
Abstract
The COVID-19 outbreak resulted in an unprecedented surge in telehealth utilization. However, the effects of policy enactment on utilization remain understudied in the literature. Our research examines the impact of policy mandates relating to federal incentive programs on telehealth utilization across states during the pandemic by considering technology infrastructure, such as broadband penetration and equipment possession. This study also considers the impact of political orientation and control factors, including income attributes, on telehealth utilization. Considering telehealth utilization in the Medicare program as a test case, this study employed the partial least square and structural equation model to analyze data from the Centers for Medicare & Medicaid Services, the American Community Survey, and the Microsoft Airband Project to draw inferences. Our study finds that telehealth legislation, broadband penetration, political orientation, and control factors have a direct significant impact on telehealth utilization, whereas incentive programs and equipment possession have an indirect impact through broadband penetration.
Highlights
- State-level data are used to investigate the impacts of factors on telehealth use - Impact of policy mandates on telehealth utilization across US states is studied - Impact of incentive programs on telehealth utilization is studied - Telehealth legislation, technology infrastructure, and politics have impact on TU - PLS-SEM is used to investigate the impact of factors on telehealth utilization
Introduction
The sudden and significant surge in telehealth utilization began with the onset of the COVID-19 outbreak has reached 38 folds higher than pre-COVID-19.1,2 Due to the need to protect patients from exposure to COVID-19 and implementation of lockdown policies during the pandemic, the federal regulatory waiver13,4 could explain the upward trend of telehealth utilization. The issue of regulation, reimbursement, and technology has been concluded as most important issues in telehealth in the American Medical Association (AMA) report.5,6 The Public Health Emergency Declaration (PHE), which empowers telehealth utilization, has been extended several times, and it points to the importance of considering policy’s effectiveness for telehealth utilization.
Telehealth encompasses the utilization of telecommunications and digital communication technologies to remotely access health care services and manage health care. This broad field includes various services such as medical consultations through video conferencing, remote monitoring of patients’ vital signs, sharing of electronic data, and dissemination of health-related information via digital platforms. Common modalities of telehealth include videoconferencing, store-and-forward technology, and remote patient monitoring. The primary objective of telehealth is to enhance the accessibility of health care, particularly for individuals in remote or underserved regions, and to increase the efficiency and convenience of health care delivery. 7
Based on the preexisting barriers and unleashing of telehealth utilization after the pandemic, the discussion of policy-driven measurement or regulation remains very limited. Hence, this research sought to understand the determinants of telehealth utilization via state-level data in the wake of the COVID-19 pandemic. To examine the association between determinants and utilization of telehealth, this research aimed to design a quantitative model and consider how telehealth legislation, technology infrastructure, incentive programs, political orientation, and control factors impact telehealth utilization.
The statewide comparison of telehealth utilization.

Note: The value in parenthesis is ranking of 51 states.
Figure 1 illustrates the conceptual model that this study designs for deepening the discussion. Conceptual model of telehealth utilization.
The conceptualization of technology infrastructure reflects the capability of bridging healthcare demand and supply via a telehealth approach. Specifically, the technology infrastructure in this research consists of broadband penetration and equipment possession.
Furthermore, the prevalence of digital equipment, such as laptops and mobile devices, shows the capability of accessing healthcare services via broadband networks. Thus, we consider
Since broadband penetration has expanded over decades and is regarded as an important driver for the digital divide and disparity in rural and remote areas,
12
the federal government initiated incentive programs dating back to pre-COVID-19 to increase the broadband penetration rate. These efforts help to improve patients’ accessibility to healthcare services and enhance physicians’ cooperation. However, there is no holistic study at the state level, so it has made it difficult for stakeholders to foresee the future trend of telehealth utilization. Therefore, this study also paid special attention to the dynamic impact on telehealth utilization of the
The
The purpose of this study was to construct and evaluate a model to explain telehealth utilization from a methodological standpoint. The well-designed model could capture the variation between explained factors and explanatory factors, and thus identifies the significant factors that have an impact on telehealth utilization through this mechanism. The modeling tool, partial least square and structural equation model (PLS-SEM), would be applied to achieve this goal.
Since this research takes these factors into account to gain a deeper understanding of telehealth utilization after the pandemic, the outcome will significantly fill the research gaps and provide useful insights for policymakers about the most important factors that affect telehealth utilization. Misallocation of healthcare resources and health disparity have been perennial issues that worsened during the COVID-19 outbreak. While telehealth utilization showed rapid growth under the regulation waiver during the COVID-19 outbreak, and particular services will become permanent legislation, the conclusion of this research will also indicate the direction to reallocate and optimize sparse resources.
The remainder of this paper is organized as follows. Next is the proposed research framework, model, and data sources. The results and discussion follow, and finally come the concluding remarks.
Methodology, research model, and results
Methodological flow and hypothesis
Figure 2 illustrates the step-by-step methodology used for this study. The methodology started with data identification and collection. At this first stage, the abstract constructs as well as the indicators of the constructs were identified and collected using several sources. After the data were prepared for the analysis, the PLS-SEM model was developed to test the hypotheses and see the impacts of factors on telehealth utilization. Stage 3 explained the results and the discussion followed. Methodology framework flow.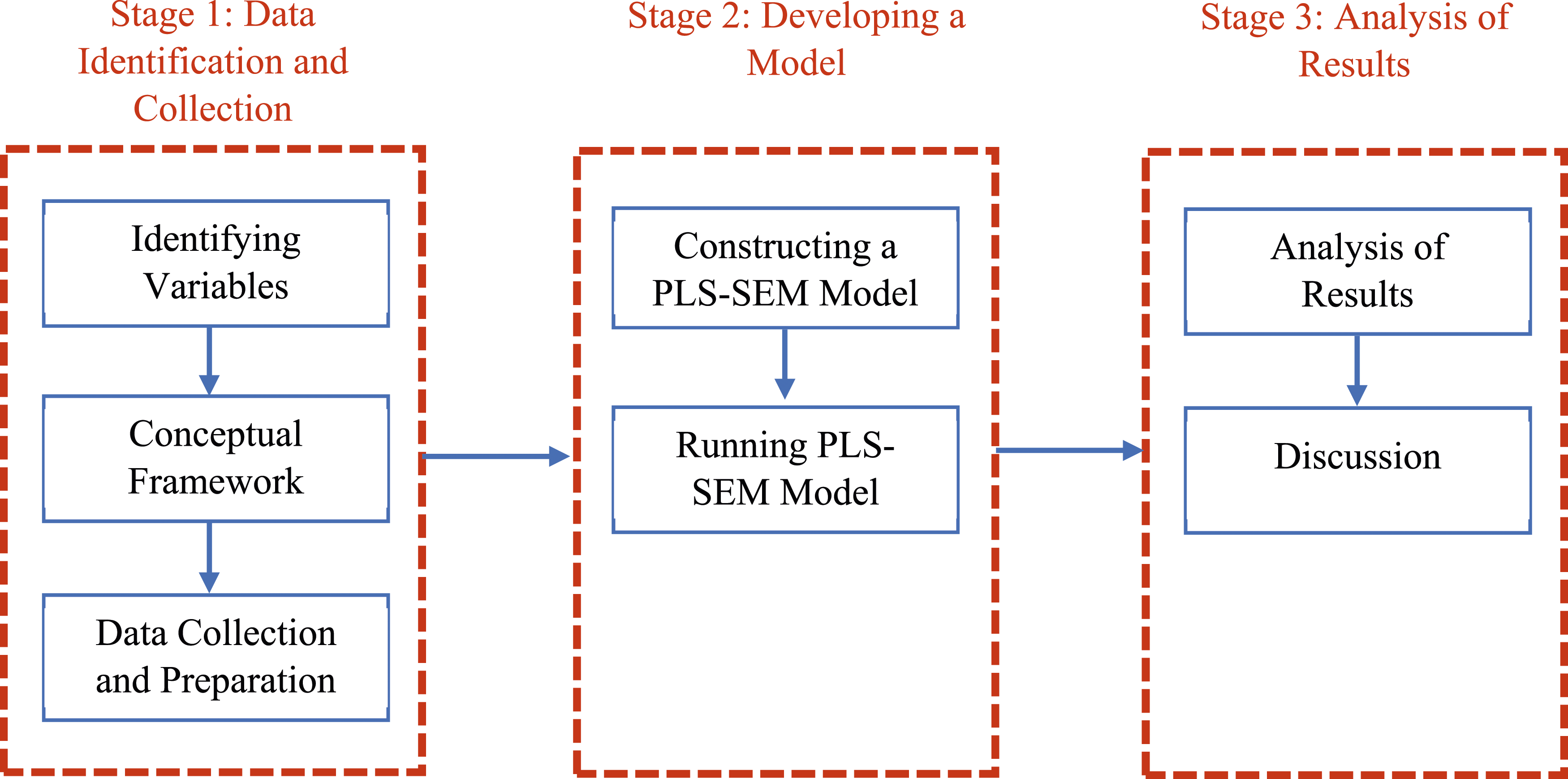
Based on the discussion above, they are six hypotheses as follows.
There is very limited literature in terms of regulation and policy in the topic of telehealth. Some commentary literatures indicated the regulatory barrier 19 by using qualitative analysis. Therefore, it gives reason for hypothesizing telehealth legislation on the utilization.
Telehealth legislation is positively correlated with telehealth utilization. After the COVID-19 pandemic epidemic, telemedicine use soared, and internet infrastructure promptly became an immediate issue. While broadband capacity (bandwidth or congestion) may be even more important in metropolitan areas,
20
broadband penetration in rural areas is a fundamental and long-standing issue that affects health care.
21
Therefore, H2 validates the hypothesized relationship between broadband penetration and use of telehealth:
Broadband penetration is positively correlated with telehealth utilization. Incentive programs have been widely used in human resources to stimulate employees’ performance and working productivity.
22
They are also commonly applied in healthcare management to achieve long-term goals of reducing medical expenditures.
23
Since the design of incentive programs features aims for a particular goal, it was also used to enhance the propensity for broadband penetration. The consideration of incentive programs in this research resulted in a better understanding of how policy-driven efforts lead to telehealth utilization in minority communities such as lower-income families. The indicator of the incentive program analyzed in this study is the Lifeline program, managed by the Federal Communications Commission (FCC), which supports minority communities in accessing telecommunication technology. Eligibility for this program is based on specific income criteria. While the program subsidizes high-speed internet for low-income households, it does not require he use of telehealth services. Hence, hypothesis H3 is proposed to examine the association, as follows:
Incentive programs are positively associated with broadband penetration. Regarding telehealth as a healthcare network system, communication either among patients and physicians or among physicians should require not only edges but also nodes that require the capability to merge into the network. Therefore, physical machines or devices will empower patients and physicians to participate in the network. Moreover, the ownership of technology devices is regarded as a derived demand for broadband infrastructure. Furthermore, equipment and healthcare access by Medicare beneficiaries have shown a significant relationship.
24
In particular, telehealth is a combination of telecommunication technology and healthcare services to bridge physicians and patients. Thus, ubiquitous digital devices and equipment are associated with telehealth utilization. Hence, this study hypothesized that equipment possession and broadband penetration are associated (H4).
25
The indicators for equipment possession are defined as the percentage of households possessing laptops and smartphones. Specifically, the “Laptop – Percentage of Possession” encompasses ownership of desktops, laptops, netbooks, or notebook computers, as defined by IPUMS USA (2021). This excludes GPS devices and other household appliances with limited computing capabilities. Additionally, web cameras are not included in this measure. During the pandemic, numerous states permitted the use of audio-only telehealth for mental health services, potentially mitigating concerns regarding the necessity for web cameras.
Equipment possession is positively associated with broadband penetration. The political orientation often could reflect the different value Propositions
26
and attitudes toward adopting new technology. Examining the progress of releasing low-power radio spectrum,
27
the debate about media consolidation and justice
28
have indicated the importance of considering the political spectrum to improve public well-being. The experience learning from the pandemic has shown that telehealth could be considered a proxy of policy instrument to deal with public health emergencies, and the political orientation can foresee the propensity of using telehealth in dealing with public health emergencies. This study aims to explore whether political orientation, represented by the red-blue spectrum, influences telehealth utilization. In the analysis, positive values indicate red states and negative values indicate blue states. If the results show statistically significant positive values, it suggests that red states have a higher tendency to use telehealth. Conversely, statistically significant negative values would suggest that blue states use telehealth more. Hence, it is appropriate to consider the impact of political orientation on the research model.
Political orientation is associated with telehealth utilization. The benefit of applying control factor is to explain whether there are any inherent differences across states. The household income was used in this research to be a control factor and validate that the higher the state’s household income shows, the higher the telehealth utilization observes. Therefore, the final hypothesis tests whether there is an association between control factor and telehealth utilization.
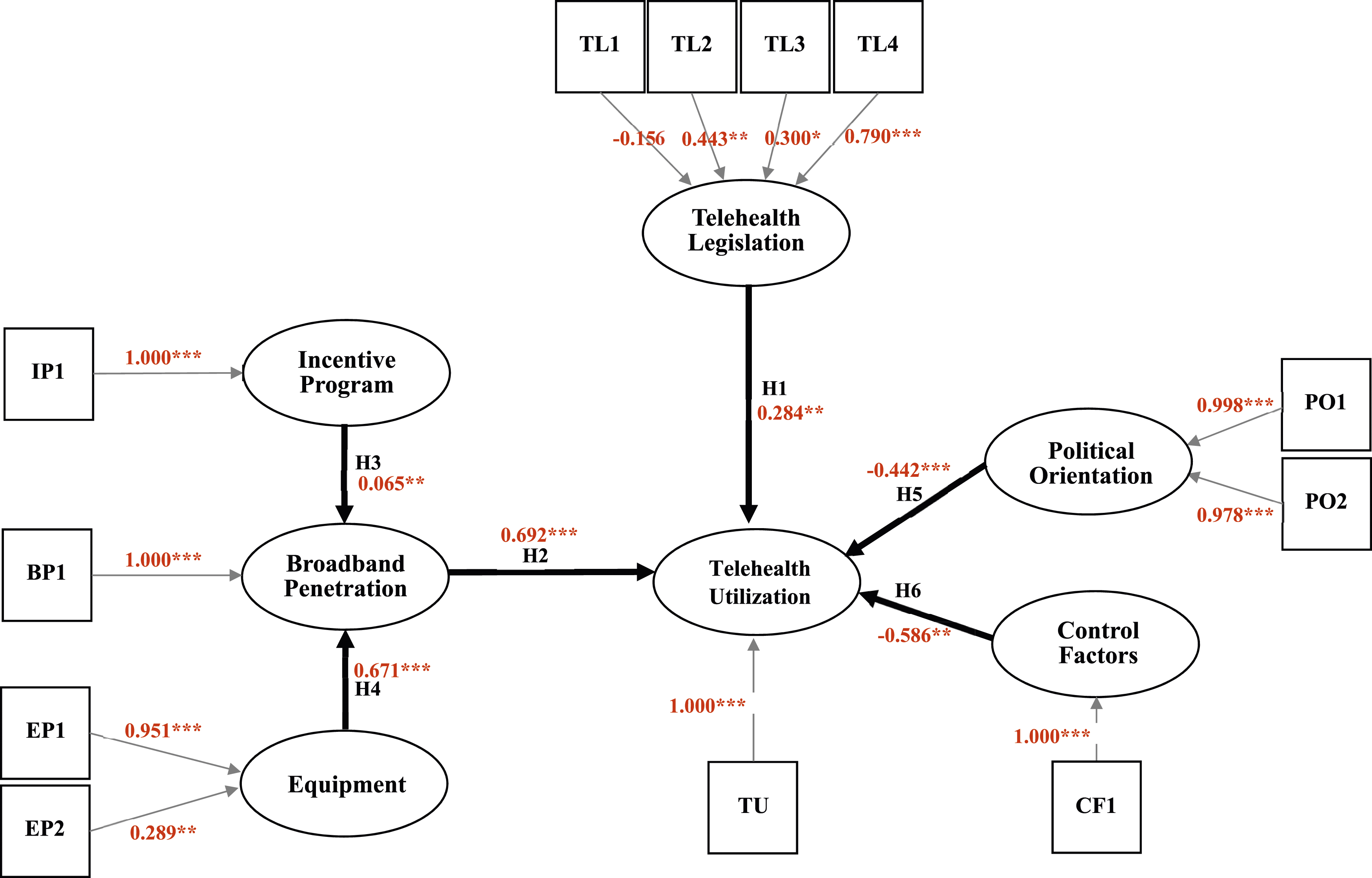
The control factor construct is positively associated with telehealth utilization. Figure 3 demonstrates the proposed conceptual model with the estimation result, showing all the indicators and their relationships with telehealth utilization. The oval represents the construct and the square stands for the indicator. The hypotheses are shown on the arrows between the factors and telehealth utilization in this figure. Moreover, indicators that help measure the latent variables (constructs) are included. Because latent constructs are abstract and cannot be measured directly, the indicators allow them to be measurable. Formative constructs were created because they are affected by the identified indicators. Table 3 presents the latent constructs (factors), their indicators, indicator acronyms, and definitions.
The result of standardized path coefficients in structural model.
Data sources
The data on telehealth utilization from the 51 US states were obtained from the CMS (2021). The data for the telehealth legislation construct that incorporates four different indicators were collected from the Center for Connected Health Policy (CCHP) (2022), Dills (2021) and the Foley’s 2021 report (Foley, 2021). The broadband penetration data was acquired from Microsoft (Microsoft’s Airband Initiative, 2021). 2 The percentage of broadband usage in the U.S. served as an indicator for this construct. Microsoft Initiative focuses on addressing the challenges of low broadband penetration in rural areas, with the goal of enhancing digital connectivity. Additionally, the possession of equipment was considered as another construct in the model. To measure this, we used two indicators: the percentage of laptop and smartphone possession. These data were sourced from the American Community Survey (ACS) via IPUMS USA (2021). The control factor construct includes household median income which sourced directly from the ACS (IPUMS USA, 2021). The state population was indirectly considered by means of telehealth utilization per 1000 state population. Since the ACS dataset comes an annual survey using nationwide sampling, the appropriate sampling weight that relies on census population had to be considered. It is also important to note that the census does not typically cover all types of data, such as laptop ownership. Therefore, American Community Survey (ACS) data was used in this study.
The incentive program data indicate the number of Lifeline subscribers retrieved from the Universal Service Administrative Company (USAC) 2020 dataset, which partners with the FCC. Finally, the data on political orientation involving the Cook Partisan Voting Index (PVI) indicator was obtained from the Cook Political Report published in 2016, and 2020. The PVI quantifies whether each state is blue (B) or red (R) 3 with the increment of Senate seats and has a numerical value whereby a positive value represents that the blue party dominates, and a negative value shows that the red party dominates. Moreover, PVI is an indicator at the state level in the U.S. that quantifies the average partisan voting share in presidential elections relative to the national average. It is important to note that PVI does not measure changes in Senate seats but is consistently based on four-year term presidential elections. The index is typically expressed as D + number for Democratic lean and R + number for Republican lean. For analytical purposes, we have recoded D + number as a negative value (-number) and R + number as a positive value (+number). Therefore, PVI is not related to Senate seats but only PVI is only about presidential election ballot votes (Cook Partisan Voting Index, 2021; Ballotpedia, nd).
Summary statistics.
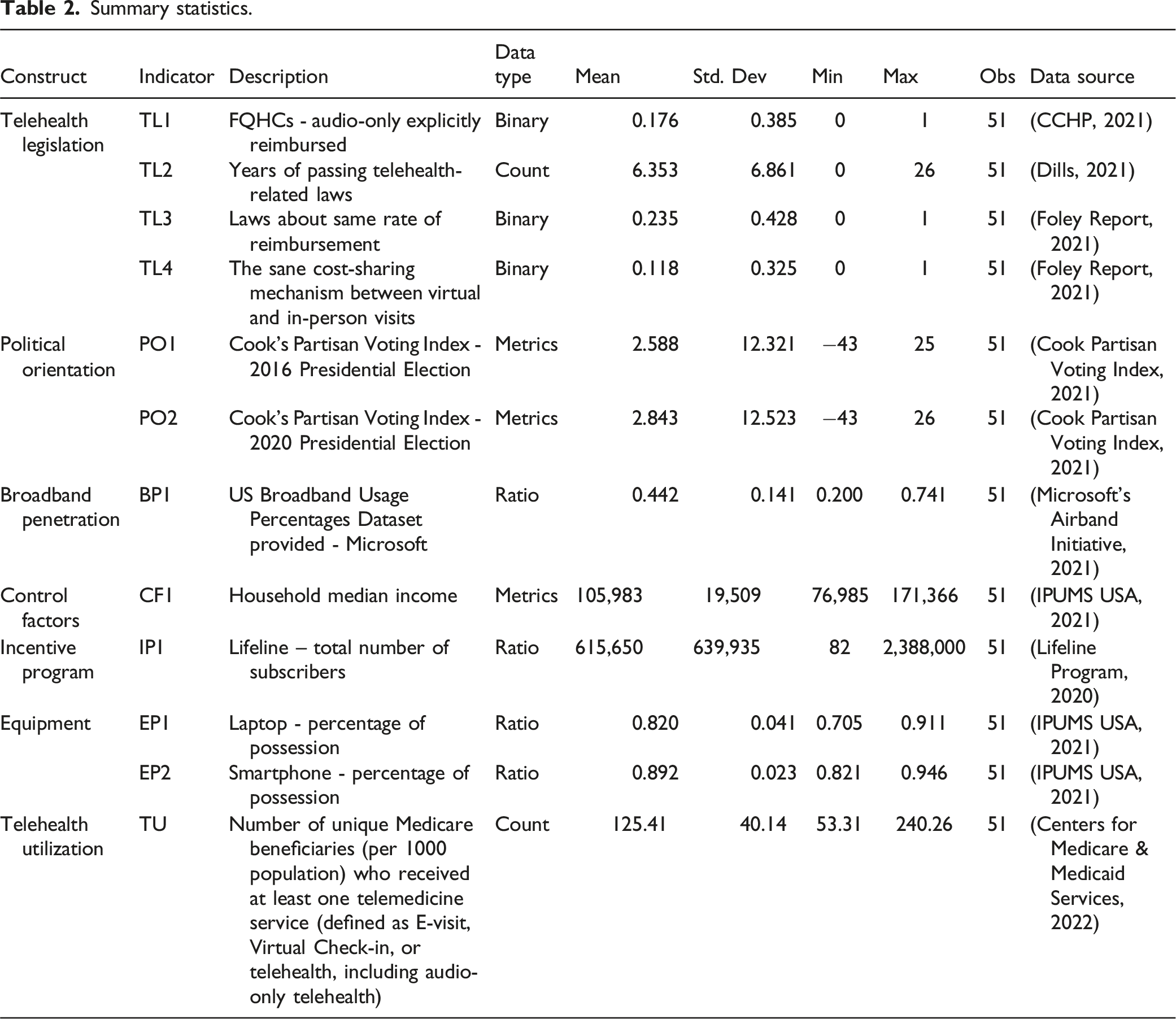
As illustrated in Table 2, Microsoft data indicates an average broadband availability of 44.2%. While there may appear to be a causal relationship between broadband and equipment possession, in our model, we utilize these factors as controls to aid in explaining telehealth utilization. It is important to clarify, however, that these factors should not be interpreted as indicating a causal relationship. Fierce Network (2022) provides detailed information on how Microsoft calculates broadband penetration. The methodology employed by Microsoft in this project significantly differs from that used by the American Community Survey (ACS). While the ACS conducts nationwide sampling, Microsoft aggregates public data from multiple sources including the Census Bureau, the FCC, BroadbandNow, and its own broadband usage data, which makes direct comparisons challenging.
Data analysis
The PLS-SEM technique used in this study has been widely applied in social science research. 29 PLS is an alternative to SEM and handles all types of variables. Different from SEM, it works even with single-item constructs. Moreover, it is insensitive to sample size considerations 30 and is particularly useful in generating estimates even with very small samples, such as 30 observations. In addition, PLS handles both reflective and formative constructs differently from SEM. For example, the constructs in this research, telehealth legislation, broadband penetration, etc., are all integrated and composite variables, 31 and they are suitable to be used as formative constructs 32 because changes in one or more indicators cause changes in the latent variable.
According to the conceptual model shown in Figure 3, the path model was expressed mathematically. In the formative measurement model, latent variable
Therefore, the latent variable 

Modeling result
This research first discusses the result of the measurement model, then the result of the structural model.
Convergent validity in the formative measurement model can be performed via redundancy analysis 33 that uses exogeneous formative latent constructs to predict endogenous reflective latent constructs. Since only formative and single-item constructs were specified in this research model, the AVE results are not applicable in this research model specification. Table A1 is included in the appendix to show the standardized loading score for all measurement models. Loading scores are mostly significant and justify model effectiveness.
Standardized path coefficients with bootstrapping.
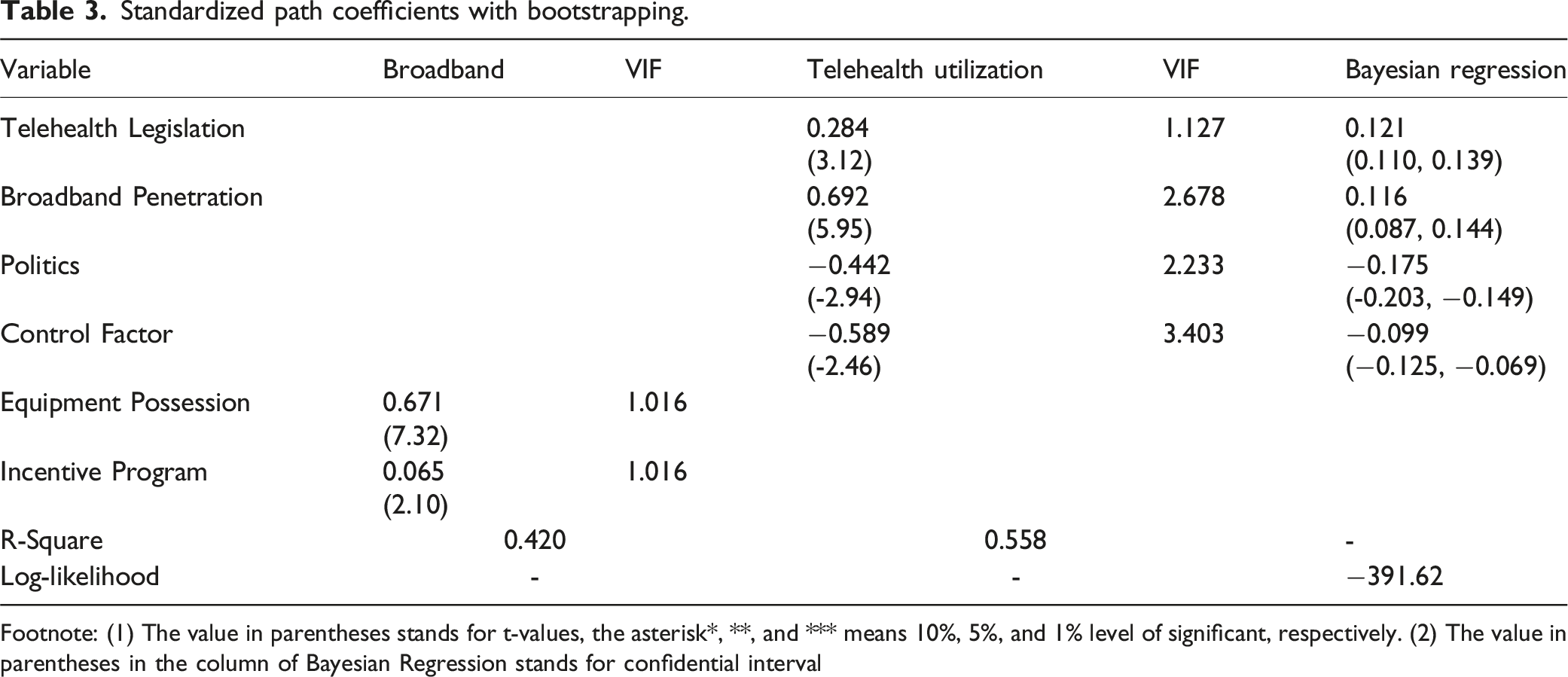
Footnote: (1) The value in parentheses stands for t-values, the asterisk*, **, and *** means 10%, 5%, and 1% level of significant, respectively. (2) The value in parentheses in the column of Bayesian Regression stands for confidential interval
First, the roles of EP and incentive programs in relation to broadband penetration were evaluated. Both were significant in the explanation of broadband penetration and had a positive impact. The result also confirmed the hypotheses H3 and H4. Second, the role of the mentioned constructs on TU was observed. The results show that telehealth legislation was significant under the 5% significance level, indicating that the presence of telehealth-related regulations was a significant driver to enhance TU. So, the hypothesis H1 was confirmed. From the policy perspective, this result indicates policy can have an impact on the TU. Technology infrastructure, including broadband penetration, was also statistically significant and had a positive impact in the explanation of TU. This result not only supports the hypothesis H2 based on the conceptual framework but also validates the importance of broadband penetration on the delivery of healthcare information and services.
In addition, the negative impact of political orientation showed that the blue states had higher TU than the red ones. So, the hypothesis H5 was confirmed as well.
For the CF construct, the results show that it had a negative significant effect and played an important role in controlling unobservable state-wise heterogeneity. Therefore, the result confirmed the hypothesis H6. This is also consistent with the existing literature. Darrat et al. (2021) have demonstrated that in states with lower average incomes, telehealth utilization is comparably higher, particularly when telephonic visits are included in the definition of telehealth. This suggests a possible preference for telehealth in regions where access to traditional healthcare services might be limited. Additionally, Yu & Hagens (2022) provide evidence that individuals in higher income states might prefer in-person visits over telehealth, potentially due to better access to healthcare facilities or greater trust in face-to-face medical consultations.
Moreover, it is important to consider the limitations imposed by our study’s smaller sample size. This constraint might amplify the influence of unobserved variables that are not fully captured by the control factors in our model. Consequently, the impact of income on telehealth utilization in our analysis could be less generalizable.
Discussions and limitations
This research focused on TU and its determinants. Understanding and identifying important factors that impact TU in a macro level study could indicate to policymakers the appropriate design of regulations and benefit for telehealth ecosystem. Although telehealth has developed over several decades, regulatory limitations and other barriers have prevented wider adoption. In particular, regulatory restrictions could be regarded as manipulable measurements to influence large-scale utilization. Compared with technological and clinical barriers, regulatory barriers, such as reimbursements in services and rates, might cause more obstacles to utilization. 34 Hence, the result from this study gives the consistent opinion with other literature and suggests that the policy plays a crucial role to direct healthcare development.
On the other hand, the various regulation waivers during the COVID-19 pandemic allowed the rapid adoption of telehealth to ease the impact of COVID-19 and create a new vision of considering telehealth as an alternative delivery model in clinical practice to either substitute for or complement conventional in-person visits. Prior literature on the clinical setting has suggested that telehealth could be a cost-effective healthcare delivery model. Hence, the discussion of legislative issues should evoke public attention to guide and optimize resource allocation in the healthcare industry. Moreover, the diversification of regulations and state statutes, such as the same reimbursement rates and services between in-person and virtual visits, have led to the difficulty of contemporaneous discussion. This study designed and demonstrated a quantitative modeling approach to consider various legislative factors together.
The discussion of broadband penetration is another manifest contribution of this research. The existing literature considering broadband penetration in the discussion of its impact on TU has shown that our results are consistent with what this research provided.35,36 Since this research used Medicare beneficiaries as a test case, the effect of broadband penetration on TU could imply that improving healthcare accessibility for elderly people should prioritize the focus on increasing broadband penetration. Since the term “digital divide” has been promulgated for decades, the FCC has created several programs and funded projects to shrink the gaps. 37 Promoting broadband penetration is considered an important policy to ameliorate economic development, education quality, and health disparities. Incentive programs—from Lifeline and the Emergency Broadband Benefit to the Affordable Connectivity Program—have been initiated and targeted to minority communities to advance the capability of using broadband to acquire benefits from connectivity. 38 However, the lack of understanding of whether the fruit of these policy-induced resource reconfigurations has trickled down to compensate for the deficiency has aroused apprehension. Therefore, considering an incentive program in the research framework could prevent either under- or over-estimating the impact of broadband penetration on TU.
Equipment possession (EP) also has an impact on broadband penetration. While the literature indicates that technological barriers hindered TU before the COVID-19 pandemic, 39 the rapid surge of TU after the pandemic seems to suggest that technological barriers might be outweighed by other factors or be less important. Owing to the prevalence of low-cost and ubiquitous digital devices and easily operable telehealth portals, the issue of technological barriers should become less important in explaining TU. Moreover, while individual-level analyses often focus directly on the user’s possession of digital devices as a determinant of telehealth utilization, our study adopts a macro perspective, emphasizing the role of broader technology and infrastructure. This approach is particularly relevant in discussions of policy and regulation, where state-level interventions can significantly impact the availability and efficacy of telehealth services. Accordingly, our findings contribute to the discourse on the need for comprehensive technological frameworks that support telehealth services at a larger scale, as discussed in Kotsopoulos & Connolly (2014). This macro-focused research aims to complement the existing literature by providing insights into how infrastructural and policy-level factors collectively influence telehealth adoption across different states.
Given the scanty research relating political orientation to telehealth, the political spectrum has been recognized as a good proxy to explain and predict the development of various health ITs. From the liberal perspective, healthcare continuity and accessibility by means of various health ITs often incline to paying more attention to eliminating healthcare disparity. In contrast, conservatives focus on the healthcare market structure that harmonizes demand and supply. Since this study examined TU during the pandemic, the result suggests that liberal-orientated states have more utilization and reflect a short-term perspective, taking advantage of telehealth implementation to deal with the public emergency. Conventionally, the blue spectrum in the US was presumed to be regarded as progressive, especially in technology adoption. Thus, the modeling result does not contradict preexisting viewpoints. 17 Since the short-term pandemic impacts have waned, whether TU in the long term could be sustained and reduce overall healthcare costs is an issue worth noting.
The most significant limitation in this research was the lack of detailed TU data, which directly leads to a small sample size issue. Moreover, less data granularity leads to difficulty in modeling operability and lowers the degrees of freedom. PLS-SEM was used as a solution method to handle this issue. Except for the TU data, the remaining indicators are all publicly available, with granularity up to the county level. Even though the trend of TU declined from the peak, current utilization is still much higher than before the pandemic outbreak. 40 Considering that debates around the legislation will continue, and TU will continue to be an important issue in the public health area, federal government agencies, such as the Centers for Disease Control and Prevention (CDC) and U.S. Department of Health and Human Services (DHHS), should pay more attention to data transparency issues, which could allow more public discussions.
Conclusion and further directions
This research attempted to understand the factors influencing TU during the COVID-19 pandemic. The conceptual framework designed in this research helped to outline the research scope, which included legislation, technology infrastructure, political orientation, and control factors. The creation of a construct represented in the conceptual framework has benefited from the various publicly available datasets. PLS-SEM was used because of the small sample size. The results of the PLS modeling show that legislation, broadband penetration, political orientation, and control factors all significantly affected TU. The conclusions of this research result in a deeper policy understanding following the COVID-19 pandemic to design and operate a sustainable healthcare delivery model.
The results highlight the significance of the technological infrastructure required for effective operation of the healthcare system, as well as the significant contribution of the suggested conceptual framework pointing to the need for appropriate legislation. Moreover, the results take into account the significance of political orientation and numerous other controlling aspects in the decision-making process. While planning and putting any project into action, policymakers and other stakeholders must take these findings into account. To address the success of TU during the COVID-19 pandemic, a comprehensive and all-encompassing conceptual framework has been developed. The merit of the methodological rigor based on the limited telehealth literature by means of macro level datasets and the outcome of this research indicate the importance of the transparency and literacy of telehealth datasets in the public domain. It also envisions the future directions of this research.
To further strengthen our study’s conclusions regarding the lasting impact of telehealth policies, we emphasize the merits of a longitudinal analysis. Tracking telehealth utilization trends over time, particularly post-legislation enactment, can provide a more comprehensive understanding of how these policies influence telehealth adoption and utilization patterns. Longitudinal data would allow for the observation of sustained effects and potential changes in usage behavior, offering valuable insights into the effectiveness and long-term benefits of telehealth initiatives. This approach could also help identify any unintended consequences or areas needing further policy adjustments, thereby contributing to more robust and informed decision-making in healthcare policy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Standardized loading scores. Note. The values out of parentheses in this table stand for standardized loadings, the values in the parentheses mean t-values. * = 10% level of significance. ** = 5% level of significance.*** = 1% level of significance. FQHC = Federally Qualified Health Center; N/A = Not Applicable; VIF = Variation Inflation Factor.
Indicator/construct
Telehealth legislation
Political orientation
Broadband penetration
Control factors
Incentive program
Equipment possession
TL1 - Audio-only explicitly reimbursed
−0.156 (−0.46)
TL2 - Law - Same reimbursement rate
0.443 (1.65)**
TL3 - Year payment parity was adopted
0.300 (2.13)*
TL4 - Cost-sharing regulation
0.790 (2.96)***
PO1 - Cook Voting Index - 2016 presidential election
0.998 (35.07)***
PO1 - Cook Voting Index - 2020 presidential election
0.978 (26.86)***
BP1 - Broadband usage percentage
N/A
CF1 - Household income
N/A
IP1 - Number of subscribers
N/A
EP1 - Laptop possession
0.951 (14.78)***
EP2 - Smartphone possession
0.289 (1.91)**