
Abstract
Summary
This study critically examines serological survey data for HIV infection in selected populations in Bali, Indonesia. Sero-survey data reported by the Bali Health Office between 2000 and 2010 were collated, and provincial health staff were interviewed to gain a detailed understanding of survey methods. Analysis of time series restricted to districts that have used the same sampling methods and sites each year indicates that there has been a steady decline in HIV prevalence among prisoners, from 18.7% in 2000 to 4.3% in 2010. In contrast, HIV prevalence among women engaged in sex work increased sharply: from 0.62% in 2000 to 20.2% in 2010 (brothel based), and from 0% in 2000 to 7.2% in 2010 (non-brothel based). The highest prevalence was recorded among people who injected drugs. Recent surveys of gay men and transvestites also found high prevalences, at 18.7% and 40.9%, respectively. Review of the methodology used in the surveys identified inconsistencies in the sampling technique, sample numbers and sites over time, and incomplete recording of individual information about survey participants. Attention to methodological aspects and incorporation of additional information on behavioural factors will ensure that the surveillance system is in the best position to support prevention activities.
BACKGROUND
The epidemic of HIV infection is recognized as a major public health threat in Indonesia. Even though the estimated national HIV prevalence is relatively low, at 0.3% in 2011, the epidemic is highly diverse, with considerable variation by geographic area. 1 While spread of infection was initially high among people who inject drugs, sexual transmission has come to represent an increasing proportion of cases detected. 2 Among the 33 Indonesian provinces, Bali has been one of the more heavily affected, ranking fifth according to the absolute number of reported diagnoses of infection over the past 10 years and second on a per capita basis, with a substantial increase in the number of diagnoses reported each year over this period. 3
Recognising the limitations of HIV case reporting as a means of public health surveillance, the Provincial Heath Office in Bali has, since 2000, conducted serological surveys in populations considered to be at higher risk for HIV infection. These surveys have become the primary source of data for tracking trends in the HIV epidemic in Bali, and results have been made available on a regular basis in provincial and national surveillance reports. The surveys have provided a general indication that HIV prevalence is increasing in some populations, particularly women involved in sex work. 4 However, the data from the surveys have generally been published only as annual, province-wide prevalences, by broad population group. Furthermore, the surveillance data have not been subject to more detailed analyses that might provide insight into their validity, nor has there been an assessment of the extent to which observed trends and patterns may be due to changes in sampling frames. We therefore conducted a study that aimed to fill these gaps and have exposed the findings to the scrutiny of peer-reviewed publication.
METHODS
We obtained copies of archival records and reports of HIV serological surveys from the Bali Provincial Health Office (BHO). As the reports did not contain comprehensive descriptions of survey procedures, we obtained further information on procedures from interviews undertaken by the first author (PPJ) with staff from BHO who had been involved in the surveys. The following summary of procedures is based on both the reports and the interviews. HIV surveys were carried out by staff from BHO using the ‘unlinked anonymous’ method. Potential survey participants were approached and their verbal informed consent sought for drawing blood to submit to serological testing for hepatitis B and syphilis. Verbal informed consent was used because, for many women involved in sex work in Bali, signing forms could be perceived as threatening. Blood specimens from those who consented were then divided into two aliquots. One portion was used for the hepatitis B and syphilis testing, and participants who were found to have syphilis were advised to attend a clinic for treatment if needed. The other portion was tested for HIV antibodies separate from all identifiers to ensure that there was no possibility of associating the results with specific individuals. According to BHO staff, the unlinked anonymous strategy was adopted because it was believed to be consistent with World Health Organization recommendations for HIV surveillance, and because BHO assumed that many people would refuse to participate in the surveys if their primary purpose was presented as HIV testing, even if unlinked. For the purposes of this paper, we reviewed only the results of the HIV testing.
Annual sero-surveys for HIV in Bali: recruitment strategies by population group
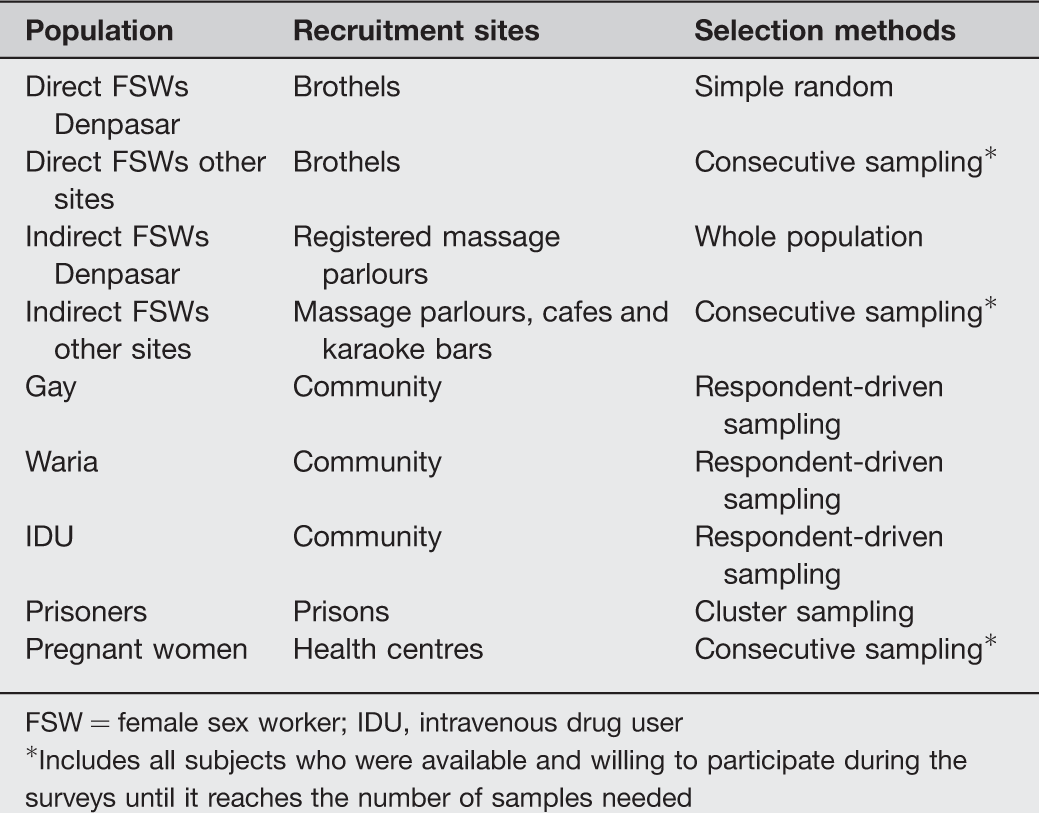
FSW = female sex worker; IDU, intravenous drug user
*Includes all subjects who were available and willing to participate during the surveys until it reaches the number of samples needed
We then used the criteria for second-generation HIV surveillance developed by the WHO/UNAIDS Working Group on Global HIV/AIDS and STI Surveillance to assess whether the surveillance data could be used to evaluate trends over time. 6 The criteria included consideration of the frequency of data collection, the appropriateness of the population being surveyed, the consistency over time of the surveillance sites and groups and the coverage of the groups under surveillance.6,7 Data obtained through procedures that met the criteria were then analysed to determine HIV prevalence and analyse time trends among subgroups by geographic location. We used statistical tests for trends in proportions to assess the trends by year.
The Institutional Review Board of the Kerti Praja Foundation (YKP), which provides HIV prevention and clinical services to people at risk of HIV in Denpasar, Bali, provided ethical approval for this study. The Bali Health Office gave permission to access, analyse and publish results of the surveys and to conduct interviews with its surveillance staff.
RESULTS
Based on internal BHO records, serological surveys were conducted in all nine of Bali's districts in the period 2000–2012. Information retained in the Health Office was in tabular form, with numbers tested and numbers found positive recorded by year, district and population subgroup. Line records of individuals tested were not available, and there was no information on age or any other characteristics of participants.
Annual sero-surveys in Bali: numbers tested by population group (2000–2010)
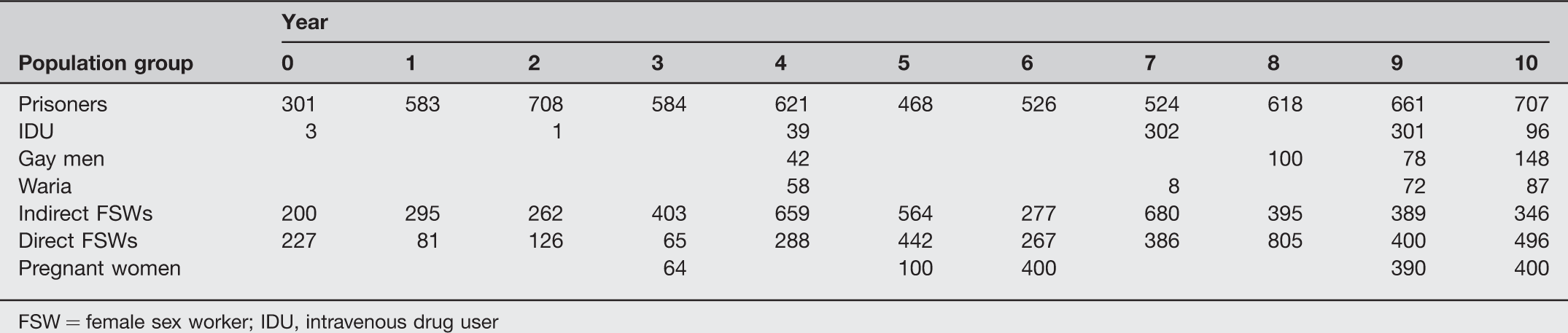
FSW = female sex worker; IDU, intravenous drug user
Annual sero-surveys in Bali: numbers tested by population group, district and year (2000–2010)*
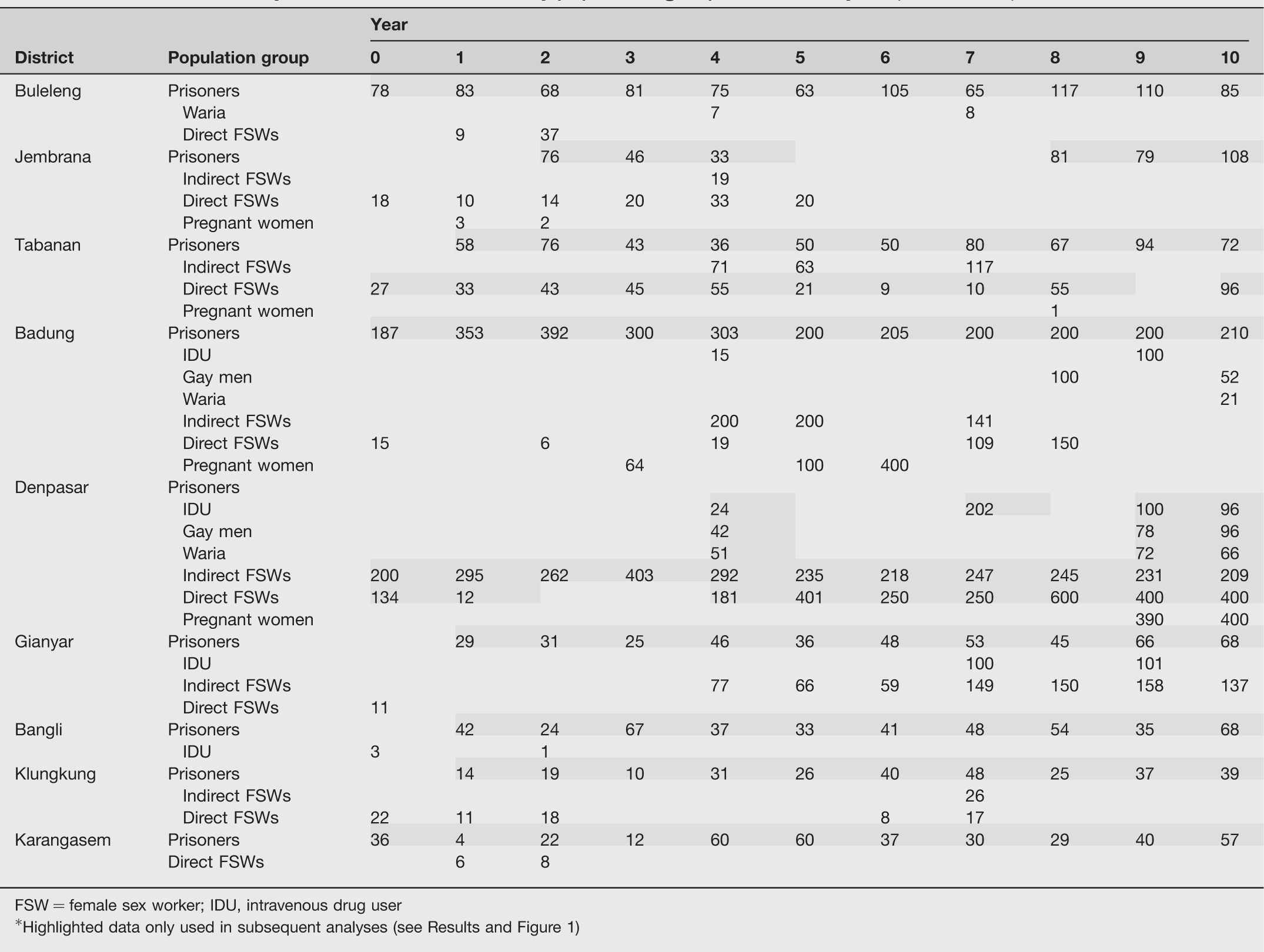
FSW = female sex worker; IDU, intravenous drug user
*Highlighted data only used in subsequent analyses (see Results and Figure 1)

HIV prevalence among selected population groups, for Denpasar (2009–2010) and for districts in which there was a consistently collected annual series
Repeated annual surveys that covered most or all of the study period with a reasonable annual sample size and that hence could provide information on time trends were available for only female sex workers, prisoners and, to a lesser extent, people who injected drugs. The BHO reports demonstrated that in Denpasar, samples for direct sex workers were obtained each year at the same three brothel complexes, and that samples for indirect workers were taken from all registered ‘traditional massage parlours’. Similarly, in Tabanan, the same site was used to obtain specimens from direct sex workers each year. In other districts, the locations of the sampling of both direct and indirect sex workers changed from year to year. The authors sought information from the BHO about the rationale for choosing specific sites in these districts each year, but were not able to obtain an explanation.
Sample sizes in each district were determined by the BHO, based on available budget. At virtually all of the sex work sites, women were recruited on the basis of their presence at the time of visit by BHO staff. All women present were invited to participate until the intended sample size was achieved (consecutive sampling). From 2006 on, and at only the Denpasar sites, women were selected using the systematic random sampling method, with YKP providing the sampling list and assisting in the field recruitment after having compiled a field census with the help of pimps and brothel owners prior to the sero-survey implementation. This methodology was reported by BHO to have been consistently applied over the period of the surveys. 4
Consistently sampled annual series results for prisoners were available from most of the districts, with Lapas Kerobokan in Badung, the biggest prison in Bali, providing the largest number of samples. Kerobokan has also been the main prison in Bali for people incarcerated for offences related to drug use. Prisoners were recruited at each site on the basis of random sampling: sample size each year was determined in advance, after which cell blocks were selected by simple random sampling and all inmates in each selected block invited to participate. Again, the methodology was reported to have been consistent over the period.
In Denpasar District, people who inject drugs were surveyed during four years of the study period. Recruitment was assisted by the local non-government organization, Yakeba Foundation, and participants were recruited using respondent-driven sampling. The recruitment methods were described by BHO as being the same each year.
Based on the requirement for consistently collected surveillance data, we limited subsequent statistical analyses of time trends to data on prisoners from all districts, sex workers from Denpasar and Tabanan and people who inject drugs from Denpasar. Figure 1 shows trends among prisoners in Badung (Kerobokan) and in the other districts. The prevalence has declined steadily in Kerobokan from 19 (CI ±5.59) to 4.3% (CI ±2.74) over 10 years (P < 0.05), and has been stable at below 3% in other districts. In contrast, the HIV prevalence among both direct and indirect female sex workers has increased steadily. Among direct sex workers, the prevalence in Denpasar and Tabanan rose from 1% (CI ±1.21) to 20% (CI ±3.53) in the 10-year period, while among indirect workers in Denpasar, in whom there had been no HIV detected at the start of the period, the prevalence was 7% (CI ±3.5) by the end of 10 years (Figure 1) (P < 0.05). For people who injected drugs, there was no indication of a change in prevalence over the four years for which surveys were conducted (P = 0.213).
DISCUSSION
This report is the first detailed epidemiological analysis of the recent shift in the HIV epidemic in Bali from being predominantly linked to intravenous drug use to primarily affecting female sex workers. People who inject drugs still have the highest HIV prevalence in Bali, but it has remained stable over the last decade. In addition, despite the strong association between injecting drugs and incarceration, 8 HIV prevalence among prison inmates appears to be decreasing. This decline may reflect a change in the prison population, the impact of harm reduction programmes or both. 8 In Denpasar and Badung there are more than five centres implementing harm reduction programmes, run by both government and non-government agencies. In Kerobokan prison itself, a harm reduction programme began in 2001, with a VCT programme commencing in 2004. 8 Furthermore, there is evidence that the population of people who inject is itself decreasing in size, with a recent study estimating the number in Bali being 700–800, compared with 2500 people in 2003.9,10 It is possible that the stable level of HIV infection reflects sampling of an ageing and diminishing cohort of people who inject drugs.
Based on the analyses reported in this paper, when restricting time trend assessment to consistently sampled sites, it appears that the increase of HIV prevalence among women engaged in sex work is real and substantial. Rising rates of HIV in this population are an important public health concern, for the women themselves, for their male sexual partners and for other women who are partners of these men.2,11,12 The Bali AIDS Commission in 2007 reported almost 3000 direct female sex workers working in brothel complexes in Bali, with most in Denpasar. 13 The Ministry of Health in 2006 estimated that more than 82,000 men were clients of brothel-based sex workers and 25,000 were clients of other sex workers in Bali.
Apart from the serological surveys, the only alternative information on HIV prevalence in populations at higher risk has come from the Integrated Behavioural and Biological Survey (IBBS) conducted in 2007 in 11 Indonesian provinces. This survey, which included 250 brothel-based female sex workers in Bali, found that the province had the second highest HIV prevalence for this population, 14% (CI ±4.3), 14 a figure comparable with the estimate of 15% (CI ±4.34) from the serological sero-survey in the same year based on Denpasar and Tabanan sites. The IBBS 2007 report also showed that consistent condom use among sex workers in Bali was low, and that the Bali workers had the largest number of clients per week among workers in the IBBS provinces.14,15
Based on sero-surveys conducted primarily in Denpasar District, HIV sero-prevalence among waria and gay men in Bali is already high. According to behavioural surveys, both groups engage in sex work, with a higher percentage among warias.2,14–16 In Bali, a recent study estimated that there were between 430 and 900 waria and 12,000 gay men living in Denpasar and Badung districts. 17 As in many developing countries, these populations can be hard to reach for prevention programmes, which may be opposed by religious and other social opinion leaders. In light of the results of our study, more importance should be placed on interventions to prevent HIV transmission in these groups. 5
Under WHO-UNAIDS guidelines, if HIV prevalence among at least one population group is consistently above 5% and below 1% in the general adult population, the HIV epidemic is ‘concentrated’, while if prevalence has reached 1% in the general adult population, then the epidemic is considered to be ‘generalized’. 18 However, it is recognized that this classification should be applied with care, as in most countries HIV prevalence among the general adult population is estimated using HIV prevalence among pregnant women, 19 which can differ substantially from estimates derived from general adult population surveys. 20
In Denpasar, all pregnant women tested were seen at primary health centres facilities operated by the government. Since many pregnant women also seek antenatal care from other facilities, mostly private, the sample of women surveyed may not be representative.18,21 A PMTCT programme run by a local NGO in the same years reported HIV infection in 1.2% (CI ±1.4) of pregnant women 2009 and in 0.87% (CI ±.85) of pregnant women in 2010 22 on the basis of 458 tested in 2010.
Our detailed examination of the sero-survey data indicates several ways in which their quality could be improved. First, survey results should be recorded and retained in line record form, and consideration given to including age, at least, as an additional field for each person in the survey. Having sufficient numbers of participants at each site for each round, and consistent sampling of sites over time, would ensure the consistency and representativeness of survey results. Increased numbers of participants would provide the possibility of analysing prevalence by age subgroups, supplying information that would provide a better understanding of epidemic dynamics.
To further inform and understand the epidemic, it would also be helpful to add behavioural questions to the sero-surveys. These would provide indicators that could be used to monitor the impact of prevention programmes.18–20,23,24 The national IBBS, run by the central government, has provided useful information regarding epidemic progress nationally, but it is undertaken with long time intervals between rounds and does not specifically address the epidemic at the provincial level in Indonesia. The IBBS could be adapted to meet local needs and research questions. Ideally, the IBBS and local surveillance system could be better integrated to prevent duplication of effort and improve efficiency.
Since the surveillance findings indicate that the epidemic is being driven by unsafe sexual behaviours, more research on social and sexual networks is needed. 25 Ethnographic and qualitative studies can provide a better understanding of network structures and how they relate to epidemic patterns, and can assist in identifying which interventions are appropriate for each population. 26
Finally, the quality and value of the surveillance system would be enhanced by the provision of local human resources to plan, implement and evaluate its activities. Capacity building in the methods of surveillance and allocation of human resources with responsibility for design and analysis of surveys are critical steps on this pathway. 23
Footnotes
ACKNOWLEDGEMENTS
We would like to acknowledge our colleagues at the Bali Health Office, especially Dr Nyoman Subrata and Dr Agus Suryadinata, for trusting us with and sharing their data for this study. We also offer our appreciation to the staff of Badung and Denpasar Health Offices for their willingness to help us validate the data. This project was carried out with support from the Australian Agency for International Development. JMK is a National Health and Medical Research Council Senior Principal Research Fellow.