
Abstract
This study aims to determine the hospital practices implemented before, during, and after birth in Turkey, and to identify the support to families during this process. Purposive sampling was used in the study to identify the hospitals to be surveyed. Ankara, İstanbul, and İzmir, the provinces with the highest number of hospitals in Turkey, were selected for the collection of data. There were 178 eligible private hospitals in these provinces. The questionnaire form of the Canadian Hospitals Maternity Policies and Practices Survey was used to collect data and the necessary permissions were obtained. There are many restrictions and variations in maternity-related hospital practices in Turkey. 71.4% of the responding private hospitals identified themselves as baby-friendly. 57.1% had a policy facilitating families being together immediately after birth, 39.5% encouraged the presence of the father in the delivery room. 44.9% did not have any policy for assessing women who were going home to potentially violent situations. Eighty-five percent reported that they did not have a written policy or guidelines about procedures regarding labor, birth, or postpartum periods. This study recommended that private hospitals should review their maternal practices and routines in an evidence-based way that helps parents, culturally sensitive standards for mothers should be developed and supervised by related health authorities, and structures should be created to effectively deal with patients’ complaints.
Introduction
Family-centered maternity care considers family as a whole and delivers an evidence-based service. Family support especially for women is of considerable importance in this context as it has positive effects on maternal and neonatal health. 1 The growing interest in family support in family-centered care and birth and the increasing importance of the evidence-based medicine have led to a redesign of hospital policies and routines in many developed countries. Nevertheless, many developing countries put more focus on improving the access of women with fatal complications to emergency obstetric care than the quality of the service for normal childbirth. In these countries it is rarely questioned whether childbirth routines rely on evidence-based practices or whether healthy outcomes are achieved. This situation may be due to the presence of varied mechanisms which make it harder to evaluate the quality of health and update clinical practices.
Complications during pregnancy, labor, and postpartum are the leading causes of death and disabilities among women of reproductive age in Turkey. It is a really challenging issue for the health policies to provide healthcare for newborns and women during pregnancy, childbirth, and postpartum in a timely and effective manner while reducing inequalities. Maternal mortality is closely associated with the quality of the delivery of reproductive health service. The birth rate at the health facilities in Turkey is 97%. 2
In the health system of Turkey, the Ministry of Health is responsible for providing quality, standard, safe and efficient service for clients and ensuring unity in practice through health personnel all over the country. Guidelines such as Prenatal Health Care Management Guideline, Postpartum Care Management Guideline, and Emergency Obstetrics Care Management Guideline have been prepared and revised by related science commissions, associations, or organizations within this scope. However, these guidelines are not unchangeable rules or legal standards for the services offered to patients. The Turkish Ministry of Health is authorized to develop policies and procedures on pregnancy, labor, and postpartum services. These policies and procedures are implemented in hospitals affiliated with the Ministry of Health. However, there are differences in private hospitals with regard to the application of these policies and procedures. They design their practices depending on their own vision and policies. For this reason there can be variations of practices in private hospitals throughout the country.
The proportion of people preferring the private sector for maternity services is rapidly increasing in Turkey with the rising level of education and economic welfare. Although policies and guidelines for common purposes are available at hospitals, there are no specific guidelines for maternity care. There is a need to reduce the number of unnecessary interventions for women, adopt evidence-based practices, and protect/promote the health of mothers and children. If an appropriate policy is formed in line with this aim, the quality of the provided service will increase to a significant extent, which will help to reduce mortality and morbidity rates. More effort and policies are needed in Turkey for the integration of best practices targeting the health needs of women and protection and promotion of public health in the health service. Concerning planning and policy development of maternity services, there are no detailed published data on the pregnancy, labor, and postpartum practices of private hospitals, nor hospital support for families during these processes. Therefore, the main aim of this study is to determine the differences between hospital practices in Turkey related to prenatal, birth, and postpartum in the sample of private hospitals.
Methods
A purposive sampling was used in this descriptive study to define the provinces with the highest number of hospitals in Turkey to be surveyed. They were Ankara, Istanbul, and Izmir. There were 178 private hospitals in these provinces. A simple random sampling technique was employed to identify the hospitals to be surveyed, and 49 hospitals were recruited. The study targeted private hospitals and excluded dialysis, in vitro fertilization, medical, physical therapy, and rehabilitation centers. Hospitals which were shut down, did not agree to take part, and did not have a maternity service were filtered out.
Data were gathered using the questionnaire form of the Canadian Hospitals Maternity Policies and Practices Survey. The questionnaire consisted of 130 questions organized into 13 main topics. Because of the wide variety of comprehensive data and topics, this study only evaluated the data on pregnancy, labor, and postpartum periods. The other sections and the rest of the data are not discussed in this article. The questionnaire form was translated into Turkish and reviewed by a group of experts with a PhD in gynecology, public health, and pediatrics. Pilot testing was conducted to ensure that the questionnaire was comprehensible and appropriate terminology was used. The questionnaire was relevant to be very well understood by respondents and reduce the number of nonrespondents. It allowed checkboxes and text.
The questionnaire was sent to the directors of the hospitals and they were requested to deliver it to the most appropriate individuals to fill it in. The respondents were managers, head physicians, head nurses, midwives, and specialist physicians. Data management and analysis were performed using descriptive statistics of SPSS for Windows (version 21.0). A standard coding was used for hospitals in data analysis. Hospitals were divided into groups by bed capacity and the number of health staff. The coding and analysis method of the original version of the questionnaire, the Canadian Hospitals Maternity Policies and Practices Survey, was taken into consideration as an example in this process. Permission was received from the Public Health Agency of Canada for the questionnaire form, and ethical approvals and permissions were obtained to conduct the study from all the responding hospitals in Turkey.
Research findings
Results
Forty-nine of the 178 eligible private hospitals in the provinces of Ankara, İzmir, and İstanbul completed and returned the questionnaire—an overall response rate of 28%. The number of the completed questionnaires was adequate and representing the population according to the results of the simple random sampling method. 71.4% of the participating hospitals were baby-friendly. 28.6% of the hospitals who said that they were not designated to be baby-friendly reported that they were in the process of becoming so. Hospital practices or routines in maternity wards are presented in Table 1.
Hospital practices or routines in maternity wards.
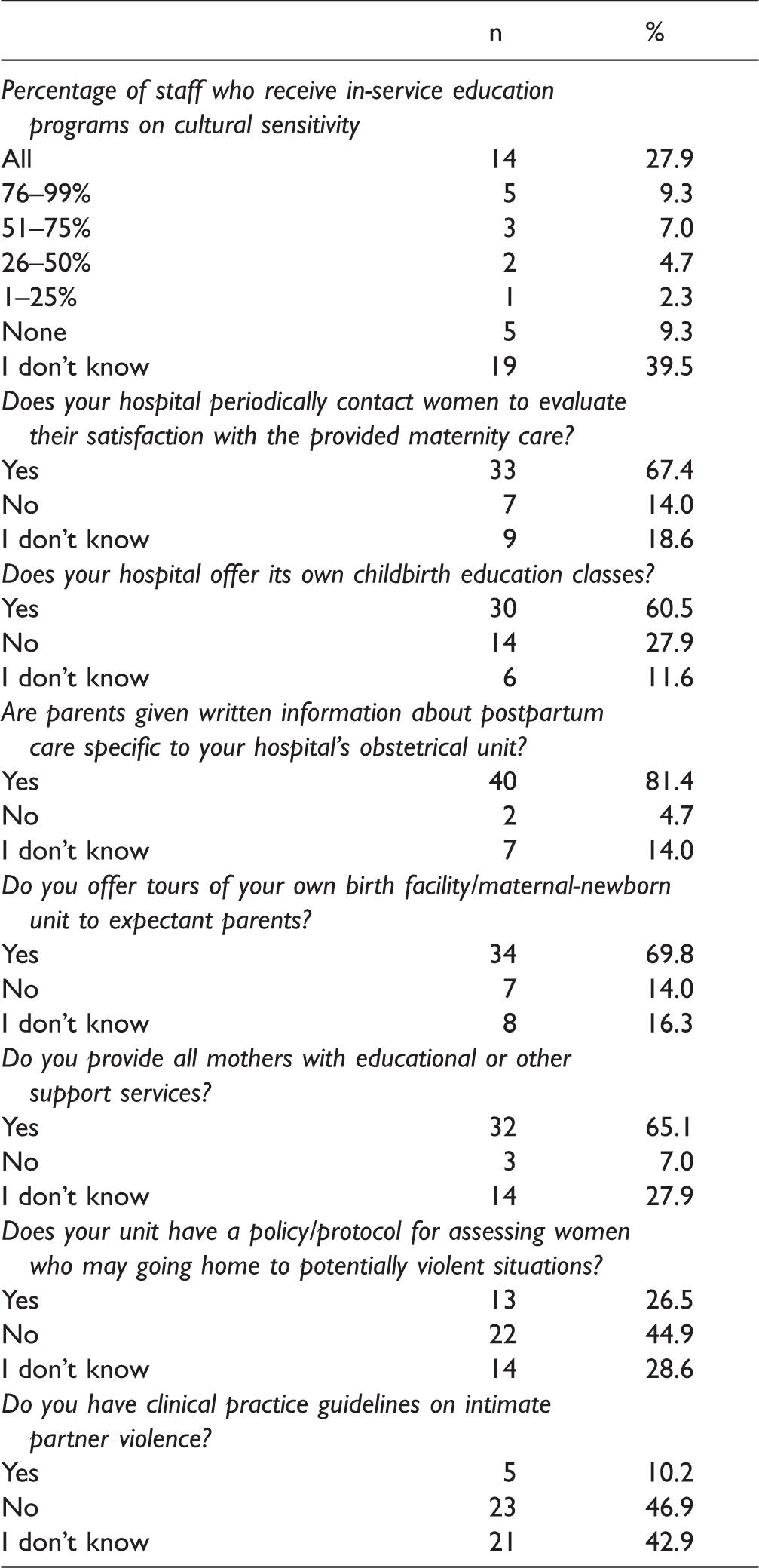
Of the hospitals, 27.9% reported that they provided in-service training programs on “cultural sensitivity” for their staff. Forty-four percent reported that they had a committee for reviewing obstetrical policies and developing guidelines. 67.4% periodically contacted women to assess their satisfaction with the provided maternity care. 69.8% offered tours of their birth facility/maternal-newborn unit to expectant parents. 65.1% provided educational support services to all expectant mothers. 44.9% did not have a policy for assessing women who may be going home to potentially violent situations. Just under half of the hospitals (46.9%) did not have clinical practice guidelines on intimate partner violence.
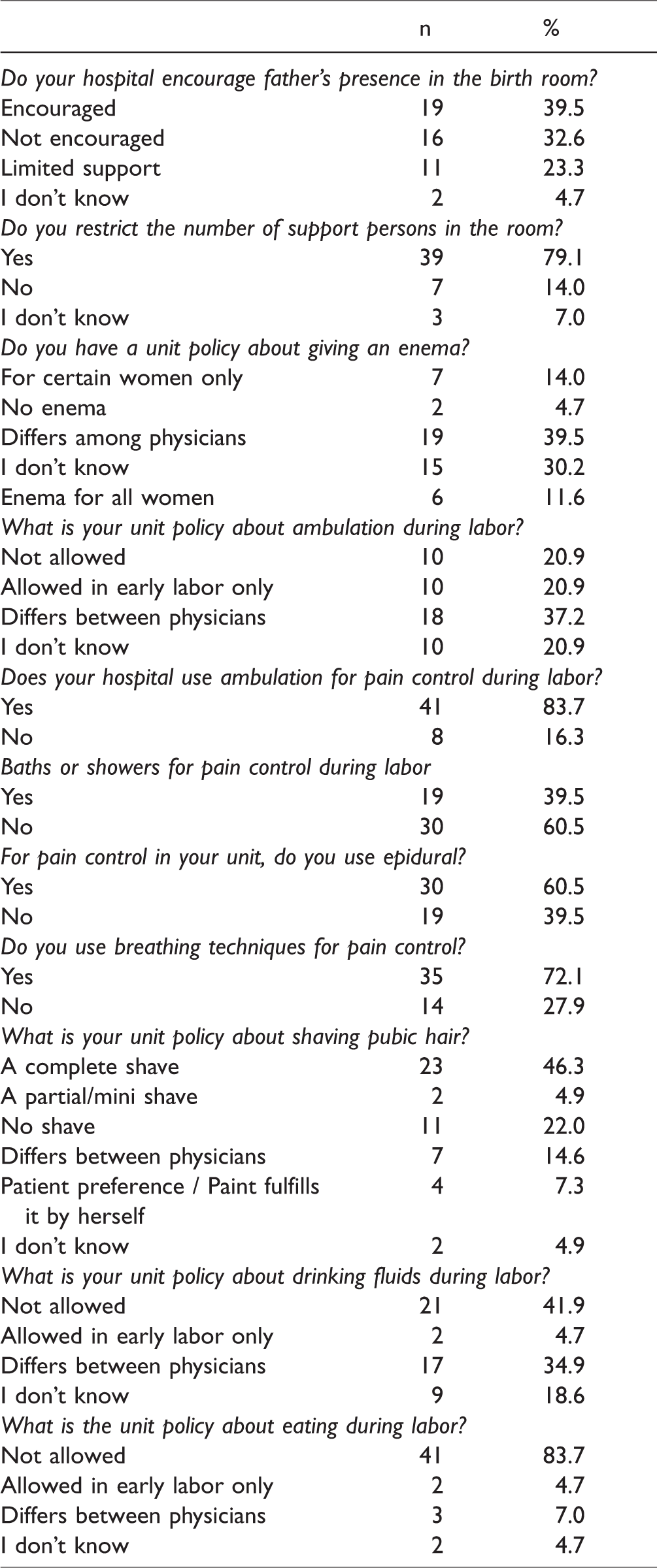
39.5% of the private hospitals reported that they encouraged fathers’ presence in the birth room during labor. The majority (79.1%) of the private hospitals restricted the number of support persons in the room. 11.6% reported that they administered enema to all women. When hospitals were asked if ambulation was available as an approach to pain control, 20.9% indicated that they did not allow ambulation during labor, 20.9% allowed it only in early labor, and 37.2% indicated that their unit policy about ambulation differed among physicians. Hospitals benefited from a variety of pain management methods such as ambulation (83.7%), breathing techniques (72.1%), epidural anesthesia (60.5%), baths and showers (39.5%). 46.3% reported a policy of complete shaving of pubic hair. 41.9% reported that they had a unit policy stipulating that drinking fluids during labor was not allowed and 83.7% reported that they did not allow women to eat during labor.
The vast majority (85.7%) of the hospitals gave mothers their first opportunity to hold the baby within 1 h. 36.7% of the hospitals gave fathers their first opportunity to hold the baby after 1 h. 57.1% of the hospitals had a unit policy stating that they cut the umbilical cord immediately. 67.3% of the hospitals did not give fathers the opportunity to cut the cord. 57.1% had a policy that facilitated families being together immediately after the birth. 57.1% reported that mothers could choose early discharge following a vaginal birth and they had formal protocols for early discharge. The length of early discharge after vaginal birth was 24 h or less in 54.2% of the hospitals and 48 h or less in 49% of the hospitals after cesarean birth. 44.9% reported that telephone contact with a health nurse was available after discharge, 20.4% reported that a home visit was available, 4.1% reported that a visit to a doctor’s office was available for women after they left the hospital, and 28.6% reported that referral to postpartum clinics was available. When we look at the policies about restrictions on visiting hours during the postpartum period, we see that 26.5% of the hospitals had such restrictions for partners, 36.7% had restrictions for siblings, and 38.8% had restrictions for grandparents.
Discussion
This study aimed to determine the hospital practices implemented before, during, and after birth in Turkey, and to identify the support to families during this process. Given that there are many variables such as practices specific to each hospital, policies and procedures in private hospitals, and the current health policy of the country, it is difficult to handle private hospitals in a broader scope under a single category. It cannot be said that the unweighted numbers in the tables account for a nationwide representative sample. Yet, because this study targeted the most crowded and wealthiest provinces of Turkey (a third of the general population), it is possible to say that it is strong enough to be regarded as a typical sample of the current situation of the issue in Turkey. It is also important to note that this study provides the first comprehensive assessment of this issue in Turkey.
It can be inferred from the study findings that hospitals in Turkey are making efforts to improve maternal health services. However, it is difficult to say that private hospitals are up to date on best practices or have mechanisms to evaluate themselves systematically. It is evident that there is limited support for families in hospitals.
Cultural characteristics determine how women and their families adapt to pregnancy, their attitudes toward it, and the extent to which they take part in the pregnancy and birth stages. It is important that nurses be familiar with the cultural practices of the families to which they provide care, which may affect pregnancy and birth process, and show consideration and respect for cultural differences. Concerning family support and cultural sensitivity, it can be seen from Table 1 that 27.9% of the hospitals indicated that all of their staff received in-service education programs on cultural sensitivity. However, most of the hospitals did not have written guidelines for providing culturally appropriate care for their patients. A similar study conducted in Canada found that one in five of the hospitals had written guidelines for providing culturally appropriate care for their patients and nearly half of the hospitals reported that at least some of their staff received such training programs on cultural sensitivity. 3
Pregnancy is one of the most risky periods in a woman’s life. Violence during pregnancy heightens this risk even more. A study conducted with 249 pregnant women about violence found that women’s exposure to different forms of domestic violence during pregnancy was over 25%. 4 According to the Society of Obstetricians and Gynecologists of Canada, “institutions and clinicians” offices should have protocols for intimate partner violence, information leaflets or handouts, and current lists of community resources for victims. Safe and secure environments, well trained personnel, audio-visual materials, and assistance are required for women to protect them from partner violence. 5 This study has found that 44.9% of the hospitals did not have a policy/protocol for assessing women who may be going home to potentially violent situations and nearly half of the hospitals reported not having clinical practice guidelines on intimate partner violence. Although annual prevalence rates of violence during pregnancy have been reported to be between 6 and 8% in Canada, nearly half of the hospitals had a policy/protocol for assessing women who were going home to potentially violent situations. 3 Lack of written guidelines or standards on cultural practices and issues of violence is viewed as problematic in terms of management. The lack of standards may mean that there are no systematic hospital records, healthcare quality assessment is insufficient, and identifying best practices is hampered.
One of the practices that have a very important role in reducing the fear and anxiety of expectant mothers is to take a tour of the birth facility with the participation of the parents. A study conducted in Canada found that almost all hospitals provided necessary training on this matter; they offered tours of their birth facility/maternal-newborn unit to expectant parents, and the majority of hospitals provided all mothers with a current list of educational or other support services. 3 This study has found that more than half of the hospitals periodically contacted women to evaluate their satisfaction with the maternity care, offered childbirth education classes, gave parents written information about postpartum care, and organized tours of their birth facility/maternal-newborn unit (Table 1).
Personal experience, social and physical environment, social support, and prior birth experiences play an important role for women in childbirth.1,6 There is a positive relationship between family support and effective management of pregnancy. 1 Support services that positively contribute to women during labor are common among hospitals in Turkey, although limited in some of them. While addressing this issue, the responsibility of the father should also be taken into account. Previous research indicated that social support for women was considerably important in the childbirth experience.7–9 According to the findings of this study, while two out of five hospitals encouraged fathers to be present in the birth room during labor, some of them encouraged their presence with restrictions or did not encourage it at all. The majority of hospitals restricted the number of visitors after birth. Hospitals were more likely to let fathers visit while they were less likely to let grandparents and siblings visit. Although cultural differences are important aspects which should not be overlooked, the presence of the father during birth is a positive practice. As for the restriction and permission policy of hospitals on visiting hours during the postpartum period, fathers experienced fewer restrictions of visiting hours. A study conducted in Lebanon found that some mothers requested to be only with their mothers instead of their partners during labour. 10 This is a cultural practice. In a study conducted in Croatia, 77% of women stated that they wished the presence of someone close to them for support during childbirth. Ninety-three percent of them considered that a support person could facilitate their childbirth process. 11 The presence of any category of a support person during labor and birth is encouraged by the Society of Obstetricians and Gynecologists guidelines (1998), the Family Centered Maternity and Newborn Care: National Guidelines, and WHO recommendations.3,12
There is increased concern that some prenatal and maternal initiatives and practices that are not evidence-based have become standard practices all over the world.13,14 A systematic review found that routine enema administration and perineal shaving were not supported by scientific evidence and could cause harm and discomfort.6,15 It is possible to see different practices in the examples of different countries. A study conducted in Croatia found that 78% of women were administered an enema. 16 This study has identified that 11.6% of the hospitals gave an enema to all women, yet 39.5% of them reported that their unit policy differed among physicians, which reinforces the argument that there is lack of evidence of this issue. Shaving pubic hair can also be the subject of different cultural practices. The hospitals participating in this study have different policies about shaving pubic hair. These policies varied by hospitals: some hospitals have a policy of complete, partial, or no shaving, while in some of them it differs among physicians or patients do it themselves. As we can see, it is very difficult to talk about a certain policy in this regard.
Restricting fluids, food intake, and movement during labor is also not supported in the literature. 16 In a study conducted in Croatia, 67% of women were thirsty during labor, 69% were not offered anything to drink, 22% felt hungry, and 95% were not given anything to eat during giving birth. It has been observed that women were not usually allowed to drink or eat during labor, although there is no basis for not allowing this practice to women at low risk.11,15 In this study, though we do not have information about whether women wished to take fluid during labor, we found that 41.9% of the hospitals had a unit policy stipulating that drinking was not allowed. Only a low number of them allowed drinking fluids in early labor only, while some indicated that it differed depending on the physician or the risk of birth. There is no standard for this matter among hospitals.
Mobility (except in some cases) has some advantages: it increases contractions that help cervical dilation, makes a mother feel more comfortable, and reduces the use of analgesia during labour. 17 Literature indicates that ambulation is one of the most comfortable positions/techniques. It is reported that breathing techniques help to ease delivery, and epidural anesthesia is more effective than other anesthesia techniques in controlling pain and collaborating with women. The study conducted in Croatia reported that 23% of women received epidural anesthesia as a method of pain control. 11 This study has identified that ambulation, breathing techniques, epidural anesthesia, and baths and showers are, in order, reported as methods used to cope with pain. One in five hospitals had a policy that did not allow ambulation during labor, while 20.9% of hospitals only allowed it in early labor (Table 2). These figures demonstrate that there are variations in practices among hospitals. When these techniques are used, it is necessary to take patients’ choices into consideration, and healthcare should be provided based on evidence-based practices. 3
Labor and delivery routines.
Postpartum care practices and routines.

If we look from a family-centered maternity perspective, mother and newborn should be considered as a whole with familial support in the early postnatal period, and direct contact between mother, baby, and father should be encouraged. 3 A baby’s skin-to-skin contact with his/her father after cesarean section enables the baby to calm down and stop crying. It also supports a mother in breastfeeding. A father’s help in feeding and caring for the newborn as well as his physical and emotional assistance plays an important role in successful breastfeeding.7–9 Early mother–newborn contact, early breastfeeding, forming policy about breastfeeding, and baby-friendly hospital practices are accepted by WHO and UNICEF as practices that have positive effects on the success of lactation.1,18 Current study findings show that most (85.7%) hospitals usually give mothers the first opportunity to hold the baby within 1 h. 34.7% of hospitals give fathers the first opportunity to hold the baby within 1 h of birth (Table 3). A study conducted in Canada found that the above-mentioned rates could rise to 100% in some of the hospitals.
This study showed that slightly more than half of the hospitals had a policy that facilitated families being together immediately after birth. When hospitals were asked if the woman’s partner was given the opportunity to cut the cord, more than half of the hospitals indicated that this never happened. Only 6% of hospitals indicated that this was frequently the case (Table 3). The study in Canada found that nearly all hospitals in Canada gave fathers the opportunity to cut the cord. Half of the hospitals in Turkey in this study had a policy that the umbilical cord was cut immediately, while 16.3% reported no unit policy on it. It appears that because of the ongoing hospital policies, fathers’ level of taking responsibility for a baby is low in Turkey and needs to be developed.
The postpartum period is an important transition for a mother, baby, and family as a whole. This is a crucial time when mother–baby bonding evolves. It is a psychologically and socially important process for the family members. 3 In this period there are some policies and practices recommended so that a family can adapt to the baby. The main one of these policies is to send the mother and baby home to their family environment. At this point early discharge is crucial to a mother for entering the family environment faster. Although there are discussions about the positive and negative aspects of the early discharge, its importance and supporting a mother with home visits following the birth are underlined in Liu et al. 19 and Cargill and Martel. 20 The study results showed that more than half of the hospitals had formal protocols that set conditions for early discharge. In most hospitals the average length of stay following vaginal birth was one day and two days following cesarean birth. Half of the hospitals had the option of early discharge for mothers following vaginal birth. The early discharge could be after 12 or fewer hours after vaginal birth, and 24 or fewer hours after cesarean birth. Although the evidence base for the most effective follow-up care model is poor, the study findings show that support after discharge is given mostly through telephone contacts and then via postpartum clinics and home visits (Table 1).21,22
Conclusion
There are different practices and policies on birth and postpartum periods at hospitals. Further research addressing the opinions of health professionals and clients receiving care in the related units is required. The primary recommendation of this study is that all hospitals should review their maternal practices and routines in an evidence-based way so as to make them useful to mothers and newborns. Women need to know what is done to them and should have the right to choose. Hospital practices in this field need to be developed and extended via legislative arrangements to cover all types of hospitals. During gestation, services that can be received at and after birth should be described to expectant mothers in detail and this should be indicated in a contract to enhance the quality of healthcare. There is a clear need to educate mothers about prenatal and postnatal care in hospitals. It is necessary to prepare and put into practice a standardized training plan for this issue for women who will give birth, current mothers, and expectant mothers. Differences in policies and practices before, during, and after birth should be eliminated. Cultural sensitivity should be shown to mothers and families, and their wishes should be taken into account. The implementation of standards such as “baby-friendly hospital” should be made compulsory, and new standards are required for the development and enhancement of perinatal care quality. There is a need for comprehensive research to be conducted in Turkey into perinatal care and family support services. It can be suggested that this questionnaire be sent to all hospitals at the national level and monitored every two years to do a general assessment of policies and practices and set standards.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.