
Abstract
Summary
The European Collaborative Clinical Group (ECCG) was inaugurated at the 26th International Union against Sexually Transmitted Infections (IUSTI) Congress in Riga, Latvia 2011. The ECCG is a network of over 100 sexually transmitted infection specialists who have come together to conduct questionnaire-based research across the European region. It is expected that this work will focus and direct guideline development. A central core group of the ECCG has also been established who are responsible for identifying suitable survey questions that will be carried out but only after approval by the full ECCG Board. The ECCG aims to conduct a maximum of two projects per year which will be presented at the annual regional congresses and published as appropriate.
Keywords
INTRODUCTION
Gonorrhoea infection rates across Europe have generally remained relatively stable and near historic lows, especially when discounting the widescale adoption of nucleic acid amplification testing (NAAT) protocols that have generated increased detection. 1 Resistance testing of clinical isolates is currently being carefully monitored through a number of laboratory initiatives. Such work has shown that the number of options for treating gonorrhoea infection is becoming limited and clinicians can no longer rely upon an oral regimen to achieve cure. 2,3 The minimum inhibitory concentrations (MICs) for third generation cephalosporins are rising and the recent reports of four patients failing ceftriaxone therapy in Europe, including one genital infection exhibiting resistance to high-dose ceftriaxone, 4 may soon mark the end of empirical single-drug outpatient therapy. The ECCG felt that an urgent review of the clinical management of gonorrhoea is necessary to determine whether clinicians have adapted their prescribing practice in light of the changing resistance data.
The ECCG 2012 project looks at the clinical management of gonorrhoea, its clinical diagnosis and first-line treatment choices for confirmed or suspected infections. The project determines whether clinicians provide single-dose therapies, the range and doses of antibiotics used and whether tests to confirm resistance profiles and cure are arranged routinely. This builds on recently reported laboratory-based studies.
METHOD
The survey was developed by the members of the ECCG core group. In developing the survey account was taken of the recent published review of laboratory facilities across Europe for the detection of Neisseria gonorrhoeae.
5
The core group was interested in looking at the clinical management of gonococcal infections and the extent to which laboratory services supported care. The survey was developed to look at the following areas:
Access to nucleic acid testing; Access to culture facilities; Access to culture resistance profiling; Choice of mucosal sites and multiple testing using different modalities in heterosexual and homosexual patients; Choice of antibiotics for definite and suspected gonococcal infection; Use of combination antibiotic regimens in the management of gonococcal infection; Role of co-administered chlamydial therapy; Management of mild and severe allergy history in relation to antibiotic choice; Planning of tests of cure and their timing; Partner notification strategies and guideline choice.
Data were also collected on the type and nature of the respondents' practice. The full ECCG survey is available at
RESULTS
ECCG regions
The population coverage from the participating 30 ECCG countries totals 746.4 million representing 90% of the European population (Figure 1). Respondents were principally in urban (79%) and government (63%) practice and worked in large clinics, defined by a population coverage >250,000 (84%). Additionally 95% were clinicians involved directly in patient care in some capacity. Other roles included public health, laboratory sciences and research.
All participants who identified themselves as either not managing gonorrhoea or as non-clinicians (12) were excluded from the analysis of the clinical parts of the survey.
Access to laboratory facilities
Only one clinician reported that they did not have access to laboratory facilities to confirm gonococcal infections. The ECCG had three responses from this clinician's country with the remaining respondents reporting the availability of confirmatory testing. Interestingly this clinician was only using high-dose ceftriaxone (500 mg) for the management of actual and suspected gonorrhoea in homosexual patients. Some heterosexual patients may have therefore been at risk of under treatment in this centre.
Access to microscopy
The majority of participants (94%) had access to microscopy for the immediate diagnosis of gonorrhoea. The 6% who do not have access to microscopy represents four countries, three of which responded with mixed availability and only one reported no microscopy facilities.
Access to culture facilities
Only 5% of clinicians do not have access to culture facilities. This represents four countries, three of which responded with mixed availability of culture and only one reported no culture facilities.
Resistance profiling of culture isolates
Of the 95% of clinicians with access to gonorrhoea culture facilities, 13% do not have access to resistance profiling on routine gonococcal culture isolates.
Gonococcal screening in low-risk heterosexuals
Despite having access to laboratory confirmation facilities, 19% of clinicians chose not to offer gonococcal screening in low-risk populations.
Sites of testing in asymptomatic men who have sex with men
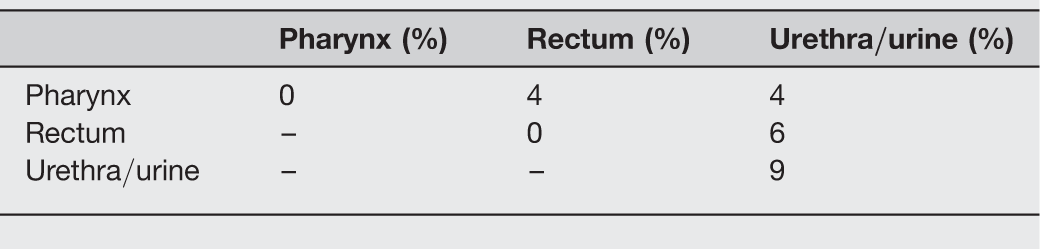
Only 65% of clinicians perform three site-testing in men who have sex with men (MSM). Both the pharynx and rectum are important sites of potentially difficult-to-treat gonococcal infection yet testing of these sites was far from universal. Most guidelines advise three separate specimens to be analysed independently.
5
Only 12% of clinicians chose not to perform any testing in this scenario. There was no correlation with the absence of three-site testing and whether clinicians work in the private sector (Table 1).
ECCG regions and participants Single and two-site testing in asymptomatic men who have sex with men (MSM)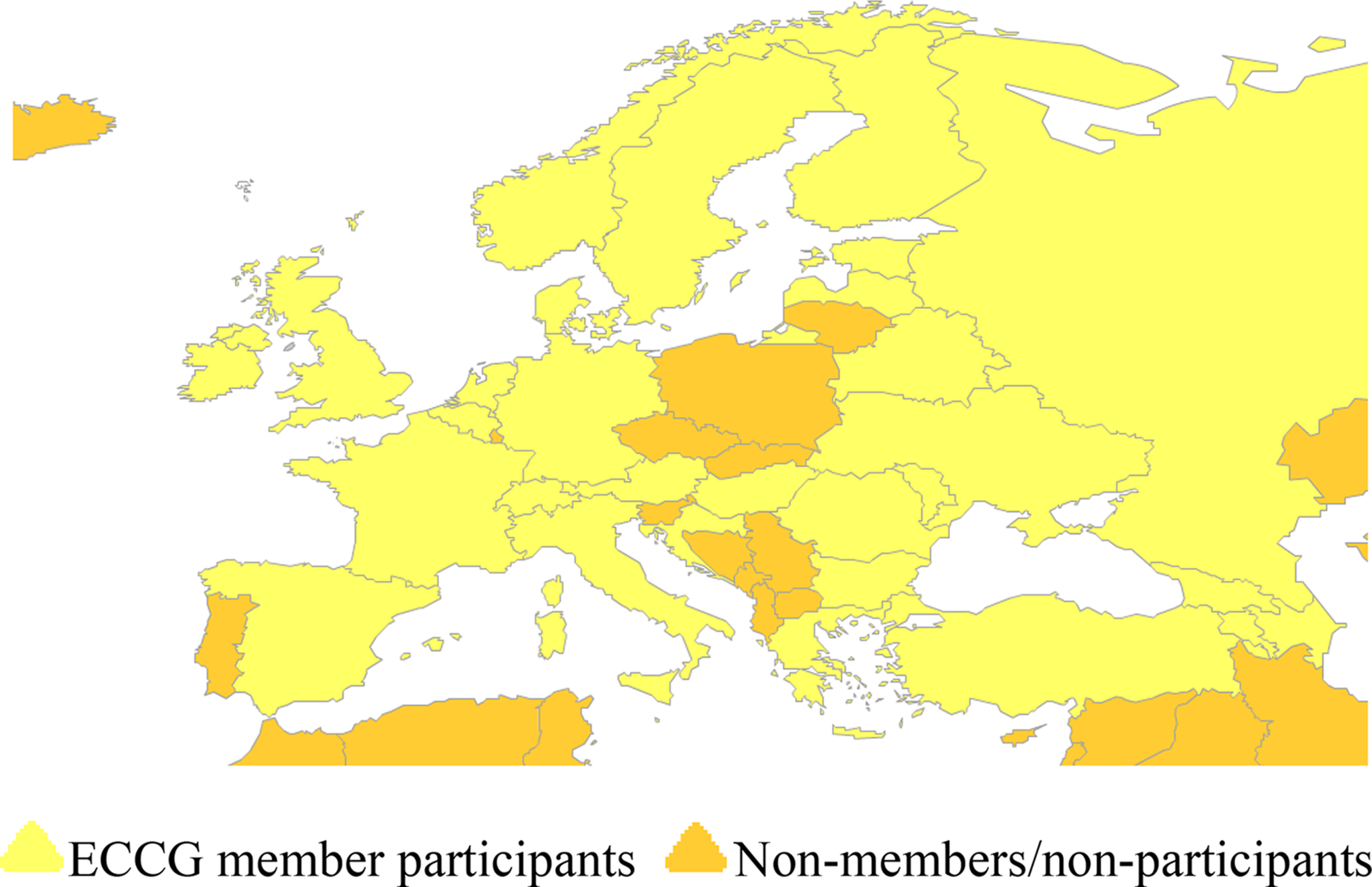
Access to NAAT
NAAT has the potential to increase the detection of gonorrhoea. It is concerning that 14% of the European population have no access to NAAT and an additional 25% have only limited access to NAAT.
Types of NAAT
In-house testing was reported by clinicians in eight ECCG countries (all clinicians in Russia, Hungary and Norway reported the use of in-house testing).
Pharyngeal and rectal site screening of asymptomatic heterosexual men and women
Currently guidelines do not advise universal extended testing in this situation but for this scenario there appears to be an element of over-testing. A minority of clinicians (5–8%) indicated that they would take rectal and pharyngeal swabs. There was no correlation with over-testing and private practice.
First-line antibiotic treatment for definite gonococcal infection
The majority of clinicians use high dose ceftriaxone at a dose of 500 mg. Most clinicians add azithromycin 1 g (49%) although some have not adopted this strategy. Eight clinicians chose to use azithromycin at a higher dose of 2 g and two clinicians chose azithromycin 1.5 g. A range of potentially suboptimal therapies are used and many of these are given as single antibiotics. One area of particular concern is the use of cefixime either with or without a second antibiotic. Resistance to cefixime is now widely described and oral therapy with this agent is not recommended by a number of authorities. 6 The presence of such prescribing may be a matter of some urgent concern.
We specifically collected data on additional therapies that would be given for possible coexisting chlamydial infection. Azithromycin or doxycycline were added 60% of the time as either part of or in addition to the regimen for the treatment of gonorrhoea. Forty percent of clinicians would not give any therapy that would cover a chlamydial infection in patients with gonorrhoea.
Treatment of asymptomatic female contacts of gonococcal infection
Fourteen percent of clinicians chose not to treat asymptomatic female partners of men with gonorrhoea. This is a surprising result. When treated, contacts of gonorrhoea appear to be treated with a similar choice of antibiotic and co-therapy for chlamydia compared with that given to definite gonorrhoea cases. Of those who chose not to treat asymptomatic partners, 90% have access to NAAT and 80% perform three site testing.
Site and type of testing in symptomatic MSM with microscopic evidence of Gram-negative diplococci
Single and two-site testing with culture in symptomatic MSM with microscopic evidence of gonococcus

MSM = men who have sex with men
Single and two-site testing with NAATs in symptomatic MSM with microscopic evidence of gonococcus
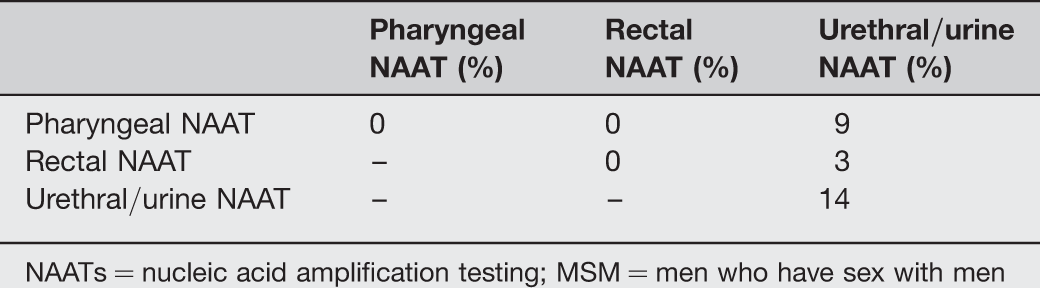
NAATs = nucleic acid amplification testing; MSM = men who have sex with men
Treatment in symptomatic MSM with probable gonorrhoea
Treatment choice in homosexual men is similar to that for heterosexuals. Interestingly some clinicians continue to use regimens which have a higher failure rate in non-genital infections. Co-therapy for possible coexisting chlamydial infection is given less consistently in MSM (69%) than for heterosexuals (80%).
Treatment in patients with a history of mild allergy to penicillin
Current guidance states that any third generation cephalosporin may be used in patients with a previous rash to penicillin. However there is a marked reduction (59%) in the number of clinicians choosing to use cephalosporins compared with previous scenarios (96–99%).
Treatment in patients with a history of anaphylaxis to penicillin
Guidance advises that cephalosporins be avoided in patients with a documented history of anaphylaxis to penicillin unless patients are first desensitized. Interestingly, there is a marked reduction in the choice of third generation cephalosporins (ceftriaxone, cefixime and cefotaxime) with only 15% of clinicians choosing this option, while there is an increase in the use of antibiotics with lower efficacy against gonococcal infections. Additionally more clinicians chose to co-administer azithromycin.
Tests of cure following treatment for definite infection
Surprisingly 26% of clinicians reported that they do not perform tests of cure following treatment, although only 16% chose to perform three-site testing. Additionally one clinician reported that they use microscopy alone to check for cure yet had already reported having access to culture and NAAT facilities.
Contact tracing – look-back period
Only one clinician did not perform contact tracing. Three months was the most frequent look-back period chosen by clinicians. There was no correlation with the length of contact tracing and private practice.
Choice of guidance
IUSTI guidelines are well used but most clinicians still use their own local national/regional guidelines.
CONCLUSION
There is considerable variability surrounding the clinical diagnosis and management of gonococcal infections by IUSTI experts across Europe. Some of this variation is of concern since antibiotic choices among many clinicians may do little to delay the development of further gonococcal resistance or may even fail to provide cure among patients with current infection.
Recommendations
Our survey found many examples of excellent and up-to-date care. Clinicians are often using the best available treatment strategies and providing therapy which will provide guaranteed treatment and delay the onward march of resistant infection. However, this was not universal and those involved in postgraduate training, continued professional development and guideline development should consider further developing, disseminating and justifying clinical standards around the following:
Guidance regarding mucosal site testing; Guidance regarding antibiotic choice; Guidance regarding antibiotic choice with allergy history; Guidance regarding tests of cure; Guidance regarding the duration of contact tracing; Clarification should also be provided as to the circumstances in which gonococcal testing can be omitted and whether epidemiological or presumptive therapy is needed if there is full access to multiple site NAAT.
Footnotes
ACKNOWLEDGEMENTS
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.