
Abstract
Introduction
Process mapping provides insight into systems and processes in which improvement interventions are introduced and is seen as useful in healthcare quality improvement projects. There is little empirical evidence on the use of process mapping in healthcare practice. This study advances understanding of the benefits and success factors of process mapping within quality improvement projects.
Methods
Eight quality improvement projects were purposively selected from different healthcare settings within the UK’s National Health Service. Data were gathered from multiple data-sources, including interviews exploring participants’ experience of using process mapping in their projects and perceptions of benefits and challenges related to its use. These were analysed using inductive analysis.
Results
Eight key benefits related to process mapping use were reported by participants (gathering a shared understanding of the reality; identifying improvement opportunities; engaging stakeholders in the project; defining project's objectives; monitoring project progress; learning; increased empathy; simplicity of the method) and five factors related to successful process mapping exercises (simple and appropriate visual representation, information gathered from multiple stakeholders, facilitator’s experience and soft skills, basic training, iterative use of process mapping throughout the project).
Conclusions
Findings highlight benefits and versatility of process mapping and provide practical suggestions to improve its use in practice.
Introduction
Improving the quality of care in a context of increased complexity and reduced resources is a significant global challenge. Recent evidence shows that most of the quality and safety problems in healthcare are caused by operational and systems criticalities.1–5 System redesign and the adoption of process-oriented management practices are therefore crucial to improve patients’ outcomes and efficiency of care delivery.5–10 Over the last 15 years, healthcare systems have drawn on tools and methods from industrial engineering to improve quality and safety.11–15 One such method, process mapping (PM) – also commonly referred to as Process Modelling –, focuses on the systems and processes into which new interventions are introduced. Within quality improvement (QI) projects, PM might be used in conjunction with visual management (VM) tools or other tools typical of industrial engineering to gain a better understanding of current practice and to design enhanced processes. 16
Since it was first introduced, the term PM has been used to designate a number of approaches and techniques. In the present study, the term refers to the ‘entire approach that leads to a holistic understanding of the process under review’. 16 By reviewing methodological literature on PM, we found that this approach includes the following five phases: PM organization and process identification, information gathering, map generation, process analysis and taking improvement forward.7,16–20 This concept of PM goes beyond the technical aspects related to the generation of the process map (visual representation of the process under analysis) 16 and embraces the social aspects involved in the PM process, such as interactions between participants.
Focusing on this definition of PM, we have conducted a review of empirical literature describing the use of PM in healthcare, which aimed to improve current knowledge on context of use, benefits and quality of reported use of PM in healthcare. This study has fed into a protocol for a full systematic review which is now under way. 21
Reviewed studies have demonstrated that within QI projects, PM is used in a variety of healthcare settings and applications, as a stand-alone methodology or as part of techniques such as lean manufacturing, six sigma, failure mode effects analysis (FMEA), or costing approaches (e.g. TDABC – time-driven activity-based costing).11–14
Studies have also highlighted that PM is particularly useful for mapping complex healthcare processes as it provides improvement teams with insight into ‘work as is’ rather than ‘work as imagined’.22–26 Similar to VM tools, typical of Lean interventions, PM can be seen as a communication tool supporting engagement and collaboration of healthcare professionals within improvement projects.27,28 However, in contrast to other techniques, PM plays a unique role within change processes in providing a shared understanding of complex systems in a way which is readily understandable by a wide range of stakeholders.
Although the informed and systematic use of PM in healthcare is advocated by researchers and practitioners,29–32 it is not routinely used in improvement approaches within healthcare organizations.31–34 Early findings from our systematic literature review 21 show that, despite the number of studies reporting on the use of PM in healthcare increasing during the last 10 years, there are still few examples of documented use of this tool in the healthcare sector.
The application in the healthcare setting of tools and approaches which are well established in other industries, such as PDSA, statistical process control or lean, is often difficult. 35 This is partly due to the environment, culture and requirements of healthcare, which greatly differ from other service and manufacturing sectors. 31 Healthcare processes are highly complex, variable and dynamic. The complexity of these processes is increased by the fact that they usually take place across different medical departments or even different organizations,36,37 thus involving a variety of stakeholders, from patients to highly specialized professional groups, each with diverse backgrounds and motivations.
The wide range of stakeholders involved and the discretionary nature of clinical decision making, make the success of a QI initiative heavily dependent on the engagement of all the participants of the process of care and their effective communication.8,32,38–40
Research findings show that to embrace the complexity characterizing healthcare systems, it is important to unpack the ‘black box’ of QI approaches in order to understand how they work in reality and how context factors such as local culture, leadership styles, and team experience of QI can influence their effective use in practice.35,41
To address this issue, Kaplan et al. 41 have developed the MUSIQ (model for understanding success in quality) framework analysing context factors influencing healthcare QI projects and their relationships. 41 However, there is little empirical research on how these context factors may influence the use of PM within healthcare improvement initiatives.
Previous literature describes only isolated empirical implementations of PM in healthcare and the analysis of articles reviewed in our systematic literature review 21 shows that in most of these studies, the way in which PM exercises are conducted is poorly documented.42,43 A few papers in the healthcare literature provide suggestions on how to conduct a PM exercise.18–20 Detailed practical guidelines for PM both in the healthcare 7 and non-healthcare16,17 field have also been developed by experts and practitioners. However, these studies assume a specific perspective and do not explicitly take into account the context in which improvement interventions are introduced.
Only one study has derived PM success factors from empirical research on real projects, drawing on case-studies of nine PM projects in three Australian organizations. 44 However, this study was outside healthcare and the perspectives analysed by the researchers were limited to modellers and project sponsors.
The lack of knowledge of QI methods and their applicability in healthcare is an obstacle to their adoption and embedding into practice. 45
Improved empirical understanding of the use of PM within QI projects is therefore required to ensure that people working in the healthcare environment are aware of the opportunities and benefits offered by the adoption of this versatile and simple technique. Such research can raise awareness on the value of PM as QI method and inform its practical implementation.
To date, no exploratory study on the use of PM in healthcare based on a systematic analysis of practice has been conducted. There is therefore a need to explore the evidence of benefits and challenges of PM use in order to support its adoption in healthcare.
In this study, we investigated the use of PM in a sample of QI projects conducted by improvement teams in the UK’s National Health Service (NHS) to understand the main benefits achieved by the use of PM in healthcare practice as well as the main success factors of PM within QI projects.
Methods
We designed the study in the form of inductive qualitative methods. We used an iterative study design characterized by cycles of simultaneous data collection and analysis. 46
Setting
This work was conducted within the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care Northwest London programme (CLAHRC NWL). This aims to improve the quality of care and patients outcomes by supporting the effective translation of research evidence into practice in the NHS and social care.47,48
Ethics
The study was reviewed and approved by the NHS Health Research Authority (IRAS project ID 188851). All respondents gave their informed consent to participate in the interviews. Participation was voluntarily and confidentiality protected. Participants were identified by peer nomination and recruited through email.
Sampling
Data were collected by purposively sampling QI projects and interviews’ participants on theoretical grounds.49,50
The sampling strategy aimed to maximize the variation between QI projects and interviews’ participants. 51
Sampling and analysis continued until data saturation was reached.46,52
Observations of PM workshops conducted during the sampled QI projects were also performed when the project team agreed.
QI projects sampling
QI projects were selected from a pool of 22 CLAHRC NWL QI projects, which last 20 months and cover a range of healthcare interventions (online Appendix).
Eight QI projects adopting PM techniques were selected to represent different care settings (primary, secondary, community or a combination) and levels of complexity of the process under investigation (online Appendix). We used the process complexity as criterion for our sampling because as mentioned in Introduction, the level of complexity may influence the benefits of PM perceived by team members and the challenges that they may encounter during a QI project. The level of complexity was assessed according to two dimensions 53 : (i) the number of organizational units involved in the process being mapped (e.g. different hospital departments); (ii) the number of different professional groups involved in the process being mapped. The resulting classification of QI projects was agreed among the research team and verified by key informants, including project leaders and QI experts from CLAHRC, project managers, clinical leaders and other team members.
Interviews’ participants and PM exercises’ observations sampling
Sampling from team was performed to provide a broad range of relevant perspectives and to increase generalizability of findings. 51
Key informants were asked to identify QI team members for interview with different roles in the QI project and different backgrounds (e.g. project managers, physicians, patients), as well as their experience of PM (Table 1).
Interviewees.
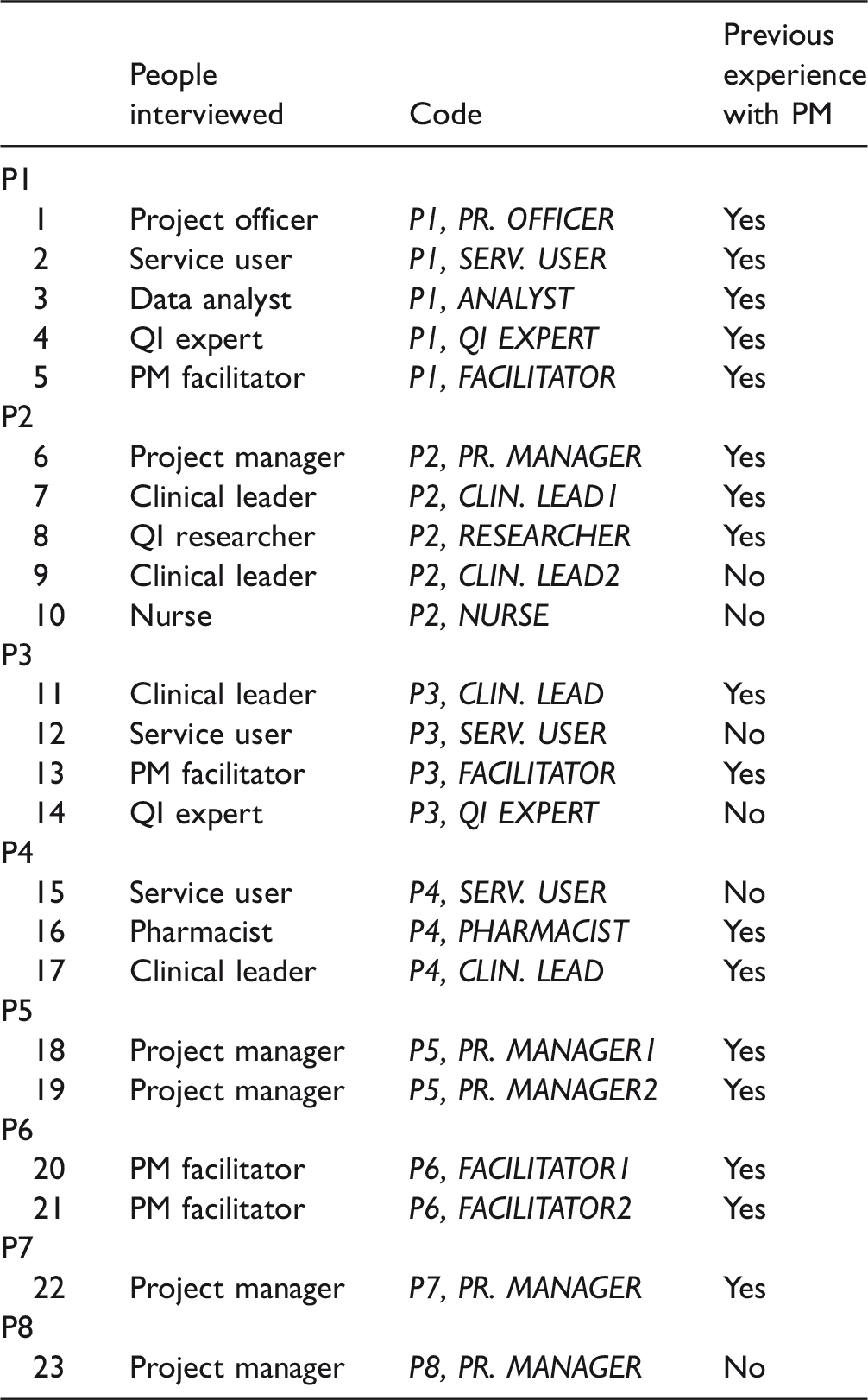
PM: process mapping; QI: quality improvement.
Data collection
Data were collected by two authors (GA, LL) between March 2016 and October 2016 from multiple sources, including interviews, project documents (project application forms, process maps, project review minutes and notes, project progress and final reports, project presentations), observations, and focus groups. The timeline of QI projects and data collection is represented in the online Appendix.
At the start of the research, informal conversations and two focus groups were held to identify the main issues that the QI teams were experiencing with PM, clarify the study research questions, identify project characteristics required for theoretical sampling and developing the interview guide. The latter was also informed by literature and progressively refined during the study.
Twenty-three semi-structured interviews were conducted by two interviewers. Interviews took about 45–60 min each and were conducted primarily in person (two telephone and two Skype). The themes explored included: participants’ experience of PM, the way in which PM was used in the project and for which purpose, its contribution to the success of the initiative, key elements that helped the PM exercise as well as problems and challenges related to its use. Interviews were audio recorded, anonymized and transcribed by independent professional transcriptionists.
Semi-structured observations of three PM sessions from two QI projects (P5, P7) were conducted to capture real-time data with the objective to gain a sense of how process maps were generated as well as of how participants were behaving and interacting. 54 The choice of the three PM sessions to observe was opportunistic, as only three PM sessions were conducted within the sampled QI projects during the observation period for which permission to observe was granted. Observation notes were taken during the PM sessions, and then transcribed and discussed among the research team. A large amount of documentation produced during all the stages of CLAHRC projects was also analysed in order to have access to projects’ details and other relevant contextual information. Observations and documentation were used only to document and corroborate interview data, which was the main input to data analysis.
Data analysis
Qualitative data analysis was guided by constant comparative techniques. 55 NVivo software was used for the analysis of the interviews. One author (GA) started to become familiarized with the interviews’ text by reading (and re-reading) the transcriptions and developed preliminary open codes. Two authors in parallel (GA, LL) progressively combined preliminary codes into sub-categories, and then grouped these into broader categories. The code structure was iteratively developed as further interviews were added to the dataset. The core categorical scheme that emerged was then applied to all the dataset. During this process, the analysis was documented in Memos with explicit links to source text. Links between categories and emerging themes were progressively developed and agreed among authors to check for consistency and validation.55,56
Emerging themes were progressively refined by comparing evidence from data with existing literature exploring in particular: the influence of context factors on the success of healthcare improvement, 26 methodological literature and practical guidelines on PM in healthcare7,18–20 and non-healthcare field,16,17 and PM success factors derived from a structured analysis of real projects outside the healthcare setting. 44
Findings
Results are presented according to: (i) benefits of PM within QI projects, (ii) success factors and challenges of PM within QI projects.
Benefits of PM within QI projects
The benefits related to the use of PM are grouped in eight major subcategories as detailed in Table 2 along with representative quotations.
The benefits of process mapping for QI project.
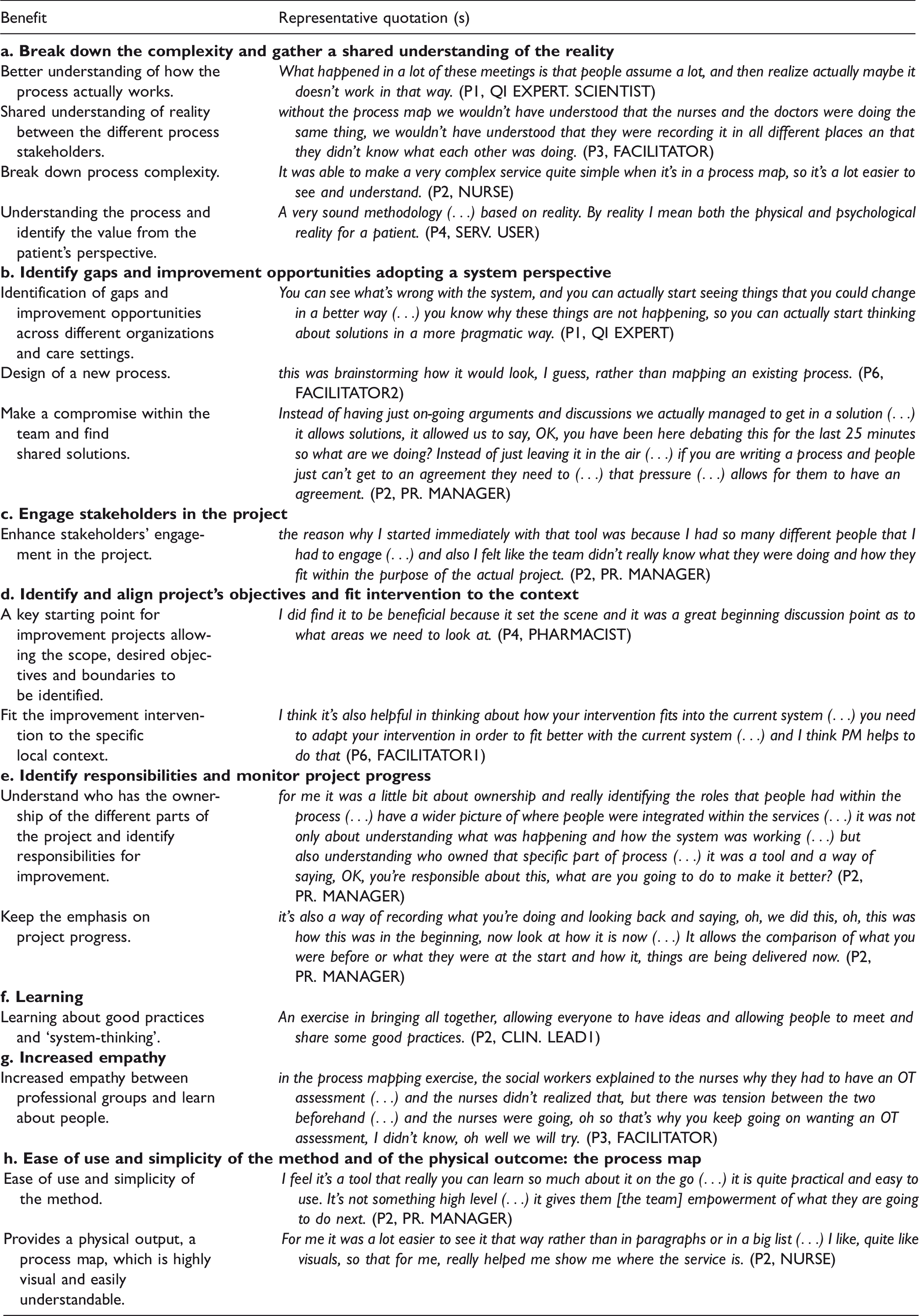
QI: quality improvement; process mapping.
According to interviewees, the main benefits of PM in healthcare are its capacity to break down the complexity of healthcare processes and provide a shared understanding of the reality amongst a composite group of stakeholders (Table 2. a). In the analysed QI projects, PM was usually (7/8 projects) conducted during facilitated multidisciplinary workshops. In many cases, this was the first time that health professionals working on the same care process talked each other: It’s a very useful stakeholder exercise, and people who maybe don’t usually meet (…) I think the greatest value is in the stakeholders all being in the same room and sharing their experience. (P2, CLIN. LEAD1)
People joining the PM exercise also stated that visually representing the process through Process Maps, was very helpful to support multidisciplinary communication during the process map generation and later during the project. The physical representation of processes was also useful to help disseminate and document the process after the project completion (Table 2. h).
According to PM participants, the use of PM in the early stages of a project allowed to effectively engage process stakeholders by involving them in the identification and refinement of project’ objectives. This helped QI projects’ teams to align project’ objectives with individual objectives, gain a better understanding of roles and responsibilities, and to adapt the improvement intervention to fit better with the local context (Table 2. c,d,e). Team members also reported that the use of PM throughout the different stages of the QI projects allowed to monitor progress and further inform change actions (Table 2. f).
Finally, interviewees reported that the social interaction of process stakeholders during the PM exercise helped increase empathy between professional groups and to decrease the resistance to change, thus allowing participants to reach agreement and arrive at a shared solution (Table 2b, g). Everybody has an opinion and those opinions are expressed and at the end of the meeting we’ve found a solution. (P1, SERV. USER) Instead of having just ongoing arguments and discussions we actually managed to get a solution and in that way that’s what felt about the process map. (P2, PR. MANAGER)
Success factors of PM within QI projects
Following the analysis of empirical data and their comparison with established literature (Data analysis), we have identified five factors related to successful PM exercises: (i) simple and appropriate visual representation, (ii) information gathered from multiple stakeholders, (iii) facilitator’s experience and soft skills, (iv) basic training, (v) iterative use of PM throughout the project.
Each PM success factor, along with examples of quotations from interviews, is described below.
Simple and appropriate visual representation
The visual representation of the process map emerged as a very important factor not only to engage participants and support the debate during PM workshops, but also for its further use during the project, such as feedback and validation, or dissemination to different organizational levels. Our data suggested that the simplicity of the methods used is crucial for stakeholder engagement, in particular clinical staff. I think one should not make it too technical for participants, otherwise it’s actually off putting. Most people in healthcare, like myself and busy clinicians, want to be able to just put out our ideas as commissioners rather than being forced to adopt kind of certain project management rules, they’re very off putting for some people. (P2, CLIN. LEAD1) The language needs to make sense to the team you’re talking to (…) What I like sometimes is actually when I need to share it with wider people like project managers, then it is good to use the standard signage for process mapping (…) What I find important is ‘de-scaring’ people (…) If I’m working with the local nursing team, I don’t want it to look too professional … So if I would do it with the local nursing team on a ward, I would maybe actually do it by hand (…) If I’m doing pretty boxes and layout, (…) possibly my nursing team on the ward will say, gosh, I never have the time to do something like that, so I can’t do process mapping. (P7, PR. MANAGER)
Information gathered from multiple stakeholders
Different data sources (stakeholders, databases, documentation) and data collection methods (observations, interviews) may be adopted to build a process map.
36
However, in our sample QI projects, participants pointed to the experience of people who actually do the work as the main information source. They’ve [facilitators] got to be able to explain and facilitate and document and capture what’s being discussed, but the thing to make sure you actually get the right information is having the right people. So it’s about their knowledge, the team structure, basically those things. (P4, CLIN. LEAD)
The involvement of stakeholders who can provide insights into actual practices is therefore essential to build a shared understanding between participants. However, many challenges were experienced in releasing staff from their daily responsibilities and engaging them in PM sessions. It’s always a challenge to persuade people it’s worthwhile giving up the time to do it, yeah, because you’re taking them away from clinical and patient facing time. (P3, FACILITATOR)
Facilitator’s experience and soft skills
While facilitators' deep knowledge of the process being mapped was not perceived as important to the success of the PM exercise, their experience with PM was reported as crucial. You need somebody who is clearly experienced in the methodology, particularly if you’re working with a group such as us who haven’t really done any formal quality improvement. (P2, CLIN. LEAD1) So sometimes people can be far too serious about things, and to have a little bit of fun with it, and to have a little bit of laughter brought in, and it helps everybody I think because they all feel good about what they’re doing. (P1, SERV. USER) Clinicians are very time poor people and investing two or three hours in a process that they haven’t quite understood why they should be wanting to do this will make it fail. Whereas (…) getting people to understand that it’s time consuming but worthwhile is a challenge, therefore a good facilitator to take that through, is incredibly crucial to the process. (P2, CLIN. LEAD1)
Basic training
Team members (with the exception of facilitators) demonstrated scarce knowledge of the range of charting software available and of the PM techniques. According to team members interviewed, training should be straightforward in order to allow people with no QI background (and little time) to understand the main concepts of PM. Providing practical examples to clarify the meaning of PM symbols to be used in the session was found to be useful to this aim.
Iterative use of PM throughout the project
Interviewees believed that the continuous revision and use of PM throughout the project is a fundamental requirement for its effective use within a QI project. I actually think that if you had somebody doing that who doesn’t know what they’re doing and isn’t going to put the work in afterwards and isn’t going to use the map with the team afterwards, it’s a waste of time (…) let’s map and then let’s constantly use that map, let’s remind ourselves why this is the intervention that we’re looking at. (P3, FACILITATOR)
Discussion
This work is the first empirical study exploring the use of PM in healthcare throughout a rigorous analysis of QI practice. Using a rich qualitative dataset based on the experience reported by a range of QI team members, we have identified the main benefits of PM within QI projects and success factors supporting its effective use.
Taking the PM process as a whole, in which the development of the process map is only one step, it emerges that there are benefits attributable to PM that may not be as readily apparent. In particular, our findings suggest that the main benefits derived from the use of PM within healthcare QI projects are not related to the graphical representation of the process, but to the social interactions between participants during all the PM process. In a health care context, this social role played by PM is maybe especially important due to the high number of participants typically involved in care processes, each with diverse motivations and specific knowledge of the process under analysis. Enhancing communication and gathering consensus among process stakeholders through their full and informed involvement is therefore a key success factor for the successful implementation of improvement projects.32,39
Our research corroborates previous findings highlighting how PM serves a crucial role within healthcare as an ‘ice-breaker’, fostering communication among healthcare professionals with highly specialized clinical knowledge and different representations of or attitudes towards the process in question.57,58 These findings confirm previous theories about QI implementation and change management in healthcare pointing to the need for consistent control over project progress and the importance of defining shared objectives and enhancing stakeholder engagement by involving them in the early stages of projects.59–61
Compared to existing healthcare literature on PM,7,18–20 mainly developed by QI experts and practitioners, this study has been informed by investigation of empirical cases, focusing on stakeholders with different perspectives and roles in PM exercises. This has allowed aspects overlooked by prior literature to emerge. For example, QI team members have reported how involvement in the PM exercise helped them to increase their knowledge about this technique and their empathetic connection with colleagues and other healthcare professionals working in the same process.
Our findings are aligned with previous QI research reporting on the influence of contextual factors on the success of QI projects. We have enriched these findings by highlighting specific issues related to the use of PM, as drawn from actual team experience. 34
We found that effective use of QI methods within complex multi-stakeholder healthcare systems is influenced not only by the methods used to conduct a PM exercise (techniques, tools, data collection, etc.), but also by the context in which they are used.
For example, we found that as knowledge and practice related to care processes is fragmented across different organizations and professional groups, involvement in the PM exercise of the right people is key.
As a consequence, the role of PM facilitators also emerges as much more significant in healthcare compared to findings from the existing literature, which focuses on other industries. 44 Their capacity to breakdown the complexity of healthcare processes and align the scope of the exercise with the scope of the project is perceived as very important for guiding QI teams that often have no previous experience of these techniques. Together with technical knowledge about PM techniques, soft skills of facilitators emerge as crucial for involving and motivating stakeholders across organizational boundaries.
Moreover, our findings reveal that while for the team members a deep knowledge of PM techniques is not perceived as essential, previous experience with QI methods is a relevant success factor. This confirms findings in research on QI 41 that highlight how previous experience positively impacts not only on the technical knowledge of PM methods, but also on the engagement of the team in the project, as it increases awareness of the benefits that are achievable.
From a practical perspective, this study helps to increase the healthcare community’s awareness of the benefits that a versatile and simple tool such as PM could provide if appropriately used throughout QI projects. In doing so, it encourages healthcare practitioners to use PM within QI projects and highlights relevant aspects to take into consideration to improve the adoption of PM in practice.
Limitations
The main limitation of this work is that most of the projects included in the study have used the same methodological approach to PM, based on multi-stakeholders meetings to generate the process maps. In only one project (P8), the process map was drawn by the QI team using data from observations. Further research is needed to test whether our findings hold in QI projects developed by teams using different approaches to conducting the PM exercise, for example by following the patients, or when PM is used within other techniques such as six-sigma or lean.
Within our QI project cases, in order to increase generalizability of the findings, our sampling strategy sought to develop a comprehensive understanding of the use of PM from different perspectives, by interviewing multiple stakeholders with different roles in each project and with different backgrounds.
Another limitation of this study is the potential for social desirability bias of responses, as some participants may have responded in ways that were seen as more desirable to CLAHRC NWL researchers they were familiar with (JR and LL). This bias was mitigated by the fact that the main researcher responsible for participants’ recruitment and data collection (GA) was new to CLAHRC NWL and unknown to the majority of interviewees.
Interviewer bias could also have influenced respondents and distorted the outcome of the interview. This bias was reduced by the use of fixed-wording questions and of two interviewers with different backgrounds and training.62,63
As PM is often part of a broader improvement initiative, participants’ experience could have been influenced by the wider complex context of the change process. 51 We have addressed this risk in the analysis phase and designed interviews questions to specify areas of interest.
Many research techniques were used to limit bias in the analysis phase and ensure trustworthiness and validity of results.64,65 These included audiorecording and independent professional preparation of the transcripts, a rigorous documentation of analysis, persistent and prolonged engagement with data, peer debriefing, data and analytic triangulation. 49 For example, the use of observations balanced the retrospective nature of interviews 54 and the involvement of QI experts in focus groups conducted during the study (from the definition of the research question to the validation of results) helped to guide the analysis and further validate findings. Moreover, the diverse background of researchers, including experienced improvement scientists, ensured multiple perspective and consistency of results.
Conclusions
There is no single recipe-book of PM techniques to ensure success – its use in practice depends heavily on the scope of the project, on the setting and organizational and behavioural aspects. However, PM project team members reported that PM was a pivotal tool when applied iteratively through the lifecycle of healthcare QI projects. The more complex a process, the more the clinical and organizational knowledge about it is likely to be fragmented, and the more likely that stakeholder objectives and interests may conflict. In these circumstances, QI projects are especially likely to benefit from PM.
These features, together with the relative ease of the method, make PM a promising technique in healthcare improvement, where more sophisticated tools and techniques often fail.
Supplemental Material
Supplemental material for The use of process mapping in healthcare quality improvement projects
Supplemental material for The use of process mapping in healthcare quality improvement projects by Grazia Antonacci, Julie E Reed, Laura Lennox and James Barlow in Health Services Management Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care Northwest London (NIHR CLAHRC Northwest London). The views expressed in this article are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Supplementary material
Supplementary material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.