
Abstract
Although peripheral facial palsy is the most common cranial neuropathy in HIV-infected patients, no series have been reported recently in the literature. In this study we reviewed the clinical records of HIV-infected patients with a diagnosis of peripheral facial palsy between 2000 and 2011 attending the Hospital Marqués de Valdecilla (Infectious Diseases Unit), a 900-bed university hospital in northern Spain. We identified eight patients (4 men, 4 women): median CD4 count and viral load were 232 cells per μL and 130,000 RNA copies per mL, respectively. Most of them presented co-morbidities, including hepatitis C virus in 75%, hepatitis B virus in 15% and tuberculosis in 15%. Aetiologies of palsy were varied: idiopathic Bell's palsy predominated at early stages of the disease, whereas secondary causes, such as lymphoma and infections were frequently the cause of paralysis in advanced HIV/AIDS. At early stages of HIV infection, facial palsy is similar, both in aetiology and prognosis, to cases in the general population. However, in advanced stages the palsy is frequently secondary to underlying complications. Clinicians should be aware of these differences to tailor the diagnostic work-up.
INTRODUCTION
Neurological manifestations of HIV have been widely described in the literature. About 70% of HIV-infected patients develop neurological complications during the disease. Any level of the central or peripheral nervous systems can be affected, 1–3 including peripheral neuropathy, which represents 5–20% of all neurological complications; 4,5 in 1–4% a single cranial nerve is affected. 4
Peripheral type facial paralysis is a relatively common neuropathy in the general population, with most cases being idiopathic. A few small case series and several cases have been described in patients with HIV infection. Most of them include patients from countries in which AIDS has a high prevalence. 6,7 However, the clinical spectrum of facial paralysis in HIV-infected patients in western countries has not been clearly established. The aim of this study was to review the clinical characteristics of peripheral facial palsy in HIV patients in a University teaching Hospital in northern Spain in order to get further insight about its characteristics and consequently provide orientation for the diagnostic work-up.
PATIENTS AND METHODS
We reviewed the clinical records of HIV-infected patients with a diagnosis of peripheral facial palsy attending the Hospital Marqués de Valdecilla (Infectious Diseases Unit), a 900-bed university hospital attending a population of about 350,000 people in northern Spain.
Clinical data were extracted from the charts according to a standard protocol. Cases in which palsy was not well established (whether it was central or peripheral) were not included. We also excluded patients in whom facial palsy episode occurred before they were diagnosed of HIV infection.
We also reviewed the literature by searching Medline for papers published in English, Italian, French or Spanish by using different combinations of terms facial palsy, paralysis, AIDS, HIV or immunosuppression. Secondary references were also checked.
RESULTS
Characteristics of patients
HBV = hepatitis B virus; HCV = hepatitis C virus; cART = combination antiretroviral therapy
*Time in relation to HIV diagnosis
The CD4 count varied largely, between 27 and 895 cells/μL, with a median value of 232. The viral load also varied, from 50 to 1,658,094 RNA copies/mL (median 130,000 copies).
The aetiology of palsy was also varied. In three cases facial palsy was the first manifestation of a severe underlying disorder; lymphoma in two cases, and meningoencephalitis in another one. CD4 count varied from 27 to 107 cells/mL. All of them presented an adverse outcome.
The other five patients presented a Bell's (idiopathic) palsy. In these cases the median CD4 count was 256 cells/μL. All but one patient in this group experienced a good outcome after treatment with corticosteroids, with or without antiviral drugs.
DISCUSSION
The spectrum of the neurological manifestations of HIV has been widely described in the literature. Approximately 70% of the HIV-infected population will develop neurological complications during the disease. 2 Central nervous system (CNS) disorders are the most common complications, whereas peripheral neuropathies are less common. 4 Palsy of the facial nerve is the most frequent cranial neuropathy in HIV-infected patients and can occur at any stage of the disease. It has been suggested that prevalence of Bell's palsy is considerably higher in HIV-infected patients than in healthy people, at least in African countries with a high prevalence of HIV seropositivity. 8 In our series Bell's palsy was diagnosed in about 0.4% of patients attending the HIV clinic during a 10-year period. Peripheral type palsy is usually idiopathic (Bell's palsy) accounting approximately for 70% of all acute facial palsies. 9,10 Secondary causes of peripheral palsy, such as Ramsay Hunt Syndrome, otitis, trauma, tumour or sarcoidosis are less common and globally represent about 30% of cases. 11
From our case series, it seems that the spectrum of facial palsy includes two different groups. On the one hand, at early stages of the disease, when the immune response is relatively preserved, the causes of facial palsy are similar to those found in the general population, with a predominance of virally-related cases, such as Bell's palsy (3 patients), and Ramsay Hunt syndrome (1 patient). This syndrome has been occasionally reported in HIV patients. Goldani et al. 12 found six cases in a review of the literature up to 2008 and reported two additional cases. Most cases did not have advanced immunosuppression, and, as in our case, CD4 counts were above 200 cells/mm3. Prognosis of Ramsay Hunt syndrome appears to be somewhat worse that for Bell's palsy. 13
Drug treatment of Bell's palsy and Ramsay Hunt syndrome tries to accelerate recovery of palsy and prevent complications. Corticosteroids reduce the risk of unfavourable recovery and should be initiated as soon as possible. The role of antivirals is controversial and general measures (such as eye occlusion) are also important. All our patients except one received treatment with steroids, associated in one case with antiviral agents. Most patients experienced a good outcome, with palsy resolution in the following months. As in our patients, in an African study including 88 patients with peripheral facial palsy the presence of HIV infection was not associated with a worse prognosis. 14
Although antiretroviral therapy was indicated in four out five of our patient with Bell's palsy, only one of them was actually taking it at the onset of the paralysis. It is well known that combination antiretroviral therapy (cART) increases CD4 lymphocyte levels, improving the patient immunity. These observations are consistent with a protective effect of cART on facial palsy.
Although unilateral palsies are more frequent than the bilateral ones, most cases of facial palsy recently reported in the literature are bilateral. This may be the consequence of a publication bias towards reporting the rarest cases. There were no bilateral palsies among our patients, presenting only one of them a recurrent episode in the same side.
Contrary to cases in the early course of HIV disease, facial palsy in patients with marked immune depression has a much more varied aetiology, including severe disorders of the CNS, such as infections, lymphoma and other tumours. Four patients in our series showed a CD4 count less than 250 cells/μL. Contrary to the group of patients with higher CD4 count, they presented a more varied aetiology (Bell's palsy only represented 25% of cases) (Figure 1). Among them, CNS lymphoma appears to be particularly frequent. That was the case in two patients in our series, both with advanced immunosuppression, and in other reports.
15,16
Given the ominous prognosis of the patients with CNS lymphoma (both patients in our series died), an optimal adherence to cART seems to be the most important preventive/therapeutic measure.
Comparison of facial palsy aetiology depending on the CD4 cell count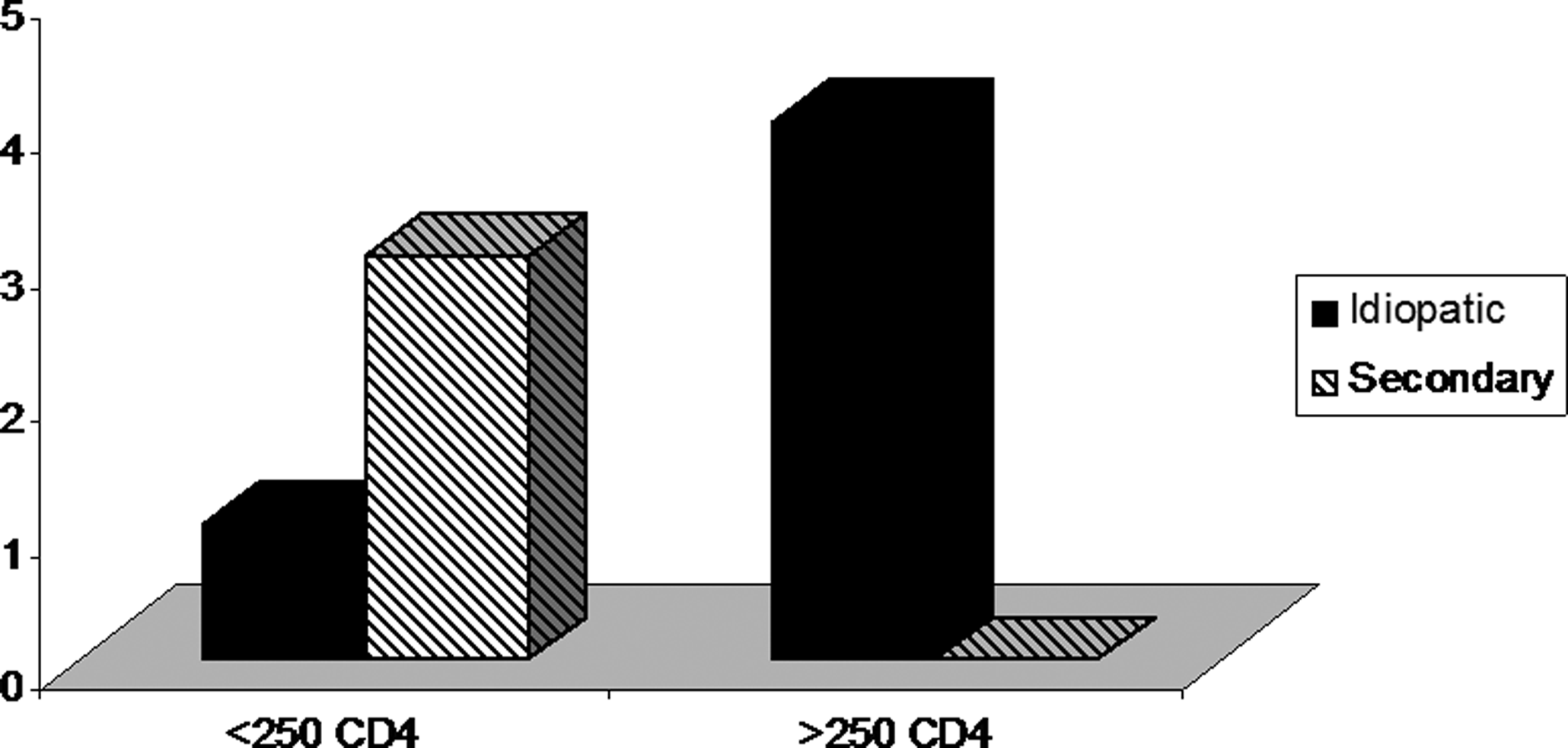
Apart from CD4 levels, different aetiologies of facial nerve palsy may be suspected on the basis of the location of facial pathway injury. Proximal palsies are usually related to more severe disorders, such as strokes, multiple sclerosis, sarcoidosis, lymphoma or aneurysms. In these cases other brainstem signs are usually present (ataxia, long tract abnormalities, limb weakness, etc.). On the other hand, distal palsies are not usually associated with major neurological symptoms. Therefore, in those patients in whom clinicians suspect a proximal lesion a more exhaustive search of the underlying cause is warranted.
In summary, and taking into account that we only described eight cases, the spectrum of peripheral facial palsy in HIV-infected patients appears to include two different sets. In patients at the early stages of HIV infection and relatively preserved immune response, the causes of facial palsy are similar to those in the general population, with most cases being virally-related (i.e. Bell's palsy, Ramsay Hunt syndrome). In these cases prognosis is similar to that in not infected patients. On the other hand, in patients who are severely immunosuppressed, a variety of aetiologies should be considered, including other infections and malignant disorders. Therefore, an extensive diagnostic work-up is justified in patients with low CD4 counts or with manifestations suggesting a proximal lesion. Optimal adherence to antiretroviral treatment should be emphasized in order to increase the probability to decrease the risk of facial palsy as well as other infectious and non-infectious complications of HIV infection.