
Abstract
Summary
This paper assesses the associations between intimate partner violence (IPV) and sexually transmitted infections (STIs) and sexual risks among HIV-positive female drinkers in St Petersburg, Russia. Survey and STI data were analysed from 285 women in HERMITAGE, a secondary prevention study of HIV-positive heavy drinkers. Logistic and Poisson regression analyses assessed associations of IPV with STI and risky sex. Most women (78%) experienced IPV and 19% were STI positive; 15% sold sex. IPV was not significantly associated with STI, but was with selling sex (adjusted odds ratio = 3.56, 95% confidence interval = 1.02–12.43). In conclusion, IPV is common and associated with sex trade involvement among Russian HIV-positive female drinkers.
Keywords
INTRODUCTION
Male partner-perpetrated intimate partner violence (IPV) and its association with sexually transmitted infection (STI) and STI/HIV risk taking behaviours (e.g. sex trade involvement) among women has been well described in multiple national contexts.1–12 IPV was associated with sex work or multiple sexual partners, prior STIs and lower condom use in Australia and the Ukraine. 1 Married women in India experiencing husband-perpetrated IPV were more likely to have HIV infection than those who did not experience IPV from their husbands. 4 Methadone-maintained women in New York with an increased risk for IPV had higher self-reported STIs. 5 Higher rates of IPV victimization were found among HIV-positive women compared with HIV-negative women in four sub-Saharan African countries.8–12 IPV is particularly pervasive in Russia, with approximately one-third of women reporting such victimization in their lifetime.12–15 Injection drug use (IDU) and alcohol use, higher in Russia than in other national contexts,13,16–20 have additionally been associated with increased risk for both HIV/STI21–24 and IPV.2,13,23 For example, in St Petersburg, alcohol misuse and certain drinking contexts (e.g. on the street) were associated with male IPV perpetration.13,25 In St Petersburg, IDU has been strongly associated with HIV/STIs. 26
Despite the extensive research on IPV and STI risks among women in cross-national settings including Russia, there has, to date, been no published research examining whether history of IPV is associated with increased risk for STI and related risky sexual behaviours among substance using HIV-positive women in Russia. As the epidemic in Russia increasingly includes cases of sexually transmitted HIV,20,23,25–27 research on sexual risk factors for HIV becomes more important. This study addresses this gap in the field by examining whether history of IPV increases risk for STI and related sexual risk behaviours among HIV-positive female drinkers in Russia. Specifically, we hypothesize that victims of IPV are more likely to have an incident sexually transmitted infection (STI) than those reporting no such history. Secondly, we hypothesize that victims of IPV are more likely to have increased sexual risk factors (selling sex, recent multiple sexual partners, a higher number of unprotected sexual encounters) than those who report no history of IPV victimization.
METHODS
Data for this study came from baseline female participants (N = 285) of the HERMITAGE (HIV Evolution in Russia – Mitigating Infection Transmission and Alcoholism in a Growing Epidemic) study, an HIV intervention study that enrolled HIV-positive heavy drinking adults from October 2007–April 2010 from five inpatient/outpatient HIV and substance use care sites in St Petersburg, Russia (see further details on methods elsewhere 28 ). Participants were at least 18 years old, Russian-fluent and HIV-positive; reported past six-month unprotected anal or vaginal sex; provided stable local addresses and a telephone number; and met criteria for NIAAA ‘at risk’ drinking levels in the prior six months. 29
In the overall study, 702 were screened and 483 were enrolled. Among the 27% who were screened but did not enter the study, the following exclusion criteria were involved. Those with unconfirmed HIV infection (n = 2), missing contact information (n = 40), attempting to get pregnant or have their partner get pregnant (n = 4), having a pending legal issue (n = 17), alcohol criteria not met (n = 110), sex criteria not met (n = 134), refusal to participate (n = 29) or too ill to participate (n = 1) were excluded. For those with contact information lacking, those living outside of 150 km of St. Petersburg (n = 2) or failing to provide contact info for two other people (n = 23), or without a telephone (n = 14) were excluded. In addition, any individuals with severe cognitive impairment or anticipated incarceration were excluded, but none met these criteria in the sample. Trained clinician research associates recruited participants, assessed their eligibility in private rooms and obtained written informed consent from those eligible and willing to participate. Participants were then surveyed via face-to-face interviews in Russian and participated in a self-administered questionnaire for particularly sensitive questions (e.g. trauma, IPV). Participants underwent STI testing by providing urine (gonorrhoea, Chlamydia, trichomoniasis) and blood (syphilis) samples. If they tested positive for gonorrhoea, Chlamydia, trichomoniasis, they were offered treatment, but they were referred to the STI clinic for syphilis. Participants received 300 rubles (US $7) for their baseline assessment participation. Procedures were approved by the Institutional Review Boards of Boston Medical Center and St Petersburg Pavlov State Medical University.
Measures
Single items assessed participants’ age, marital status and education. Depression was measured by using the Beck Depression Inventory II (BDI-II).30,31 Alcohol assessments asked about the quantity and frequency of alcohol consumption using a 30-day timeline follow-back (TLFB) instrument. Heavy drinking was defined as either reporting >7 drinks per week or any binge drinking (> 3 drinks in a day), in the past 30 days. 32 Drug use assessments included any use of heroin, prescription analgesics, marijuana, sedatives, tranquilizers or stimulants over the last year, and drug dependence according to the CIDI-SF. 33 Any past 30-day IDU was assessed using an item from the Risk Behavior Survey (RBS).34,35
Our primary independent variable, IPV victimization, was assessed via items based on the Conflict Tactics Scale-2 36 (Has a partner ever threatened you with violence, pushed or shoved you, or thrown something at you that could hurt? Have you ever had an injury, such as a sprain, bruise, or cut because of a fight with a partner? Has a partner ever insisted on or made you have sexual relations with him/her when you didn't want to?). A participant was classified as ‘yes’ for IPV victimization if a positive response was recorded. 36
The primary outcome, current STI, was assessed via urine testing for Neisseria gonorrhoeae, Chlamydia trachomatis and Trichomonas vaginalis and blood testing for syphilis (including confirmatory ELISA testing). Details on STI diagnostics are described elsewhere. 28 A secondary outcome, STI ever, was assessed via self-report on survey items asking whether the participant in their lifetime had ever had syphilis, gonorrhoea, Chlamydia and trichomonas.
Additional secondary outcomes included sex risk behaviour variables which asked participants about their sexual episodes and number of unprotected sex encounters (inconsistent condom use) in the past three months. 37 They were asked about alcohol and drug use before sex in the past 30 days (for their last 5 partners in the past 3 months). Two sex trade involvement items from the Risk Assessment Battery (RAB) 38 measured how often in the past three months the participant ‘had sex so they could get drugs’, and ‘were paid money to have sex with someone’.
Data analysis
Descriptive statistics were obtained for demographics, STI, sex risk behaviours and substance use behaviours for the overall sample and stratified by IPV victimization status. Bivariate associations were assessed via chi-square tests, t-tests or the non-parametric Wilcoxon rank sum test as appropriate.
Simple and multiple logistic regression analyses were used to assess the association between IPV victimization and the primary outcome, STI. Separate analyses were performed to assess each of the secondary outcomes, multiple sex partners and selling sex, reporting odds ratios (OR), and crude and adjusted over-dispersed Poisson regression analyses reporting incidence rate ratios (IRR) for the number of unprotected sex episodes. All adjusted analyses controlled for demographics (age, marital status and education), IDU, heavy alcohol use and depressive symptoms. Adjustments were not made for multiple comparisons due to the exploratory nature of the study. All analyses used two-sided tests and a significance level of 0.05. All statistical analyses were conducted using SAS version 9.3 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Sample characteristics
Demographic and HIV/STI risk profile of female HIV-infected heavy drinkers in St Petersburg, Russia (N = 285) and stratified by history of IPV victimization

STI = sexually transmitted infection; IPV = intimate partner violence; SD = standard deviation; IDU = injection drug use; IQR = interquartile range
Over three-quarters of participants (78%, N = 222) reported a history of IPV victimization (Table 1). Bivariate analyses suggested that participants reporting a history of IPV victimization were significantly more likely to report multiple sexual partners (P = 0.02) and selling sex (P = 0.01). Also, it is worth noting that albeit not statistically significant, participants reporting a history of IPV victimization appeared more likely to report any history of STI (P = 0.10).
Associations between IPV and STI
Logistic and Poisson regression analyses assessing associations between IPV victimization and the outcomes – STI and sex risk behaviours
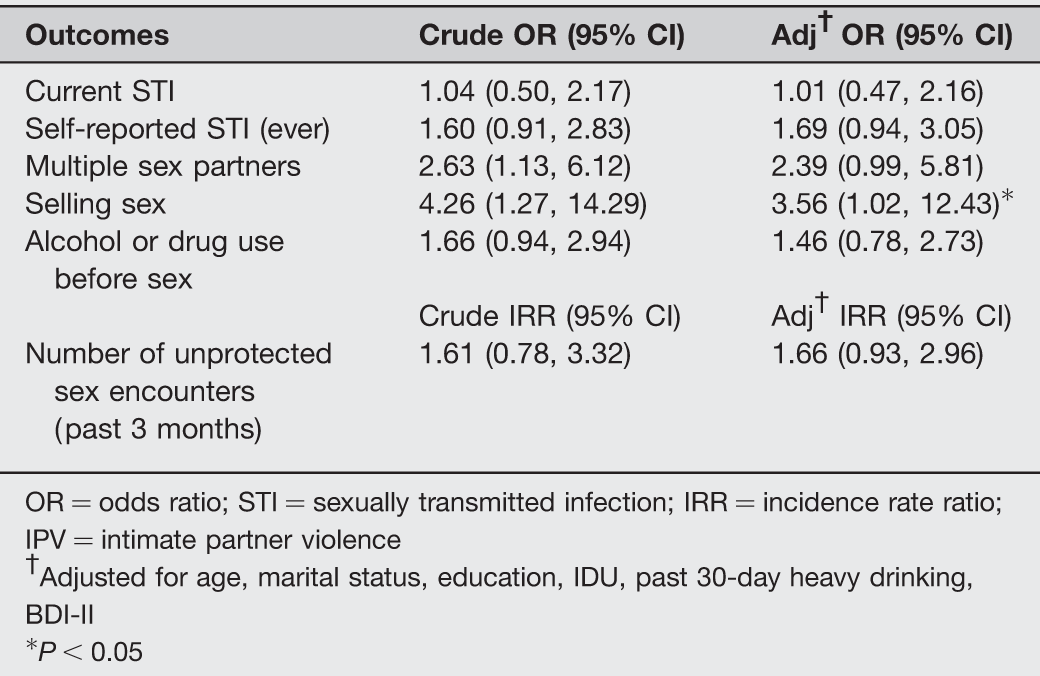
OR = odds ratio; STI = sexually transmitted infection; IRR = incidence rate ratio; IPV = intimate partner violence
†Adjusted for age, marital status, education, IDU, past 30-day heavy drinking, BDI-II
*P < 0.05
Associations between IPV and sex risk behaviours
The multivariable analyses demonstrated that lifetime IPV victimization was associated with higher odds of having the secondary outcome of selling sex (AOR = 3.56, 95% CI = 1.02, 12.43) (Table 2). Among the covariates, past 30-day IDU was positively associated with selling sex (AOR = 3.44, 95% CI = 1.57, 7.55) while being married or living with a partner was negatively associated with it (AOR = 0.38; 95% CI = 0.17, 0.87). Self-report STI ever was not significantly associated with IPV victimization (AOR = 1.69; 95% CI = 0.94, 3.05). No significant associations between lifetime IPV victimization and other secondary outcomes of sex risk behaviours were observed in adjusted analyses (Table 2). However, although not statistically significant, notable effect sizes were observed for each of the other sexual risk behaviours: having multiple sex partners (2.39; 95% CI = 0.99–5.81), alcohol and drug use before sex (1.46; 95% CI = 0.78, 2.73) and the number of unprotected sex encounters (1.66; 95% CI = 0.93, 2.96).
DISCUSSION
History of IPV victimization is common among female HIV-positive Russian heavy drinkers and is significantly associated with increased risk for sex trade involvement, but not having a current STI. The apparent lack of an association between history of IPV and current STI is surprising given the extensive evidence of this association previously found in non-infected but at risk women in Russia 39 and HIV-positive women in other national contexts;4,40,41 this may be attributable to use of different timeframes for these variables of focus and possibly a lack of study power. Nonetheless, findings of heightened risk for IPV among those engaged in sex work is consistent with previous research across national contexts,42–45 including Russia. 39 Research suggests that IPV increases risk for entry into sex work, 46 but also is more likely to occur in the context of sex work and with regular paying and non-paying partners. 47 These findings support ongoing work documenting the synergistic effects of violence against women, substance use and sex work involvement, which appears to be present among HIV-positive women. Such a phenomenon has been well documented in other women who use drugs or engage in sex work in Africa, Southeast Asia, Canada, Mexico and the USA,48–52 and effective interventions for women have been developed that simultaneously address these synergistic health concerns. 53 The findings in this paper emphasize the need to consider the long term and synergistic effects of IPV and substance use and sex work involvement among women living with HIV.
Recent sex work involvement was reported by more than one in seven of the HIV-positive women in this study, demonstrating that further exploration of sexual risk (e.g. unprotected sex) may be required for this population. In addition to the observed association between IPV and recent sex work involvement, recent IDU was also associated with greater involvement in sex work. Again, this association between sex work and IDU has been well documented,54–56 and other studies from Russia have demonstrated a significant association between IPV and IDU.45,57,58 Furthermore, women may experience IPV as a result of stigma from their HIV-positive status, having multiple partners or from their involvement in sex work.59–61 Current findings support the potential utility of targeting violence prevention interventions towards HIV-positive substance using women in Russia, especially those engaged in sex work. The notable prevalence of IPV victimization in this HIV-positive sample (78%) is higher than that seen in other populations of women in Russia, including those recruited from STI clinics.13,19,62,63 These findings of IPV being more common among HIV-positive women have also been seen in South Africa and Bangladesh.64,65 However, previous research from Russia and elsewhere also documents a strong association between substance use and IPV victimization;13,19,63 hence, high prevalence of IPV findings may also be attributable to this study's focus on heavy drinkers and inclusion of a large proportion of injection drug users.
The sample of heavy drinkers, many of whom also reported recent injection drug use, may use substances as a means to cope with trauma acquired during past experiences of IPV or current engagement in sex work.66,67 The high percentage of women who report either moderate or severe depression also supports the potential that women may self-medicate using alcohol or injection drugs. Findings from this study should be considered in light of study limitations. Most participants’ characteristics were based on self-reported data; as such, the data used are subject to recall and social desirability biases. Attempts to mitigate this risk included using trained assessors and self-completed portions of the assessment for particularly sensitive data. As noted previously, use of differing time frames across some of our variables of interest (e.g. lifetime IPV sexual victimization, unprotected sex in past three months, current STI) may have affected some study findings. Cross-sectional data analyses do not allow an interpretation of the findings in terms of causality. Findings of this study should also be interpreted with caution because the study cannot be generalized beyond HIV-positive individuals, women and those identified as ‘at risk’ drinkers. However, the findings contribute to understanding the associations of IPV with an important population in Russia, HIV-positive female drinkers. Of note, this sample was largely comprised of those who were in clinical care, limiting generalizability to HIV-positive Russian female drinkers who do not obtain health care. Furthermore, we did not collect data on income or employment that distinguishes between sex work and non-sex work employment. This is as an area that requires further exploration in future research because of the potential significance of HIV-positive women's economic and financial needs on the associations between IPV, substance use and sexual risk for this population.
Nonetheless, findings from this work support previous research from Russia and elsewhere, highlighting the synergistic relationship among gender based violence, substance use and sex work involvement in heightening risk for HIV and HIV transmission among women.48,50,68–70 Secondary HIV prevention efforts must consider the effects of IPV on likelihood of ongoing sex trade involvement for substance using HIV-infected women in Russia.
Footnotes
ACKNOWLEDGEMENTS
The authors wish to acknowledge the participants in the HERMITAGE study, as well as the clinical and administrative study staff, and the Data Coordinating Center at Boston University. Support for this work came from the National Institutes of Health R01AA016059, K24-AA015674, U24AA020778, U24AA020779 and T32 DA023356.