
Abstract
Background
While health systems are primarily designed for acute health issues, managing life-long conditions often results in chronic care discontinuity. This refers to situations where a chronic patient’s planned care fails to actualise.
Research Design
This study descriptively explores the reasons behind chronic care discontinuity in outpatient care.
Data Collection
Data was collected via interviews and a focus group with healthcare professionals, and a patient survey specifically targeting chronic abdominal patients.
Analysis
Using grounded theorising the Discontinuity of Chronic Care (DoCC) framework was developed, to identify and categorise reasons behind chronic care discontinuity.
Results
The framework reveals that reasons for discontinuity can be largely divided into healthcare system related factors—including caregiver, technological, and process challenges—and patient-related factors such as situational and internal psychological challenges.
Conclusions
The DoCC-framework provides a valuable tool for analysing various patient processes, offering healthcare managers insights to improve the management of chronic patient journeys. Additionally, it guides healthcare professionals to better focus their development efforts on challenges they have the capacity to address.
Keywords
Introduction
Chronic diseases continue to present significant challenges for healthcare systems worldwide. 1 As people age the incidence of chronic diseases tends to rise dramatically. 2 With higher life expectancies becoming common, we can expect the burden of chronic diseases to increase in the future.3,4 The increasing prevalence of chronic diseases could even be referred to as an epidemic. 5 Though the growing number of chronically ill is a known fact, many healthcare systems remain designed for acute and episodic care needs.6,7 Such design can lead to the neglect of healthcare management strategies that would focus on proactive and comprehensive care, which would in turn help maintain overall health, quality of life, and manage chronic illnesses better. A clearer focus on the management of chronic diseases has been shown to lead to improvements in patient health outcomes, quality of life, and in the end, reduce costs incurred by the healthcare system. 8
Chronic conditions have been studied from many perspectives, and frameworks, such as the ‘Chronic Care Model’ 9 and ‘Quadruple Aim’ 8 for better managing chronic care processes have been both proposed and implemented. In addition, there is existing evidence on the negative effects of care discontinuities such as worsened treatment outcomes, 10 higher hospitalization rates, 11 and increased costs.12,13 Thus, it is pivotal that the phenomenon of ‘discontinuity’ be properly defined, understood, and studied so that effective interventions can be developed to reduce the number of patient journeys that are affected by them. Exploring the reasons behind care discontinuities could help healthcare managers to identify root causes of sub-optimally performing healthcare systems and thus focus improvement efforts. However, currently there is a dearth of knowledge specifically around the causes of discontinuity in chronic care.
This study addresses this gap and builds on the knowledge of the stream of literature on chronic care management. Improved continuity of care can lead to a plethora of positive outcomes such as improved health outcomes and patient experience, and reductions in the cost of care, leading to an overall more efficient and enjoyable care process. To facilitate this development, the reasons behind care discontinuities must be understood. As such, this study’s contribution is a novel framework for analysing the causes of discontinuities in chronic care, the ‘discontinuity of chronic care’ (DoCC) -framework, which enables the systematic analysis and categorization of the causes behind discontinuity of care in chronic patient journeys. Identifying the causes of discontinuity allows for targeted and systematic use of interventions to improve chronic care management.
Background
As is the case with many concepts derived from vernacular, the concept of ‘discontinuity of care’ does not have a universally agreed-upon definition. The term has evolved and expanded over time, and it’s meaning largely depends on the context of use and the interpretation of the researcher. Some refer to discontinuity to the non-realization of a care plan 14 or unrealised follow-ups such as labs, screenings, and referrals, 15 while some consider it a disruption of the physician-patient care relationship12,16 or unrealised relational, informational or management continuity,17,18 while others would define it through voluntary disenrollment. 19 Many of these definitions overlap with what many would consider fragmentation or a dispersion of care between providers.20,21,22 This study builds on the definition by Petersen et al. 14 where discontinuity of care is defined as the non-realisation of intended care, namely a care plan. In other words, what actually happens to the patient (patient journey) is not equal to the intended care (care plan). The term often used in this paper ‘discontinuity of chronic care’ refers to discontinuity of care with patients suffering from a chronic disease.
Care term definitions.

Management models designed for better care delivery for chronic patients have been proposed in literature. One of the prevalent models is the Chronic Care Model (CCM), which is a high-level framework that highlights six interrelated elements of chronic disease management 9 —decision support, health care organization, clinical information systems, self-management support, delivery system redesign, and community resources— which together lead to a systemic change where well-informed and engaged patients interact with prepared and proactive practice teams. Barr et al. (2003) critiqued the CCM for neglecting health promotion and disease prevention and suggested an expansion to tackle this by adding two elements to the model - creating supportive environments and strengthening community action. 5 Despite the advancements of the CCM in enhancing care delivery, it still predominantly addresses methods for improving care without thoroughly examining the underlying issues that necessitate these improvements. Thus, it completely skips identifying the root causes of discontinuities in chronic care, which is crucial for devising effective solutions and interventions. Identifying the causes of discontinuities is particularly vital as a heuristic method, given the constrained resources of healthcare organizations. In practice, it is often impossible to integrate all elements of the CCM to care delivery, and certain factors may even fall beyond the control of healthcare providers.
The antithesis of discontinuity of care, the continuity of care has been given ample attention in literature, with Haggerty et al. 18 underlining three key categories of continuity: informational, management, and relational. First, informational continuity involves seamless information flow among providers and care touchpoints. Second, management continuity addresses the dynamic patient needs, ensuring sensitive and responsive care. Third, relational continuity emphasizes stable, continuous patient-caregiver relationships. Not all three factors of continuity of care need to be fully realized for patients to perceive high-quality, seamless care. For example, a patient may still experience satisfactory care even if their caregiver changes (indicating a discontinuity in the relational aspect) if care management and informational continuity are well organized. Thus, the continuity of care model does not give practical indications for care providers on where to focus on their care processes. The model lacks practical guidance for enhancing care continuity.
Both models used as an example offer high-level guidance for improving care continuity but fall short in providing practical instructions for healthcare organizations. There is a pressing need for more actionable insights that delve into the deeper aspects of improving care continuity. Understanding the root causes of care discontinuities can provide the necessary practical guidance.
Methods
The study adopted a case study approach using a combination of qualitative (focus group, interviews) and quantitative (survey) methods, with the qualitative data taking the primary role. The healthcare professional (HCP) participants were generalists while the patient survey focused on patients with gastrointestinal disorders. The research process is presented below in Figure 1. Research process.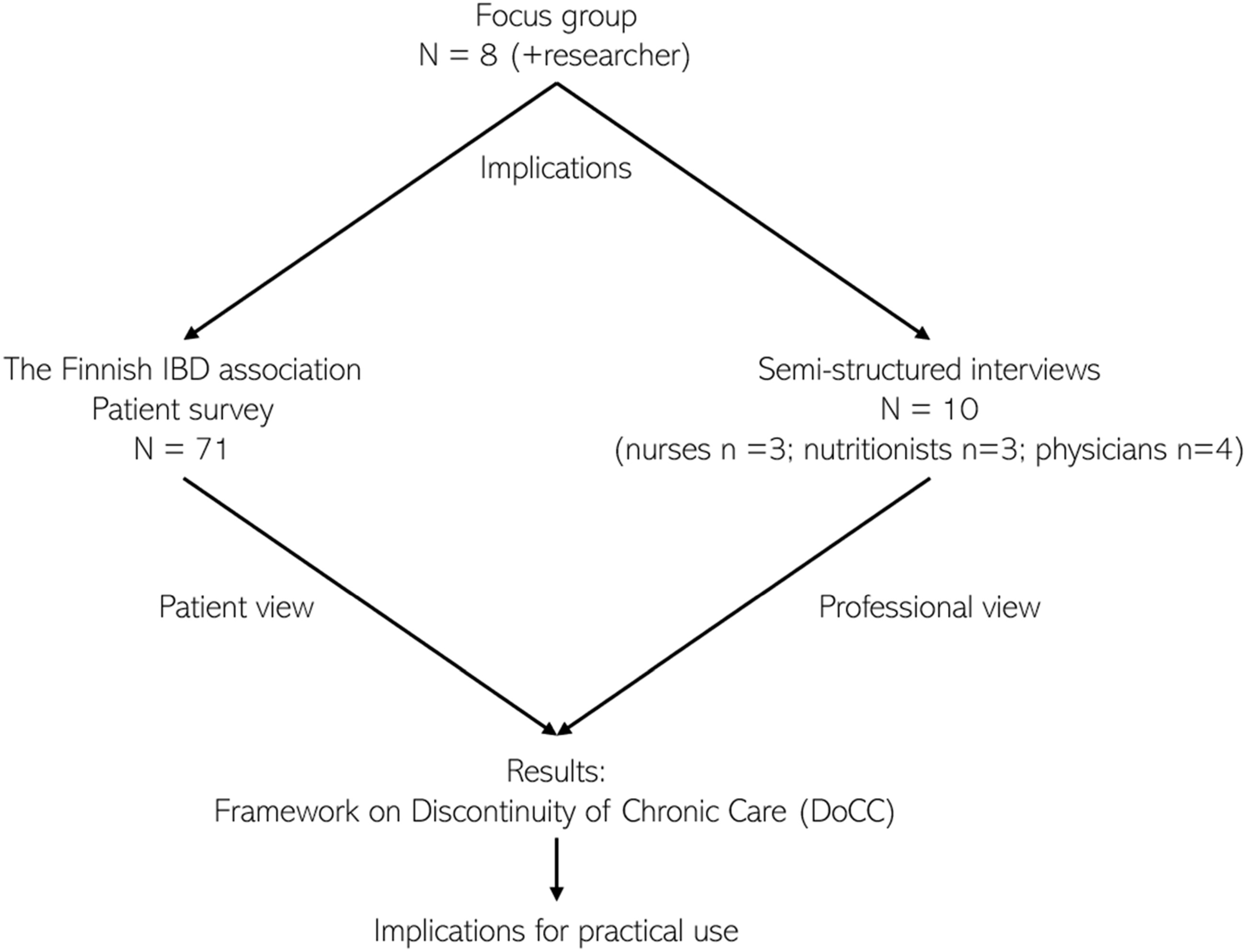
Data collection
The data collection started with a focus group with Finnish HCPs providing a general understanding of the discontinuity phenomenon. Based on these results, a survey was conducted for chronic gastrointestinal patients. Finally, individual interviews with Finnish HCPs were conducted. The data collection was conducted by one of the researchers, who, at the time, had no previous contact with the participants or the partner organisations. The participants for the focus group and interviews were purposely selected and further contacted by the data collector through email. After first contact, new contacts (n = 3) were established through a snowball effect.
Focus Group: the focus group discussion took place on 04.02.2021 via Microsoft Teams and consisted of physicians and nurses working in private healthcare with a managerial position in the fields of patient service, internal operations, development, and specialised healthcare (N = 7, 6 = Female, 1 = Male). These individuals have a clear and broad overview of the organisation and the possibilities and limitations inherent to it. The duration was 2 hours. Three themes (“care adherence”, “prevention of discontinuity”, “enhancing care plan use”) were chosen from literature to guide discussion in the two-hour focus group and the data collector acted as the facilitator. The guiding questions can be found in Appendix 1. The seven participants were divided into three interdisciplinary groups based on their knowledge on the chosen themes. As the facilitator could not attend all three discussions at the same time, all the discussions were recorded, and an online note-taking tool was used to help identify the key ideas from the discussions.
Survey
A survey was conducted (N = 71), and respondents were recruited with the help of the Finnish IBD (Inflammatory Bowel Disease) association called “IBD ja muut suolistosairaudet ry”. A link to the patient survey was shared on a social media platform where the Finnish IBD association reaches 7697 followers (15.4.2021). The survey was open for 1 month. The median respondent was a female aged between 36 and 45. 89% of respondents were working age and had lived with their condition for at least 2 years. The survey can be found in Appendix 2.
Interviews
Semi-structured interviews were conducted and recorded via Microsoft Teams, with HCPs (nurses n = 3, physician n = 4 and nutritionists n = 3), more detailed descriptions are provided in Appendix 4. The interview questions were not sent beforehand to the interviewees. The questions were refined between authors; however, they were not piloted beforehand. The questions can be found in Appendix 3. Interviews were conducted until data saturation. Transcripts were not returned to the participants for commenting. The interviews were conducted in Finnish and the length varied from an hour to an hour and a half and each participant was interviewed once. The data collector took field notes during the interviews.
Data analysis
ATLAS.ti was used to manage the data and conduct coding of the focus group and interview recordings. The first order codes were grouped into inductively derived themes which were then connected using interrelatedness mentioned by the interviewees.
Participants were offered a voluntary presentation on the findings. A framework for care discontinuity is built using grounded theory as a dialogue between observations and conceptualizations. 23
Results
Focus group
The focus group discussions imply that patients should have responsibility for their own care as they have a prominent role in achieving care balance. However, this should not lead to negligence of the patient nor the management of their care plan. The responsibility of the patient should be to report about their care to the care manager as agreed. Also, the rules for when the patient should contact care personnel should be constructed. Patients’ self-management should be supported by guidelines describing when and how patients could adjust their own care.
Patient motivation and adherence was discussed in the second group. It is not enough to provide information to the patient to gain lasting change. Effective lifestyle interventions are often the treatment, and this requires a motivated patient adhering to their care. In addition to facing the patient as an individual, the patient’s own perception towards their condition and situation plays a significant role. Patient self-monitoring and reporting was highlighted again, and autonomous symptom mapping was suggested to relieve healthcare resources.
The third group focused on care plans and the use of care plan management tools. They asserted that care plan management should begin in the doctor’s office, as a care plan must exist before it can be managed. The need for implementing care planning to physicians’ work methods was highlighted. Also, a knowledge gap in using care plan tools was mentioned. Often nurses end up acting as a technical support for physicians leading to suboptimal care resource allocation.
Survey
When prompted about the nature of care the respondents would like to receive, one answer rose above all: a constant contact person who could be contacted when symptoms change, or the care plan is unclear to the patient. The next most popular answers were (1) receiving information about lifestyle changes which support treatment for their illness and (2) support regarding these required lifestyle changes. Support from other sources like from family members or peers did not get significant endorsement.
Ownership of their own treatment was clear among the respondents, as 86% answered that responsibility of care should either be equally distributed between the patient and caregiver, or the responsibility should be more with the patient. The remaining 14% answered that the responsibility should lie more on the caregiver. This suggests that not adhering to a care plan does not necessarily stem from patients’ motivational or adherence issues. Ergo, the challenges are more likely to reside in the care management processes.
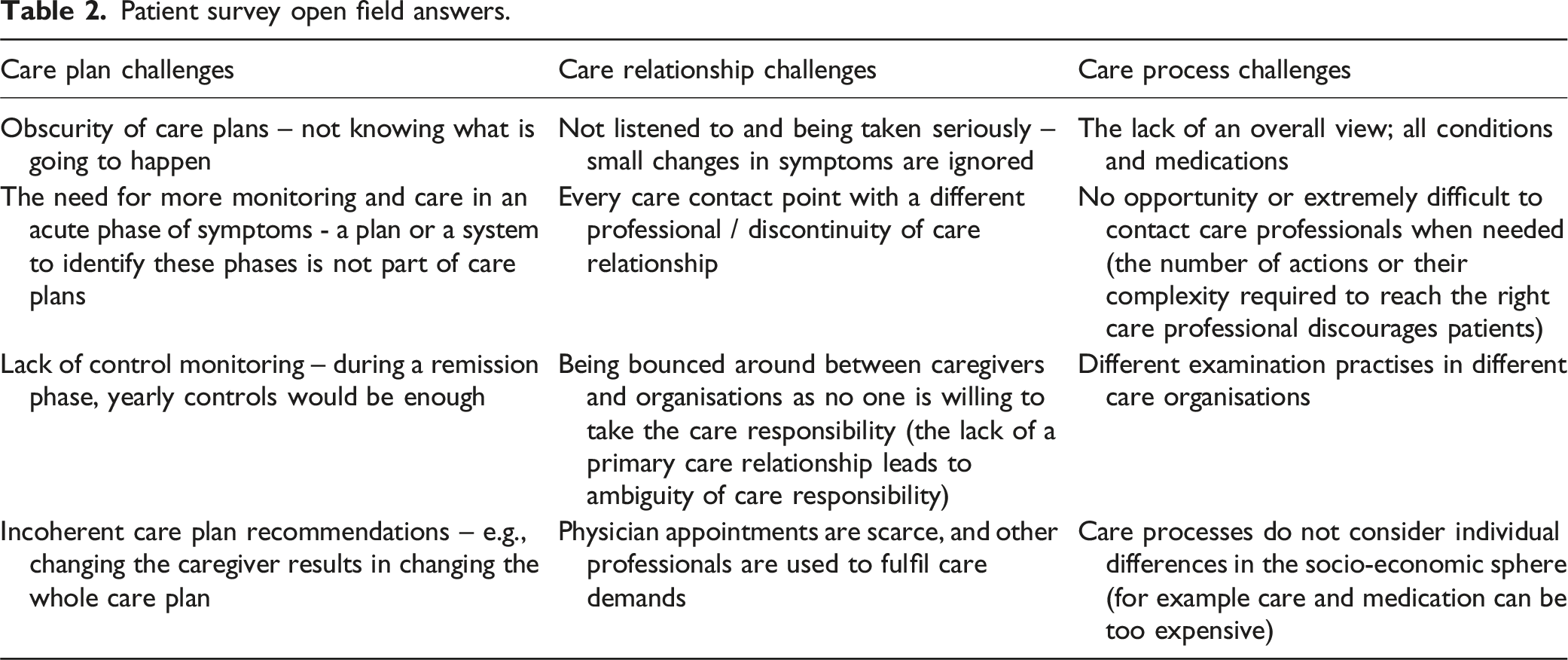
Patient survey open field answers.
Interviews
Examples of evidence synthesis into key takeaways from the interviews.

Patients’ care responsibility
A lack of faith in patients’ ability to take initiative is visible in the interviewees’ comments. This is a discrepancy as the survey indicated patients being willing to take responsibility, yet this does not show to the caregivers. Thus, there must be obstacles hindering patients in taking responsibility. Table 2 “Patient survey open field answers” clarifies possible challenges faced by patients.
Humane factors
In addition to not knowing when to be active, patients might simply just forget, which might explain some care discontinuities. Sometimes the reason can be fear; if a procedure is scary or uncomfortable for the patient, the patient might decide not to go on with the care plan. The interviewed nutritionists face the reality that patients can be afraid to come to their appointments due to false assumptions, such as being judged.
Fluctuating care needs
Nutritionists and physicians alike identified a common misconception among some patients; “if I’m not hurting, I don’t need care”. Patients are motivated to come to appointments when they have symptoms but when symptoms relieve, they are prone to voluntarily drop out of care. In other cases, the relieving of symptoms can act as motivation to continue care.
Motivation
Motivation naturally fluctuates in time but there are some things caregivers can do to help to build and upkeep motivation and care adherence. Nutritionists had identified that the focus on motivating the patient is emphasised in the beginning of care and upkeeping the motivation gets more often neglected. The interviewed nutritionists also identified well how too high, unrealistic, or ambiguous goals can demotivate patients as the feeling of failure sinks in when these goals are not met. Overall, the lack of change is demotivating whereas positive results often induce motivation. Sometimes lack of results can evoke shame in the patient and self-criticisms leading to a higher risk of dropping out of care. Other motivational causes include dissatisfaction with care results, and disbelief of any care helping them.
Appointment times
Interviewees emphasised the importance of the first appointment – the connection and communication with the patient is established and a positive atmosphere supports care adherence. On the other hand, the importance of concreteness was emphasised. For example, lifestyle changes should be integrated concretely into the patient’s life. This is also where the importance of other caregivers in addition to physicians arises, as often shorter physician appointments are not enough to dive into the concrete levels of care.
Process related challenges
Based on the interviews, virtual care plans are underproduced and paper instructions are still common for care planning even though these cannot be promptly updated, and they can be easily lost. The use of digital tools which enables the creation of virtual care plans is not systematically taught to new employees or other willing participants.
The level of detail in care plans varies, resulting in “invisible work”. For example, a patient may call to ask about their care plan, but answers provided by the nurses are limited to the information written by the physician in the health record system and may require extra investigative work to provide the patient sufficient answers. Another challenge is that patient monitoring responsibility is ambiguous and there is no unequivocal role definition as to who the primary caregiver is and thus responsible for the care plan. A caregiver cannot generally access a patient’s health history in other health records outside their organisation either because it’s technologically impossible or required consents are missing, which complicates monitoring the care plan.
Caregiver related challenges
Caregivers are not supported in taking responsibility for their patient’s care plan actualisation - there is a lack of supportive tools and incentives. Due to the caregivers having different ways of working, issues with information flow and automation arise. In addition, there are no resources allocated to a continuous physician-patient relationship, and appointment times are often perceived as too short.
Framework for discontinuity of chronic care (DoCC)
The results are combined to provide a uniform understanding of chronic care discontinuity. As data collected through different methods were coded, conjunctive themes for the root causes behind discontinuity emerged, and were named as challenges regarding a broader care related theme. Two main sources for the different challenges were identified: healthcare system and patient.
Thus, the reasons behind discontinuity of chronic care are divided into two main categories: (1) reasons related to the healthcare system, and (2) reasons related to the patient. Healthcare system related reasons can be divided into three sub-categories: (a) caregiver challenges, (b) technological challenges, and (c) process challenges. (a) Challenges related to caregivers’ work found in this study were related to short appointment times and increasing responsibilities leading to dissatisfaction in caregiver-patient-relationship. Especially in stuffed physician appointments focusing on the patient is challenging. (b) Technological challenges include user challenges with technology (e.g., elderly, deteriorated eyesight, lack of equipment); siloed health technology development between care organisations leading to information flow obstacles; digitalisation as an ongoing process leads to constant changes which can result in incomplete development, implementation, and caregiver education; and finally there are legislation restrictions protecting health records which hinder rapid health technology development and implementation as digital tools in healthcare are often considered medical devices that are highly regulated.
Caregiver and technological challenges are associated with incentivised disenrollment from care, which means that external factors play a big role in the patient’s decision to discontinue care. (c) The challenges related to the organisational processes include care responsibility obscurity between caregivers and across organisations; staggering care plan implementation; disjointed care and health monitoring; incoherent ways of working leading to care quality inconsistencies, and information flow challenges between caregivers; and lack of continuous care access for the patient. Chronic care discontinuity related to process challenges can be associated to a type of involuntary disenrollment. In these cases, the patient does not want to discontinue care but for some reason the system and its processes push the patient out of care.
Key findings of healthcare system related reasons for chronic care discontinuity can be summarised in three points; (1) caregiver challenges during appointments take focus away from the patient who might feel not being cared for in a way they expect; (2) instead of supporting care, technological solutions can feel cumbersome for the patient and incentivise care discontinuity; and (3) established healthcare processes do not support care continuity for all patients namely chronic patients who require lifelong health monitoring and continuous care access.
The patient-related reasons can be divided into two sub-categories: (a) situational challenges and (b) internal psychological challenges. (a) Situational challenges relate to the realities of being a human, for example, moving abroad, changing jobs, or family issues. As these situational challenges cannot be avoided, they can only be accepted as care anomalies which healthcare systems have no power over. (b) Internal psychological challenges, on the other hand, can be affected by healthcare systems and caregivers. For example, the right information can correct misbeliefs which could have previously led to unnecessary fears of procedures, doctors, hospitals etc. In our data, common misconceptions found are related to care need evaluation by the patients themselves, and uncertainties related to care plans and contact needs (e.g., when to contact care personnel). Overall, chronic discontinuity related to these kinds of personal reasons is initiated by the patient. In these situations, the patient willingly discontinues care making it a voluntary disenrollment.
This synthesis is summarised in the framework for discontinuity of chronic care (DoCC) in Figure 2. Framework for discontinuity of chronic care.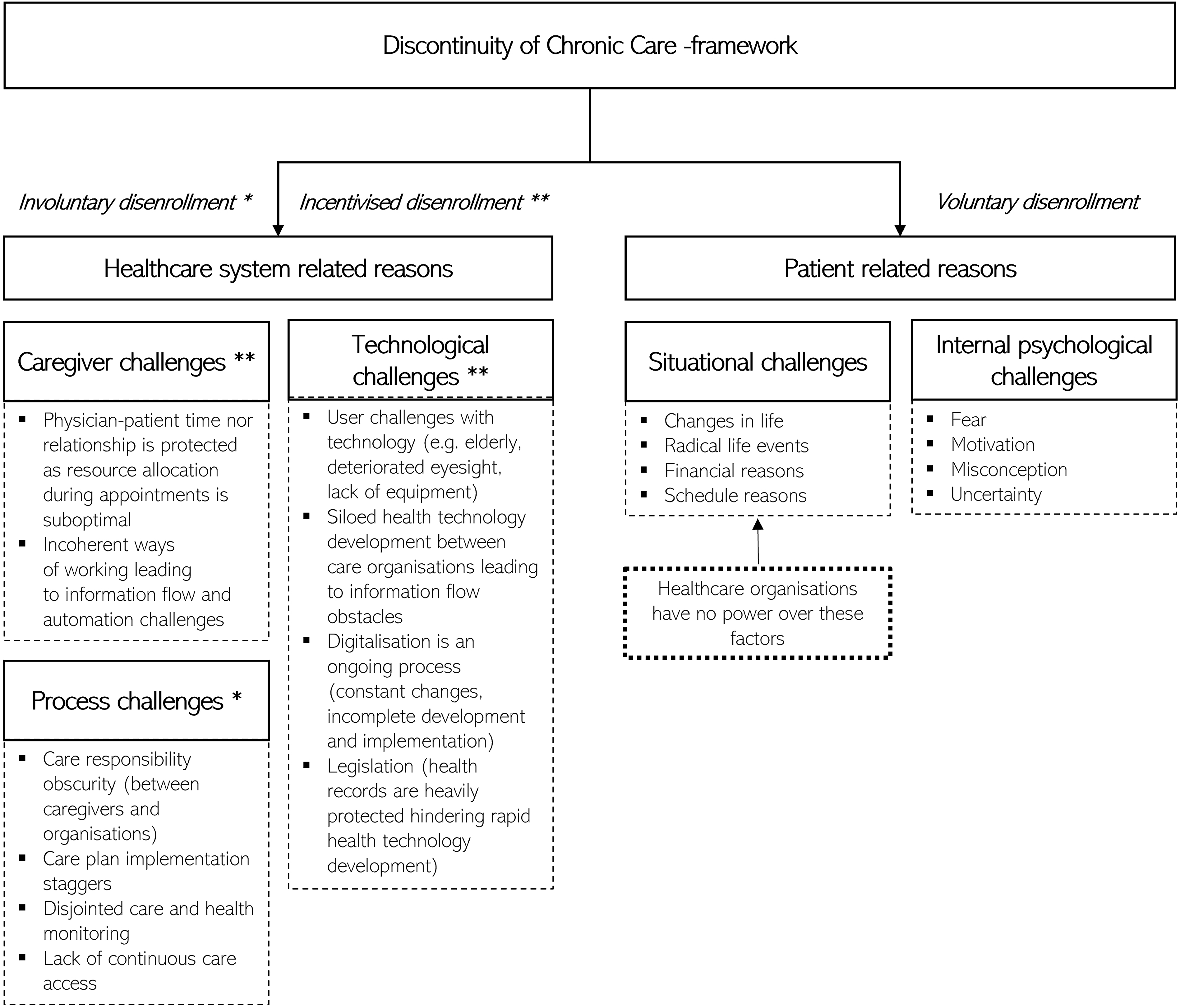
Discussion
This study has identified five main categories linked to discontinuities in chronic care, each having characteristics related to either the healthcare system or the patient. Patient-related reasons include personal circumstances (i.e., scheduling conflicts or financial constraints), and internal psychological challenges (i.e., fear of treatment or misconceptions about the necessity of care). The system-related reasons involve technological challenges (i.e., incompatible information systems or lack of necessary technologies), care professional-related challenges (i.e., insufficient appointment times or burdensome information systems), and process challenges (i.e., a lack of standardised care plans and unclear roles of key care professionals).
This study has several limitations. First, the results are based on a single case study, possibly limiting their generalizability. This also includes the fact that the specific characteristics of the partner organization (i.e., private provider) may have influenced the results and validation of the results in other healthcare organization is needed to further verify them. Notably, public and private healthcare systems may have different motivations for mitigating care discontinuity. Similarly, the study did not consider all chronic diseases as the patient perspective focused on gastrointestinal patients. This study also didn’t consider the differences in prevalence of the different causes of care discontinuities within different patient segments (i.e. socioeconomic groups), which could greatly differ.
Challenges with relational continuity are well researcher and known to be prevalent. 24 The challenges could be tackled by, for example, assigning patients to physicians, developing booking processes and facilitating follow-ups. 25 Similarly, the shortcomings of processes and technologies are well studied and include challenges like process flexibility, system integrations, compliance and security, user acceptance, and data quality. 26 Situational challenges faced by patients have also been identified in previous research as patient’s fear 27 and equity challenges related to financial barriers 28 have been known to affect service use. The individual findings that are combined here into the DoCC-framework are well documented in previous literature and the DoCC-framework adds to this body of literature by further validating these findings and bringing them together to give healthcare managers a holistic picture of continuity challenges. What is more surprising is that despite Finnish law mandating that “if necessary, a plan for research, treatment, medical rehabilitation or other similar measures must be drawn up” (Laki potilaan asemasta ja oikeuksista 857/2004, 4a §), the results indicate that care plans remain a problematic topic, with the primary issue being seemingly a lack of standardization. It is often unclear who should be responsible for formulating and overseeing the care plan, especially in multi-provider care, and different professionals and organisations adopt different forms and content for care plans, resulting in confusion and difficulty in real-time care monitoring. This lack of clarity can even leave some chronic patients without any plan. A standardized care plan (often based on a care pathway) is essential as it allows for general treatment monitoring and provides a benchmark for comparing actualized treatment.29,30 If a patient’s journey deviates from the care plan due to discontinuity, corrective actions can be taken by identifying the discrepancies. 26
This study builds on existing literature that underlines the complexity and individuality of chronic care management. Previous frameworks, such as Chronic Care Model 9 and its expansions (e.g., Barr et al. 5 ), examine chronic care processes from a broader perspective. The theoretical contribution of the study lies in the DoCC-framework which expands the discussion of continuity to deeper descriptive levels. These results add to this body of literature by focusing specifically on care discontinuity in the chronically ill and its underlying causes through the DoCC-framework. The DoCC-framework gives healthcare organizations tools to categorise the causes of chronic care discontinuity and enhance patient management with targeted interventions. To this end, the framework is complementary to the three-level categorisation postulated by Haggerty et al. 18 and specifically aimed at chronic care processes. The framework can also guide the allocation of resources by identifying causes of discontinuity that warrant immediate attention. For policymakers, the framework may work as a tool to help identify potential avenues for both further exploration and to aid in resource allocation in an organizational level. Furthermore, the DoCC-framework may work as a ‘boundary object’ between policy makers and health managers to help them communicate with common terminology.
Discontinuities in chronic care can lead to unnecessary use of healthcare resources and lacking health outcomes. Identifying the root causes of these discontinuities is critical for developing effective preventive measures, and this is where DoCC-framework can play a pivotal role in facilitating the discovery process. Furthermore, our findings highlight the importance of standardization among healthcare organizations in the creation of care plans.
Supplemental Material
Supplemental Material - Causes of care discontinuity in chronic outpatient care: A mixed method case study
Supplemental Material for Causes of care discontinuity in chronic outpatient care: A mixed method case study by Anu Vehkamäki, Märt Vesinurm, Riina-Riitta Helminen, Olli Halminen and Paul Lillrank in Health Services Management Research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.