
Abstract
Human immunodeficiency (HIV)-infected patients and men who have sex with men (MSM) have a higher rate of high-grade anal intraepithelial neoplasia (HGAIN), a likely precursor to anal cancer. This retrospective study describes the outcome of treating MSM with incident biopsy-proven HGAIN in an urban community health setting with access to outpatient ablation or operative treatment. The main outcome was freedom from HGAIN at follow-up. One hundred and fifty-three met inclusion criteria; 86 (56%) were HIV-infected. Eighty (52%) received outpatient ablation, 49 (61 %) had a follow-up within nine months. Among those, 26 (53%) were free of high-grade disease, 19 (39%) had high-grade disease; and 4 (8%) had unknown grading. In a logistic regression model, a lower extent of anal disease (1 quadrant versus 2, 3 or 4 quadrants) at the time of treatment was significantly associated with a lower probability of high-grade disease (P value 0.04). HGAIN could be managed in a community health setting; however, systems are needed to ensure follow-up care.
Keywords
Introduction
The prevalence of human papillomavirus (HPV)-associated anal squamous cell carcinoma continues to increase among HIV-infected patients despite the advent of combination antiretroviral therapy (cART). 1 This lack of benefit is in contrast to AIDS-defining cancers such as Kaposi sarcoma which have been declining with cART. 2 Persons at highest risk for anal cancer include HIV-infected patients, men who have sex with men (MSM), women with high-grade cervical lesions as well as those with cervical and vulvar cancers.3–7 Anal cancer has an annual age-adjusted incidence rate of 1.5 per 100,000 person years in the US general population; however, its rate among HIV-infected MSM was estimated to be 70–100 per 100,000 person years.8–11 Given that MSM account for approximately 50% of the HIV-infected patients in the USA, addressing HPV-related disease should be an important component of the preventive health care of HIV-infected patients at risk.
Screening HIV-infected MSM for anal cancer with annual anal cytology has been shown to be cost-effective with a ratio of $16,600 per quality-adjusted life year saved, a value similar to other accepted screening tests such as colon cancer screening. 12 For anal screening to become widely used there needs to be additional evidence that treating high-grade lesions affects disease progression.
High-resolution anoscopy (HRA) is a technique used to detect high-grade anal intraepithelial neoplasia (HGAIN), the likely precursor to invasive anal squamous cell carcinoma. Cohort studies involving HRA clinics at tertiary care centres have shown encouraging treatment results.13–17 For example, Cranston et al. reported a 64% efficacy which was defined as normal or low-grade biopsy at follow-up after treatment using infrared coagulation (IRC). Far less is known about treatment outcome among those attending community health settings with access to ablation therapy for lesions at high risk for progression to anal cancer.
The purpose of this study was to describe the outcome of treating incident biopsy-proven HGAIN in HIV-infected and non-HIV-infected MSM receiving primary health care in an urban community setting. We were specifically interested in the rate of high-grade disease after treatment with ablation.
Methods
Study setting and population
Fenway Health (FH) is the region's largest community-based primary care provider of HIV/AIDS medical and mental health services. It serves approximately 10,000 patients including 3200 HIV-infected patients. Sixty percent of the overall male population is MSM and 92% of HIV-infected patients are MSM (Chris Grasso, Fenway Institute, personal communication, 11 August 2011). FH has had a computerized health-information system since the mid-1990s. MSM who received their primary care at FH and were diagnosed with high-grade anal lesions treated either at FH or at its affiliated tertiary care hospital Beth Israel Deaconess Medical Center (BIDMC) during the time period from 1996 to 2010 were eligible for study inclusion. Patients were initially identified because anal cytology testing had been performed. Patients with any abnormal cytology underwent a more invasive examination with either outpatient or operative evaluation. Only those who had their first intervention during the specified time period were included. Treatment consisted of either outpatient ablation using a high-frequency desiccator or operative management with carbon dioxide laser destruction. All patients had incident, biopsy-confirmed HGAIN and at least one follow-up visit. All follow-up visits included a digital rectal exam and an internal examination with either outpatient HRA or operative evaluation. Patients with a history of prior anal or colorectal cancer or major colorectal surgery were excluded. Those who had been treated for anal dysplasia at another institution prior to joining FH for primary care were not included.
HRA is a procedure similar to cervical colposcopy and allows the identification and biopsy of abnormal tissue. HPV lesions turn white with the addition of acetic acid, a process known as ‘acetowhitening.’ Three percent acetic acid was used to visualize abnormal tissue and identify lesions which needed to be biopsied. High-frequency desiccation involves treatment in an outpatient setting with local anaesthesia. In this procedure, electric current is used for precise excision with limited blood loss. Operative carbon dioxide laser destruction uses infrared light energy to vaporize affected tissue. Grades of anal intraepithelial neoplasia (AIN) range from AIN-1 to AIN-3, with HGAIN defined as AIN grade 2 or higher, including carcinoma in situ (CIS). The study was approved the Fenway Health Institutional Review Board. Agencies funding this study had no role in the collection, analysis or interpretation of data.
Study design and definitions
We performed a retrospective cohort study of patients with incident HGAIN during the specified time period. Each biopsy was recorded using the highest histological grading noted in pathology report. Medical record review was performed using an abstraction form to document relevant past medical history, laboratory data including CD4 cell count for HIV-infected patients, anal biopsy and anal cytology results. Information on the extent of disease as measured by the number of anal epithelial surface quadrants involved was also abstracted. Duration of follow-up was delineated by the date of the initial pathology with high-grade disease and the date of the most recent office follow-up visit.
Data analysis
Summaries are provided for the percent of patients with first follow-up between three and nine months after ablation and the percent of patients with recurrence during that time period. We also used polychotomous logistic regression for patient outcome. Outcome was divided into three categories: recurrence, lack of high-grade disease or unknown status. Those classified as ‘unknown status’ had an internal exam, but did not have a specific grading recorded in the chart. Exact power calculations were based on the Fisher exact test. All P value significance levels were two-sided. The following covariates were tried in the logistic regression model: number of epithelial surface quadrants involved (1 versus 2, 3 or 4), age (<42 versus age ≥42, where 42 was the median age) and HIV status. The number of affected quadrants described the extent of disease. Statistical analyses were performed with SAS 9.2 (SAS Institute, Cary, NC, USA).
Results
Two thousand and twenty-four anal cytology tests were performed and there were 295 cases of biopsy-confirmed high-grade disease. Two-hundred and thirteen incident cases of HGAIN were identified. Of those, 14 patients who were not treated and 46 patients who did not have at least one follow-up visit with either outpatient HRA or operative evaluation were excluded. One hundred and fifty-three MSM patients met inclusion criteria. One subject was diagnosed with invasive anal squamous cell cancer at the initial evaluation and was excluded from follow-up analysis.
Baseline characteristics are presented in Table 1. The cohort included predominantly Caucasian MSM (89%) and 86 (56%) were HIV-infected. Mean duration of HIV diagnosis was 11.7 years and median CD4 count 514 cells/mm3 with a range of 21–1308 cells/mm3 at the time of diagnosis. Seventy-seven percent of HIV-infected patients were on cART at the time of diagnosis. Sixty-four percent of the 153 patients had a known history of anogenital warts. HIV-infected patients were more likely to have a current history of substance use (31% versus 15%, P value 0.02). Of the 153 cases, 63% had disease classified as either AIN-2 or AIN 2–3 (Table 2).
Baseline characteristics by HIV infection status

Indicates presence of characteristic at initial diagnosis
Initial biopsy result

AIN = anal intraepithelial neoplasia; AIN 1–2 and AIN 2–3 were used in pathology reports. Categories included AIN 1–2, AIN 2, AIN 2–3 or AIN 3 for high-grade disease
Treatment included either office-based ablation with a high-frequency desiccator or operative carbon dioxide laser destruction. Eighty patients (52%) were initially treated with ablation. Of those, 49 (61%) returned for follow-up at least once between three and nine months after treatment. Among those, 26 (53%) were free of high-grade disease, 19 (39%) had high-grade disease and 4 (8%) had unknown disease grading. The outcome in patients with an operative procedure could not be analysed because of the lack of regular follow-up evaluations. Table 3 shows the percentages of freedom from high-grade disease, presence of high-grade disease and unknown for various subgroups.
Outcome in patients with high-grade disease who underwent outpatient ablation and were seen between three and nine months
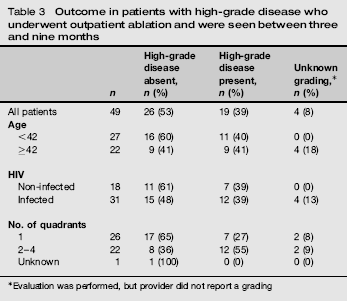
Evaluation was performed, but provider did not report a grading
A polychotomous logistic regression model including HIV status, dichotomized age (<42 versus ≥42) and extent of disease captured by the number of epithelial surface quadrants revealed that lower extent of disease was significantly associated with a lower probability of high-grade disease at the first follow-up (P value 0.04) (Table 4). ‘Univariate Risk Ratio’ and ‘Univariate P value’ refer to the model containing only that covariate, and ‘Adjusted Risk Ratio’ and ‘Adjusted P value’ refer to the model containing all three covariates. This study had a large enough sample size to have 80% power to detect a significant difference between true percents free of high-grade disease of 72% and 30% for the two age groups or 81% and 37% for the HIV-infected and non-HIV-infected groups.
Logistic regression for freedom from high-grade dysplasia 3–9 months post-treatment

Discussion
This retrospective review describes the treatment outcomes in both HIV-infected and non-HIV-infected MSM at an urban community health centre with access to ablation treatment for HGAIN during the cART era. Of the evaluable subjects, 52% were treated with ablation and 61% returned for their first follow-up at least once 3–9 months after ablation. Fifty-three percent were free of high-grade disease at that time.
Lower extent of disease as captured by the presence of only one quadrant involved at the time of treatment was significantly associated with a lower probability of high-grade disease at follow-up (P value 0.04). This may be explained by the possibility that small burdens of HGAIN are easier to identify and fully treat after one ablation session compared with larger burdens of disease. Age and HIV status were not significantly associated with response to treatment. This might have occurred because of the small sample size with follow-up at 3–9 months, or because the timing of our analysis did not allow us to assess the long-term prognosis associated with HIV status or with age. A larger cohort of patients followed prospectively at regular time intervals for a longer time period might show different results.
The natural history of HPV-related anal carcinoma has yet to be fully elucidated; however, given similarities in associated HPV types and histological correlations between anal and cervical carcinoma, HGAIN (AIN-2 or greater) is believed to be the likely precursor to invasive anal carcinoma, and ablation of these lesions may decrease the patient's long-term risk for development of anal carcinoma. Management of HGAIN includes ablation either in the outpatient setting or in the operating room, depending on the size and extent of disease. Patients are then re-examined with HRA at approximately six months after the procedure. 18
Prior to our study the published data on outcome of treating anal dysplasia were derived from tertiary referral centres during the early or pre-cART era. In a cohort of 68 HIV-infected patients Goldstone et al. 14 found a per-individual lesion success rate of 72% in HIV-infected and 81% in non-HIV-infected patients after treatment with IRC in an office-based setting at a median follow-up of 2.5 years. Success rate was defined at the probability of destroying an individual high-grade lesion with its first treatment. The same group recently published data on long-term outcome with a median follow-up time of five years. The probability of freedom from high-grade disease at follow-up was 67% for HIV-infected and 80% for non-HIV-infected. Nevertheless, the rate of loss to follow-up was about 30%. 16 The same group also published on the efficacy of treatment with electrocautery ablation (ECA). In that study patients were followed for at least five months. In non-HIV-infected and HIV-infected MSM the probability of curing a lesion after first ECA was 85% and 75%, respectively. 17 Treatment success was defined as no evidence of HGAIN on HRA or benign cytology if a follow-up HRA was not performed. Cranston et al. reported a 64% efficacy with using IRC in HIV-infected MSM. Efficacy was defined as normal or low-grade biopsy at follow-up. Patients were followed for a mean of 140 days after the intervention. 15 In a cohort of 181 HIV-infected and non-HIV-infected patients, Nathan et al. 13 showed that 63% were disease-free at 12 months. Patients were treated with either laser ablation, excision or imiquimod.
Although we had access to information on up to 13 years after the initial diagnosis (range, 0.6–13 years), we were not able to accurately evaluate long-term outcomes, given the lack of follow-up anal examination at regular time intervals. Identifying factors contributing to this lack of regular follow-ups will be important to improve the care of HIV-infected patients who are living longer in the cART era. Patient factors might include other competing health issues or social factors that might interfere with adherence to follow-up and engagement in care. As 32% of patients had a past or current history of illicit drug use, programmes that address this particular issue might have an impact on engagement in care in this population at highest risk for HPV-related anal carcinoma. In addition, if patients have misconceptions about genital HPV infection and its management, it would be important to specifically identify factors unique to the MSM population to overcome this barrier. Lastly, system-related factors might include the limited accessibility of providers with expertise in HRA and ablation of HGAIN, or limitations in knowledge of the primary care provider with respect to the potential utility of screening for and treating HGAIN.
The current study shows that identification and treatment of HGAIN could be carried out in an urban community setting with access to ablative treatment; however, systems need to be in place to ensure follow-up care after interventions. Future studies are needed on the long-term outcome of treating HGAIN in community health centres. As HIV-infected patients live longer, their care will likely be shifted from specialized tertiary care centres to primary care settings. There will therefore be a need for more intensive cancer surveillance as non-AIDS-defining malignancies become more prevalent in the post-cART era. Implementation of systems to ensure proper follow-up care for those receiving ablative therapy for HGAIN is also needed. Addressing the high rate of HPV-related disease should be an important component of preventive health care for all MSM, especially those who are infected with HIV.
Footnotes
Acknowledgements
The authors thank Chris Grasso, M.P.H. for extracting information from the electronic medical record. They also thank Erika D'agata, M.D., M.P.H., Linda Baldini, R.N., and Christopher Rowley, M.D., who provided guidance and critical review of the manuscript.