
Abstract
This study examines the extent to which important personal characteristics of nursing home residents affect the well-being of caregivers, as reflected in their levels of work-related positive and negative affect. To do this, we applied the Job Demands-Resources model to the analysis of caregivers’ work-related well-being by focusing on residents’ residual cognitive capacity and their perceived adequacy of resources. A multiple regression analysis was carried out based on combined data from a sample of 1080 caregivers and 290 residents from 13 nursing homes in Italy. Predictors of caregivers’ positive and negative well-being included job characteristics such as workload and social support. As expected, residents’ perceived adequacy of resources was positively related to caregivers’ well-being positive affect. Unexpectedly, residents’ residual cognitive capacity was associated with higher rather than lower levels of caregivers’ well-being negative affect. The quality of the interaction between residents and caregivers in nursing homes is contingent on their respective expectations and capabilities, and reciprocal perceptions of the outputs exchanged.
Keywords
Background
Customers have become a central feature within the service industry, which places operational and emotional pressure on frontline employees. They are increasingly required to have higher levels of productivity, flexibility and responsiveness, while at the same time remaining more available for work; all conditions that may be detrimental to their well-being. 1
The health care industry, particularly the long-term healthcare sector, is a notable example of this trend towards customer-centric care. In fact, frontline employees (caregivers) typically experience high levels of operational complexity (24/7), as well as increasing and challenging demands when interacting with vulnerable customers (residents). 2 The context of our research project is within this environment - the long-term healthcare sector. The aim of this study is to present and test a research model that reverses the literature’s dominant view that employee-related constructs explain customer-related constructs.3,4 Specifically, we examined the impact that resident-related constructs, residual cognitive capacity and perceived adequacy of resources had on the well-being of caregivers in nursing homes (NHs). We did this by using residents’ self-measured constructs and objective characteristics, as well as caregivers’ self-measured constructs. Exploring the well-being of employees at a deeper level, and generally the well-being of caregivers overall, is important as these professions are seeing a staff shortage in mature economies with ageing populations. 5
In order to conduct this research, we drew on the Job Demands-Resources (JD-R) theory 6 to develop and test a five-component JD-R research model using survey data from a sample of 1080 caregivers and 290 residents from 13 NHs in northern Italy.
Employee well-being
Here we focused on work-related employee well-being, which is defined as the overall quality of an individual’s subjective experience functioning at work. 7 In particular, we focused on so-called ‘happiness well-being’ 8 with a special reference to core dimensions of both positive affect (e.g. enthusiasm) and negative affect (e.g. uneasiness) at work. 9
Job demands and resources
The J-DR model has been widely used to explain work-related employee well-being. 10 Specifically, job demands refer to aspects of a job that require mental, physical, or emotional efforts that may result in potential strain for individuals. Job resources refer to parts of a job that helps to reduce job demands and/or contribute to personal development and goal achievement, such as autonomy or social support. 6 As such, job demands are expected to be associated with higher levels of negative affect and lower levels of positive affect, while job resources are expected to contribute to positive affect and help reduce negative affect.
As part of our research model, we included one job demand and four job resource variables, which have been shown in extant studies to have a positive impact on positive affect and a negative impact on negative affect. The first (job demand), workload, refers to the extent to which a caregiver perceives that the amount of work s/he has to do is more or less adequate. 11 More specifically, the level of workload also captures the effort demanded from caregivers because of residents’ health status in terms of having enough time to get everything done on the job, the overall perceived adequacy of the workload, the speed and the hardness required by the job. 12 The second, access to information, refers to the caregiver’s perception that the organization provides enough adequate and relevant information about the efficient and effective management of services. The third, organizational justice, relates to the extent to which a caregiver perceives that s/he is being treated fairly by the organization through the recognition of tangible and intangible contributions. 13 The fourth, interpersonal relations with colleagues, refers to the extent to which a caregiver perceives that the quality of his or her relationships with colleagues is high. 14 The fifth, relations with residents, relates to the extent to which a caregiver perceive that the quality of his or her relations with residents is high. 15 As a job demand variable, workload is expected to be negatively related to well-being, so that there will be a negative relationship with positive affect and a positive relationship with negative affect. In contrast, the remaining job resource variables are expected to be positively related to well-being – so that there will be a positive relationship with positive affect and a negative relationship with negative affect.
Residents’ variables
To our knowledge, the literature lacks studies that take into account the impact that resident-related constructs might have on the level of caregivers’ emotional well-being; therefore, we included two constructs related to residents of NHs in our research model. The first construct, perceived adequacy of resources, refers to the extent to which residents viewed the services they received to be of an adequate quality. The second construct, residual cognitive capacity, relates to an important specific personal characteristic of the residents themselves, namely their objective level of cognitive autonomy and self-sufficiency. This parameter is of particular relevance as the lower is the residual cognitive capacity, the more likely is that the residents in question will engage in behaviors that are increasingly demanding for caregivers. 16 Previous studies17,18 have shown that the behaviors of residents with a reduced residual cognitive capacity might lower the level of wellbeing of caregivers, to the extent of determining, among others, phenomena of stress, burnout and depression. Consistent with this line of argument, a study 19 show that caregivers taking care of Parkinson’s disease residents with mild cognitive impairment experience higher levels of burden, when compared with colleagues assisting Parkinson’s disease residents with normal cognition, pointing at the fact that “… even in the early stages of the disease the presence of impaired cognition places an additional load on caregivers”.( 19 , p. 8)
As potential resources, and in line with JD-R theory, we expected both residents’ perceived adequacy of resources and residual cognitive capacity to be positively related to caregivers’ well-being (i.e. to have a positive impact on their positive affect and a negative impact on their negative affect) (Figure 1).
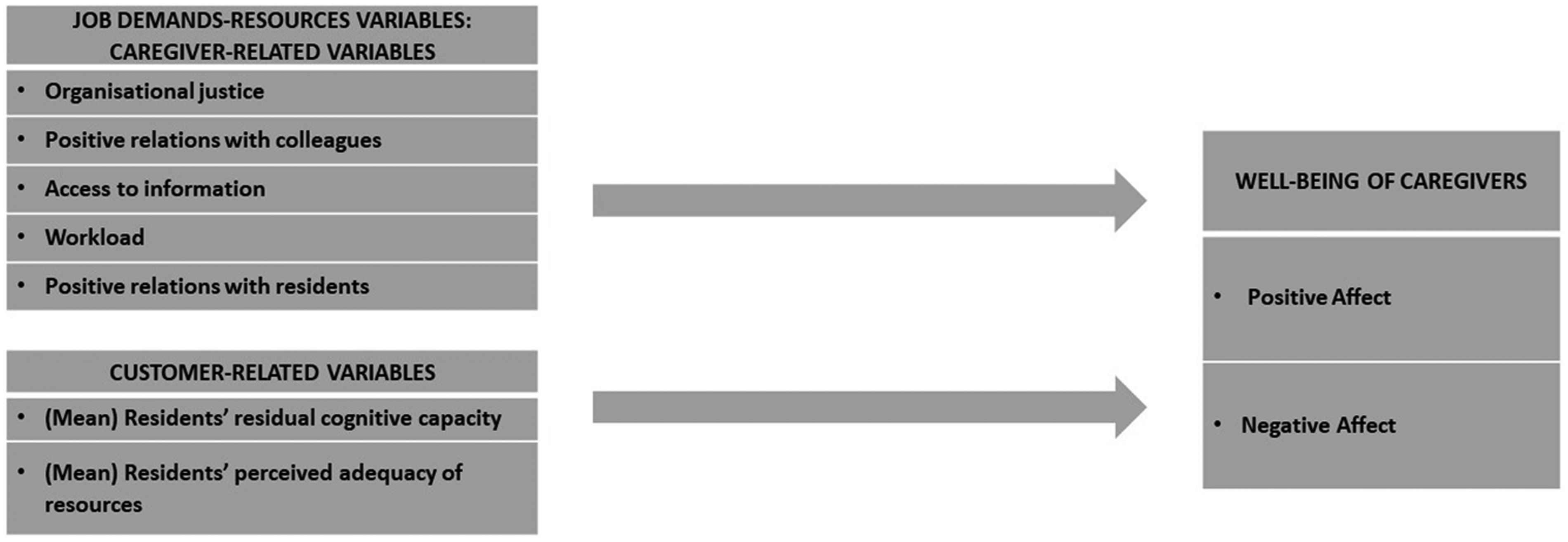
Research model.
Methods
Research context
The long-term health care sector has been growing rapidly in most of the mature economies for the past three decades, 20 due to ageing demographics, fewer families taking care of older family members, as well as the shifting of care for the elderly from hospitals to nursing homes.1,21 In Italy, our research context, the current percentage of those over 64 years old is 22.6% of the population, and it is expected to reach 23.9% in 2021 22 suggesting a significant increase in future demands for services for the elderly. Nursing homes offer a wide range of services, such as providing meals, personal care, social activities, physiotherapy, medical checks and therapy with the main aim of preserving the cognitive and physical capacities of residents, and their overall dignity and quality of life. 23 However, all these activities are offered in a context characterized by a lack of public funding and resources, and an emphasis on efficiency, which constitute additional sources of pressure on caregivers with potentially negative consequences for their well-being.
Data
The data for the present study were collected through two independent surveys carried out among NHs associated with the Nursing Homes Observatory of the LIUC Università Carlo Cattaneo (Italy), mostly concentrated in the northern part of Italy. The study has been carried out according to the research ethics code of LIUC Università Carlo Cattaneo, and in compliance with the Italian national framework about data collection (“Decreto Legislativo 30 giugno 2003, n. 19”).
The first survey, aimed at nursing home residents, was carried out between July 2013 and February 2014. Direct distribution of the questionnaires was not considered feasible or appropriate given the advanced average age of residents; therefore, the general manager of each NH that participated in the study agreed to identify one or two caregivers that would act as facilitators. They would help residents fill out the questionnaire by reading it repeatedly until they were certain that the questions were understood by the residents. In order to properly manage the data collection protocol, the facilitators participated in a half-day training delivered by one of this study’s authors. Each nursing home administered the survey to a random sample of between 15% and 20% of the residents. The questionnaire was anonymized and resident participation was on a purely voluntary basis. In total, 895 valid questionnaires were collected from 54 NHs with the support of 71 facilitators.
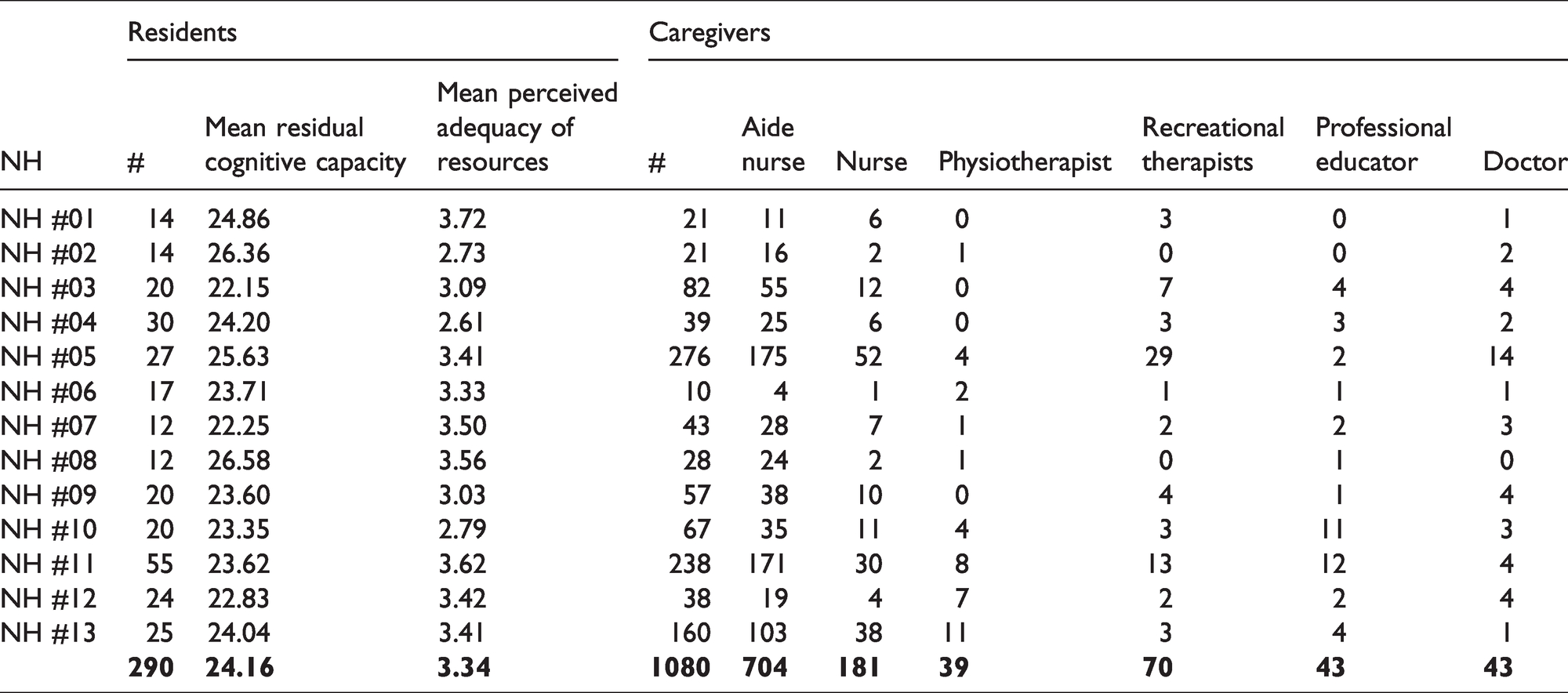
The second survey, that focused on the well-being of caregivers, was conducted in 2014 and 2015. A paper version of the questionnaire was delivered to the management of each NH, who distributed and collected the completed surveys in an anonymized way and on a voluntary basis. Overall, the second survey covered a total sample of 2157 caregivers in 26 NHs, of which 13 of these 26 NHs had also participated in the first survey. For our study, we concentrated on those 13 nursing homes who had participated in both surveys and their frontline caregivers who had continuous and/or regular contact with residents. For this reason, we included in the study nurses, nurse-aids, physiotherapists, recreational therapists, professional educators and doctors; administrative staff was excluded from the analysis. The final data set for the analysis comes from 1080 caregivers and 290 residents from the 13 matched NHs. Details of our final dataset are presented in Table 1.
Final dataset for residents and caregivers in nursing homes.
In this context it is important to note that the two-wave temporal design of the study, whereby data from residents were collected at time 1 followed by data from caregivers at time 2, is in line with the causal ordering of our hypotheses which propose that residents’ personal characteristics have an impact on employee well-being, rather than the other way around as is commonly discussed in the literature. In other words, the causal ordering of the hypotheses is aligned with the temporal design of the study thereby minimizing any potential problems of reverse causality in the analysis.
Measures
Dependent variable
The well-being of caregivers was measured using the Job-Related Affective Well-being Scale. 24 This scale differentiates six positive emotional states (calm, content, relaxed, enthusiastic, optimistic and cheerful), from six negative ones (tense, uneasy, worried, depressed, gloomy and miserable). The responses in the scale relate to the frequency of those emotional states (1 = never; 5 = always). All the positive and negative items loaded on their expected factor and both scales showed good reliability (.84 and .85 respectively).
Independent variables related to employees
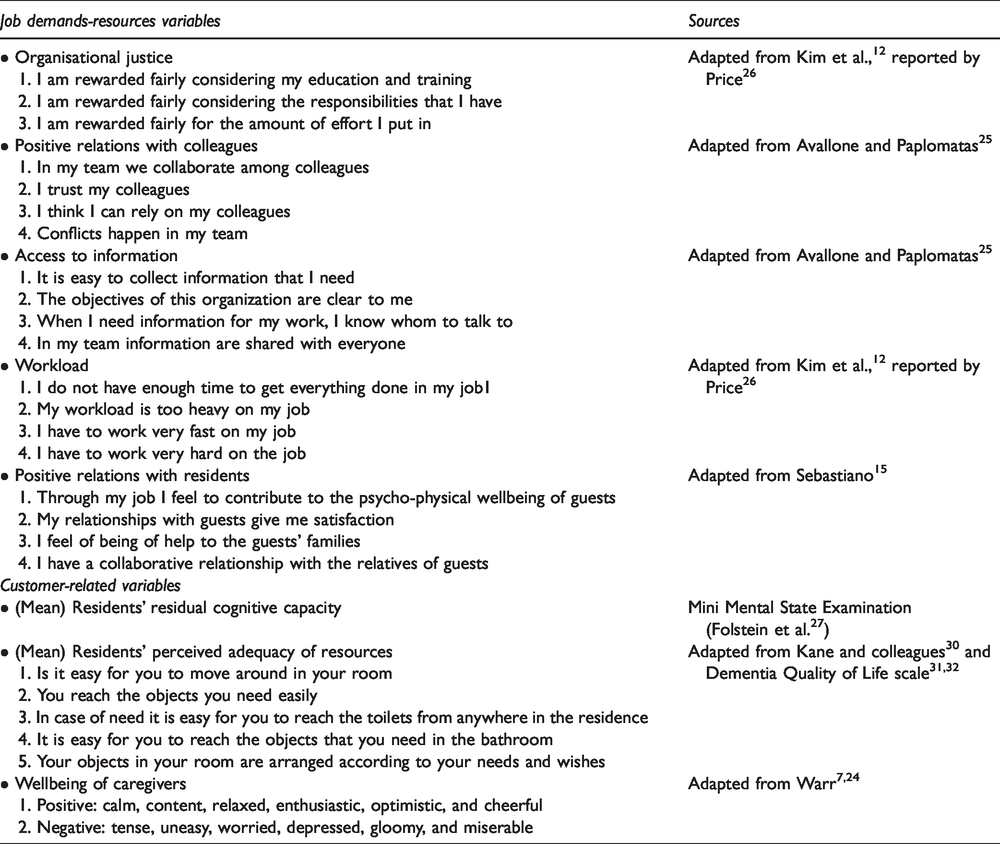
Access to information and interpersonal relations with colleagues were measured by using 25 two four-item scales. We measured organizational justice and workload by using,12,26 three-item and four-item scales respectively. Relations with residents was measured with 15 four-item scale designed to assess the quality of relations of caregivers with residents and their families.
Responses to all items used to construct the above scales were scored on a five-point Likert scale measuring a respondent’s agreement or disagreement with the item in question (1 = strongly disagree; 5 = strongly agree). Factor analysis of all the items showed that they loaded properly on five different factors. The reliability analysis showed and alpha coefficients of .80 for access to information, .76 for interpersonal relations with colleagues, .89 for organizational justice, .73 for relations with residents and .73 for workload.
Independent variables related to residents
The resident’s cognitive capacity was measured using the Mini Mental State Examination (MMSE). 27 Being the most widely used psychometric tool, 28 this test is regularly used to measure the cognitive loss deriving from ageing related illness. The MMSE is meant to establish what the residual cognitive capabilities are in terms of, for example, attention, orientation, calculation, language, recall, and ability to follow simple commands. The scale has thirty points where thirty is associated with full cognitive capabilities. Given the cognitive state of some of the residents, the following categories of residents were discarded from the survey: 29 non-responsive residents with degenerative advanced cognitive diseases (e.g. Alzheimer, etc.); residents who had lived in the nursing home for less than three years; residents with Mini Mental State Examination MMSE of less than 10; and clinically unstable residents.
The perceived adequacy of services was measured by the 30 5-item functional competence scale involving an adapted version of the Dementia Quality of Life scale.31,32 Within their residual physical and cognitive capacities, this measure is supposed to assess the adequacy of the physical environment which can support, or limit, the autonomy of residents. 30 All of the items loaded properly on one single factor with a reliability coefficient of .82.
It should be noted that the resident-related variables used in the main analysis were the average cognitive capacity and perceived adequacy of resources scores for each NH. Specifically, for each of the 13 NHs in the study, we calculated the average level of residents’ cognitive capacity and of perceived resource adequacy and then used these mean scores as predictors of individual caregivers’ positive and negative affect within each organization (see Tables 1 and 2). The correlation between residents’ mean cognitive capacity and perceived resource adequacy was .12 (p > .05). Scales and related items for constructs are provided in Appendix 1.
Predictors of employee positive and negative affect (standardised estimates).
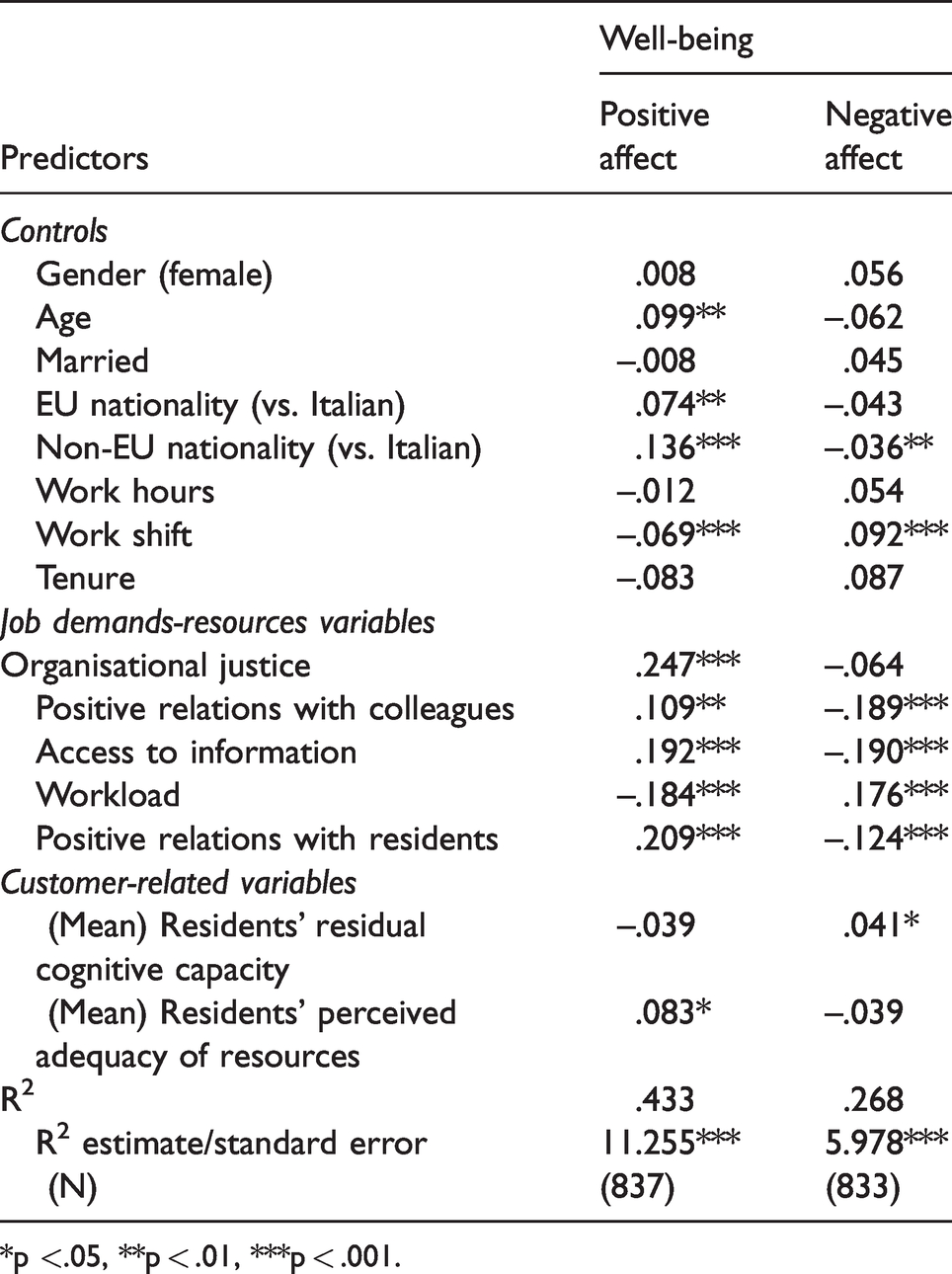
*p <.05, **p < .01, ***p < .001.
Control variables
Several control variables were included in the analysis. These included demographic variables such as gender (1 = man; 2 = woman), age, marital status (single = 1; married = 2), nationality (1 = Italian; 2 = European; 3 = non-European) and work tenure stated in years. We also included some work-related controls, such as whether the respondent worked part-time (= 1) or full-time (= 2), and whether s/he worked shifts according to 24-hour-shifts (1 = yes; 2 = no). Following the procedure suggested in another studies, 33 a number of other control variables such as the number of children, organizational tenure, type of employer and commuting time, were also examined; however, the preliminary analysis showed that they did not have any significant effect. For this reason, they were excluded from the final analysis. In Appendix 2, we provide mean, SD, ranges and correlations for all variables used in the study.
Analysis procedures
The data were analyzed using a multiple regression in Mplus 7.3. To take account of the potential non-independence of observations due to the potential nesting of respondents within the 13 nursing homes, the study hypotheses were tested using the complex procedure in Mplus.
Results
Table 2 reports the results of the main regression analysis designed to test the research model. Columns 1 and 2 of the table show the results for the positive and negative affect of well-being, respectively.
As can be seen, a number of the controls were significantly related to either a positive or negative affect, or both. Employees working on shifts, for example, reported lower levels of positive affect combined with higher levels of negative affect. Older employees also tended to exhibit higher levels of positive affect, as did non-Italian employees who came from either outside, or within, the European Union.
All of the main job demands and job resources variables included in the analysis were also significantly related to both positive and negative affect. In all cases, the relationships were in the expected direction, consistent with J-DR theory. 6 Specifically, the job demand variable was associated with lower levels of employee positive affect and higher levels of negative affect. In contrast, all the job resources variables, including organizational justice, positive relations with colleagues, information sharing, and positive relations with residents were associated with higher levels of positive affect coupled with lower levels of negative affect.
It is worth noting that in a separate analysis we also examined the interaction between job demands and resources to test the buffering hypothesis from the JD-R model and determine whether the various job resources in our model helped to reduce the negative effect of workload on caregivers’ well-being. However, none of the interactions were significant suggesting the absence of any clear JD-R moderator effects in our data (results available upon request).
Most importantly, the results in Table 2 show that caregivers’ positive and negative affect of well-being were associated with the two main resident-related predictors in our study, namely average residents’ residual cognitive capacity and average residents’ perceived adequacy of resources in each NH. However, the relationship between these two resident-related variables and caregivers’ well-being was more complex than anticipated. Specifically, residents’ perceived adequacy of resources was significantly positively related to employee positive affect (standardized estimate = .083, p < .05). Contrary to what we expected, however, residents’ perceived adequacy of resources was not found to be significantly (negatively) related to employee negative affect (standardized estimate = –.039, p > .05). At the same time, contrary to what we expected, residents’ residual cognitive capacity was not significantly (positively) related to employee positive affect (standardized estimate = –0.39, p > .05), nor was it significantly negatively related to employee negative affect. The relationship between residents’ cognitive capacity and employee negative affect, in fact, was positive (standardized estimate = .041, p < .05) rather than negative.
Overall, therefore, our results suggest that the link between resident’ residual cognitive capacity and their perceptions of the adequacy of services, and the well-being of caregivers is more articulated than expected. Specifically, residents’ cognitive ability was associated with higher levels of negative affect amongst caregivers and, therefore, had a generally negative effect on caregivers’ well-being. In contrast, residents’ perceptions of the adequacy of resources was associated with higher levels of caregivers’ positive affect and, therefore, had a generally positive effect on their well-being. Finally, the R-squared values of the regressions indicate that the explanatory power of the model is quite good – taken together the variables in the model explained 43.3% and 26.8% of the variance in the positive and negative affect of caregivers respectively.
Discussion
This study offers interesting empirical findings, contributing to the literature on the well-being of employees in the long-term healthcare sector in different ways. First, all the caregiver-related job demands and job resources variables included in the analysis were found to be significantly associated with positive and negative affect in the expected direction, thereby confirming not only the general applicability of the JD-R model, but also its specific value in helping to understand employee well-being in the long-term healthcare sector.
Second, while as expected residents’ perceived adequacy of resources emerged as a positive predictor of caregivers’ positive affect, it was not a significant predictor of their negative affect. One possible explanation for this mixed finding may be related to the fact that, because of their fragility due to their age and health conditions, residents of NHs tend to have fairly basic and simple needs and expectations linked, for example, to food, shelter and comfort. Although helping to satisfy basic needs of this kind requires effort on the part of caregivers, the demands involved may not be so great as to generate undue stress and strain for the employees involved. At the same time, however, effectively responding to residents’ needs and contributing to their day-to-day well-being can be experienced as highly rewarding by the caregivers involved. In addition, through processes of emotional contagion, 34 happier residents can also be expected to result in happier and more satisfied employees. 35 Although taken together the above arguments begin to explain the mixed pattern of findings linked to residents’ perceived adequacy of resources, this is an area that clearly requires further research. Future research could also usefully extend the present analysis by examining the more general characteristics of care homes, such as their size and financial performance, that might affect residents’ perception of the adequacy of resources in the first place.
Third, while residents’ residual cognitive capacity was not found to be significantly related to residents’ positive affect, contrary to expectations, it was found to be associated with higher, rather than lower, levels of caregiver negative affect. On this, our results do not seem to be in line with the findings of other studies.17–19 A possible explanation for this unexpected finding is that residents who are mentally present and active may have, and be able to articulate, a more complex set of needs and expectations than residents with more limited cognitive capabilities in terms of, for example, involvement in social activities, hobbies and outdoor events. In this respect, residents with higher RCC, being more present cognitively (and frequently physically autonomous) might demand and require a more customized and interactive demand for services, together with an individual and careful relationship with the caregivers. In contrast, residents with limited levels of RCC, being less present cognitively (and frequently less physically autonomous) often need more basic and standardized services and are less capable of appreciating the quality of the human interaction with the caregivers. Hence, more cognitively alert residents may be more demanding and require greater attention and effort on the part of caregivers, who might then perceive this type of residents as a hindrance to the delivery of more standardized and potentially fewer demanding services, when compared to residents with more limited cognitive capabilities. In turn, this is likely to place greater pressures and demands on caregivers, thereby potentially increasing negative affect and undermining their overall sense of well-being at work. Once again, this represents an important area for further research especially in times of COVID-19, due to which the majority of recreational and social services have been suspended generating dissatisfaction on the part of both residents and caregivers.
Conclusions
Our conclusions are consistent and complementary with those of 36 who, based on a study specifically centered on the well-being of nurses older than 45, emphasized the fact that “patient-care centeredness seems to be an important characteristic of practice for ageing hospital nurses providing well-being at work” (p. 19). Our study, focusing on the extent to which important personal characteristics of nursing home residents affect the well-being of caregivers, hopefully might shed some new light on the interaction between residents and caregivers in the long-term healthcare sector. More generally, while our study is contextualized within the long-term healthcare sector, our findings could be generalized to other sectors of the healthcare industry, as well as to the services industry more widely. In fact, the results of our study are consistent with those from the wider services industry literature according to which the quality of the interaction between customers and employees is seen to depend on the expectations and capabilities of both customers and employees, as well as on their mutual perceptions of the outputs exchange. 37
Scales and related items for constructs.
Mean, SD, ranges, and correlations for all variables.
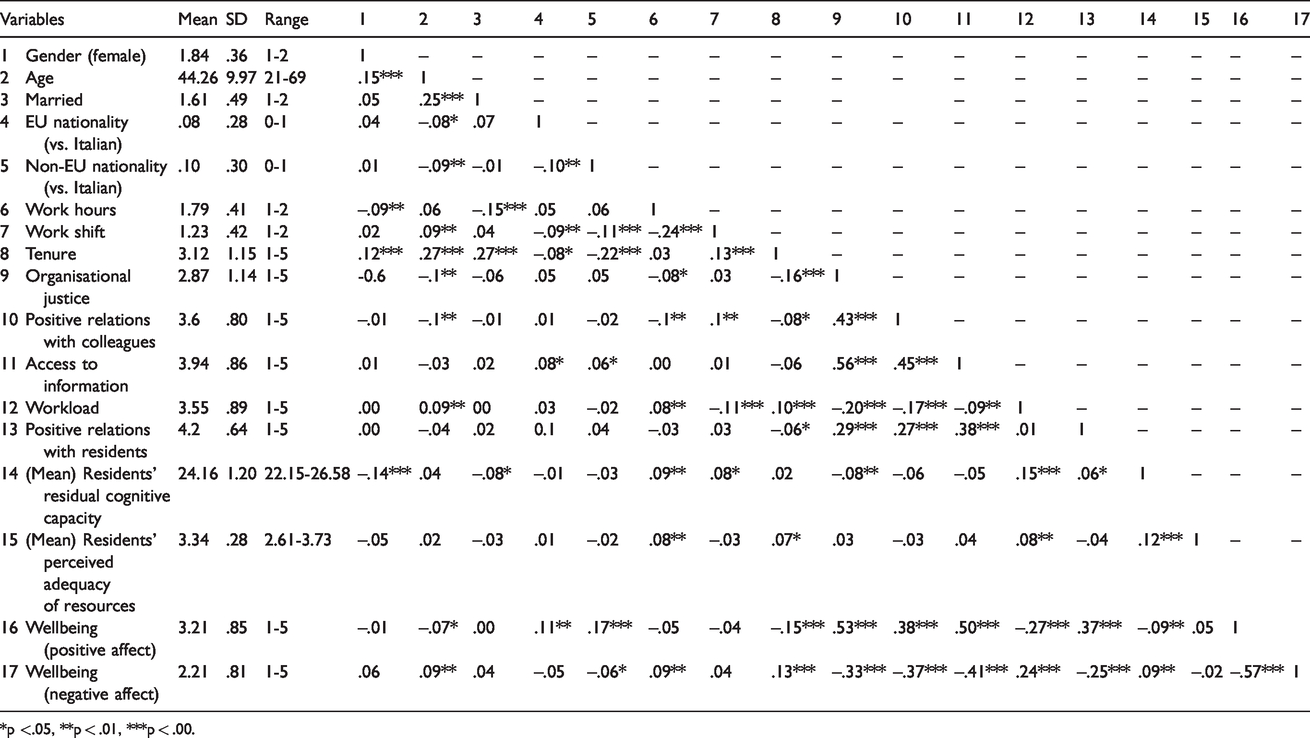
*p <.05, **p < .01, ***p < .00.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.