
Abstract
The significance of investigating innovation in academic medical centers has been underscored, as they are recognized as leaders in frontline innovation and accelerators of healthcare advancement. The factors that contribute to innovation success, particularly those associated with benefits, can be identified by examining innovation attributes in relation to innovation process stages. This study aimed to understanding the innovation process by identifying the key factors that characterize innovation and their outcomes in academic medical centers. The central research questions were: what are the main attributes of innovation in an academic medical center? and which innovation attributes influence the outcomes of innovation in an academic medical center? Clinical directors from one academic medical center in Italy, Careggi University Hospital, responded to a questionnaire. Exploratory factor and regression analyses were performed to analyze the data. The findings highlighted the crucial role of middle managers in promoting and developing significant high-quality innovations. Our study deepens the innovation attribute framework and enables a better understanding of the relationship between attributes and benefits in the healthcare context. From a practical perspective, our study equips academic medical center administrators with a tool to evaluate innovation attributes and their relationship with outcomes, enabling better leverage of the potential benefits.
Introduction
Universities and research hospitals are vital components of health innovation systems because of their roles in adopting, reproducing, and generating medical knowledge. 1
The significance of innovation, even in regulated environments such as healthcare, is recognized also for the crucial role that hospital management’s knowledge of innovation processes plays in improving the quality of care. 2 Wu and Hsieh 3 have identified a taxonomy of hospital innovation and its significant impact on perceived quality of care.
The importance of investigating innovation, especially in academic medical centers (AMCs), has recently been highlighted. AMCs are considered leaders in frontline innovation 4 and accelerators of healthcare innovation. 5 However, research on the innovation process in AMCs is scarce despite its recognized potential for advancing theories related to care improvement. 4
Particularly, studies need to focus on innovation activities within hospitals that collect survey data at both hospital and unit levels. 1 However, most of the existing literature focuses on the relationship between the various attributes of innovation in healthcare and their diffusion, 6 with many findings lacking universal applicability. 7
Research specifically dedicated to the benefits associated with different innovation attributes remains limited and conceptually inconsistent. While Adams 8 consider benefits to be part of the innovation attributes themselves, recent contributions offer a contrasting perspective. For instance, Syeed 9 has argued that benefits should not be regarded as attributes of innovation, but rather as outcome associated with various attributes. Our study aligns with this latter perspective, treating benefits not as inherent attributes of innovation, but as measurable outcomes resulting from the presence or influence of specific attributes.
Specially, this study examines the attributes or factors that contribute to the success of an innovation, particularly those associated with innovation performance and output—the benefits of innovation— by examining them in relation to innovation stages. Unfortunately, the literature on the nature of innovativeness in healthcare organizations and its relationship with outcome is scarce. 10
This study aimed to address this gap in the understanding of the innovation process in hospitals by identifying the key factors that characterize innovation and its outcomes in AMCs. The study sample comprised clinical directors from one of the most important AMCs in Italy (Careggi University Hospital). From a practical perspective, our study aimed to provide AMC administrators with a tool for evaluating innovation attributes and their relationships with outcomes. This tool is intended to help administrators leverage the potential benefits of innovation.
The remainder of this paper is organized as follows: the second section presents the theoretical background of innovation attributes; the third section is dedicated to methodology; the fourth section presents the results; and the final section presents the discussion and concludes the study.
Theoretical background
Innovation attributes
In the innovation literature, studies examining innovation attributes play a pivotal role. Attributes are defined as the “perceived characteristics, descriptive properties, qualities, or features belonging to an entity” (Adams et al., 11 p.43). Many studies identify innovation attributes based on Rogers’ 6 framework, which outlines the perceived characteristics of innovation that influence adoption decisions. Numerous studies have confirmed the applicability and effectiveness of Rogers’ model in healthcare contexts. For instance, Cranley et al. (p.13) described Rogers’ attributes as “a comprehensive model to describe characteristics of an innovation”. 14 Greenhalgh et al. 12 emphasized the predictive value of innovation attributes in determining the success of innovation implementation. More recently, Huybrechts et al. 13 interpreted their findings through Rogers’ framework, identifying actions that support and facilitate innovation uptake. Légaré et al. 15 addressed Rogers’ innovation attributes as both facilitators and barriers in the decision-making process in clinical practice. Similarly, Urquhart et al. 16 confirmed that attributes influence the implementation and use of complex innovations in cancer care. He et al. 17 further demonstrated that innovation attributes significantly enhance adoption intention within healthcare setting.
Adams, 8 using Rogers framework, developed and validated a tool, the “Perception of Innovation Questionnaire,” based on a survey conducted within the National Health Service (NHS), to measure the attributes of innovation in healthcare. However, other studies have not assessed the applicability of this tool in different contexts. This has been the object of further in-depth and qualitative analyses aimed at defining the taxonomy of innovation. 7
Given the complexity of innovation attributes in healthcare and the heterogeneity of literature findings, this study focused on the innovation attributes in AMCs and aimed to provide an exploratory instrument to measure this phenomenon, based on the scales validated by Adams. 8
Therefore, the following research question was proposed to deepen the understanding of innovation attributes in AMCs:
The relationship between attributes and results
Rogers’ 6 framework was applied to healthcare by Adams et al., 7 who identified a taxonomy of innovation in healthcare. They found that analyzing the entire innovation process is essential to better understand innovation attributes and their impact on adoption. Adams describes this process as a “multi-stage temporal process” which encompasses “a series of events that occur in a more or less dynamically variable sequence within organisational and social settings that affect the behaviour of occupants in some ways” (Adams et al., 11 p. 46). The significance of adopting a process-oriented perspective has been emphasized in a recent study stating that “a deep understanding of innovation framing is not possible without considering the stages of the innovation process” (Reynolds, 18 p. 18). This perspective allows a better understanding of the relationships within and across innovation contexts. According to this perspective, innovation progresses through three stages: creation, adoption and implementation, and success measurement and achievement of desired outcomes. 19
By shifting the focus from an examination of attributes to innovation process stages, we can identify which attributes contribute to innovation success. Research has demonstrated that innovation attributes significantly impact innovation performance and outcomes. 20
In healthcare, the impact of hospital innovation on perceived quality of care has been demonstrated. 3 However, the effects of different innovation attributes on benefits have not been thoroughly analyzed. The following section examines the key relationships identified in innovation literature, which we aimed to verify in healthcare, particularly, AMCs. Attributes linked to benefits were selected based on prior studies that highlight the importance of the polythetic classification of attributes, reaffirming the multivariate nature of innovation. 7
The literature identifies various innovation outcomes in healthcare. In this study, we synthesized them into three areas: (1) actual operation and efficacy, referring to the extent to which innovation meets its intended objectives; (2) organizational and professional profile; and (3) recognition, within or outside the NHS (observability). The selection was based on the classification found in the literature and refers to the scale known as Adams’ Innovation Benefits. 7 In light of the specific context and objectives of our study, and in order to simplify the analysis, we chose to include only a subset of the dimensions originally proposed. We considered these dimensions sufficient to effectively investigate the phenomenon under examination.
Determinants of actual operation and efficacy
Studies have identified several determinants related to one of the principal benefits of innovation in healthcare—the ability to achieve planned outcomes in terms of problem-solving. First, when an innovation is tested and experienced, uncertainty regarding its outcome is reduced, leading to a more positive reception of the innovation. 6 In healthcare, the opportunity to try an innovation and becoming familiar with it can mitigate the common reluctance of members within organizations to engage in innovation activities 21 and help achieve desired results. 22 The more the information gathered about innovation in other contexts, the greater is the reduction in the surrounding uncertainty. 23
Second, when an innovation is adapted to fit the organization, the success of its implementation is facilitated. 22 In particular, an organization’s ability to adapt to local requirements and needs is considered condition for effective and efficient. 24
On the contrary, certain attributes can negatively impact actual operations. In a hospital setting, the changes inherent in innovation are not easy to implement, for example as the introduction of innovation requires significant local variations in practice. 25 Routine, defined as “procedures and staff behaviours that occur regularly as part of normal hospital operations, as distinct from extraordinary implementation efforts that often accompany the introduction of a new practice” (Brewster, 26 p. 2) is generally favored in hospitals. Thus, when innovation aligns with existing work practices and routines, it is more likely to be adopted. 12 Conversely, many innovations in hospitals “fail to integrate into organizational routines,” making implementation and achievement of planned results more difficult (Brewster, 26 p. 2). Therefore, when an innovation deviates from pre-existing routines, the likelihood of its success diminishes.
Furthermore, in healthcare the relationship between risk and actual operations has been demonstrated; it is linked to innovation stages. During early stages, the uncertainty and risks make it impossible to predict efficacy in terms of patient benefits. 23
Determinants of profile
AMCs compete globally with other institutions, as recognized by the significant impact of biomedical research as a driver of economy. 27 The status of an AMC is crucial for new research and healthcare innovation funding and for attracting and retaining high-quality staff. 28 This can be considered an important benefit of innovation in AMC. From the perspective of professionals, innovation is critical at the personal level. As Rogers 6 (p.215) notes, “one of the important motivations for almost any individual to adopt an innovation is desire to gain social status.” Other studies have found that individuals pursue innovation to enhance their social status or elevate their professional prestige. 29 Moreover, a change that aligns with established professional values can strengthen organizational identification 30 and, in turn, influence the organization’s image. 31
Organizational prestige is also associated with a broader scope of research and development projects in clinical trials. 32
Innovation can be fueled by risk-taking, although it may have negative consequences. Risk-taking can be driven by either organizational goals or personal prestige. 33 Thus, risk-taking is another widely recognized determinant of status. Status-driven risk-taking is motivated solely by the desire for increased wealth, power, and prestige, with the primary goal being the attainment with these rewards. However, this relationship has not been demonstrated in healthcare.
Determinants of observability
“Observability is the degree to which the results of an innovation are visible to others” (Rogers, 2003, p. 232). 6 To achieve a high degree of innovation diffusion, the benefit of the innovation should be evident and adaptable to specific needs. 25
Literature identifies several determinants of observability in healthcare. First, in healthcare organizations, particularly hospitals, the changes inherent to innovation face various barriers 25 (Hayes, 2013): nature of work, workforce characteristics, and leader-workforce relations 21 (Nembhard et al., 2009). To enhance and promote the innovation process, the importance of networking, both within and outside the organization, has been emphasized as it increases access to resources and knowledge. 34 In hospitals, interorganizational social capital facilitates knowledge sharing, thereby reducing barriers to organizational learning. 35 Moreover, the external prestige derived from innovation drives a greater scope for innovation projects 32 Thus, observability increases when the impact of innovation extends to a wide network within and outside the organization.
Second, literature highlights the influence of risk on visibility. Healthcare services are often considered challenging environments for innovation because they involve high levels of risk. 21 However, the importance of risk-taking in innovations in hospitals has been emphasized also in terms of organization’s visibility. 32
Based on the literature review, we formulated the following research question:
Methods
Sample
The Careggi University Hospital was chosen as the study setting because it is an AMC with continuous innovation and adoption. With 1144 beds and 5467 employees (in 2022), it is the largest hospital in Tuscany in terms of employee numbers. Furthermore, AMC is a social setting in which innovation is facilitated by the characteristics of their members (e.g., years of formal education, higher status, attitude toward science, and involvement in knowledge networks), which leads them to frequently adopt new ideas. 36
The questionnaire was administered to all clinical unit directors (n = 118) across eight clinical departments in the hospital. All participants provided written informed consent to conduct the study.
Prior to the administration of the online questionnaire, meetings were held with the clinical departments to which the clinical unit directors belong, in order to present and explain the questionnaire.
The directors, with the help of their staff, were asked to identify one innovation from 2021 to 2023 that they considered the most important and significant and complete the questionnaire with reference to that innovation. Furthermore, the directors classified the innovation according to the taxonomy proposed by Wu et al. (2015) 3 : medical, which is directly related to the diagnosis, treatment, and prevention of disease in the hospital (technology and method), or administrative, which pertains to relationships with employees (internal management) and patients (external management).
The survey was conducted online from August to September 2023 using LimeSurvey.
Measurement instrument translation
Adam’s questionnaire for innovation attributes7,8 was translated and adapted to an Italian AMC. To strengthen the translation process, two pairs of translators (two native English and two native Italian speakers) independently translated and proofread the back-translated version. The research team compared the two back-translated versions, original version, and two Italian versions, to verify any discrepancies. The agreed upon Italian version of the questionnaire was administered.
This version was submitted to a pilot sample (three directors from operating units of another hospital) to verify the clarity of the items. The pre-testing showed good acceptance by respondents.
Adams et al.’s 8 newness, ideation, application, and benefits scale consists of the following subscales: novelty, departure, disruption, risk, ideation, adaptability, uncertainty, scope, complexity, actual operation, relative advantage, profile, and observability. Psychometric indicators were measured on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). Table 1S (Supplemental Digital Content) shows the original categories, subcategories, and number of items in the questionnaire and the complete version of the instrument.
Other variables
In addition to the observed indicators, three variables were investigated in the survey: number of years as director of the complex operating unit, number of employees within the operating unit and time spent in managing the operating unit. The latter was measured on a scale of 0 to 100. The organizational features of AMCs (e.g., the number of employees within each complex operating unit) were obtained from the hospital management. Other organizational and personal variables may have influenced respondents’ perceptions; however, we chose to limit control to a few elements that were considered more objective than others, such as those assessing respondents’ familiarity or level of expertise with managerial topics.
Data analysis
Exploratory factor analysis (EFA) using the principal component extraction method and varimax rotation was used to adapt the measurement instrument to the context of Italian AMCs. Prior to factor extraction, Bartlett’s chi-square test of sphericity (p < 0.05) 37 and Kaiser-Meyer-Olkin (KMO >0.5) measures of sampling adequacy were used to assess the suitability of the data.34,38 Then, item purification was conducted based on the following exclusion criteria: highest factor loading less than 0.5, cross-loadings between more than one component greater than 0.4, communality less than 0.3, and Cronbach’s alpha less than 0.7.39,40 Subsequently, descriptive statistics (mean ± SD) were calculated for each item and each component that emerged from the EFA. To address the issue of the different numbers of items measuring each attribute, the component score was calculated using the mean item score constituting the indicators. Three multivariate linear regression models were used to examine the assumed associations between the factors identified by the EFA and the determinants of innovation benefits identified in the literature: actual operation, profile, and observability. EFA was performed using SPSS v. 28, and linear regression models were constructed using STATA v. 18.
Results
A total of 97 questionnaires were returned (response rate: 82%). Table 2S (Supplemental Digital Content) shows the characteristics of the AMC departments and questionnaire response rates for each department. The AMC comprised 118 operating units and 1185 health workers, with a median of 8 per operating unit. The main type of innovation mentioned by responded was medical (58%), which comprised methods (30%) and technology (28%). The remainder consisted of administrative innovations (42%), divided into external (22%) and internal management (20%). 3
Medical innovations primarily involved diagnostic and treatment procedures, care pathways and clinical processes. For instance, one innovation involved the adoption of neuromodulation techniques and the use of botulinum toxin, another introduced the Eye Movement Desensitization and Reprocessing (EMDR) for the treatment of patients who had experienced abuse and violence, a third focused on standardizing and implementing a comprehensive care pathway for thyroid nodule, from diagnosis to treatment.
Technological innovations encompassed diagnostic, therapeutic and support systems. Diagnostic advancements included imaging technologies such as the installation of a PET/CT system with a semi-automated dose administration mechanism, and the integration of artificial intelligence in 3D and 4D echocardiographic imaging. Therapeutic innovations featured image-guided brain surgery, combining neuro-navigation with multimodal neurophysiological monitoring. Additional innovations involved health IT systems, including the implementation of telemedicine services and the development of electronic medical records and databases.
Internal management innovations focused on planning systems, human resource management and resource allocation. One project involved the co-management of a departmental sub-intensive care unit, reorganizing work schedules and enhancing collaboration across three complex operating units. Another example was the transformation of a hospital ward into a variable-intensity critical care area, allowing bed capacity to be adjusted based on patient severity and available resources. A further innovation concerned the functional reorganization of surgical services, assigning specific competencies and responsibilities to general surgery units.
External management innovations aimed to strengthen patient relationships and ensure continuity of care across healthcare settings. Examples included initiatives to promote breastfeeding among mothers of extremely preterm newborns, and the implementation of transition pathways from pediatric to adult care for patients with immuno-mediated diseases and congenital metabolic disorders, ensuring continuity during adolescence.
Tables 1–4 show the factor analyses of newness, ideation, application, and benefit scales, respectively, after purification of items and factors. Factor loadings are displayed by size, with those >0.5 in bold, and factors are numbered according to the percentage of variance explained, with factor 1 explaining the maximum variance.
Newness scale
Results from the Exploratory Factor Analysis of the Newness scale.
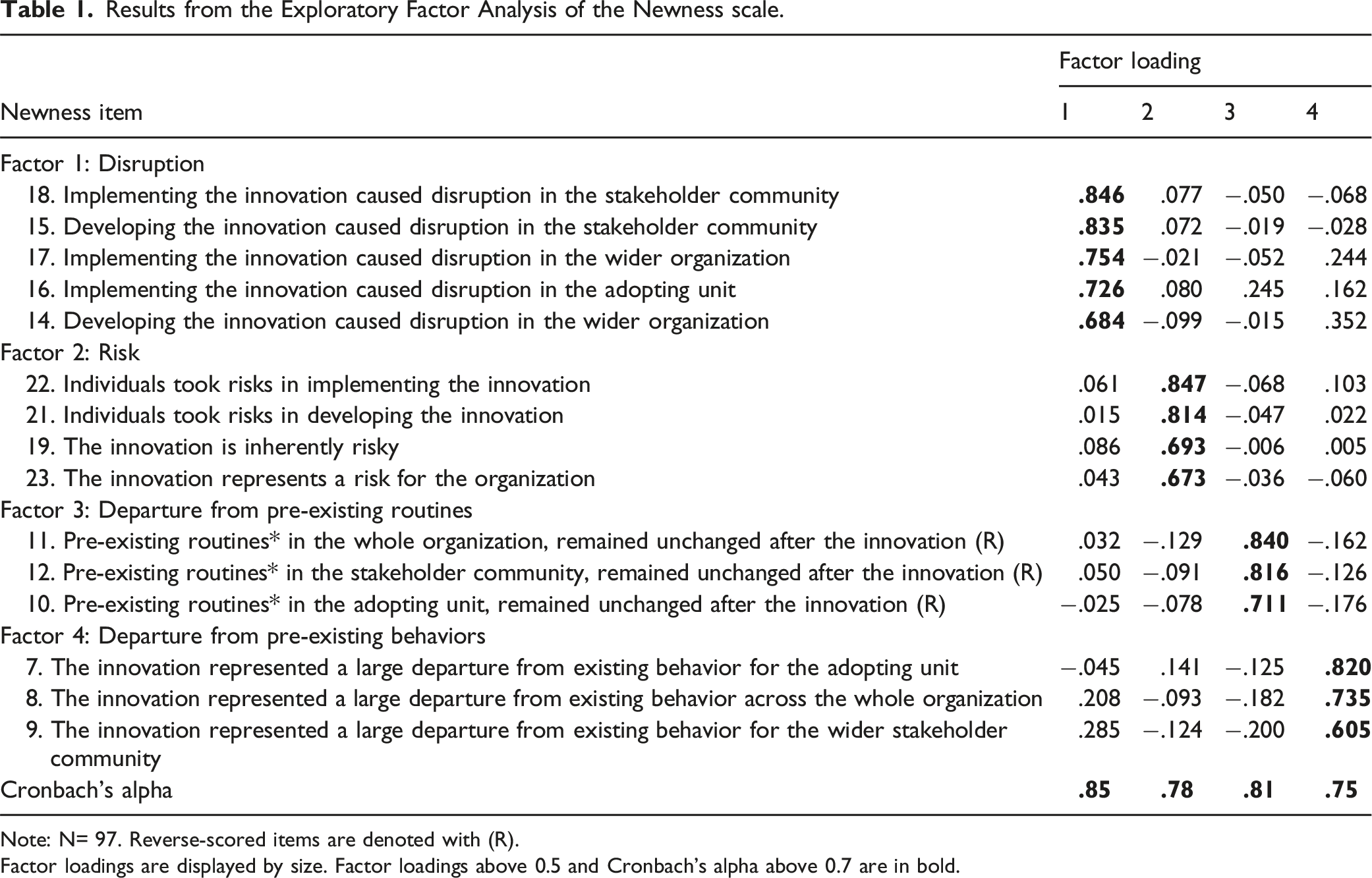
Note: N= 97. Reverse-scored items are denoted with (R).
Factor loadings are displayed by size. Factor loadings above 0.5 and Cronbach's alpha above 0.7 are in bold.
Ideation scale
Results from the Exploratory Factor Analysis of the Ideation scale.
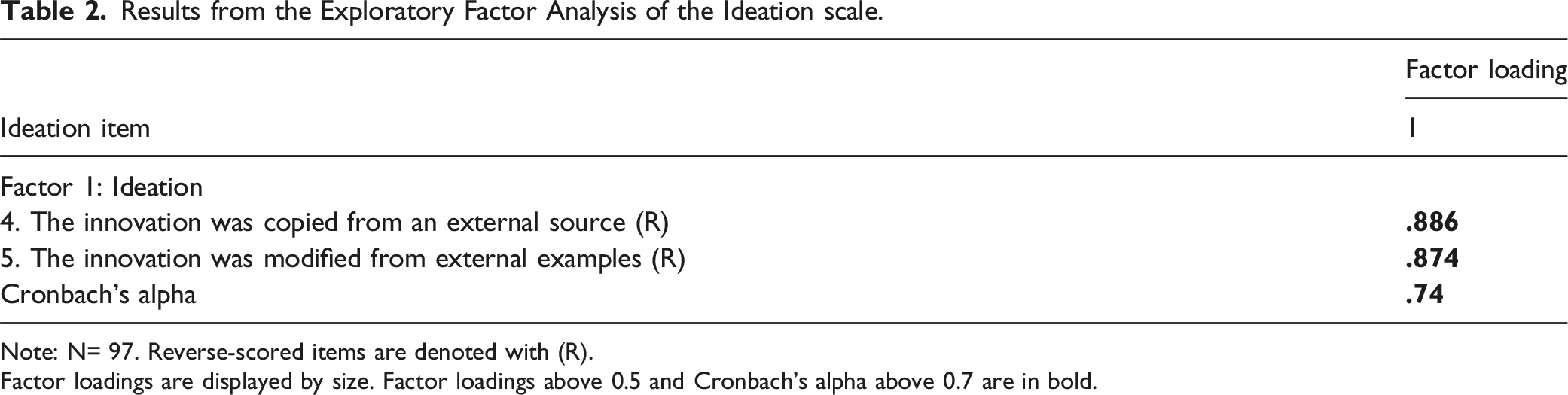
Note: N= 97. Reverse-scored items are denoted with (R).
Factor loadings are displayed by size. Factor loadings above 0.5 and Cronbach's alpha above 0.7 are in bold.
Application scale
Results from the Exploratory Factor Analysis of the Application scale.
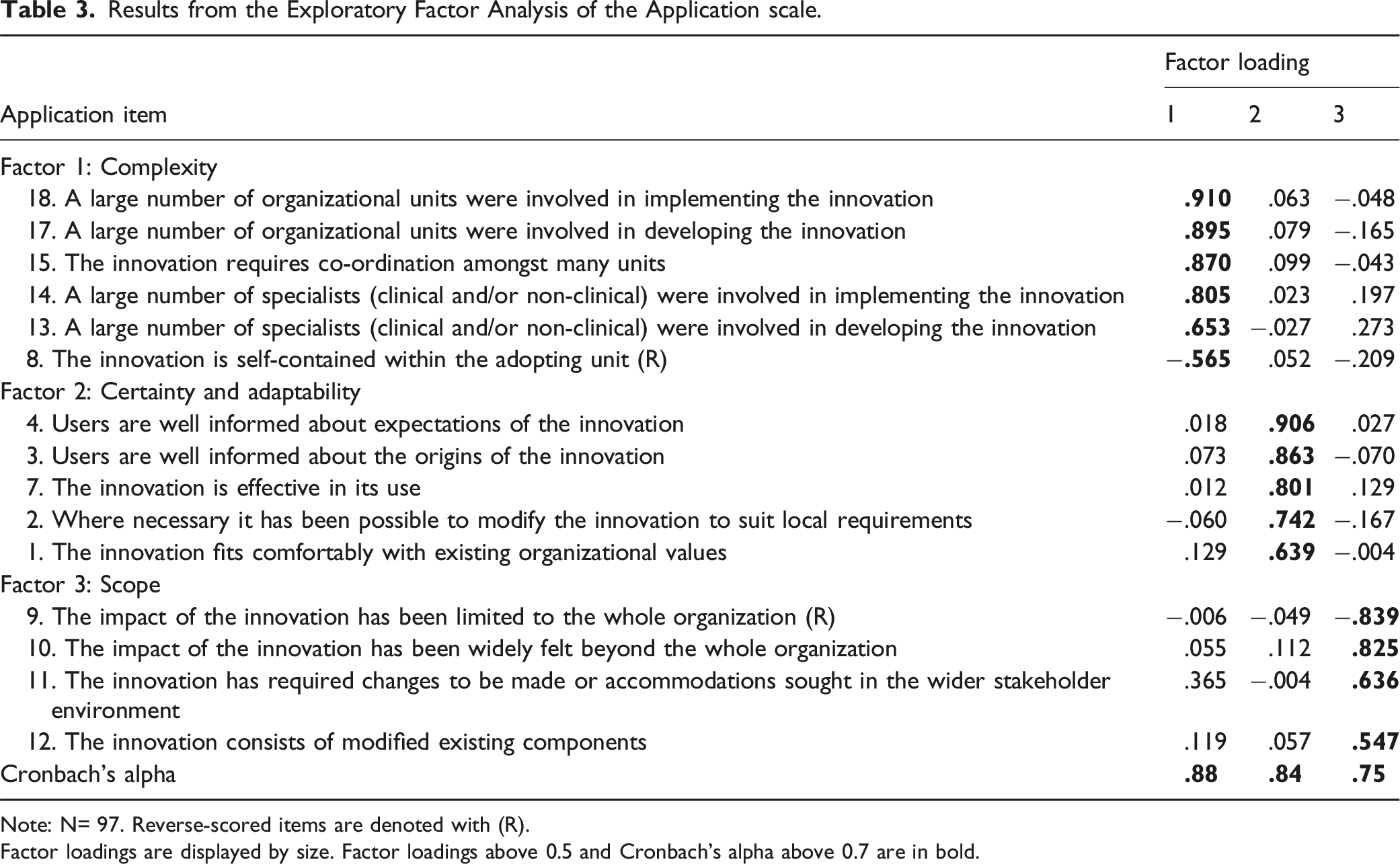
Note: N= 97. Reverse-scored items are denoted with (R).
Factor loadings are displayed by size. Factor loadings above 0.5 and Cronbach's alpha above 0.7 are in bold.
Benefit scale
Results from the Exploratory Factor Analysis of the Benefit scale.
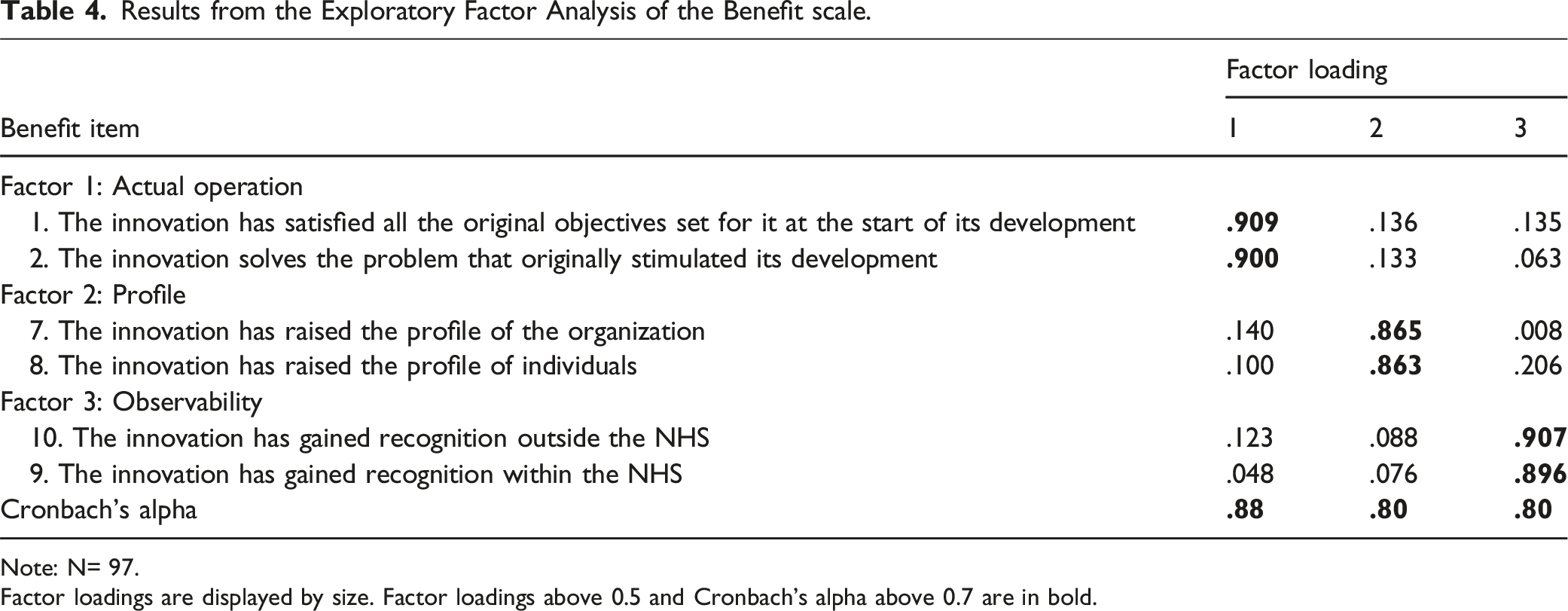
Note: N= 97.
Factor loadings are displayed by size. Factor loadings above 0.5 and Cronbach's alpha above 0.7 are in bold.
Descriptive statistics
Table 7S (Supplemental Digital Content) reports the means and standard deviations of the components extracted from the EFA and purified samples. Risk had the lowest mean (1.97 ± 0.92), while certainty and adaptability had the highest (4.68 ± 0.49). In newness, only departure from pre-existing routines slightly exceeded 3, with disruption, departure from pre-existing behaviors, and risk scoring lesser. In benefit scale, actual operation had the highest score (4.11 ± 0.79), followed by profile (3.96 ± 1.07), while observability had the lowest (2.62 ± 1.42).
Linear regression models
Multivariate linear regression analyses were conducted to identify the determinants of the benefits extracted from the EFA: actual operation, profile, and observability (Figure 1). The main predictor of actual operation was certainty and adaptability (adjusted beta = 0.58; p < 0.001); it positively influenced actual operation, while departure from pre-existing routines (adjusted beta = −0.20; p = 0.021) negatively impacted it (Table 8S). The relationship between risk and actual operation was not significant. The determinants of profile were certainty and adaptability (adjusted beta = 0.56; p < 0.001) and scope (adjusted beta = 0.19; p = 0.030; Table 9S), while the relationship between risk and profile was not significant. Predictors of observability included risk (adjusted beta = 0.20; p = 0.032) and scope (adjusted beta = 0.36; p < 0.001) both positively impacting observability, with scope having a higher impact (Table 10S). Results of the linear regression models: relationships between the attributes of innovation and benefits.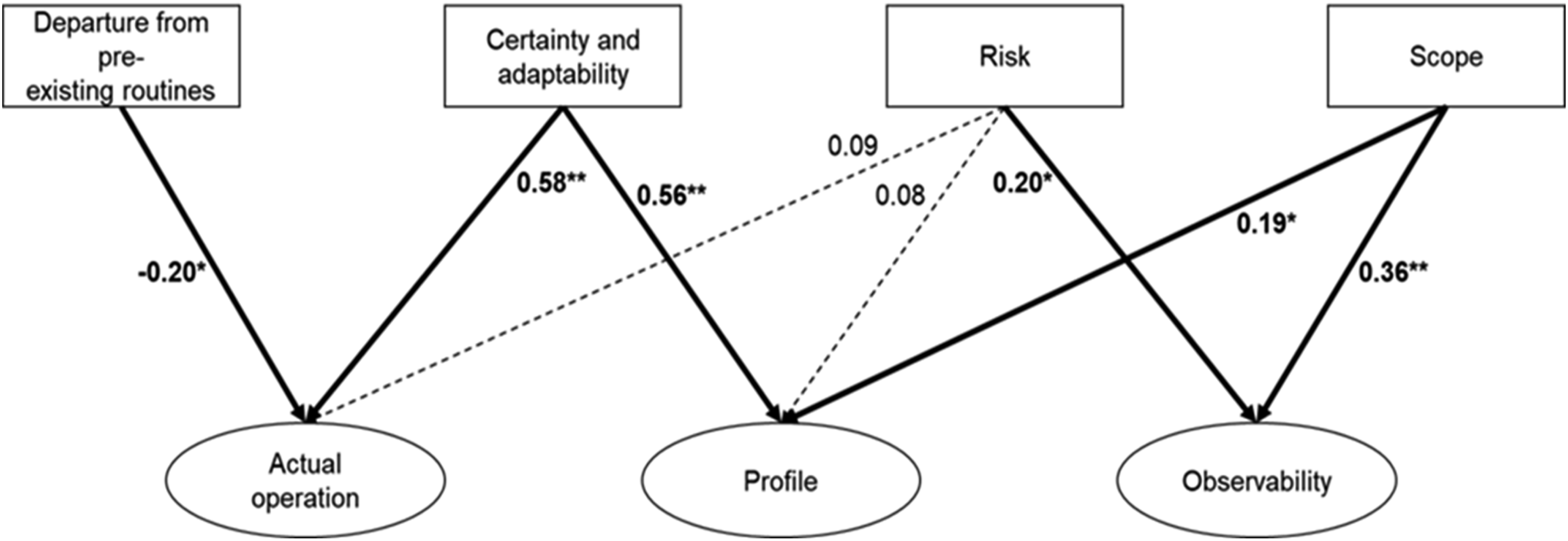
The control variables number of years as director of the complex operating unit, time spent in managing the complex operating unit, and number of employees within the complex operating unit were not significant in any of the regression models.
Discussion
The application of Adam’s instrument to our sample through an EFA confirmed the validity of all scales, except ideation, for an AMC. This may be because ideation could not be measured with a single subscale of the original model. Furthermore, we found differences in the validity of other subscales. In particular, several peculiarities and differences emerged compared to Adams’s framework.
Regarding RQ1, the main innovation attributes in an AMC were highlighted.
Our results showed that the primary factor explaining the newness in an AMC is the disruption, followed by risk, and departure from pre-existing routines and behaviors. The separation of the latter two factors in our analysis, respect to previous framework, clarifies the distinctions between routine and behavioral departures in an AMC, allowing these aspects to be captured and analyzed separately. The literature underscores the importance of examining routines and behaviors in AMCs, as such analysis is crucial for understanding effectiveness in the academic field, as confirmed by previous studies. 41
Regarding the application dimension, if complexity is the primary explanatory factor, certainty and adaptability were perceived as the most important attributes characterizing the innovations. The attribute of certainty and adaptability, resulting from the integration of two subscales compared to the original framework, is considered by professionals a distinctive element of the innovations in an AMC, synthesizing the effectiveness of innovation, a key element emphasized in the literature on healthcare innovation. 21
The Ideation dimension, following factor analysis, was found to consist of a single factor. Although this may not fully capture all aspects originally included in the scale, it can still be considered a valid measure of the phenomenon, especially in light of the number of questionnaires collected in the present study.
Three principal factors measure the benefits in an AMC. The first factor, actual operation, reflects the perceived capacity to achieve the planned results and was recognized by professionals as the most significant benefit of the innovation. The second important factors was the profile, confirming the perceived relevance for the attractiveness of an AMC in both individual and organizational terms. 28 Our study thus demonstrates that the professionals seem to be more interested in the benefits related to internal results (actual operation and profile) than those related to institutional visibility (observability).
In summary, with respect to the first part of our analysis, the main factors explaining the attributes of the innovation in an AMC were identified, and the original instrument to measure these attributes was simplified and adapted to an AMC, while maintaining its validity with a reduced number of items. This is a positive outcome of the application of the tool, as it facilitates the administration of a more concise questionnaire. The length and complexity of the original tool have drawn criticism from some respondents, and this represents a significant advancement for future research.
Regarding RQ2, our findings reaffirm previous research highlighting the importance of considering the relationships between innovation attributes 14 and the impact of various attributes on innovation outcome. 20
Regarding the first benefit of innovation, actual operation, the certainty of expectations and adaptability to local requirements positively influence operational effectiveness based on the perceptions of our sample. This suggests an enhanced ability to meet original objectives and solve related problems. Our results align with those of previous studies, indicating that the opportunity to experiment with and adapt to an innovation fosters stakeholder involvement 22 and improves overall output. 21 Additionally, we found that a significant deviation from pre-existing routines negatively impacts innovation in healthcare, supporting previous literature findings. 26 Innovations are more likely to achieve their intended objectives and effectively address problems if they do not deviate from established practices. The impact of innovation on pre-existing practices remains a critical factor in achieving objectives and must be mitigated through appropriate training and personnel selection to bridge the gap in skills required for new processes. Finally, a well-demonstrated relationship between risk and actual operation was not confirmed in our study. This connection may depend on the phase of innovation, 23 which was not explored in our study. Therefore, the regression analysis was unable to capture this relationship.
The second benefit of innovation, profile achieved by organization and individuals, is affected by the attributes of certainty and adaptability and scope. Our sample demonstrates that innovations that align with existing organizational values and can be adapted to local use (key dimensions that explain the factor certainty and adaptability) tend to contribute to the organization’s profile. 30
Furthermore, our study reaffirming the well-established relationship between scope and prestige, as demonstrated by Malik et al., 32 shows that a broader scope positively impacts the prestige of both organization and its individuals. However, the relationship between risk-taking and profile demonstrated in other studies on different sectors was not found in our study. This may be due to the greater reluctance to take risks in a hospital, 42 particularly given the nature of innovation and its potential consequences for patients. 32
The third key benefit of innovation in healthcare is its observability, which facilitates diffusion. 6 Our results confirmed that innovation with a broader impact, both within and beyond the organization, exhibits greater observability. Moreover, consistent with previous research, 32 this study identified that the level of risk associated with an innovation as well as the willingness of professionals to take risks significantly influence its observability also in an AMC. Our findings confirmed that higher levels of risk-taking and innovation risk correlate with increased observability.
These insights underscore the critical interplay between innovation attributes and their outcomes in healthcare settings, highlighting the need for careful consideration of existing practices and organizational alignment to maximize the benefits of innovation.
Conclusions
A major significance of our study is the identification of a more efficient tool for describing and capturing the complexity of innovation processes in an AMC. Managerial studies often undervalue the importance of practical results, as opposed to conceptual results. In this case, the usefulness of the tool can be appreciated both in terms of future research and, more importantly, as a resource to be used to facilitate, promote, and control innovation.
In fact, the presentation and discussion of the results at Careggi University Hospital served as an opportunity for effective organizational learning at various levels: • for hospital management, it provided a better understanding of the key determinants that influence clinical leaders’ judgment and motivation; • for departments, it helped compare their choices and results with those of other departments. • for clinical leaders, it facilitated self-reflection on the implicit priorities underlying past choices.
Innovation is a continuous practice in many organizations, particularly AMCs. By adopting the perspective of continuous change, the new simplified questionnaire can assist AMCs in an exercise designed to “make sequences visible and show patterns” 43 in an effort to provide new directions and greater purposefulness to the process of change.
We also aimed to provide new insights into innovation processes from the unique perspective of clinical leaders, who are key actors in an organizational context inevitably shaped by the logic of professionalism. 44 When asked to identify and describe the perceived characteristics of most significant innovations, their responses highlighted the importance given to the innovation’s contribution to professional recognition (profile).
From this perspective, professional benefits—at the organizational or personal level—are nearly as valued as the benefits derived from the practical functioning of innovation. This outcome is not entirely unexpected; the influence of professional over managerial dimensions in shaping clinicians’ organizational behavior is well documented. However, this study offers additional insights.
First, it provides an operationalized and quantitative measure of the importance of two dimensions—professional recognition and organizational functionality— which require balancing and monitoring through managerial intervention. Second, given the higher score assigned to the profile factor than to observability, the findings highlight that professional recognition (profile of the organization and individuals) is not easily captured within institutional frameworks (systems and organizations). Instead, subjective evaluation is predominant in this domain.
A final remark concerns the central role of the factor certainty and adaptability as a determinant of successful innovations, both in terms of actual operation and professional recognition (profile). The methodology we employed—the selection of innovations by respondents, administration of a questionnaire, and an ex post perspective—did not allow us to distinguish whether this factor represents an ex-ante intrinsic characteristic of the innovation or a result of the organization’s ability to manage the conditions that make an innovation viable. This implies that each item in this factor should be viewed as an indicator of the level of risk associated with innovation during the decision-making process. Simultaneously, during the implementation phase, it should be treated as a variable to address targeted managerial interventions.
From this perspective, our study offers practical guidance for management by leveraging the questionnaire as both a diagnostic tool during the decision-making phase and a framework for active and informed management throughout the implementation process.
Limitations and further research
Potential methodological limitations of this study concern two main aspects.
The first relates to the choice of a conceptual model operationalized through a validated set of specific questions. While a more open-ended approach might have yielded richer insights, it would have risked compromising methodological rigor.
The second concerns the use of an online questionnaire. Although this format was chosen, the methodology included a series of preliminary meetings with the departments to which the organizational units belong, in order to ensure a sufficient and consistent understanding of the questionnaire items.
The effectiveness of our tool could be confirmed by using a larger sample size or more than an AMC. Additionally, only one innovation perspective was analyzed. Other factors that influence innovation could be included in future analyses because the traits of the adopters can influence the success of the innovation process. Recognizing that every study has inherent limitations is fundamental to continuously improving the methods and tools used. However, the lack of consideration of all the variables involved in evaluating an innovative process is an inherent limitation of experimental research. 11
Important avenues for future research may include the integration of perspectives from other stakeholder groups, such as patients and nurses. This would allow for a more comprehensive exploration of innovation within Academic Medical Centers (AMCs), broadening the analysis to include the viewpoints of various healthcare professionals. Additionally, conducting the study in a different time frame—outside the post-COVID context—through a longitudinal approach could offer deeper insights and enhance the robustness of the findings.
Supplemental Material
Supplemental Material - An exploratory study on attributes and benefits of innovation in academic medical centers: Evidence from Careggi University Hospital
An exploratory study on attributes and benefits of innovation in academic medical centers: Evidence from Careggi University Hospital by Anna Romiti, Mario Del Vecchio, Salvatore Zimmitti, Daniela Matarrese in Health Services Management Research
Footnotes
Acknowledgements
Authors thanks all the directors of clinical units of Careggi University Hospital who participated in the study.
Consent to participate
Written informed consent to participate in the study.
Author Contributions
Conceptualization: AR and MDV; data curation: AR and SZ; formal analysis: AR and SZ methodology: AR and SZ; supervision: AR, MDV and DM; writing—original draft: AR, MDV, SZ; writing—review and editing: AR, MDV, SZ, and DM.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Careggi University Hospital (2023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.