
Abstract
Summary
In 2008, guidelines aimed at reducing undiagnosed HIV infection were published, recommending normalization of testing. Local initiatives were carried out in south-west London including an extensive primary care education programme. This study aimed to establish the impact of these initiatives on HIV diagnoses. Data on all new diagnoses referred to our centre were collected and analysed from patient records. A total of 394 patients were newly diagnosed with HIV from 2007 to 2011. Diagnosis in primary care and other non-sexual health (SH) settings increased by 184% during this period. There was an increase of 37% in the median CD4 count at diagnosis, taking the figure to 372 cells/mm3 in 2011. The proportion of patients presenting with a CD4 count of <200cells/mm3 decreased by 24%. The evidence suggests that these local initiatives were successful in increasing HIV diagnoses outside SH settings, particularly in very late presenters.
INTRODUCTION
The number of people in the UK currently living with HIV is estimated to be around 86,500 (∼0.1% of the population), although a quarter of these individuals are unaware of their infection. 1 A study in 2005 showed 25% of new diagnoses to be ‘very late’ presenters, with a CD4 count of <200 cells/mm3. 2 Data from the Health Protection Agency in 2010 suggest that late diagnosis (CD4 <350 cells/mm3 within 3 months of diagnosis) continues to remain a problem in the UK. The main barriers to early diagnosis include addressing the stigma attached to HIV and encouragement of testing wider populations, not simply those with a high clinical suspicion.
There have been a number of initiatives, supported by both medical and government agencies to encourage wider HIV testing. Prior to 2001, patients usually had to present to a Sexual Health (SH) clinic and request an HIV test. In 2001, the National Strategy for Sexual Health and HIV recommended all patients attending an SH clinic be offered HIV tests. Guidelines published in 2008 by the British Association of Sexual Health and HIV (BASHH), the British HIV Association (BHIVA) and the British Infection Society (BIS) recommend that medical professionals get informed consent for HIV testing in the same way as other investigations, without the need for pre-test counselling. It was also recommended that testing be a norm across all health-care settings to reduce stigma. 3
The National Institute for Clinical Excellence (NICE) also released guidelines in March 2011 to promote ways of increasing HIV testing in black Africans and in men having sex with men (MSM).4,5 Recommendations included advice on promoting HIV testing in these two groups and reducing barriers in these communities.
Despite this, many non-SH settings have not implemented testing programmes. For example, the Clinical Effectiveness Committee of The College of Emergency Medicine released a position statement in June 2011 stating that ‘HIV testing should only be performed in the emergency department when it influences clinical management and improves patient care’. 6 Additionally, it suggests that emergency departments are not suitable for ‘ad hoc’ screening, which goes against the 2008 guidelines of testing all in higher prevalence areas. 3 In addition, the British Society for Colposcopy and Cervical Pathology wrote to all its members in 2011 discouraging HIV screening in colposcopy clinics (Dr M Pakianathan, re. letter from the British Society for Colposcopy and Cervical Pathology to its members, personal communication). Further work is required to challenge attitudes if non-SH departments are going to further contribute to the reduction in the number of late diagnoses.
LOCAL INITIATIVES
Since the launch of the guidelines a number of initiatives have taken place by clinic staff at our centre to promote HIV testing in non-SH settings. One of these has been an extensive general practice education programme involving visits to 48 out of the 52 general practices in NHS Wandsworth, which is a geographical sector of SW London with a population of 294,564. This programme took place between January 2009 to June 2010, and raised the importance of HIV testing. In addition, in 2011, the Primary Care Trust 7 piloted HIV point of care testing for new general practice registrants; 48% of the 8146 patients offered accepted a HIV test, and 0.1% (4 patients) were unknown positives. Education programmes have also been incorporated into hospital teaching programmes with non-SH medical professionals and also in hospital ‘Grand Rounds’. The SH clinic also pioneered a teaching tool to raise HIV testing awareness outside SH medicine and in hospital settings. SWAGNET (south-west London HIV and GU clinical services network) developed a clinical indicator diseases tool kit for primary care clinicians across south-west London in 2009. 8 Additionally, in March 2011 NHS Wandsworth supported the emergency department at St George's Hospital undertaking a pilot study, routinely offering HIV testing to all patients having blood tests undertaken in the department; with plans to run a longer pilot in 2012.
This study describes changes of patterns in HIV diagnoses following recent guidelines and local interventions, in particular describing diagnosis by primary care and other non-SH settings, median CD4 count at diagnosis and proportion of patient presenting very late (CD4 count <200 cells/mm3).
In 2009, 51% of new diagnoses of HIV in London were late (CD4<350 mm3) and 29% were very late (CD4<200 mm3). 9 South-west London had the highest proportion of late diagnoses of HIV in London: 56% were late diagnoses and 34% were very late. 9
METHODS
Data on all new diagnoses referred to the HIV outpatient service, including ethno-demographics, place of diagnosis and baseline CD4 count, are entered prospectively into a database. Previously diagnosed patients having received HIV care elsewhere transferring into the service were excluded. Data from January 2007 to December 2011 were analysed. SH settings included genitourinary (GU) medicine clinics, and non-SH settings included accident and emergency (A+E), outpatient clinics, antenatal clinics, general practice and inpatients. Fisher's exact and unpaired t-tests were used for statistical analysis.
RESULTS
Percentage of patients in study separated by year and gender

SH = sexual health
Comparing the periods before (2007 and 2008) and after the transition year (2010 and 2011), there was a 108% increase in diagnosis of HIV in non-SH settings from 52 to 108 patients (P < 0.0001). This correlated with a total increase in HIV diagnosis (Figure 1).
Numbers of patients newly diagnosed with HIV presenting at either SH or non-SH settings between 2007 and 2011. SH = sexual health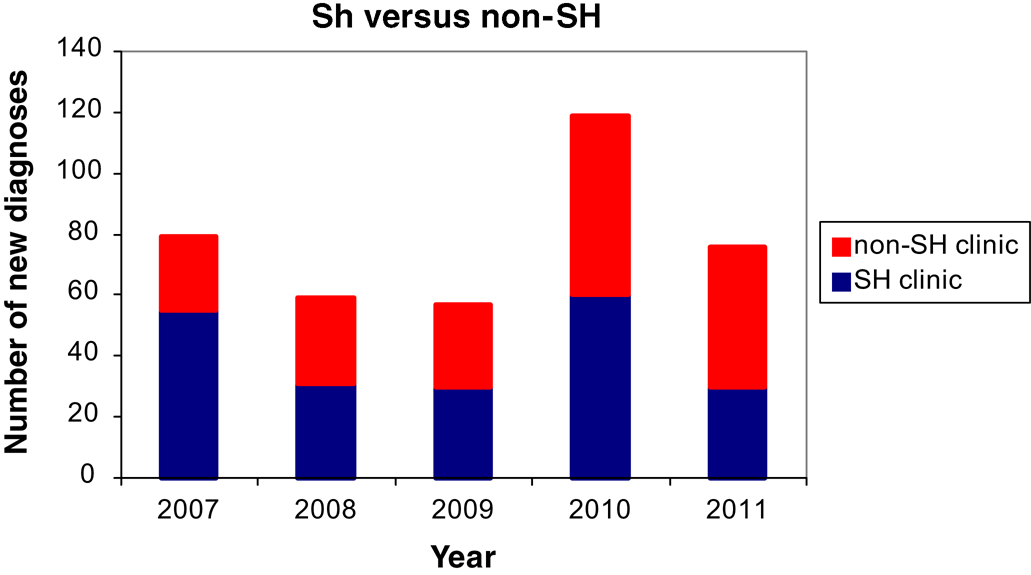
Overall black Africans were the most common ethnic group to be newly diagnosed with HIV (n = 155, % = 40). In non-SH clinics, the most common ethnicity in new diagnoses was black African/Caribbean n = 115 (% = 63). In SH clinics, the most common ethnicity in new diagnoses was white (n = 97, % = 47). The median age of the black African/Caribbean patients in non-SH clinics was 41 years, and 67% of this group were women. The median age of the white patients in SH clinics was 37 years. In total, 91% (n = 88) of this group were men and 70% (n = 68) were MSM.
The most common routes of exposure were heterosexual intercourse in those presenting to non-SH clinics and MSM sex in SH clinics. Comparison of the median cell counts before and after transition year showed an increase in the median CD4 count at diagnosis from 233 to 304 cells/mm3 (Figure 2), an increase of 30%. There was a corresponding reduction in the proportion of very late presenters (CD4 count <200 cells/mm3) from 2009.
Median CD4 count in newly diagnosed patients with HIV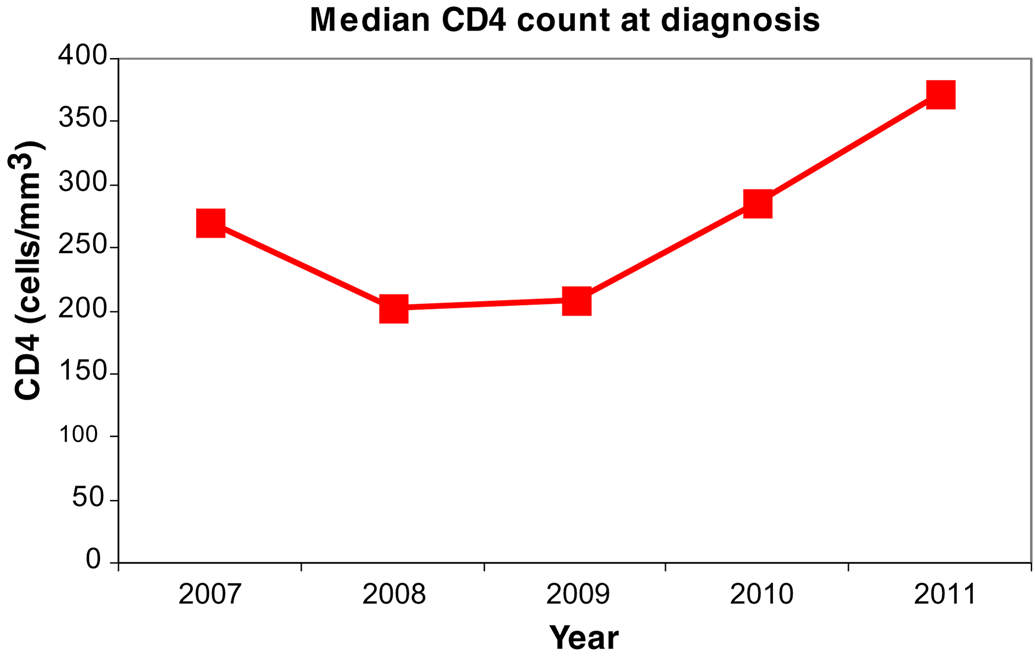
Comparison of the proportion of very late presenters (CD4 count <200 mm3) before and after transition year, 2007 and 2008 with 2010 and 2011, showed a decrease from 47% to 34% (P = 0.0295).
DISCUSSION
There was a significant increase of HIV diagnosis in non-SH settings after the transition year (2009) (see Figure 1). This suggests that with the use of local initiatives complementing the 2008 guidelines, non sexual-health-care professionals are testing for HIV.
Figure 1 shows a reduction in the number of diagnoses in 2011 both in SH and non-SH settings, as compared with 2010. This is unlikely to be connected to a reduction in onward transmission due to local initiatives and National guidelines as it is over too short a period.
The NICE guidelines suggest focus should be on increasing HIV testing in black Africans and MSM,4,5 and results here support that these two prevention groups are disproportionately affected by HIV locally. These data show that the majority of new HIV diagnoses in white individuals are in MSM (71%); and while heterosexual contact was the most common route of exposure, the majority of these patients (82%) were of black African, Caribbean or black Other.
SH clinics are perhaps generally viewed as more ‘friendly’ environments for MSM, due to their advertisement of confidentiality and their encouragement of regular attendance of MSM. This is suggested by the higher proportion of MSM with new diagnoses in SH clinics. Outside of SH clinics, black African (median age 41 years) women are more commonly diagnosed, as they may be less likely to visit an SH clinic. These women are likely to perceive themselves as low risk for sexually transmitted infections (STIs), yet are high risk for HIV because of country of origin or their partner's country of origin. Without HIV testing in non-SH settings, these patients risk being diagnosed with advanced HIV-related disease.
The median CD4 count at diagnosis increased from 2009 onwards, the year after the National guidelines were published. The CD4 count at diagnosis has continued to increase and has led to the median count in 2011 to be >350 cells/mm3, indicating that the majority of patients in that year were diagnosed ‘early’ (see Figure 2). Early diagnosis will contribute to a reduction in the morbidity and mortality associated with HIV and improves public health risk with reduced risk of onward transmission. Equally, the percentage of ‘very late’ diagnoses, with CD4 counts of <200 cells/mm3, has significantly decreased since 2009. Published data for London in 2009 showed Wandsworth to have a higher proportion of very late diagnoses than the general trend in London. 8 It is not possible to compare local trends in HIV diagnoses referred to our centre with the rest of London as the data for London are not yet published for the time period studied. It will be useful to compare our recent results with the rest of London when these results are published. Data were not collected from other hospitals and SH clinics, and so a comparison between Wandsworth and other neighbouring areas could not be undertaken.
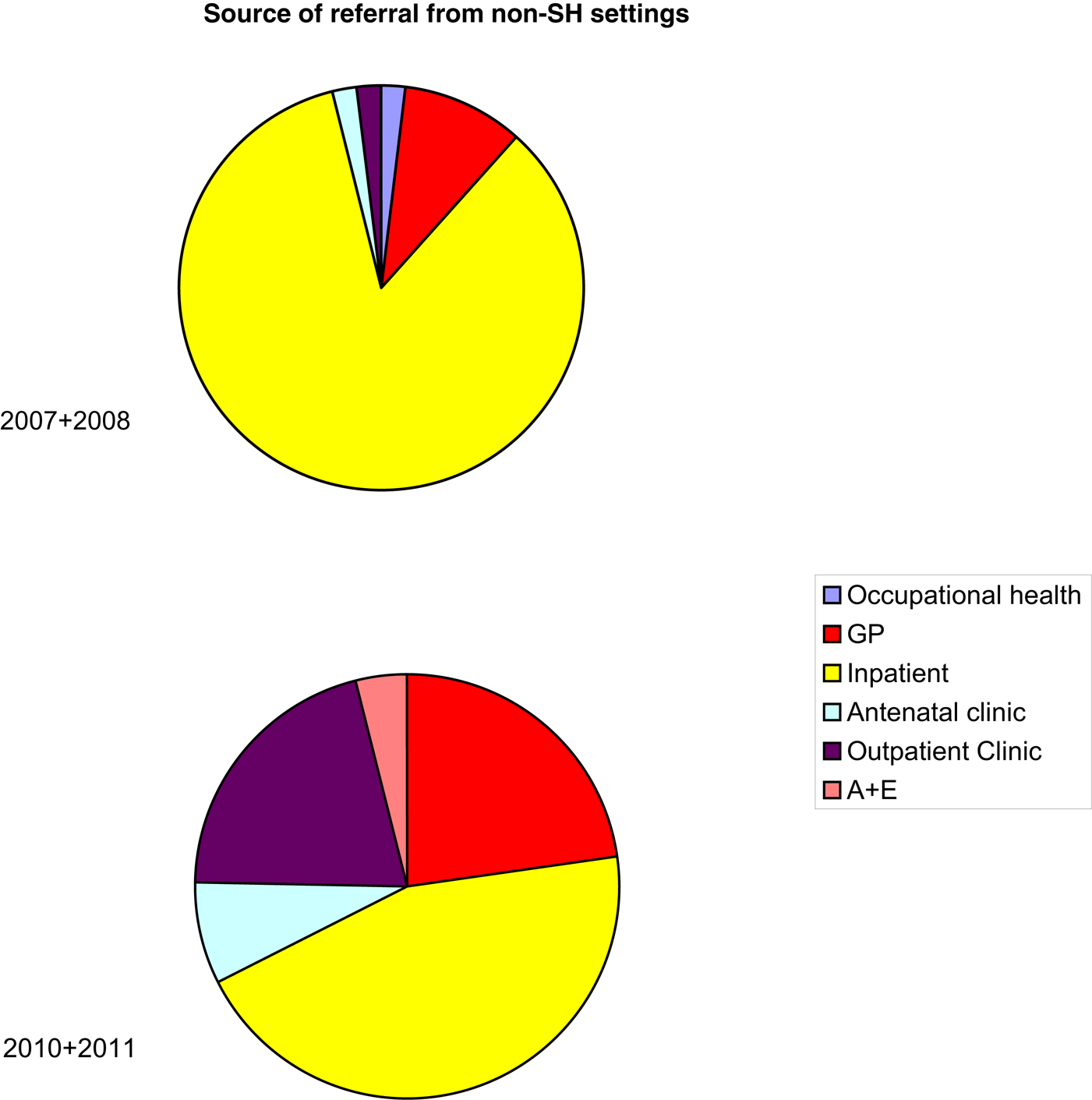
Although non-SH HIV diagnoses have increased in recent years, early diagnosis is still more likely to occur in SH clinics than in other settings (Figure 3). This is not surprising given that ambulatory, well, and often younger patients attend SH clinics where HIV testing is more routine. It is also not surprising that inpatient and hospital outpatient clinics diagnose patients with symptomatic disease when they attend. Diagnosis in primary care is the main non-SH setting where diagnosis levels have steadily increased (see Figure 4) this may be due to on-going initiatives. In the future, with continued and increased initiatives to encourage HIV testing the percentage of early diagnoses is anticipated to increase, resulting in the reduction of morbidity and mortality associated with HIV.
Proportion of patients with CD4 >350 cells/mm3 at time of diagnosis with HIV in SH settings compared with non-SH settings. SH = sexual health Pie chart showing the different sources of referral pre-transition year (2007+2008) and post-transition year (2010+2011) from non-SH settings. SH = sexual health; GP = general practice; A+E = accident and emergency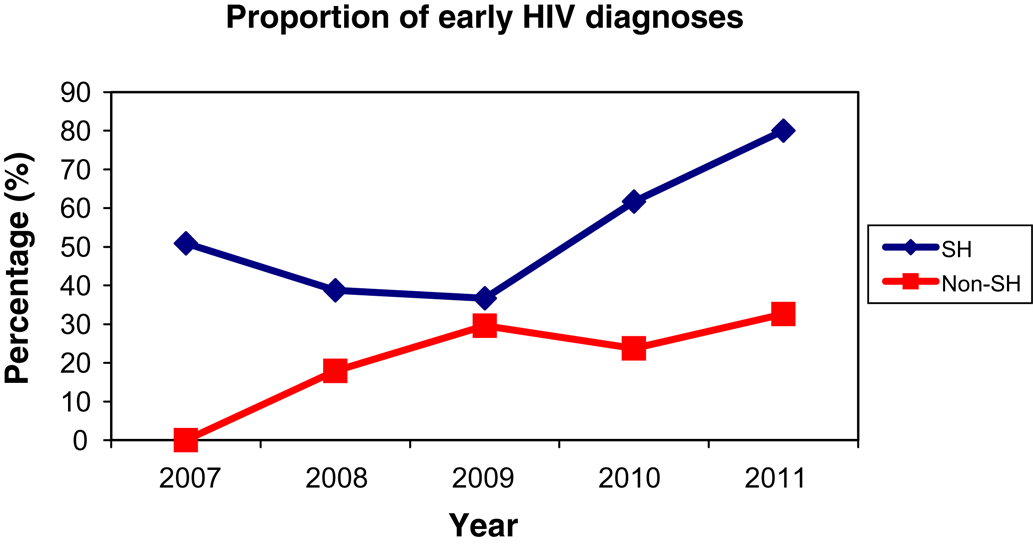
In the future, it is hoped with continued and increased initiatives to encourage HIV testing, the percentage of early diagnoses is anticipated to increase, resulting in the reduction of morbidity and mortality associated with HIV.
CONCLUSION
Results from this study demonstrate that there has been a significant improvement in earlier diagnosis of HIV and the diagnosis of HIV in non-SH settings. The median CD4 count has increased significantly since 2007–2008, suggesting people are being diagnosed earlier. The trend of the proportion of very late presenters is falling.
Despite the challenges of conflicting positions between the National HIV testing guidelines and some specialist societies (Dr M Pakianathan, re. letter from the British Society for Colposcopy and Cervical Pathology to its members, personal communication), 6 evidence suggests that local initiatives are successfully implementing National guidelines. If the momentum of the success is to continue, further work will need to be done to continue to engage, challenge and support initiatives for diagnosing HIV earlier.