
Abstract
Background
Waiting times and waiting lists result from an imbalance between the demand for and the supply of healthcare services. 1 Thus, when the demand exceeds the supply, waiting lists ensure making patients wait.
Nowadays, public systems can offer only a limited range and volume of services due to the financial constraints they face. Moreover, a growing ageing population accompanied by the epidemiological transition is widening the gap between the demand for services and the opportunity to pay by public administrations.
2
To date, chronic oncological and neurodegenerative disorders are the principal expenditure voice for the healthcare sector. Failure to anticipate such challenges means less accessibility, longer waiting times, and loss of quality of the healthcare system. Waiting time is a critical item both for patient satisfaction
3
and for the healthcare chain: • Poor clinical outcomes. Time-to-treatment initiation is a determinant of clinical outcomes, especially in cancer care, while there are mixed results for elective care.1,4–6 • Low productivity. Long waiting times cause poor clinical outcomes and stress, which lead to reduced productivity. An empirical analysis of the Fraser Institute estimated the cost of waiting for medical treatment in Canada at $2.1 billion in 2019.
7
• Inequality. Waiting lists are one of the main reasons for unmet needs in healthcare by limiting access to services and care.8,9 In its report on inequalities in access to healthcare, the European Social Policy Network (ESPN) stated that, in many countries, patients bypass waiting lists in the public sector by consulting private specialists or offering informal payments.
8
These practices result in inequalities, unmet needs, and lower clinical outcomes, especially for patients of lower socioeconomic status.
In such a context, governments must consider (and solve) this problem to allow citizens to have a quality care experience and to be compliant with internal laws and European legislation, too. Many Constitutions recognize accessibility to healthcare as a right of the population and not just citizens. 10 European Union (EU) also recognized the right to “timely access health care” in the 16th article of the European Pillar of Social Rights. 11 Furthermore, undue delay for treatment in the country of affiliation is a formal condition for the application of the EU Cross Border Healthcare Directive. 12
As mentioned above, long waiting times are common issues for public administration, particularly for universal, tax-funded, single-payer healthcare systems that operate gatekeeping arrangements.13,14 Gatekeeping for secondary care could be both a resource and a disadvantage: although it can be a way to control the use of resources, it can become a means to ration the delivery of services 15 to the detriment of lower-income patients. Many OECD countries.1,5 face these situations.
This study investigated the waiting times in specific contexts in the OECD area for non-urgent ambulatory care. In particular, the authors selected counties based on specific characteristics and elements such as: • Universal, tax-funded healthcare systems with gatekeeping arrangements. • General practitioners (GP) provide gatekeeping arrangements for outpatient services.
16
• Ambulatory cares are the principal source of health care. The increasing burden of chronic disorders in the ageing population progressively pushes from hospital settings to ambulatory ones. Besides, prevention medicine and risk factor management entail more follow-up and monitoring consultations, thus increasing the demand for outpatient care. Digital health technologies support this shift.
Examples of health systems that do not correspond to the characteristics highlighted above are the Bismarck model system (Germany, France, and the Netherlands) and private and not statutory ones (USA).
To conclude, this analysis aims to identify the principal effective policies or their combination in universal, tax-funded, and single-payer healthcare systems in OECD countries that improve the governance of outpatient waiting times. Furthermore, the authors want to fill a gap in the literature on waiting times strategies through a literature review and to expand current knowledge on policies implemented in those contexts with a focus on outpatient care. In fact, to date, none of the literature reviews17–19 nor OECD reports5,20,21 published on PubMed examine universal, tax-funded, single-payer systems.
Review of the literature: Scoping review
The authors of this manuscript have chosen the scoping review to conduct their analysis among the numerous possible literature reviews. The authors aim to map and summarise the qualitative and quantitative research’s evidence concerning reducing lists and waiting times.
Given the methodological choice of the scoping review, the authors did not conduct a quality assessment of the studies. Moreover, PubMed is the only database where the research was carried out.
The research question under review can be stated as follows.
A waiting list is made up of the list that expresses the number of requests registered for service in ratio to delivery time. This time is primarily measured as the interval between the time of registration by a supplier and the time of performance of the service. Which active governance or operational policies, both within and outside healthcare structures, can improve the management of waiting lists for non-urgent outpatients? Which contextual elements affect the management of waiting lists for the same population target?
Methods: Search string and inclusion/exclusion criteria
In October and November 2022, we searched the PubMed electronic database for studies on health policies and health-related issues using two research strings: 1. (ambulatory)AND(waiting)AND(time*) 2. (outpatient)AND(waiting)AND(time*)
Before entering search terms into the database, the authors pre-set the following search filters: • Publication date: from 2000/01/01 to 2022/09/30 • Species: Human • Text availability: free full text
The authors used a 2-step process to evaluate which studies to include in the review. 1. Selection by keywords: only articles including specific keywords in their titles or abstracts were selected. The searched terms (both singular and plural) were “waiting time”, “waiting list”, “process improvement”, “management”, ”reduction”, “accessibility”, “outpatient”, and “ambulatory”. 2. Selection by content. The authors decided on ex-ante and ex-post inclusion and exclusion criteria which articles include in the review. In particular, the inclusion criteria are: a. Studies that take place in one or more OECD countries with healthcare systems primarily based on universal, tax-funded, single-payer models. For example, Beveridge-type systems (United Kingdom, Italy, Spain, Portugal, Norway, Sweden) and National Health Insurance (NHI) ones (Australia, Canada, New Zealand). b. Studies describing the impact of a policy or combination of policies on waiting time in outpatient/ambulatory care. These included, among others: medical appointments with specialists, minor surgeries that do not require hospitalisation or inpatient care, outpatient medical examinations, etcetera. c. Comparative interventional studies describe the scenario before and after the introduction of a policy. Studies had to present actual cases (not only planned but also expected or simulated) and report quantitative data on the effects of the interventions implemented. d. Publication in English.
On the other hand, the exclusion criteria are: a. Studies in progress, not yet concluded, or protocols only.
Once the selection ended, the authors summarised the articles' content in seven points to highlight the principal characteristics of the studies: 1. Country 2. Type of Study 3. Main policy implemented 4. Level of implementation a. Local (micro) if policies are implemented in a single hospital/clinic. b. Regional (meso) when the implementation contest is a provincial/regional network of hospitals or clinics. c. National (macro) when the entire national territory was the subject of the new policies implementation. 5. Main outcomes of the policy/policies implemented on waiting times. 6. Cost analysis. Although the authors have not conducted an analysis of the articles' quality, they have verified the presence or absence of a cost analysis of the intervention. It is because the presence of this analysis allows more complete considerations concerning the implemented policies. 7. Clinical outcomes analysis. While reviewing the articles, the authors realised that not all contributions analysed the impact of new policies on clinical outcomes. Although the lack of this analysis is not sufficient to exclude the article from the review, its presence is relevant for any considerations on the real impacts of new policies.
Results
The result of the 2-steps analysis, as described in paragraph 2.1, allows the author to select which articles to include in the final review. The analysis has been carried out on both strings of research.
Chronological search sequence 1.
Chronological search sequence 2.

This allowed for two additional articles to be included in the review.42,44 Hence, the number of articles included in the review is 41.
To conclude, the authors also searched other scientific literature for the discussion of the results Figure 1. PRISMA Flowchart for literature review.
Findings
Characteristics of the articles included in the review.
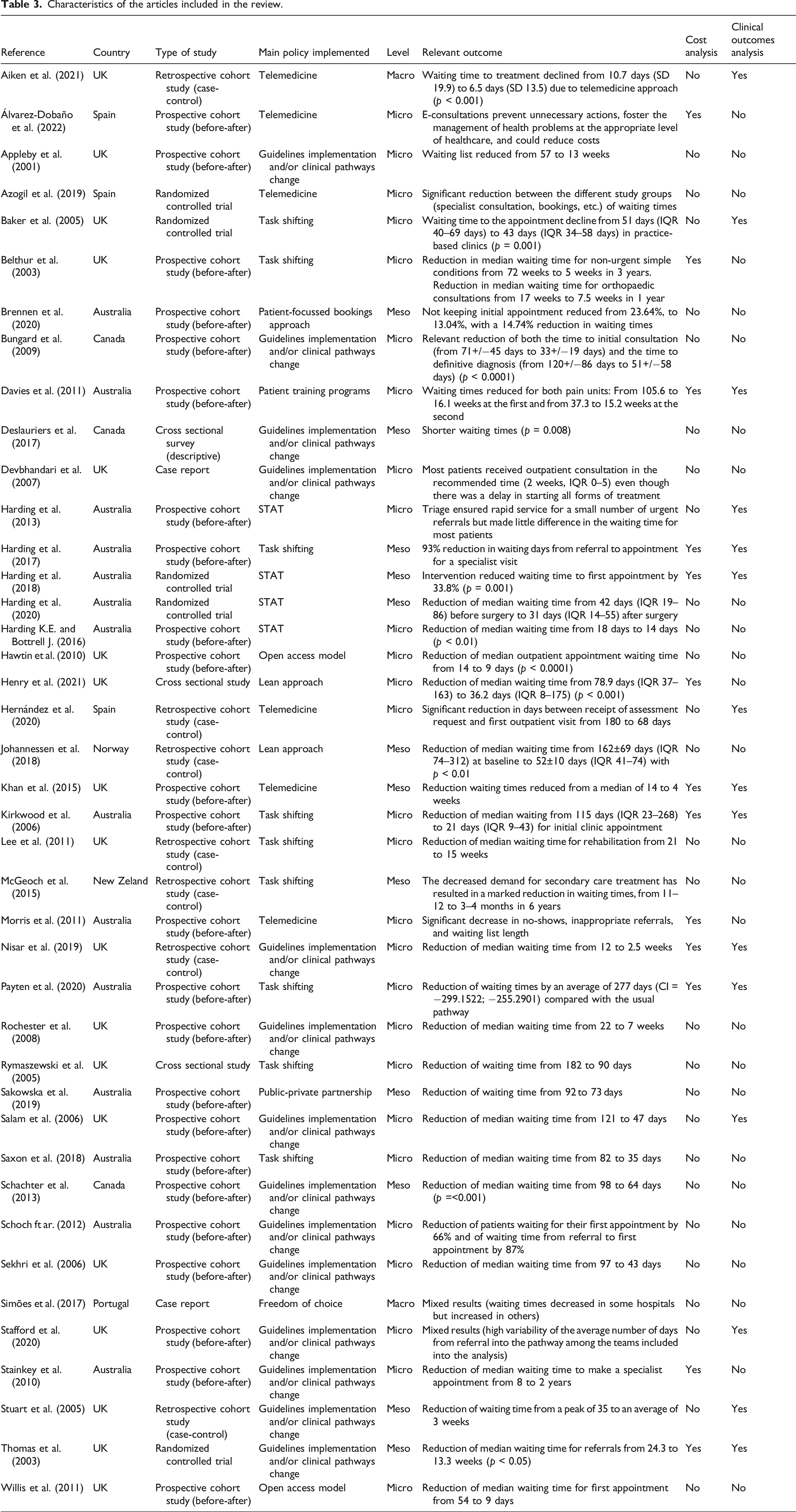
The main policies identified were: guidelines implementation and/or clinical pathways change (14), Task shifting (9), Telemedicine (6), STAT 1 (4), Lean approach (2), Open access (2), Public-private partnership (1), Patient training programs (1), Patients-focused booking approach (1) and Freedom of choice (1).
The majority (24 out of 41, 58,5%) of the articles included in this review were based on prospective cohort studies. Only 5 studies (12%) analysed the impact of interventions through randomised controlled trials. This represents a key-limitation in collecting evidence on policies having a positive effect in reducing waiting times. 26 studies (63%) described interventions implemented at micro level, thus in a single hospital or clinic. Only 2 articles (5%) focused on policies introduced at macro-level. Firstly, this may reflect a great heterogeneity and variability among providers in enacting interventions on waiting lists, delegated to local organisations. Secondly, this may suggest that results of policies implemented at national level are poorly documented in the literature. As discussed below, extension of the review to national reports may potentially enrich the findings of this study.
The prevalence of articles from anglo-saxon countries, such as Australia, Canada, New Zealand and the UK (36 out of 41 studies) may suggest that these are particularly sensitive to the issue of long waiting times for outpatient care.
The majority of studies (28 out of 41) did not include data on intervention-related costs. Similarly, 26 out 41 articles did not illustrate any clinical variable to show the impact of the policies on clinical outcomes.
Discussion
This literature review highlighted several key areas and policies that health systems have focused on to improve the management of waiting lists. It is difficult to prove the causality of the relationship between the implemented policies and the reduction in waiting time as in none of the articles was performed a multifactorial analysis. Indeed, the poor utilisation of randomised case–control studies besides the difficulty in isolating other variables potentially affecting waiting times hindered the identification of clear causation between a given policy and its effects on waiting times. The complexity of the interactions and the potential feedback effects between supply and demand make it particularly challenging to isolate and control the multiple variables affecting waiting times. For this reason, most studies on waiting time governance draw on pre-post observations and consider a given policy as the only independent variable. Despite its practicality, this approach may be misleading and generate biased results. Considering the limitations and difficulties of generalisation, it is possible to hypothesise the existence of a causal relationship between the policies identified and waiting times.
Furthermore, there was large variability in the impact measures the studies applied, which makes a comparison of their effectiveness difficult. This reflects the lack of homogeneity in the definition and measurement systems for waiting time across OECD countries.42,52
Although the implementation of a single policy, rather than a group of combined measures, was rarely observable in the articles included in the review, in most cases a main intervention for each article was clearly identifiable. When this was not possible, the authors decided to group some interventions in a macro-policy called “guidelines implementation and/or clinical pathways change”. The difference with respect to the other policies highlighted in this study lies in the fact that, in the studies classified with “guidelines implementation and/or clinical pathways change”, it was not possible to identify a main policy impacting the system. All the measures implemented have been contextual and not consequential. In particular, the interventions considered into this macro-policy are maximum waiting time, waiting list update, triage, guidelines for triage, no-show policy, and rapid access clinic. Studies classified under this macro-policy included 2 or more measures listed above.
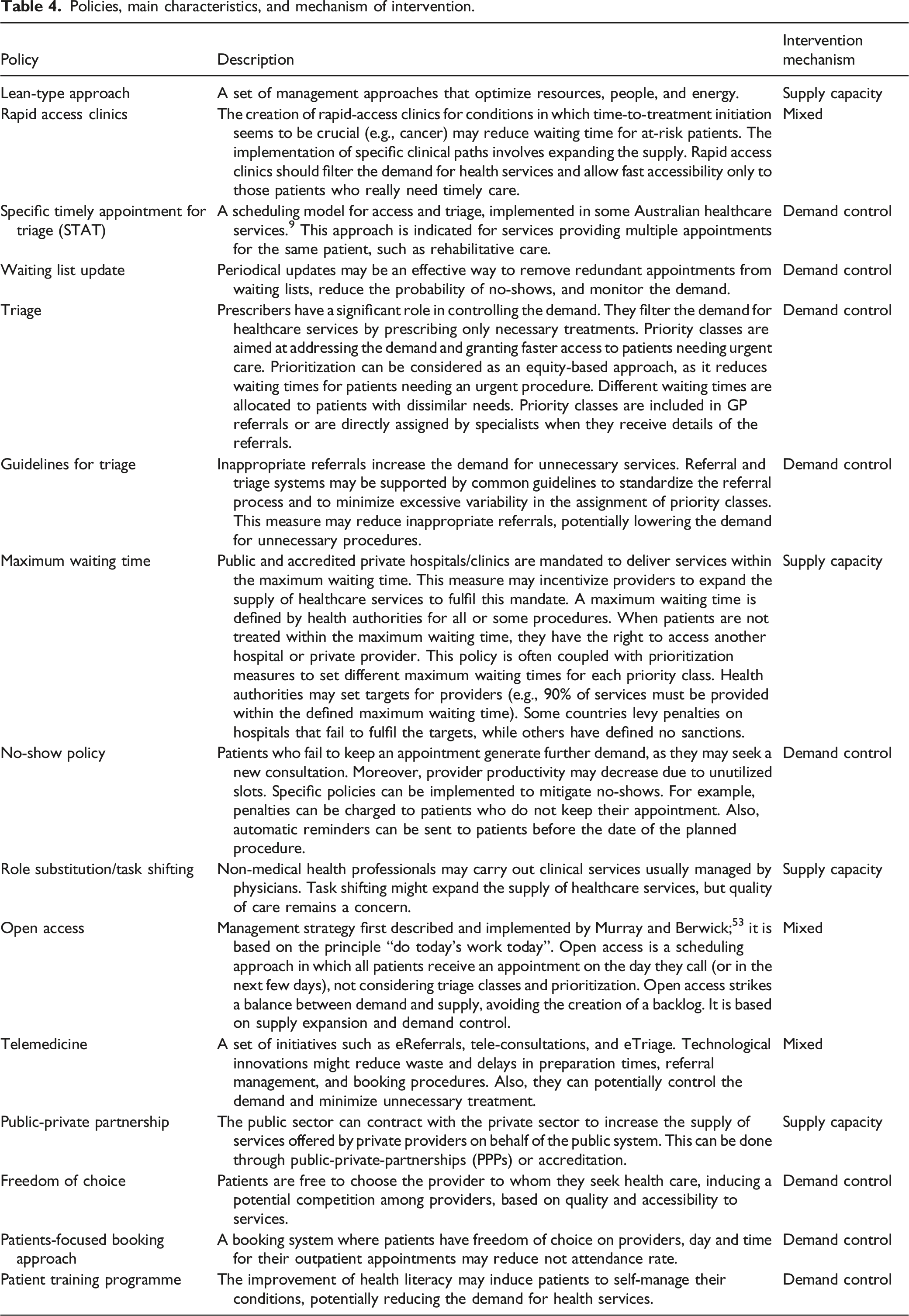
Nonetheless, the authors identified 15 policies for the governance of ambulatory waiting time and grouped them in three main categories (Table 4): 1. Generation of supply capacity. Policies that may strengthen or expand the supply of health services, such as: o Lean-type approach o Maximum waiting time o Task shifting o Public-private partnership (PPP) 2. Control of demand. Policies that may reduce, control, or manage the demand for health services, such as: o Specific Timely Appointment for Triage (STAT) o Waiting list update o Triage o Guidelines for triage o No-show policy o Patient-focussed bookings approach o Patient training programs o Freedom of choice 3. Mixed interventions. Policies that may impact on both the demand for and the supply of health services, such as: o Rapid access clinics o Open access o Telemedicine Policies, main characteristics, and mechanism of intervention.
Among the policies identified in this review, guidelines implementation and/or clinical pathways change is the most employed strategy described in 14 out of 41 studies (34% of articles). This can certainly be explained in how difficult it is to apply a policy without changing the overall picture. Furthermore, observing the results of the studies, the choice to modify various aspects of taking care of patients appears to be efficient from an organisational point of view and with significant effects on the reduction of waiting time. However, the authors underline that the prevailing absence of cost and health outcome analysis leads to strong limitations in the evaluation of such interventions.
Task shifting was described as the main intervention in 9 studies (22%). GPs or allied healthcare professionals (nurses, physiotherapists, speech therapists etc.) participated in tasks traditionally performed by specialists. There are two, often combined, main approaches to task shifting: 1. Non-specialist health professionals triage the patients and filter the demand. 2. Non specialist health professionals provide care or perform examination.
Change in the task mix may allow specialists to focus on more complex cases, while allied healthcare professionals filter the demand and provide care to less severe patients. This is particularly relevant in a scenario of physician shortage, as time savings for specialists lead to potential supply expansion.
In most cases, the active engagement of all professional groups is emphasised and described in detail, highlighting the relevance of solid cooperation and change management in task shifting interventions.
Task shifting approach seems to be common in Anglo-Saxon countries. However, this may be not easily applied in other countries, where legal barriers, cultural and professional silos hinder a less rigid task distribution.
The implementation of telemedicine to shorten waits for outpatient care was described as the main intervention in 6 studies (14,5%). Telemedicine, per se, is a mode of care delivery. For its peculiar characteristics, the authors have decided to consider it as a separate policy. Indeed, it may have a more direct impact on waiting lists by speeding up processes for cases that do not require in-person care, improving accessibility and, thus, reducing the rate of non-attendance. Moreover, it can be combined with other policies, such as triage, list audit and task shifting. Telemedicine provides an innovative tool for supply expansion, particularly in ambulatory services where physical examinations or instrumental diagnostic procedures are not performed. The dramatic increase in the adoption of telemedicine since the beginning of the COVID-19 pandemic has demonstrated its potential capability to substitute face-to-face outpatient consultations. It will likely become even more a part of routine practice as healthcare organisations seek to recover the backlog of services postponed during the current pandemic. In the identified papers, telemedicine include: • Doctor to patient e-consultations:13,53 a service usually provided in-person by a specialist with the patient and now delivered from remote. • E-referrals:
53
clinical data gathered by allied health professionals and referred by specialists through an online data sharing platform. • Doctor to doctor e-consultations:
54
a remote consultation between a specialist, the GP and, if necessary, the patient, to provide guidance to the GP and avoid unnecessary demand to in-person specialist care. • E-triage: (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3417931/pdf/prom-2-151.pdf) remote filtering and auditing of demand conducted by a healthcare professional with a patient.
These approaches have diverse levels of technological complexity. Digital literacy of patients and healthcare professionals is a key-point to be considered when implementing various kinds of telemedicine solutions.
Specific Timely Appointments for Triage (STAT) is an approach described in four out of 41 articles. As mentioned above, this is a method implemented in Australia, which includes measures such as new scheduling system, minimization of touch points and triage. Given its precise protocol and the findings in literature, the authors have decided to distinguish it from guidelines implementation and/or clinical pathways change. STAT, as extensively described in the handbook published by the initiator of the method may be effective in reducing waiting times in services provided to most patients over more than a single occasion of service, so that there is some flexibility in how the service is delivered. However, “It is unlikely to be the answer to long waiting lists in a diagnostic service, for example, where every patient attends for a single standard 30-min appointment”. 15
An additional point to be considered is the limited scenario of implementation. Indeed, STAT has been introduced only in Australia. To further investigate its impact on waiting time, this method should be implemented also in different contexts.
Lean is described as the main intervention in 2 articles (5%). Lean methodology is a well-known approach, aimed at optimising people, resources, effort, and energy of an organization. Its implementation in the healthcare sector is not a novelty. 54 Despite its promising impact, the effects on waiting times should be further investigated.
Open-access model was the main intervention in 2 articles (5%). By approach, open access has a significant positive effect on waiting time. However, the implementation of a “same-day” service is a challenge for many healthcare organisations. Main risks include the economic sustainability of the service and the potential unpredictability of demand, which may generate unexpected requests able to break the delicate balance between daily demand and daily supply.
Other policies described in one article each are: freedom of choice, public-private partnership (PPP), patient-training programme and patient-focused booking approach. The limited findings for the impact of these interventions on waiting time do not allow the authors to make specific hypotheses. The authors believe that, among these policies, the idea of reducing demand by increasing patient health literacy seems particularly interesting. Further investigations should be pursued to better understand the relationship between health literacy, demand and waiting time for health services.
Only 13 (32%) papers included cost analysis, mainly specifying the economic effort in the scenarios before and or after the intervention. Major savings are obtained in some measures involving task shifting. This showed that, assuming an adequate level of care provision, the employment of allied healthcare professionals in tasks traditionally performed by specialists, may represent a cost-effective solution to reduce waiting times. In papers presenting interventions that might lead to cost increase, such as open and rapid access services, costs are not analysed. When considering interventions to reduce waiting times, costs should be given more attention, to guarantee long-term sustainability of the policies. This is even more relevant in periods of budget constraints and shortage of resources.
Data on clinical outcome are analysed in 15 (36,5%) papers. In most cases, adverse events were monitored to understand whether the intervention decreased the quality of care, in comparison with the former scenario. This was particularly important in those interventions involving task shifting, where the maintenance of adequate standard of care, while less experienced professionals are employed, represents a major concern.
In a limited group of cases, interventions did not have a negative impact and improved both the waiting time and the clinical outcome.
Conclusions
Despite the issue’s relevance in many countries, the current literature on ambulatory waiting time governance is scarce and mainly based on observational studies. Randomised controlled studies are rare. Most articles in the present review focused on local interventions implemented in a single hospital or a group of clinics. Limited data transparency and availability may have hindered the identification of policies and the analysis of critical cases. Moreover, the decision of the authors to include only articles written in English could have affected the range of approaches to the governance of ambulatory waiting times identified.
Some policies may have been implemented, even at macro level, without a study being conducted and published in scientific journals. More information on the implementation of policies for the governance of ambulatory waiting times may be obtained from national or regional health authorities either directly through interviews and surveys or indirectly through consultation of official websites and reports. Moreover, the distribution by country may reflect a particular sensitivity to the issue of long waits for outpatient care. In-depth research with a focus on countries such as Australia and the United Kingdom may be warranted. Furthermore, greater transparency of data on clinical outcomes and costs is desirable, to assess the actual cost effectiveness of different policies.
The limited results from this literature review suggest the need for future research extended to other sources and methods. It is desirable that more policies are analysed in studies to allow the academic community and decision makers a more accessible and transparent comparison of different governance approaches through real-world data collected on a large scale.
The limitations of this review notwithstanding, a set of policies for the governance of ambulatory waiting times implemented in OECD countries with universal, tax-funded healthcare systems was identified. This provides a starting point for further analysis and a useful tool for academics, healthcare managers, and policymakers.18,55–66
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.