, the results of the study show that it is not the single methodology/model that makes the difference but how the different quality improvement strategies and tools interact to each other and how they are coherently embedded with the overall organizational strategy.
Introduction
Quality improvement (QI) has become an increasingly important issue over the past few decades, with many countries establishing the provision of high quality, safe health care as a national priority. One of the World Health Organization’s priorities is establishment of effective strategies for ensuring quality of patient care within each healthcare system. 1 Consequently, policymakers of industrialized countries share an interest in implementing quality management practices to deliver appropriate care to patients, achieve positive clinical outcomes, avoid unnecessary clinical complications, and ensure efficient use of resources (e.g. Blaise and Kegels, 2 Kunkel and Westerling, 3 Macinati, 4 Makai et al., 5 Pejović et al., 6 Simou and Koutsogeorgou, 7 Cohen et al., 8 McGlynn et al., 9 Wachter, 10 Leape and Berwick, 11 and Ross et al. 12 ).
This paper aims to analyze the strategies employed by Italian and American hospitals to improve quality of care. We administered in Italy a survey instrument used by Cohen et al. 8 to analyze the QI strategies employed by American hospitals in reaction to the publication of the US Institute of Medicine (IOM) report 13 that documented numerous deficiencies in patient care quality and safety.9–12 In a subsequent report the following year the IOM 13 called for a redesigned US healthcare system to resolve patient safety errors. Shortly after the publication of the IOM reports, US hospitals began to design different types of QI and patient safety initiatives.14–17
The US healthcare system is large and complex, with approximately 4900 community hospitals and a mix of private and public insurance programs. Since 2010, the healthcare system has undergone major reforms in new service delivery models (e.g. accountable care organizations containing networks of hospitals and physicians) and new payment models that reward providers for their performance in delivering more effective and less costly care.
In contrast, the Italian healthcare system is a publicly-funded system that guarantees universal coverage. It has three tiers: the central government at the top level; 21 regional governments in the middle; and approximately 200 local health authorities (LHA) with their own hospitals and other healthcare facilities (as well as 100 independent hospitals not under the jurisdiction of a LHA a ). Since 2001, the system has undergone massive decentralization, with regions now having jurisdiction on all healthcare issues including promoting policies to improve quality. 4 Italian hospitals, like those in the US although almost a decade later, implemented new QI initiatives after a series of national and regional programs stressing the critical importance of improving quality. 18
Despite the growing literature in QI systems, it is unclear which strategies and tools have been actually used by hospitals and with which results. In fact most of the scientific studies have focused their attention on the evaluation of the application and effectiveness of single specific QI tools and methodologies. However, as shown by Walshe 19 in his bibliometric analysis, over the last two decades, we have seen the successive rise and fall of a number of concepts, ideas or methods in healthcare QI (QI); tools, methodologies or even terms often rise in popularity, are used for three or four years and then fall out of use or fashion again. 19 It can be seen, for example, that “medical audit” and “clinical audit” did so in the early and mid-1990s and that a similar burst of interest in total quality management (TQM) was followed by a somewhat more sustained interest in continuous QI. 19 In recent years the buzzwords are represented by terms such as lean thinking and six sigma. These results show that it is not the single methodology that makes the difference but how the different QI strategies and tools interact with each other and how they are coherently embedded with the overall organizational strategy.
The present paper, unlike most previous studies in the field, aims to carry out a more comprehensive assessment of the QI systems looking at the interdependence between the different tools and components with the aim to understand which features work and which do not. We try to accomplish this goal by comparing two different systems that, even though in different periods in time, because of external pressures, have gone thorough massive reforms and innovation in their QI systems.
Other studies20–27 have shown in the past that comparing practices, innovative organizational solutions or QI strategies, adopted in several countries, can actually provide useful insights to both managers and policy makers. Hussey et al., 28 for example, have compared international data on the quality of medical care in Australia, Canada, New Zealand, England, and the United States. They found that each country had at least one area of care where it could learn from international experiences and one area where its experiences could teach others. Ferlie and Shortell 21 investigated deficiencies in care in the United Kingdom and the United States and proposed four levels of interventions to improve the quality.
Sluijs et al. 22 analyzed the relationship of government quality policy and quality management in health care by comparing two countries with different quality policies (Netherlands and Finland). The objective of Wagner et al.’s 26 research was to investigate agreement and disparities in the implementation of quality management activities in the Netherlands, Hungary, and Finland. The results indicated that government legislation or financial reimbursement can stimulate the implementation of quality management activities more than voluntary and bottom-up approaches.
Having said that—in order to partially fill the gap found in the scientific literature—the paper aims to address the following two research questions:
What QI strategies have Italian and American hospitals implemented in response to external pressures to improve quality? What characteristics of the QI systems implemented in the two countries actually facilitate improvement of patient care quality?
In the next sections, we present the methodology, findings, discussion, and policy and managerial implications.
Research methodology
Sampling and survey administration
In the US survey, the sampling included all short-term, nonfederal, general service hospitals that had at least 25 beds in 2004. The survey was sent to the universe of 4237 hospitals. The final sample contained 470 hospitals, a response rate of 11%. The sample is similar to that of the population except for overrepresentation of large hospitals and teaching hospitals and underrepresentation of small hospitals (including nonmetropolitan hospitals and non-profit hospitals). Although this is a less than desirable response rate, as discussed in more detail in the original paper reporting on this survey 8 and in a recent paper addressing the issue of potential bias from non-response, 29 valid results can nevertheless be obtained from surveys with low response rates.
In the Italian survey, the questionnaire was mailed to the quality manager or general manager of all 229 public healthcare providers (teaching hospitals (AOU), independent trust (AO), research hospitals (IRCCS) and local health authorities (LHA)) with a cover letter explaining the purpose of the study, followed a few months later by a telephone call. The survey was conducted between September 2011 and September 2012 with a response rate of 27% (Table 1). Before analyzing the data non-response bias tests were carried out in accordance with Oppenheim. 30 A t test was conducted to examine whether there were systematic differences between early and late responses. No statistically significant differences in the means scores were found between early and late responses for any of the variables included in the study, thus revealing that non-response bias was not a problem in this study. All the questionnaires were fully completed and, thus, none of them was excluded.
Respondents’ characteristics in Italy and the US.
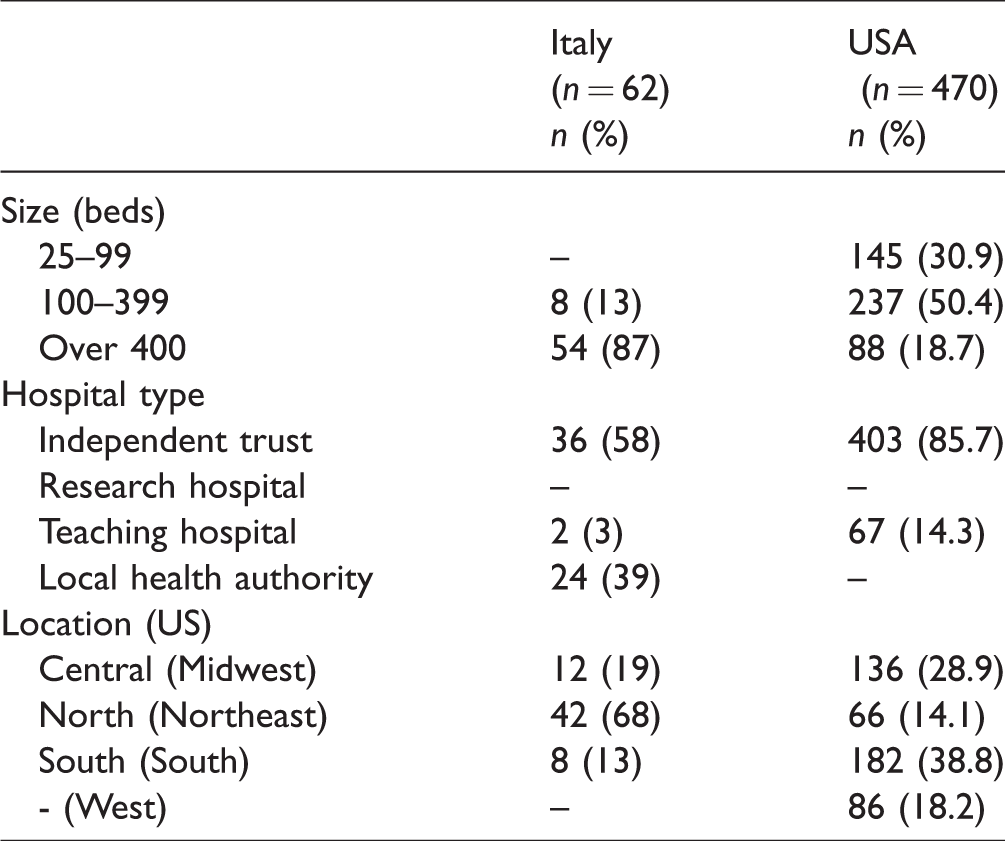
Sample hospitals were similar to the population of Italian hospitals in terms of institutional arrangement (independent trust versus LHA versus teaching hospital) except for underrepresentation of hospitals from the south.
Questionnaire
This study employed a survey method to collect data; in particularly, we adapted to the Italian context a questionnaire that was first developed and tested by Cohen et al. 8 in a previous study carried out in US hospitals. 31 This American survey was based in part on previously established surveys17,32 and endorsed by the Health Research and Educational Trust of the American Hospital Association and the US Department of Veterans Affairs Health System.8,31
As explained in the introduction the two surveys were administered in two different time frames; this circumstance does not undermine the robustness of the study since the objective of the paper is to evaluate the different reactions of the two systems in response to external pressures, that occurred in the years immediately preceding each survey, to improve quality and safety of care provided to patients.
The survey followed the detailed procedures outlined by Dillman. 33 First, the questionnaire was tested in five different pilot case studies and slightly changed to consider the specificities of Italian context regarding, for example, the different hospital organizational structure or the different national and regional institutions in charge of QI policies. The Italian version of the questionnaire was a translation of the original validated American research instrument. Specifically, the questions were compiled in English, and then translated into Italian and back translated in English by two independent translators to ensure that the content of the questions remained unchanged.
The distribution procedures involved (a) sending a pre-notice mail announcing the survey; (b) sending another mail containing the questionnaire 34 ; and (c) three follow-ups by telephone calls. The questionnaire was sent by e-mail to all chief quality officers (CQOs) of Italian public Independent Trusts and LHA. We ensured to respondents that the completed questionnaire was directly received by the researcher and, in doing so, we protected respondent anonymity and reduced evaluation apprehension by assuring respondents that there were no right or wrong answers. 35
The questionnaire included the following five sections with a total number of 51 questions. Specifically, the survey was structured as follow:
hospital quality managers and their role (3 questions); hospital approach to QI (11 questions); quality tools and methodologies (17 questions); quality measures and information system (14 questions); assessment of patient care quality (6 questions).
For most questions, a 5-point scale was employed, which asked respondents to indicate their agreement with statements about the hospital and/or its practices (response categories ranged from strongly disagree to strongly agree). For other questions there was a list of options where the respondents were asked to select the one/s used in their organization. Respondents had also the chance to select the option “I don't know” if he or she were not able to identify an opinion by not answering to a question.
As mentioned in the introduction, we have designed this survey not only to depict the state of QI initiatives in the two countries but also to understand which models and approaches work better in improving quality of care. In order to accomplish this second goal the survey contains two different types of questions:
a first type of question assesses, in objectives terms, if the characteristics of the two systems are consistent with the standards and best practices found in the scientific literature; a second set of questions assess, on the other hand, the perceptions and evaluations of CQOs about the level of quality of care offered in their organizations and the actual impact of models and tools implemented at their hospital.
The comparison of the actual characteristics of the QI systems with the guidelines commonly found in the quality literature and with the perceptions of CQOs allowed us to draw some conclusions regarding the impact of different QI models and tools reported in the discussion.
Statistical analysis
The analyses performed followed the approach of Cohen et al. 8 and were conducted in two steps: (i) descriptive and (ii) bivariate analyses.
First, for all the questions of the survey we performed descriptive statistics by calculating percentages and means to explore the trends and type of QI strategies (in terms of tools, methodologies and approaches).
Second, bivariate analyses were carried out in order to examine the association between the nurse-to-bed ratio and the “Quality managers’ assessments of hospital quality” questions. For each of the five questions—“patient care today versus what it should be,” “patient care today versus 3 years ago,” “comfort in having a family member treated without being present to monitor the care,” “the hospital’s QI focus has resulted in major performance gains,” and “patient satisfaction is where it should be”—we combined the top two categories and the bottom three categories.
Statistical significance was interpreted using p values of less than .05. Data was analyzed using SPSS.
Findings
Hospital quality managers and their roles
The first section of the survey investigated the quality managers’ responsibilities and their roles in the organization. First, quality managers were asked to declare whether quality was a priority in their hospital strategic and/or business plans. In both countries CQOs reported QI to be considered an important organizational goal. Nearly all hospitals (98% IT; 93% US) included QI as a priority in their strategic and/or business plans and included quality related goals in their formal budgeting process. In addition, 96% of respondents in the US and 70% in Italy reported having a quality council or other high-level management committee whose primary purpose was to oversee and coordinate QI activities.
Table 2 shows the responsibilities of Italian and US hospital quality managers. In both countries, the roles and responsibilities of these managers extend beyond the traditional focus on quality assurance (as opposed to QI), which consisted primarily of medical audit and other retrospective reviews, to more proactive areas such as institutional accreditation and control of ISO 9000 standards for performance measurement (93% US; 55% IT), patient safety (83% US; 45% IT), patient satisfaction measurement (50% US; 44% IT), and clinical risk management (56%: US; 44% IT).
Quality managers and their roles.
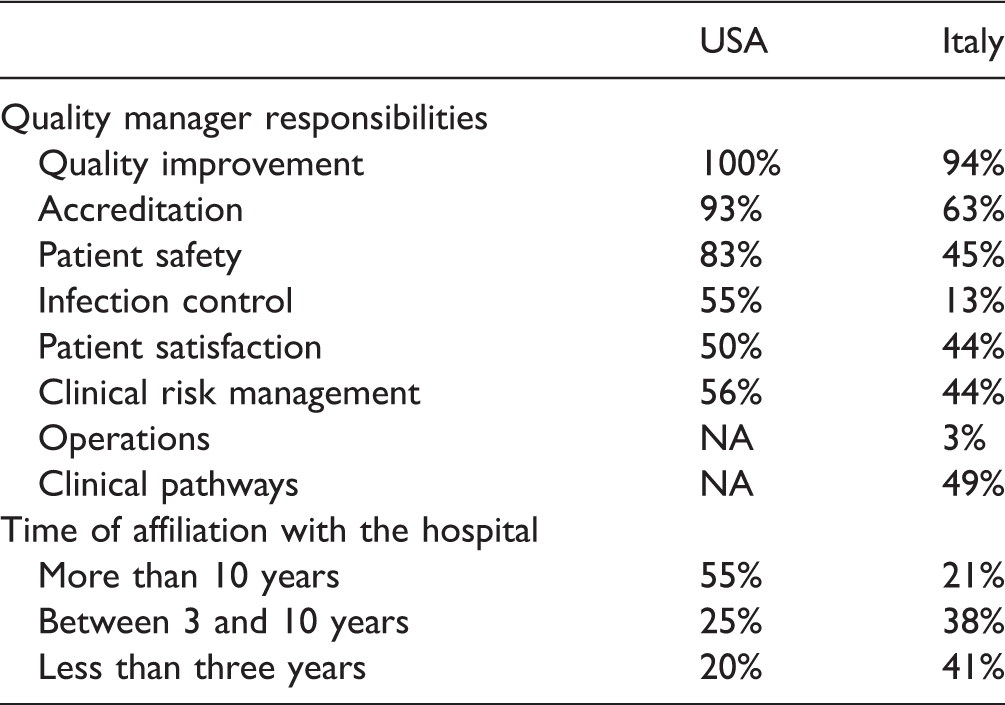
NA: not available.
However, in Italy, the role of the CQO is more limited than in the US. Hot issues such as patient safety and clinical risk management were among CQO responsibilities in less than half of hospitals, infection control in only 13%, and operations management in 3%.
Table 2 shows the time of affiliation of quality managers. Most US CQOs (80%) reported long affiliations with their hospitals, with 55% having worked there more than 10 years compared to only 21% of Italian respondents.
Hospital approach to QI
In this section the survey asked about the hospitals’ approach to QI (Table 3) and the presence and scope of training programs specifically dedicated to quality (Figure 1).
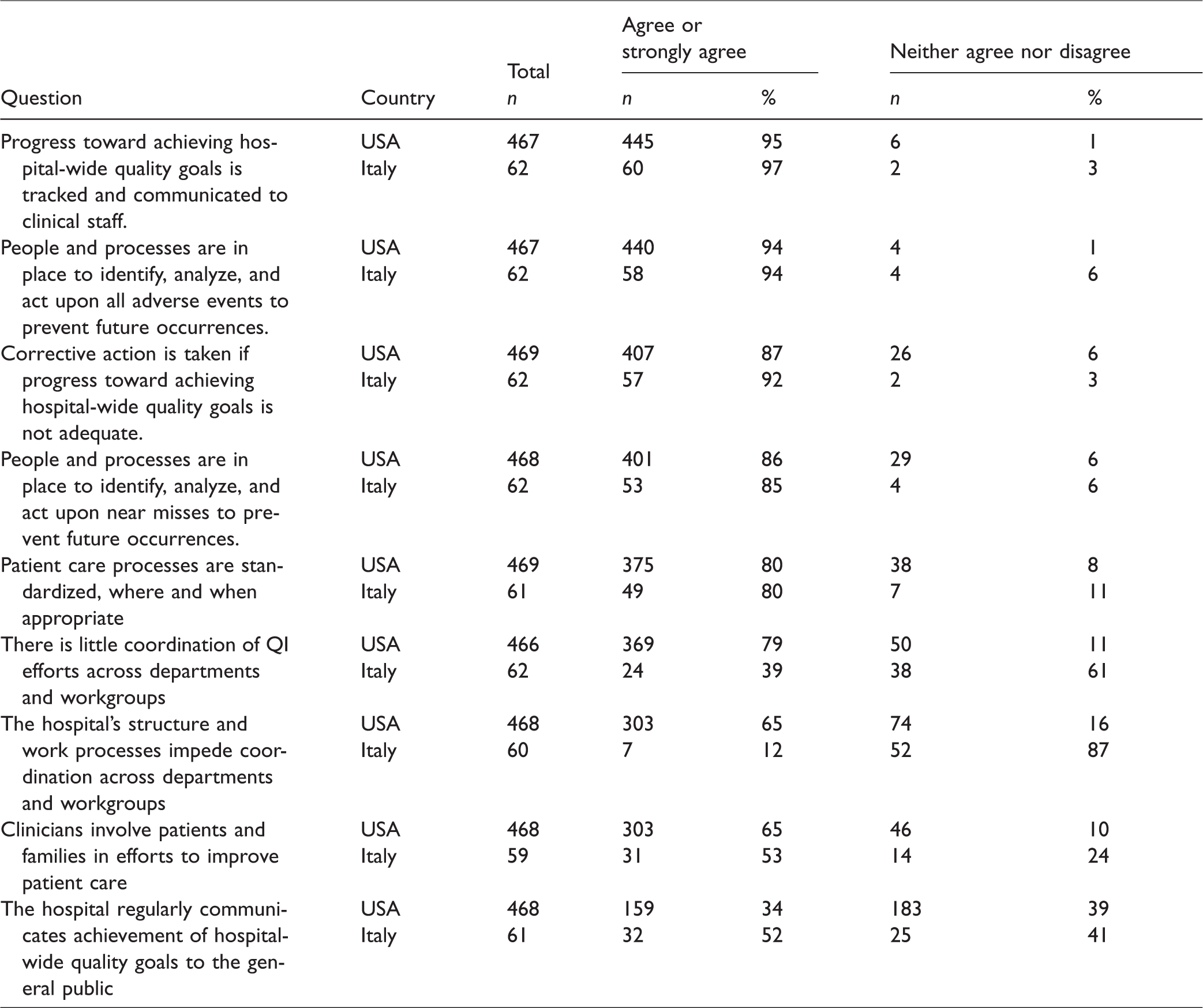
Hospital approach to quality improvement.
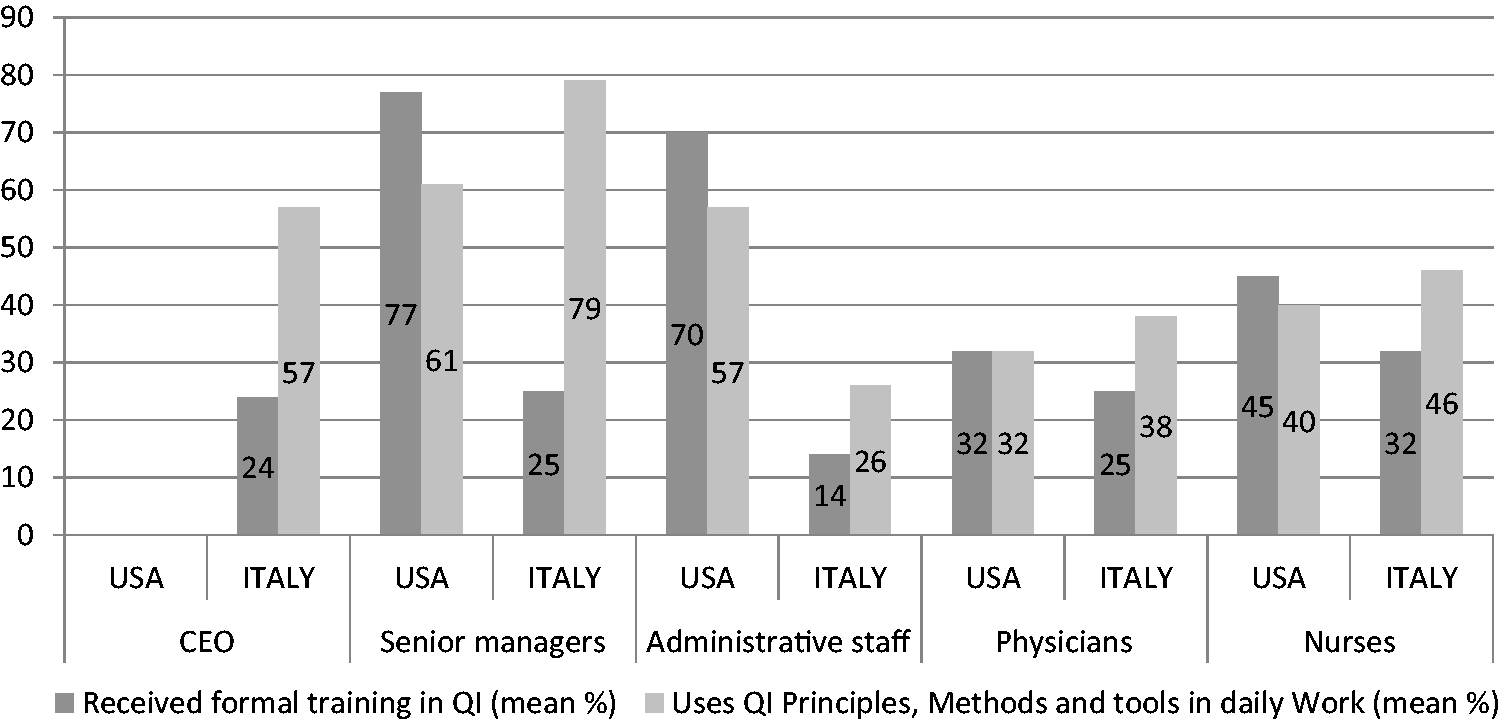
Staff involvement, training, and use of quality improvement (QI) methods.
Managers were asked to indicate their agreement regarding nine statements about the hospital quality practices and processes using a 5-point scale. To describe the phenomena we combined the top two response categories (strongly agree and agree) and the bottom three categories (neither agree nor disagree, disagree, and strongly disagree). Italian and US quality managers agreed or strongly agreed on many aspects of QI related to patient safety: “progress toward achieving hospital-wide QI goals is tracked and communicated to clinical staff” (95% US; 97% IT); “people and processes are in place to identify, analyze, and act upon all adverse events to prevent future occurrences” (94% US; 94% IT); “corrective action is taken if progress toward achieving hospital-wide QI goals is not adequate” (87% US; 92% IT); “people and processes are in place to identify, analyze, and act upon near misses to prevent future occurrences” (86% US; 85% IT); and “patient care processes are standardized, where and when appropriate” (80% US; 80% IT).
Differences in responses to the above questions between the two countries were small. In contrast, 79% of US CQOs perceived “little coordination of QI efforts across departments and workgroups” and 65% thought the hospital’s structure impeded such coordination compared to only 39% and 12% of Italian managers, respectively.
Both in the US and in Italy, relatively less attention has been paid to data dissemination to the public (34% US; 52% IT) and to involvement of patients and families by clinicians in QI efforts (65% US; 53% IT). This circumstance is at odds with what has been reported in the scientific literature.8,17,19,21 where it has been claimed that empowerment of patients would enhance patient satisfaction and compliance. In addition, the recent US Affordable Care Act mandates that hospitals set up patient advisory groups.
In this section the survey has also examined: (i) the scope of training programs specifically dedicated to quality; and (ii) the use QI methods and tools in the daily work. The data (Figure 1) show significant differences between Italy and the US regarding the typical target of these training programs: senior manager (77% US; 25% IT), administrative staff (70% US; 14% IT), physicians (32% US; 25% IT), and nurses (45% US; 32% IT).
Quality tools and methodologies
Table 4 shows the tools and methods used by Italian and American hospitals in QI projects. We asked quality managers to rate whether a specific quality tool/method was: “used widely or hospital-wide”, “used moderately” or “used minimally”. The most commonly used clinical QI strategies in Italy and the US were related to actions to prevent adverse drug events (70% US; 47% IT), clinical pathways (47% in both cases) and disease- or condition-specific QI projects (50% US; 39% IT). In general, the similarities between the two systems were:
Quality tools and methods.
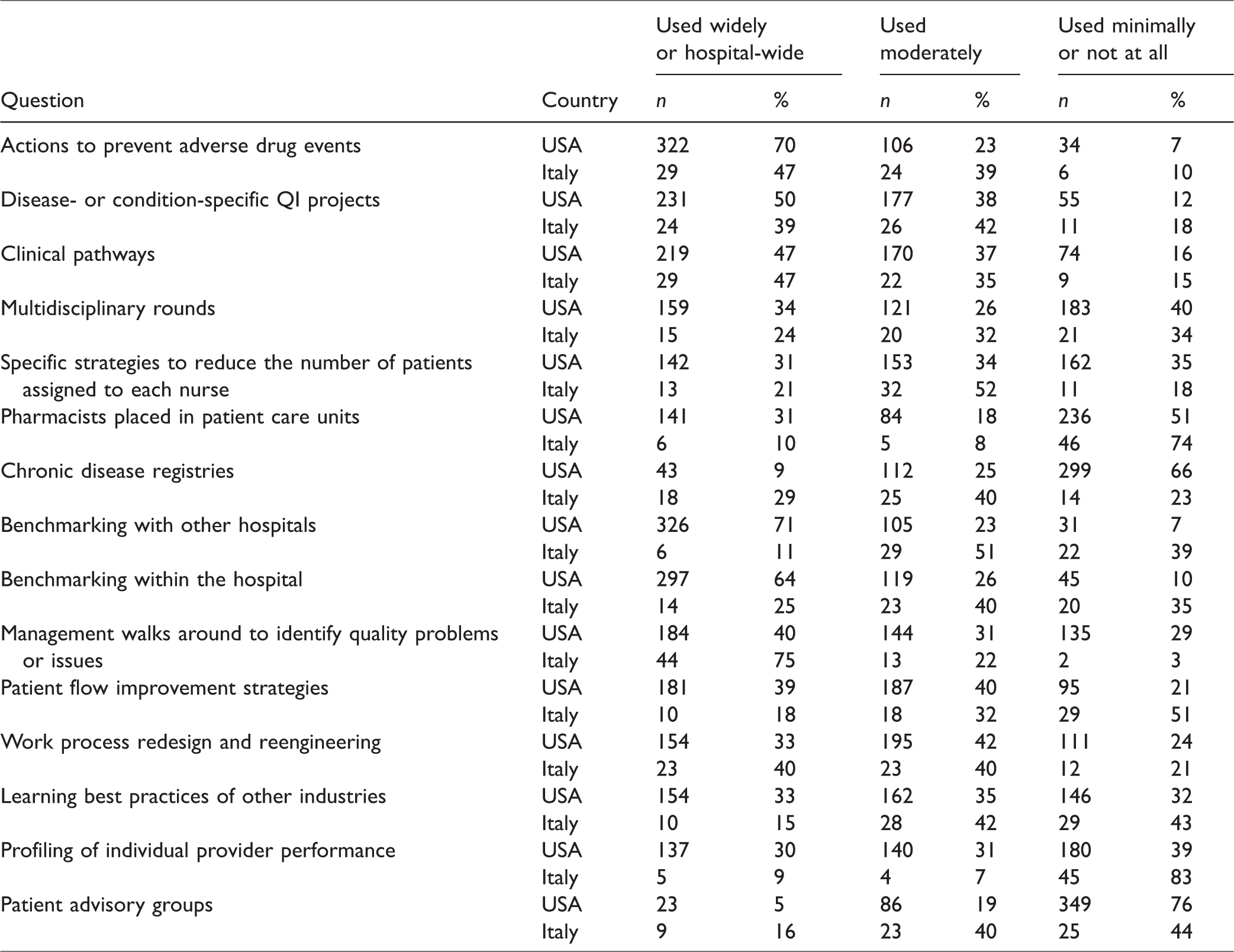
Clinical governance approaches and tools, such as disease-specific QI projects and clinical pathways. There is widespread awareness that clinical decision making must be supported by protocols and guidelines.
Drug management as a source of medical errors. In both countries, however, the role of pharmacists in QI is relatively small.
Adoption rates of QI techniques widely used in the manufacturing industry are very low: in Italy, only 6% of hospitals used statistical process control (SPC), 5% used six sigma and 10% used lean thinking techniques. Similar results were found in American hospitals: 19% SPC, 6% six sigma, and 6% Lean.
QI initiatives aimed to reduce nurses’ workloads were consistent in both countries. The shortage of nurses in both systems is of great concern36–38 particularly as the linkage between nurses’ shortage and quality of care has been demonstrated by several studies.27,39–41 Particularly the work of Aiken et al. 27 has clearly shown that the association between nursing and the quality and safety of hospital care is remarkably similar across Europe and the US.
In US hospitals, the nurse-to-patient ratios were significantly associated with two of the quality manager assessment questions. For the “patient care today compared with what it should be” question, the mean ratio for hospitals with high ratings (above or well above expectations) was 1 nurse to 5.0 patients while the mean ratio for hospitals with lower ratings was 1 nurse to 5.4 patients (p < .01). For the “patient satisfaction” question, the mean ratios were similar (1 nurse to 5.0 patients in hospitals with high ratings versus 1 nurse to 5.4 patients in those with lower ratings, p < .01). Nurse vacancy rates showed statistically significant relationships with three of five assessment questions. Mean vacancy rates for hospitals with high versus low ratings on the “patient care today versus what it should be” question were 5.7% and 8.3%, respectively (p < .001); mean rates for hospitals with high versus low ratings on the “family member” question were 6.2% and 9.6% (p < .001); and rates on the “patient satisfaction” question were 5.9% and 7.8% (p < .01).
In Italian hospitals, the nurse-to-bed ratios were significantly associated with two of the quality manager assessment questions. For the “patient care today compared with what it should be” question, the mean ratio for hospitals with high ratings (above or well above expectations) was 1.6, while the mean ratio for hospitals with lower ratings was 1.5 (p < .01). For the “Hospital focus on improving patient care has resulted in major performance gains” question, the mean nurses-to-beds ratios were 1.7 in hospitals with high ratings vs. 1.5 in those with lower ratings, p < .01).
A major difference between US and Italian hospitals was the use of data for benchmarking purposes. Italian hospitals typically were more reluctant to do benchmarking analysis both within the hospital and with other organizations. In contrast, for the US, benchmarking with other hospitals (70%) and benchmarking within the hospital (64%) were the top two QI activities widely used.
The survey also explored two other aspects of QI activities:
the influence of external institutions on hospital QI strategies; and the adoption of health information technology.
Quality managers were asked to characterize on a 5-point scale from very negative to very positive the influence of different nationally prominent QI initiatives and organizations on their hospitals’ QI efforts. In the US, the CMS’s QI Organizations and the IHI’s 100,000 Lives Campaign were, respectively, the organizations and initiatives most often cited (89%, 88%) by respondents as having had very positive or somewhat positive influence on their hospitals. In Italy, the Regions and the Ministry of Health were the organizations most often cited (respectively, 76%, 74%) as having had very positive or somewhat positive influence on their hospitals.
Figure 2 summarizes the results regarding the adoption of health information technology (HIT) tools in the US and Italy. In the US, quality managers reported that medication management systems (e.g. Pyxis) and picture archiving and communications systems (PACS) were the most commonly adopted HITs, having been implemented hospital-wide in 69% and 51% of hospitals, respectively. In Italy, the most commonly implemented information technologies were PACS (68%) and inpatient electronic medical record systems (EMRs) (37%). The data show that, despite intense debate about the possible impact of information technology on healthcare delivery, many information technologies had not spread widely in either country at the time of the surveys. It should be noted, however, that at least in the US the adoption of HITs, especially EMRs, has increased substantially since this time. 42

Health information technology.
Quality measures and information systems
Table 5 reports the quality measures most commonly reported to hospital boards of trustees, senior managers, department managers, clinical staff, and others employees in the US and Italy. b In Italy, the measures most commonly reported to boards of trustees included: patient satisfaction results (85% of hospitals); QI project results (79%); overall hospital risk-adjusted mortality rates; hospital-acquired infection rates (66%); and waiting times for outpatient clinic appointments (92%). In US hospitals, the most commonly reported measures were: patient satisfaction results (95%); QI project results (89%); hospital-acquired infection rates (84%); adverse events (82%); and medication error rates (81%).
Quality of care measures and reporting.

Quality measures that went unmonitored by more than 20% of US hospitals included: waiting times for outpatient clinic appointments (45%); unplanned ICU readmission rates (43%); procedure-specific mortality rates (35%); disease-specific mortality rates (30%); and emergency department diversion rates (23%). In Italy, more than 20% of hospitals did not measure: overall hospital risk-adjusted mortality rates (26%); adverse events (31%); medication error rates (37%); emergency department diversion rates (42%); disease-specific mortality rates (47%); near miss events (50%); unplanned hospital readmission rates (53%); procedure-specific mortality rates (69%); unplanned ICU readmission rates (71%); and individual physician profiles of quality performance (76%).
Italian hospitals exhibit a lower rate of reporting quality measures, many of which are reported only to the top managers. This restricted information flow is at odds with QI principles. Also, some indicators are not collected, such as: individual physician performance; errors in drug prescription; and patient flow indicators (e.g. “unplanned hospital readmission rates” or “ICU bumps”).
Italian hospitals pay greater attention than their American counterparts to waiting times. This may reflect, in part, greater concern about equity issues in Italy than in the US Furthermore, in Italy, waiting time is a critical issue since it represents a way of “rationing” the demand for care, which is free at the point of consumption.
Assessment of patient care quality
The last section of the questionnaire aimed to evaluate the performance of QI systems in hospitals (Table 6). The CQOs were asked to evaluate:
Quality managers' assessments of hospital quality.

the quality of patient care provided at their hospital; and
the impact of the different QI initiatives put in place.
CQOs were asked to rate patient care today at their hospitals compared with what they thought it should be, using a 5-point scale ranging from well below expectations to well above expectations. In the US, 36% of quality managers said that patient care was either above or well above their expectations, while in Italy only 3% responded that way, with 80% responding that patient care met their expectations.
When asked to rate patient care today compared with three years ago, using a 5-point scale ranging from “much worse” to “much better,” 87% of American CQOs and 64% of Italian CQOs, respectively, said that care was better or much better compared to the past. Only 10% of American managers versus 36% of Italian managers reported that patient care today is the same compared to three years ago.
About the same proportion of managers in the US and Italy (68% vs. 71%) agreed or strongly agreed that they would feel comfortable having a family member treated at the hospital without being present to monitor the care. However, only 28% in the US agreed or strongly agreed that patient satisfaction was at the level where it should be compared to 87% of respondents in Italy who felt this way. Quality managers in both countries perceived QI activities as having produced positive or very positive impacts on several organizational areas in their hospitals:
patient care outcomes (97% in US; 98% in Italy); staff motivation and skills (86% in US; 100% in Italy); productivity (70% in US; 93% in Italy); and physician–nurse relationships (68% in US; 73% in Italy).
Discussion
As mentioned in the introduction, Italian and American hospitals, although in two different time frames, have both been urged by external forces to extensively redesign their QI strategies in order to keep up with a general expectation (from policy makers and citizens) to improve the overall quality of care.
In both nations quality issues have gained traction among hospital managers such that: (1) QI is explicitly mentioned in hospital strategic plans; (2) quality-related goals are systematically included in the budgeting process; (3) clinicians are becoming more aware of the necessity to change processes and behaviors to improve the safety and quality of healthcare delivery; and (4) there is shared agreement on the critical importance of standardizing clinical decision making and patient care processes through the adoption of clinical pathways.
However, the study shows differences between the two systems that offer interesting material to draw some conclusions on which models and tools are effective in improving quality of care. As explained in detail in the methodology session, we support these conclusions in two ways: we have compared the features of the QI systems adopted in the two countries with (i) the standards and best practices present in the scientific literature and; (ii) the evaluations expressed by CQOs.
First, on average, American hospitals have a less fragmented and more system-wide approach to QI, specifically:
the scope of responsibilities for quality managers is wider (Cfr. Table 1); quality metrics refer to different dimensions (such as patient safety and patient flows logistics) and are diffused and communicated hospital-wide (Cfr. Table 4); and QI training and programs target a wider spectrum of categories, including, for example, the administrative staff (Cfr. Figure 1).
We conclude that American QI systems are, in this perspective, better off since there is a strong body of literature43–49 providing evidence that a system-wide and integrated approach to quality has a significant impact on overall organizational performance.
It is worth noting, in this benchmarking analysis of the two systems, that the siloed approach found in some Italian hospitals might be explained by the mainly public nature of the Italian healthcare system; in fact, many features of Italian healthcare management practices are inspired by a bureaucratic approach to dealing with new issues and problems through interventions in the formal organizational structure. For example, when the problem of medical litigation arose, the Minister of Health recommended that organizations set up a specific organizational unit dedicated to dealing with this area (see, for example, the National Health Plan 2009–2011). The same is true for operations management, which is an area of growing importance. 50 Some Italian regions (e.g. Tuscany and Lombardy) have required hospitals to set up offices dedicated to patient flow management. This bureaucratic thinking (“we have a problem, let’s set up an office to deal with it”) introduces the risk of creating silos in the overall organization resulting in poor communication among different units and adoption of only a partial approach to solving problems.
On the other hand, Italian hospital organizational structure designed around the so-called clinical directorates (CDs) seems, based on our findings, to work well. Italian CQOs state, on average, that they not experience problems of coordination of QI efforts across departments and workgroups and they do not perceive that the current hospital’s structure and work processes impede coordination across departments and workgroups (Table 2). Italian CDs are “intermediate organizational arrangements through which defined parts of larger hospitals’ health services are managed” and have been part of the Italian National Health Service (INHS) by law since the major reform of, 1992.51,52 Despite initial resistance to change, the new organizational model, when actually applied, c has been effective in: (1) improving hospital clinical governance through better integration of clinical pathways; and (2) exploiting economies of scale and scope, by sharing resources (beds, OR, ambulatories, etc.), technologies, and ancillary staff. 51 Thus, CDs appear to mitigate some of the limitations of the bureaucratic approach.
Finally, in both countries the shortage of nurses is considered a major impediment to the improvement of patient safety and quality. Data from the surveys clearly show a significant positive correlation between nurse-to-patient ratios and quality managers’ perceptions about the levels of safety and quality.
Policy and managerial implications
In both countries the concept of QI is now well accepted and both surveys show a cohesive organizational culture that embraced QI as a strategic priority. For health care managers and policy makers, it is important to understand which organizational characteristics actually favor QI and safety. In this sense the comparative analysis of the two countries provides useful insights.
Our study, as well as the literature on QI, suggests several criteria for policymakers and executives to use in selecting improvement strategies. First, given that quality is a multi-dimensional concept,3,4 it is essential that a QI system, if it is to be comprehensive, include strategies that address all dimensions of quality. The most widely recognized dimensions of quality are represented by the IOM’s six aims: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity. 13 Furthermore, we believe that a healthcare organization should develop a strategic plan specifying important dimensions of quality and design improvement strategies that are aligned with these priorities. 53 A second criterion to consider in selecting improvement strategies is the impact the strategy is likely to have on quality of care. For example, the impact of nursing on quality was highly ranked in our study, thus calling for strategies aiming to achieve better patient-to-nurse ratios and for innovations in health care supply chain54 management that reduce nursing time dedicated to logistical activities. Third, policymakers and executives should consider implementing strategies that address areas in which performance is lacking. In our study, these included extended responsibilities such as clinical risk management for QI offices and widespread dissemination of performance feedback among Italian hospitals, organizational structures to facilitate coordination among US hospitals, and involvement of patients in QI strategy development in both countries.
A final relevant message of our study is that, in order to be successful, any QI methodology or tool must be highly integrated with the other organizational components. For example, the Italian CDs model (indicated in the survey as an effective organizational design to favor clinical governance and multidisciplinary collaboration) must be managerially sustained through, for example, the appointment of administrators and operations managers supporting the role of the Chair, and developing grouping of clinical units consistent with these goals. The hospital information architecture (more advanced and complete in the case of American hospitals) must be aligned to the new managerial models, such as the patient-centered healthcare model in Italy and the accountable care model in the US, that call for a more integrated approach to care where assets and resources are shared by the different hospital clinical specialties. A limitation of the study is that the data are self-reported, which is inherent in surveys conducted by questionnaire. A second limitation is the low response rates in both surveys. However, while a survey with a low response rate will have less precision but not necessarily greater bias, it still can yield informative findings; this is particularly true if there are large numbers of respondents, as is the case in these two surveys (see Meterko et al.29). A third limitation is that the questionnaires were sent only to top hospital managers responsible for QI and it is unknown whether their perceptions and opinions were shared by clinicians and patients in their institutions. Nevertheless, the approach and methods used in this study are sufficiently robust to offer a broad picture of the QI strategies actually used in Italian and American hospitals and the similarities and differences that exist between the two systems, thus providing useful insights to managers and policy makers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stefano Villa has been recipient of a Fulbright Research Scholarship 2017-2018.