
Abstract
India’s first health policy document in 1946 envisaged an ambitious health system comprising delivery of public health programs by the national governments and primary and secondary care by the state governments. Nearly seven decades later, neither of the ambitions have been realised. The delivery of public health programs is limited and uncoordinated, whilst primary and especially secondary care is of poor quality and unaffordable to the bulk of the population. This article assesses India’s health policy reforms and argues that at each juncture the policy instruments it utilised were inconsistent with the goals it was trying to achieve. The health care sector required more intervention than the central and state governments offered. The meagre funds allocated to public health programs and the unwillingness and inability of state governments to shoulder responsibility for primary and secondary care led to the dominance of the private sector in delivery, out-of-pocket financing, and fee-for-service payment to providers. Recent reforms have made some progress in addressing the lacunae but are handicapped by the pervasive dominance of the private sector which severely limits the choice of policy tools available to the government.
Introduction
Health policy has been at the centre of the policy reform agenda around the world for some decades, which is unsurprising, given the enormous economic and political costs of getting it wrong. Yet governments around the world continue to embark on reform paths that are known to worsen the problems of costs and access that they were intended to address. This is an article on the experience of India that took a series of wrong turns and is struggling to recover.
India’s first policy paper on health care published in 1946, The Bhore Committee Report, envisaged an ambitious health care system comprising delivery of public health programs by the central government and primary and secondary care provided by the state governments (Bhore, 1946). Nearly seven decades since, neither of the goals have been realised. The private sector has gradually come to account for an overwhelming share of hospital beds and health care spending. The skeletal network of public hospitals, understaffed and ill-equipped to deal with current demand for health care services, is choked with patients who are unable to afford private care.
Whilst India has made significant strides in improving public health outcomes, it fares poorly across almost all public health indicators relative to other economies at similar incomes and development and to its immediate neighbours (Dreze and Sen, 2011). Not only has the government failed to achieve its ambitious goals laid out in the Bhore Committee Report, but through a series of missteps has created a health system that severely limits access and promotes inequity.
India’s health policy failures have been well catalogued in the literature and policy debates and are largely attributed to the lack of resources, poor governance, urban–rural disparities, poor infrastructure, inadequate workforce, and stemming from other challenges associated with poor social infrastructure: poor education and literacy levels, lack of sanitation and hygiene, poor access to drinking water, and so on (Das Gupta, 2005; Dreze and Sen, 2011; Forgia and Nagpal, 2012; Radwan, 2005; Rao 2015; Rao and Choudhury, 2012; Rao et al., 2011). Its rising health care costs, mostly financed through out-of-pocket (OOP) spending by households, and consequent issues of access and equity have received limited attention only to be accepted as an outcome of a poorly functioning public health system.
This study addresses two interrelated questions: What was wrong with health care reforms in India? Why did India embark on the wrong health care reform path? The objective of the analysis is to understand how and why governments embark on avoidable policy misadventures in the hope that other governments, and indeed many scholars, will learn from their errors going forward.
In responding to these questions, this study employs a qualitative research design completed in two phases during 2013–2014. In the first phase, the authors completed a survey of the academic and extant literature relying primarily on Web of Science, SCOPUS, and Google Scholar in 2013 on health policy reforms in India and health system governance and health care reforms. India-specific policy documents and reports published by the Ministry of Health and nationally representative surveys published by the Ministry of Statistics and Programme Implementation (MOSPI) were also reviewed. This was followed by a series of semistructured interviews (n1 = 12) with senior policy makers of government officials and officials at the Ministry of Health at the central government and three state governments (Tamil Nadu, New Delhi (U.T), and Jharkhand). The objective of these interviews was to understand the broad institutional arrangements and governance relationships between stakeholders in India’s health system and if they varied across states. Reflecting on the literature survey and the interviews, the authors constructed a simplified normative framework of health care governance, mapping the role of a system of incentives and controls to manage economic behaviour of key stakeholders in the health system, whilst allowing the government to intervene and shape outcomes.
In the second stage of research, the authors applied the framework to assess health care reforms in India. To validate the data and emerging propositions, the authors conducted a second round of interviews (n2 = 12) with senior health policy officials (4) and hospital administrators (8) in public hospitals across three different states (Maharashtra, Karnataka, and Punjab) in 2014. The data collected from the 24 interviews were analysed in the context of the framework on health care governance developed and the two questions posed at the outset of this article.
The next section develops a simplified framework of health care governance focusing on the role of incentives and controls. This is followed by a review of health care reforms in India vis-à-vis the framework developed in this article. The concluding section discusses what was wrong with India’s reforms and why did it pursue these reforms.
Effective health care governance: A system of incentives and controls
The market’s potential to allocate resources efficiently holds great appeal to policy makers seeking optimal use of their spending and often is the cornerstone of contemporary reforms across most domains of public service delivery (Ramesh and Araral, 2010). The standard assumption is that competition amongst producers lowers prices, improves quality of services and ultimately societal welfare for both consumers and producers. However, the market’s ability to allocate resources efficiently and improve outcomes in the health care sector is compromised as most health care services despite being private goods have features of public goods (Blomqvist, 2011; Harding and Preker, 2003; Weimer and Vining, 2011). This implies that the market left to its own devices would produce less than optimal amount of health care services that are needed in a society.
The systemic governance failures that afflict the health care sector across modes of governance largely stem from the uncertainty associated with individual health outcomes and the stochasticity in the onset of illness. To overcome the welfare loss associated with this uncertainty, and to smoothen consumption during periods of illness and periods of good health, there is a strong economic case for pooling of risks in a given population through any feasible mechanism (e.g. insurance, tax-financed plans, etc.). However, the gains from risk pooling, in reality, have to be traded off with the welfare losses caused by asymmetries in information and conflicting incentive structures between consumers (patients), providers (physicians) and the third-party (insurer) who underwrites the contract. This trade-off has been well documented in the health economics literature. However, theoretically simulated solutions to deal with the malfeasance to engage in moral hazard, cream skimming, and adverse selection have failed to yield effective results when translated to policy or practice.
The conventional approach of dealing with market or government-centric failures is to rely on an alternate mode of governance in the provision and financing of the good or service (Weimer and Vining, 2011). This however has limited utility in the health care sector, as the governance challenges are deeply entrenched across modes of governance. For instance, the challenges associated with information asymmetry, which places providers in the dominant position due to users’ inability to assess the cost or quality of service or indeed even the need for it (Dranove and Satterthwaite, 2000; McGuire 2000), are prevalent in both state-financed as well as privately insured plans. Malfeasance of moral hazard wherein both users and providers have the incentive to overutilise health services if they know that the costs will be borne by a third party, insurer, or the government (Zweifel and Manning, 2000), which results in overconsumption of services and eventually overspending are equally pervasive in publicly financed plans. Adverse selection wherein high-risk users seek generous insurance coverage, insurers look for low-risk users, and providers look for sicker patients who are fully insured (‘cream skimming’) (Rothschild and Stiglitz, 1976), is one of the few failures that is not dominant across government modes of governance. Without government regulation, adverse selection and cream skimming can lead to a ‘death spiral’ of the insurance plan (Cutler and Zeckhauser, 2000; Pauly et al., 2007).
Whilst the market failures associated with asymmetrical information and moral hazard are equally pervasive in government-financed health care programs, governments can potentially address some of these shortcomings in health care markets. Thus, for instance, it can directly provide those services with public goods features or pay private providers to produce them. Similarly, it can use its position of authority and regulate providers to disclose information on quality, price, and outcome information to empower users vis-à-vis providers. It can also reduce the scope for adverse selection by banning risk selection by insurers and providers and mandating compulsory insurance for the population segment. There are also tools available to governments for containing moral hazard by altering payments and financing mechanisms in ways that reduce the incentive for overservicing or overcharging (Harding and Preker, 2003).
In reality, these are extraordinarily difficult tasks that require a level of information and political and administrative capabilities that most governments lack (Wu et al., forthcoming). The incomplete information on consumer and producer behaviour and the cost and benefits of different medical options make it difficult for the government to make informed choices. Even when they are able to make a good choice, governments may lack the capacity necessary to implement the choice in the face of opposition from vital stakeholders.
Public choice and new public management theories that emerged in the 1980s buttressed by neoclassical economic scepticism towards the effectiveness of governments’ ability to provide services recommended that governments purchase the service from private producers on a competitive basis. However, these theoretical propositions failed to recognise policy domain-specific nuances and size of governance failures that the unfettered pursuit of efficiency can result in. Indeed, an uncompromising pursuit of improving efficiency through the market mechanism is an unworthy goal to pursue due to the severe impediments it encounters in the health care sector.
A more worthwhile goal would be effectiveness, defined as the extent to which goals are achieved, which in the case of health care is providing basic access to all those who need it, regardless of the technical efficiency of the mechanism. It does not mean that effective mechanisms are necessarily inefficient: it rather implies that technical efficiency is not their primary concern. To achieve effectiveness in health care, it may be necessary for the government to intervene comprehensively by establishing an overarching policy framework that incentivises desired behaviour whilst constraining the undesired behaviour of key stakeholders: providers, users, and the third party. The innate incentive of the three key stakeholders are not compatible with the goals of effectiveness, nor are they aligned with the goals of each other, which lead to suboptimal outcomes even when they are technically efficient.
For instance, health care providers have an inherent incentive to exploit their monopoly power and information advantage over patients and the third party. Users have an inherent incentive to continue to seek medical treatment and not be cost-conscious consumers when they know that the costs are borne by a third party. Similarly, the third party has inherent incentives only to insure healthy patients or pass on costs across the risk pool it insures through higher premiums. Therefore, the government has to intervene to shape economic behaviour of these agents through a series of incentives that encourage desired outcomes whilst penalising any form of economic malfeasance. The overarching framework of incentives and controls will need to be accomplished through offsetting hybrid tools (rather than state- or market-centred tools) to achieve the balance between incentives and controls (Ramesh et al., 2015). Without such a governance framework, and the will and capacity to apply it, the goal of achieving effectiveness will remain elusive.
An orchestrated use of policy tools will enable governments to achieve the goal of providing universal health at costs affordable to society more effectively than either through market mechanisms or government regulations. The incentives for malfeasance under any form of conventional insurance or state-sponsored health plan by all stakeholders are large and cannot be controlled through either the market or regulation (Preker et al., 2007).
The proliferation of studies on health systems (Hafner and Shiffman, 2014; Mills 2014; World Health Organization, 2007), health care governance (Balabanova et al., 2009; Brinkerhoff and Bossert, 2008; Savedoff, 2011), design aspects of financing arrangements (Langenbrunner et al., 2009; Liu, 2003; Paolucci, 2011; Preker and Langenbrunner, 2005) and case studies on recent health care reforms in middle-income economies (Bonilla-Chacín and Aquilera, 2013; Hanvoravongchai, 2013; Savedoff et al., 2012; Somanathan et al., 2013) underscores the need for orchestrated efforts across multiple dimensions of health systems to achieve universal coverage.
The current reform orthodoxy in the international health policy community advocates a complex schema that developing economies with impoverished capacities must accomplish to achieving universal coverage. Whilst this is a useful endeavour in the march to achieving universal health care coverage, in many developing economies including India, the challenges that afflict the sector are more fundamental: governments are unable to steer the sector and shape health outcomes.
The framework developed in this article therefore takes a much narrow perspective and focuses only on the extent to which health policy reforms have been able to overcome key governance failures that afflict the health care sector. The framework therefore eschews many of the complexities and nuances of the type of policy tools required, its settings, its institutional prerequisites for them to be used effectively; similarly, the nature of regulations and the sequence of these regulatory controls in shaping behaviour. In doing so, for the purposes of this article, it usefully sidesteps the controversies in the health policy literature on specific choices on policy tools and instruments and their efficacy in organising the health care system (e.g. Should tax financed or contributory plans be used to expand government programs – Mills, 2014).
The essential proposition that this framework tests is the extent to which these incentives and controls, i.e. the ‘building blocks’ of an effective health system, were incorporated into health system reforms, India would be able to intervene in its health sector and shape outcomes. Without the ability to steer the health care sector and shape outcomes, implementing checklists on achieving universal health care coverage is a wasteful endeavour.
Health care reforms in India: An overview
India was a British colony until 1947 and the colonial government had little interest in health care of the population other than its own employees. After independence, the government focussed on industrial development and, later, agricultural development whilst neglecting social sectors such as education and health. The health policy components of the Five Year Plans until the 1970s emphasised sanitation, control of communicable diseases, and family planning rather than delivery or financing of medical care. India’s early health policy documents, particularly those by the Bhore Committee in 1946, the Murdaliar Committee in 1956, and the Kartar Singh Committee in 1967 envisioned the delivery of primary care through a network of subcentres and primary health care centres (PHCs); secondary care through community health care centres (CHCs); and advanced treatment at specialised hospitals in large cities. The lower level health facilities, which were funded and operated by state governments, provided free services to everyone who needed them and, in theory, acted as ‘gatekeepers’ to tertiary care through a referral system.
However, starved of funds and with limited accountability, the health centres were poorly run, suffered from chronic absenteeism, often out of essential medical supplies and equipment, and avoided by patients other than those without an option (Radwan, 2005). Most of these subcentres are housed in thatched huts or single rooms due to poor rental allowance that is allocated to them (Rao, 2015). The primary and community health centres also face debilitating shortage in manpower and infrastructure. A Government of India Report on Health Statistics in 2012 estimated that the shortfall in health care infrastructure was nearly 25% at the subcentres and PHCs and 40% at CHCs (Government of India, 2012). The report estimated that over 40% of the available positions for specialist doctors at CHCs were lying vacant due to shortage of applicants willing to work in rural areas and in small towns.
The only exceptions were district and specialty hospitals in urban areas that had to cater not only to an increasingly urban population but also to rural patients who flocked to these hospitals bypassing the primary and community health care centres. Unable to keep pace with the growing demand, public hospitals could only provide inadequate and low-quality service. The void was filled by the private sector which flourished under government neglect. Of course, they offered little relief to those without the resources to pay for the services.
To the extent the government did try to improve health care delivery, it concentrated on relatively privileged groups employed in the formal sector. The 1950s saw the expansion of new programs for the civil service and armed forces. These schemes offered comprehensive benefits for members and their dependents either at their own hospitals or reimbursed treatment at approved private hospitals. Expenditure on these schemes gradually increased to form as much as 10% of total government expenditure on health care by 2011 (Gupta and Chowdhury, 2014).
The government also established mandatory Employees State Insurance Scheme (ESIS) for those employed in the formal private sector and their dependents. The ESIS, supervised by the Ministry of Labour, functions through a network of hospitals owned by ESIS as well as recognised private hospitals. After nearly 60 years in operation, it covers less than 5% of the labour force or about 55 million individuals, including dependents. The utilisation rate of the ESIS program has consistently declined despite efforts to empanel private hospitals. A recent study found that ESIS members availed only 15% of the outpatients and 35 of the inpatient services from ESIS facilities (Dash and Muraleedharan, 2011)
By the 1960s, India had in place a barely functioning health system for the majority of the population and a slightly better system for the public sector and formal private sector employees. The neglect of medical care for the vast majority of the population allowed the private sector to grow and dominate health care delivery in the country. By the end of the 1960s, the share of public hospitals had declined from 92% of all hospitals in the country to a mere 50% and further to 10% in recent years. In contrast, private hospitals expanded to own 60% of all hospital beds and employ 80% of all health-care workers (Government of India, 2011). Health care financing in India has been increasingly more private, as the central and state governments together formed only 17% of total health spending in the 1950s and 12% in the 1960s (Bhat and Jain, 2004), which was one of the smallest public shares in the world. In the absence of public financing, private finance, almost entirely in the form of OOP payments, dominated.
Accession to the Alma Ata declaration in 1978 refocused the government’s attention on health and led to the publication of the National Health Plan (NHP) in 1983, the first policy document on the subject since independence. The document was full of platitudes about equity and justice and set fixed health outcome targets but contained few details on how it intended to achieve them. Indeed, of the eight health care components of the Plan (Nutrition, Prevention of food adulteration, Maintenance of drug quality, Water supply and sanitation, Environmental protection, Immunisation, Maternal and Child Health Services, School Health, and Occupational Health), none dealt with curative services, the most expensive component of health care. The sixth five-year centralised plan (1980–1985) of the Indian government explicitly recognised the need for privatisation of the health system (Duggal, 2007). With government sanction, the private sector continued to thrive and expand. At the end of the Plan period, all Plan goals were found to have been missed (Rao, 2015).
The macro-economic crisis in 1991–1992 and fiscal stringency conditions associated with the loan from the International Monetary Fund to Government of India resulted in significant downsizing of health budgets across state governments. Most capital investments across most Indian states were stopped due to paucity of funds; the only new health programs implemented were to control infectious diseases, family planning, and child immunisation, all of which financed through World Bank loans. The scaling back on public programs, and absence of regulations on private providers, allowed providers to flourish and new hospitals mushroomed across India (Rao, 2015). During 1991–2003, private health care expenditure in real terms grew almost three times higher than per capita income (Bhat and Jain, 2004).
After nearly two decades of policy drift, aggravated by the economic crisis the government announced a new National Health Policy in 2002, which was reaffirmed in the 10th Five-Year Plan (2002–2007). In addition to the familiar proclamations of commitment to equity, affordability, primary care, and the need for increased government spending, NHP 2002 heralded two new departures. For the first time, the government stated that it would promote decentralisation and explicitly stated its intention to expand the role of the private sector in health care. The change in shift was followed by unprecedented devolution of responsibility for health care to local government coupled with exponential growth of private delivery. The marriage of privatisation and decentralisation promoted by the new policy resulted in increasing fragmentation of the health system and aggravated the dismal state of the health care system. 1
Horizontal fragmentation refers to the division of responsibilities across several government agencies, whilst vertical fragmentation refers to the division of responsibilities across different levels of government. The Indian Constitution assigns primary responsibility for the provision and financing of health care to state governments. However, most broad-based taxes are collected by the central government giving rise to vertical fiscal imbalances, which is offset through block and specific-purpose grants to state governments based on equalisation formula. However, the transfers have been insufficient to significantly reduce fiscal disparities across states, particularly in states with poor health outcomes (Rao, 2015; Rao and Choudhury, 2012; Rao and Singh, 2005).
Disparity in terms of administrative capacity and fiscal resources across Indian states is vast and aggravated with decentralisation, which affected the sector’s performance. In 1993–1994, the state with the lowest public health spending per capita (Bihar) spent 53% of what the highest (Punjab) spent. By 2008–2009, this share had declined to 32%, showing rapid increase in interstate fiscal disparities. Southern states such as Karnataka, Kerala, and Tamil Nadu have been relatively more successful at delivering health care than Eastern and North-eastern states.
Similar variations in health workforce and health outcomes were also evident across states in India. Health care workers per 1000 residents ranges from 1.0 in Bihar and Uttar Pradesh to about 4 in Kerala and New Delhi. There was a 63% difference in infant mortality rates between rural and urban India in 2012 (Government of India, 2015). In 2012, the average life expectancy at birth in the central state of Madhya Pradesh was 12 years lower than the southern state of Kerala (Rao, 2015) Similarly, the share of births attended by skilled personnel ranges from low 30s in Uttar Pradesh, Jharkhand, Chhattisgarh, and Assam to the high 90s in Tamil Nadu and Kerala. Kerala, Maharashtra, and Tamil Nadu have maternal mortality rates (MMR) below 100, whereas poorer states including Assam, Uttar Pradesh and Uttarakhand have MMR closer to 300 (Government of India, 2015).
In 2005, soon after winning the election on ‘common man’ platform, the Indian National Congress-led government began to increase public funding for health care and intervene in the sector through increased spending. It launched the National Rural Health Mission (NRHM) which focused on improving maternal and child health and providing primary care to rural population in the 18 least developed states (out of 28). The central government provides funding to state governments on a matching basis for delivering NHRM programs. Since many states lack both administrative and fiscal capacity to implement the program, less than half the funds allocated by the national government was actually spent (Rao and Choudhury, 2012). Further, the increased central funding through NRHM did not necessarily result in increased spending on the sector due to cutback in expenditure by state governments (Duggal, 2009; Rao and Choudhury, 2012).
NHRM did little to help the population to access resources necessary to pay for health care. A nationally representative sample studied in 2006 found that 40% of those hospitalised had to borrow money or sell assets to pay for their health care expenses; and 35% of those hospitalised fell below the poverty line after paying for hospital-related expenses (MOSPI, 2006).
The Indian government took the first serious steps towards establishing national health insurance with the launch of Rashtriya Swasthya Bima Yojana (RSBY) in 2007. The scheme provides free inpatient and outpatient in designated private and public facilities to recognised poor households to a maximum of INR 30,000 (USD 500) per annum. State governments identify eligible families, but the scheme is implemented through private insurance companies. The premium for the scheme is shared 75:25 between central and state governments. Many states have introduced more generous versions of the scheme. RSBY and related programs expanded rapidly and by 2010 they covered over 300 million people, or more than a quarter of the population, up from 55 million in 2003–2004. More than 180 million of the newly covered were people living below the poverty line.
In 2010, the government established the High Level Expert Group (HLEG) following the realisation that the sector required more comprehensive reforms than what had been done to date. The report, published in the following year, for the first time since Independence proposed detailed measures for the government to take to reform the sector. It recommended universal access to essential services through integration of all health programs under the central government’s direction, massive increase in government funding, strengthening of the role of district hospitals, and stronger regulation of the sector.
The effects of the reform measures adopted in recent years are encouraging according to recent health statistics. The launch of NRHM and RSBY slowed down the growth of OOP expenditure, from 71% in 2005 to 58% in 2012 (Figure 1). Remarkably, and contrary to popular perceptions and theoretical expectations, health care spending as share of national income also declined from 5% to about 4% of GDP during the period (Figure 1).
Health care expenditure in India 1995–2012. Source: WHO (2014).
The decline in total health spending in India was consistent with experience of other countries such as Thailand and China which also experienced decline following increased government spending and reduced OOP. High OOP is often accompanied by weak government supervision of the sector which allows providers to overservice and overcharge (Ramesh and Wu, 2009; Wu and Ramesh, 2009). Correspondingly, decline in OOP reduces the scope for overservicing and overcharging which has the effect of reducing total expenditures.
Whilst OOP expenditure has begun to decline, India is left with a highly fragmented and privately organised health system. As shown in Figure 2, the responsibility for financing and, especially, administering health care programs is divided amongst different levels of government. The central government accounts for about 31%; state governments about 64% and local bodies about 5% total public expenditure on health care (Gupta and Chowdhury, 2014).
Central and state government health care schemes. Source: Authors.
Central government ministries including Health, Defence, Labour, Railways administer separate health care programs with limited coordination between them. The Ministry of Labour & Employment administers the mandatory social insurance program ESIS through a network of its own hospitals as well as select private hospitals across the country. The Ministry of Labour & Employment also administers the RSBY Scheme in conjunction with health ministries of state governments. The Ministry of Health, which accounts for a fifth of public health expenditure, administers the NRHM and other public health care programs. Many of these programs are delivered at the district level in state governments, again with limited coordination.
The Ministry of Health in state governments is primarily tasked with running a network of primary, secondary, and tertiary hospitals that provide free treatment to all residents. These hospitals are owned by the state government and are run by full-time public employees. There is no coordination or supervision of these hospitals with the central government’s Ministry of Health. The state governments however coordinate RSBY and NRHM programs with the central government as they are jointly financed. In addition to the network of public hospitals, many state governments often run their own health care programs. These are based on social insurance principles and administered by a third-party insurer. Health programs of Tamil Nadu, Karnataka, and Andhra Pradesh predate the RSBY and have somewhat different institutional and financing arrangements. Newer programs, as in Himachal Pradesh, rely on the RSBY architecture but provide for extended coverage and have more generous benefits.
Whilst the central government aims to expand health care coverage through public insurance, it is encumbered by the sheer complexity of the current institutional arrangements spread across several government ministries at different levels of government. However, increased centralised funding and the vertical integration of the NRHM program are believed to have improved coordination between state and central governments.
Discussion
What was wrong with India’s health care reforms?
Simplified framework of incentives and controls in an effective health system

Incentives and controls in health system in India
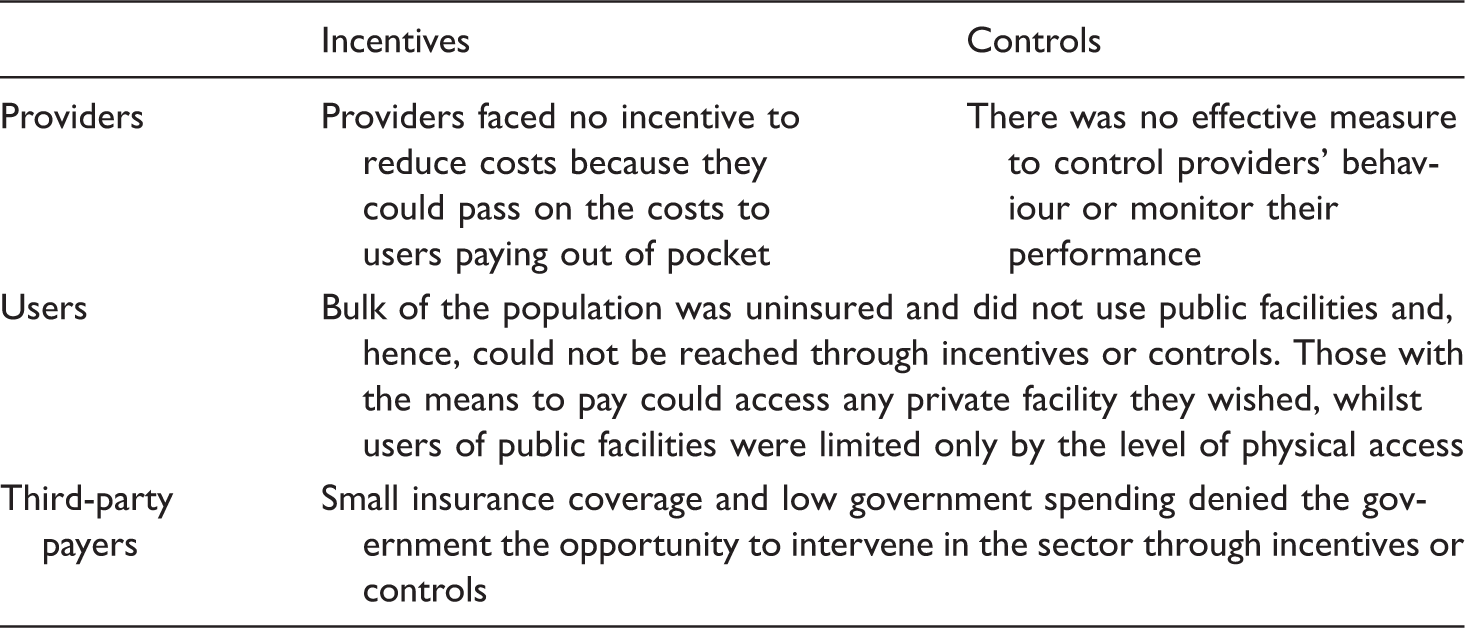
The reliance on OOP has had an incapacitating effect on the government’s ability to influence the sector through the users. Since most users could visit any provider they wished and pay them directly (through OOP payments), the government had no direct way to affect their behaviour either through incentive or control. Those able and willing to pay for health care did so but with the disadvantage of information asymmetry and absence of effective controls on providers’ behaviour which increased the financial burden on them and on the society as a whole.
Third-party payers have played a similarly insignificant role as a health policy tool in India. Public spending on health care has been so small that the government could not meaningfully use fiscal transfers as a tool for either incentive or control. Similarly, insurance covered less than 5% of the population which was not large enough to offer the government a tool for shaping the sector’s behaviour and performance. The ESIS, the largest insurance scheme in India until recently, provided services at its own facilities, which were run poorly and largely avoided by members, thus reducing the opportunity for government to intervene in the sector.
Whilst providers offer the government a potentially powerful tool for affecting the functioning of the health care sector, in the case of India, the potential was severely limited by the financing and payment mechanisms that exist in the country. OOP and fee-for-service (FFS) require appropriate monitoring to ensure that providers do not engage in moral hazard that undermines population’s access to necessary health care. But in India, as mentioned earlier, there was no meaningful control over FFS charged by providers and no substantial help for users with their OOP payments.
Indeed, the government had limited incentive to control FFS or OOP, because government officials and elite groups were already covered by comparatively generous programs and so did not face the burden that the rest of the population faced. Whilst health care providers are politically and economically powerful in most countries (Duran-Arenas and Kennedy, 1991; Fuchs, 2011; Pauly, 2009), they are especially powerful in India due to their overwhelming size. Their monopoly over prescription of diagnosis, treatment procedures, and drugs coupled with information asymmetry allows them to evade accountability to the government as well as users. The inability of the government to shape and influence outcomes in the health sector through users and third-party payers due to weak governance arrangements further emboldens providers to pursue their interests unencumbered.
Providers, insofar as they are driven by profits, compete aggressively to attract patients but, once successful, use their monopoly power and information advantage to maximise their income. This resonates with the health care reform experience of China and Vietnam over the past decade. Health care providers (public hospitals in this case) were incentivised to generate and retain revenue through user fees from patients. This resulted in rapidly increasing costs mostly financed out of pocket by patients with insignificant improvements in health care outcomes (Ramesh and Wu, 2009; Somanathan et al., 2013). Strict government monitoring and regulations can constrain such behaviour but require high level of information and administrative capacity on the part of the government (Wu et al., forthcoming). However, once material interests of dominant actors are advanced in a reform process, the government has limited options for reform. It requires formidable capacity across many dimensions for the government to change status quo and empower other stakeholders in the health system.
India’s federal political system and decentralised administrative system further undermine effective governance of the sector. The horizontal and vertical fragmentation over the provision of health care services stymies the government’s ability to deliver quality health care through the public sector, allowing private providers to dominate the sector to their advantage.
The recent launch of NRHM and RSBY has created new opportunities for the government to establish a system of incentives and controls. Notwithstanding their failure to achieve targets (Ashtekar, 2008; Rao and Choudhury, 2012), evaluations show that the NRHM improved access and utilisation at primary centres (Husain, 2011). For the purposes of effective health care system outlined in this article, the central government financing for the NRHM gives it the leverage to intervene in the sector, an opportunity it sorely lacked in the past. In exchange for funding, the government can now impose conditions, monitor progress, and hold state governments accountable on key performance indicators as continued funding is contingent on meeting targets. This in turn pressurises state governments to improve the performance of their health care facilities.
Similarly, the design of the RSBY allows the government to exploit its monopsony power as a large purchaser of health care services, a powerful tool to exert market power in the health care (Preker and Langenbrunner, 2005). The government has negotiated package rates with hospitals in its network for most illnesses. As of 2012, a total of about 5000 private hospitals and 3000 public hospitals across 25 states had joined the RSBY (Forgia and Nagpal, 2012). Whilst the benefit package is relatively small (USD 500) per family per annum, it gives the central government leverage to establish incentives for providers and controls over treatment costs. As a large purchaser of services, it allows the government to also implement controls over the third-party payers (i.e. insurance companies) who until recently were inactive participants in India’s health system.
This resonates with universal coverage reform experiences of Indonesia and Thailand. The universal coverage reforms underway in Indonesia aim to integrate many of the insurance schemes under the BPJS Health Insurance Organization, making it the world’s largest single-payer health system. The National Health Security Office performs the similar function in Thailand’s health care system and has been instrumental in the success of Thailand’s universal coverage reforms (Tangcharoensathien et al., 2014).
The design of the RSBY has also empowered users, the weakest and most vulnerable stakeholder in the system. Benefits are portable and patients can visit any empanelled provider in India. Whilst competition for patients amongst providers does not drive down prices in health care due to various market failures (Dranove and Satterthwaite, 2000; McGuire, 2000), it does force physicians to compete on quality of services. This not only reduces the power of the physician agency but also empowers patients who had previously remained vulnerable and at the discretion of the health care providers.
Experiences from universal coverage reforms underway across developing economies suggest that the ‘near poor’ and those employed in the informal sector are the most challenging population segments to cover under contributory programs. China and Thailand have avoided this challenge by abandoning contribution requirement from users in their health financing schemes. The Popular Health Insurance rolled out in Mexico also financed from federal and state governments revenues (Bonilla-Chacín and Aguilera, 2013). The noncontributory design of the RSBY, with portable benefits, makes it an attractive proposition for targeted beneficiaries to enrol. However, its low benefit level and low levels of government spending limits their usefulness as policy tools for promoting policy effectiveness. The HLEG recommends that the government must increase health care spending from 1.2% of GDP currently to 3.0% by 2022 to make a significant improvement (Government of India, 2011). However, the increased government spending on health care unaccompanied by appropriate incentives and controls discussed earlier will only result in ballooning of health care costs without ameliorating issues of access and equity in the long run.
Why did India embark on the wrong health care reform path?
As the government reflects on the wide-ranging recommendations of the HLEG it is opportune to reflect on why did the Indian government not begin to address the health care problems afflicting the country earlier. Why did the government allow the mix of FFS-OOP to flourish unchecked despite their known deleterious effects?
In the initial years after independence, the government’s economic plans had prioritised industrial and agricultural development and largely neglected social policy including health care. The government also had limited incentive to intervene in the health sector as elites and government officials had access to generous plans and health policy was not an electoral priority until recently. Governments fought and won elections on more palpable political problems such as unemployment, economic growth, and corruption that concerned India’s insular electorate. The ensuing discussion has also argued that even if it wanted to, it did not possess the required policy tools to influence and shape outcomes in the health care sector as private providers emboldened by the FFS-OOP mix had come to dominate the sector.
The perils of cost escalation associated with FFS payments are not unique to India and have plagued both developed and developing economies. Whilst FFS can be a highly efficient mechanism for paying service providers, success in the case of health care depends on meeting numerous conditions. The misuse of ‘physician agency’ associated with FFS payments can be countered by using various institutional arrangements to reduce their market power, but whether it is done depends on the capacity to design the necessary governance arrangements and intervene in the sector.
The dominant reform thinking during the 1980s and 1990s also contributed to weakening of the health care system in India. The prevailing consensus amongst leading international organisations during the period was that the main policy problem in the developing countries was overbearing governments which had to be reined in if policies were to succeed. Policy documents of the World Bank from the 1980s to 1995 recommended developing economies to rely on user fees to finance health care and generally employing market mechanisms to finance and deliver public services (World Bank, 1997). Public provision and financing of services, government regulation and control were considered anathema by the mainstream public management orthodoxy during this period (Ramesh and Howlett, 2006), a trend that continued till the Asian Financial Crisis in 1997 (Ramesh, 2009). Most governments responded to the crisis by implementing reforms that increased public resources available to pay for health care without corresponding measures to wind back FFS payments or implement controls to monitor increase public financing of private care.
It is only as recent as mid-2000 that analysts began to appreciate the importance of systemic incentives and controls accompanied by government oversight, implicit in the reform prescriptions of ‘strong purchaser of healthcare services’ and using ‘innovative provider payment contracts’. Recent trends in health care reforms around the world reveal widespread efforts to employ institutional arrangements such as utilisation reviews, fee withholding mechanisms, and diagnostic-related groups and capitation payments to curb payments to providers (Harding and Preker, 2003; Langenbrunner et al., 2009; Langenbrunner and Somanathan, 2011; Preker et al., 2000; Preker and Langenbrunner, 2005).
The higher acceptance of enhanced government stewardship and control over the health system coincided with a change of government in India. The Indian National Congress-led government came to power in 2004 with the promise of expanding social programs and over the 10 years enacted legislation to increase government expenditure across a range of social policies including health, employment generation, education, and food security. The reforms have given the government some levers to intervene in the health sector to improve performance. The reach of the reforms is still limited though, and the government needs to do more if it is to achieve its ambitions of universal health care. Indeed, the increased public spending may promote windfall for providers if not accompanied by further incentives and controls on their behaviour.
Conclusion
This article has argued that effective health policy requires systemic regulation and oversight of the medical sector through coordinated use of policy tools to manage economic behaviour of providers, users, and insurers. When viewed within the context of effective governance framework proposed in the article, India’s health policy failed along every key dimension. With little government spending or national insurance, the government had few policy leverages over the sector. Regulating the providers, most of whom were private, was its only workable instrument and the government did not deploy it effectively.
This article’s contention is that health care reforms in India failed to achieve their professed goals because the government did not exercise the needed stewardship over the health system and indeed weakened it. Not only did the government not intervene to reduce the market power of private providers, it gave them unfettered access to exploit the inelastic demand for health care services. The problem of poorly regulated private providers was aggravated by, and entwined with, the FFS-OOP instrument mix which favoured private provision and financing. Overcoming the political and economic leverage of providers who thrived in the absence of government regulation for more than five decades was a daunting challenge and the government failed to meet it.